
Abstract
Introduction
The objective of this systematic review was to synthesise the evidence for cognitive strategy training to determine its effectiveness to improve performance of activities of daily living in an adult neurological population.
Method
Medline, CINAHL, EMBASE, PSYCInfo, PsycBITE and Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews were searched until August 2019. Studies examining the effect of cognitive strategy training on functional performance were included. Population criteria included adults with non-progressive neurological conditions. External and internal validity of included studies was systematically evaluated using an appropriate methodological quality assessment for each study design. A content analysis was conducted of the methodologies used.
Findings
Forty-one studies met the inclusion criteria and were appraised for content, 16 randomised or quasi-randomised trials were meta-analysed. Trial quality was generally ‘good’, Physiotherapy Evidence Database scale scores ranged from 3 to 8 (out of 10). For activity performance outcomes post-intervention, there was a significant benefit of cognitive strategy training over usual care (standardised mean difference 0.79, 95% confidence interval 0.49–1.09; P < 0.00001).
Conclusion
More high-quality research is needed to strengthen the evidence base for cognitive strategy interventions to improve activity performance outcomes for adults with non-progressive neurological conditions.
Systematic review registration
PROSPERO CRD42016033728
Introduction
Cognitive strategies are mental plans of action that assist the person to approach task performance systematically, thus allowing people to learn new skills and perform tasks with improved accuracy and efficiency (Toglia et al., 2012). Cognitive strategy use is common in task performance when people without a neurological condition are faced by novel or challenging tasks (Bottari et al., 2014; Toglia et al., 2012). After neurological impairment, however, people frequently experience persisting physical, sensory and cognitive impairments that impact on their ability to perform everyday tasks. Activities that were previously familiar present the individual with novel challenges as they attempt to perform them with altered capacity. As a result, there is an increased need to use cognitive strategies to support and improve the performance of everyday tasks. The ability to select and use cognitive strategies efficiently is commonly impaired (Kennedy et al., 2008; Krasny-Pacini et al., 2014). For example, individuals may not anticipate difficulties that will arise during task performance and consequently fail to initiate strategy use as the need arises or they may not spontaneously generate a range of strategies and as a result persist in using inefficient strategies (Bottari et al., 2014; Kennedy and Coelho, 2005).
Cognitive strategy-based interventions aim to promote functional recovery by restoring the individual’s ability to use cognitive strategies to compensate for impairments resulting from their neurological condition (Chung et al., 2013; Geusgens et al., 2007b). It has been suggested that cognitive strategy interventions have the potential to promote additional functional recovery beyond the intervention because an important emphasis is teaching the individual to generalise skills learned to solve performance challenges not directly addressed in the intervention. Cognitive strategy interventions are of particular relevance to occupational therapists as a means to facilitate client goal attainment and improve the client’s ability to participate in meaningful activities of daily living (ADL) in a variety of environments. As a result, there is growing interest in cognitive strategy training and several different interventions or approaches have been described.
Previous systematic reviews have examined the efficacy of cognitive rehabilitation interventions, including cognitive strategy training, for individuals with executive impairments following traumatic brain injury (TBI) (Cicerone and colleagues, 2005, 2011, 2019; Kennedy et al., 2008; Kumar et al., 2017) and stroke (Chung et al., 2013; Poulin et al., 2012). Findings suggest that cognitive strategy training may improve performance on measures of executive functioning (Cicerone et al., 2011, 2019; Chung et al., 2013; Poulin et al., 2012). However, the effect of cognitive strategy training on the performance of everyday tasks is largely inconclusive in these previous systematic reviews. In addition, new studies investigating the efficacy of cognitive strategy training have been published since these earlier reviews. Therefore, the purpose of this review was to determine whether cognitive strategy training improves performance of everyday tasks for adults with neurological conditions, including TBI and stroke. The review was guided by the research question: ‘Is cognitive strategy training effective at improving ADL performance in adults with neurological conditions?’
Methods
Design and search strategy
Inclusion criteria.

ADL: activities of daily living.
Selection criteria
Participants
Studies were included if they involved adult participants with non-progressive, neurological conditions (non-traumatic or traumatic causes). The number of participants, their mean age and time since onset of acquired brain injury and type of rehabilitation setting were recorded to examine the similarity of the studies.
Intervention
Studies were included if they examined the effect of cognitive strategy interventions. Cognitive strategies were defined as ‘goal-directed and consciously controllable processes that facilitate or support performance as learners develop internal procedures that enable them to perform the desired skill’ (McEwen et al., 2009a: 263). Comparative interventions included usual care (also known as standard therapy or conventional therapy), any other cognitive rehabilitation approach, or no-intervention controls.
Outcome
Studies were considered if they included at least one outcome measure of performance of everyday activities (such as self-care, productivity or leisure), which could be either a standardised measure or observational assessment. In studies in which several activity performance measures were available, reviewers chose the outcome measure that most closely reflected the performance of meaningful ADL. Activity performance outcome measures used and timing of measurement were recorded to assess similarity of studies.
Study design
Intervention studies of any design were included, given the recency of the intervention approach.
Data extraction
One reviewer (RS) extacted data on study design, participant characteristics (including age, diagnosis and time since injury), a description of the experimental and comparator intervention (including content of intervention, rehabilitation setting, timing of intervention post-injury, duration and dosage) and outcome measures assessed. Two reviewers (RS and NAL) extracted outcome data. Outcome data extracted included sample size and results for activity performance measures. When available, the authors extracted pre/post-mean change scores and their standard deviations (SD), confidence intervals and P values, and if not available the authors extracted post-intervention scores (e.g. mean (SD) or median (interquartile range) scores). All calculations were based on the data in the published article, except in one case in which additional data were requested and provided by the study authors (Kessler et al., 2017). When included studies reported insufficient information (e.g. missing SD), data were converted to enter an estimated value using methods described in the Cochrane Handbook of Systematic Reviews (Higgins and Green, 2011). All outcome data and calculations were independently cross-checked by a third reviewer (LC).
Risk of bias and methodological quality assessment
Three researchers (RS, TH and MM) independently rated the methodological quality of included studies using an appropriate methodological quality assessment tool for each study design. Consensus was reached through discussion when there were differences in ratings. A third author (MM or NAL) was consulted to resolve differences in ratings when consensus could not be reached. Only the ratings of randomised controlled trials (RCTs) and quasi-RCTs are reported; all other ratings were used to determine the internal/external validity of the overall body of literature.
The methodological quality of RCTs and quasi-RCTs was assessed using the Physiotherapy Evidence Database (PEDro) scale. The PEDro scale is a reliable (Maher et al., 2003) and valid (de Morton, 2009) criterion-based measure of trial quality. It examines 11 criteria to determine the selection, performance, detection and attrition biases present within a study. Scores range from 0 to 10. Studies that score 9–10 on the PEDro scale are considered to represent ‘excellent’ methodological quality, 6–8 ‘good’ quality, 4–5 of ‘fair’ quality and 3 and below of ‘poor’ methodological quality. When available, scores were extracted from the Physiotherapy Evidence Database (www.pedro.org.au). When a study was not included on the PEDro database, two researchers (RS and TH) independently rated the study.
Non-randomised comparative study designs were rated using the Downs and Black checklist (Downs and Black, 1998). This checklist provides a profile of methodological quality across four areas including: study reporting, external validity, internal validity (bias and confounding) and statistical power. The authors used a modified version of scoring for the statistical power criterion previously employed in other studies (Silverman et al., 2012), thus producing a total score of 28, with higher scores indicating stronger methodological quality.
Single participant designs were rated using the Risk of Bias in N-of-1 Trials (RoBiNT) scale (Tate et al., 2015). The RoBiNT rates across two subscales: the internal validity scale which examines design, randomisation, behaviour sampling, participant, practitioner and assessor blinding and treatment adherence; and the external validity and interpretation scale which assesses reporting of baseline characteristics, setting, dependent variable, independent variable, raw data record, data analysis, replication and generalisation. The RoBiNT is scored out of a total of 30, with higher scores indicating stronger methodological quality.
Data synthesis
Levels of evidence.
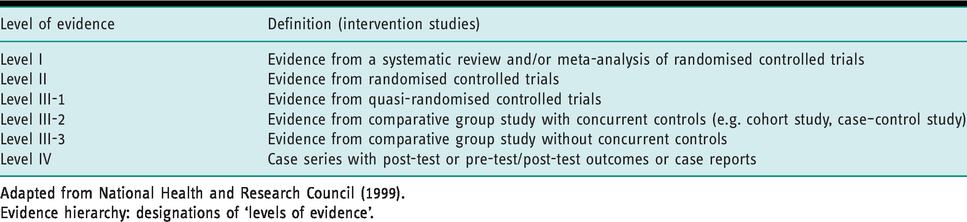
Adapted from National Health and Research Council (1999).
Evidence hierarchy: designations of ‘levels of evidence’.
Results
Flow of studies through the review
The search strategy identified 4112 studies. After duplicates were removed, the titles and abstracts of 2846 studies were screened. The full texts of 123 potentially eligible studies were retrieved. Eighty-two studies did not meet the inclusion criteria; Figure 1
Flow of studies through the systematic review (Moher et al., 2009).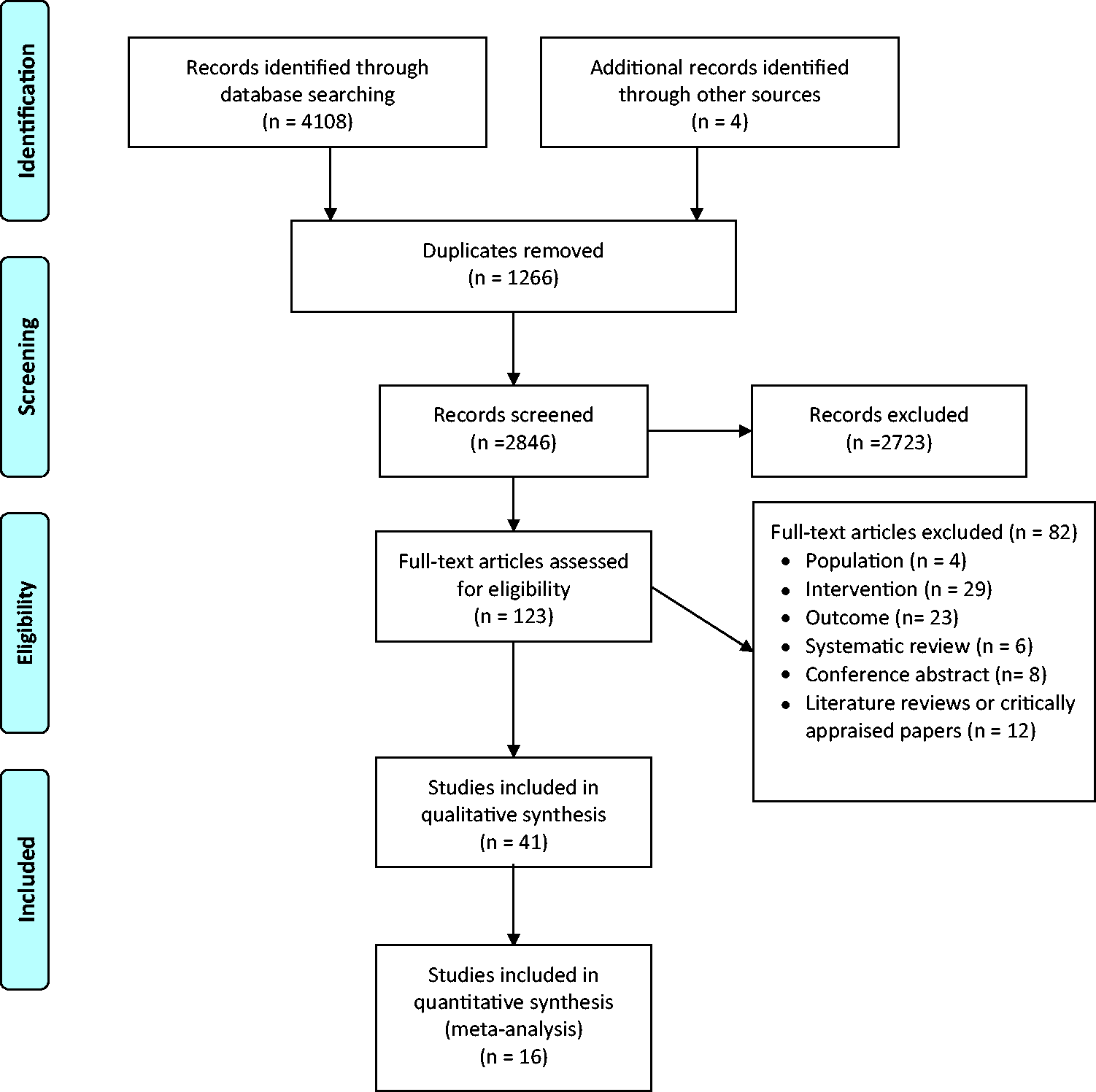
Summary of included studies: interventions and participants (n = 41 studies).

Exp: experimental group; Con: control group; min: minutes; wk: week/s; mo: months; yr: years; TBI: traumatic brain injury; BT: Brain Tumour.
Study presented longer term outcomes from previously reported trial or conducted additional analysis of trial data.
Summary of included studies: research method (n = 41 studies).
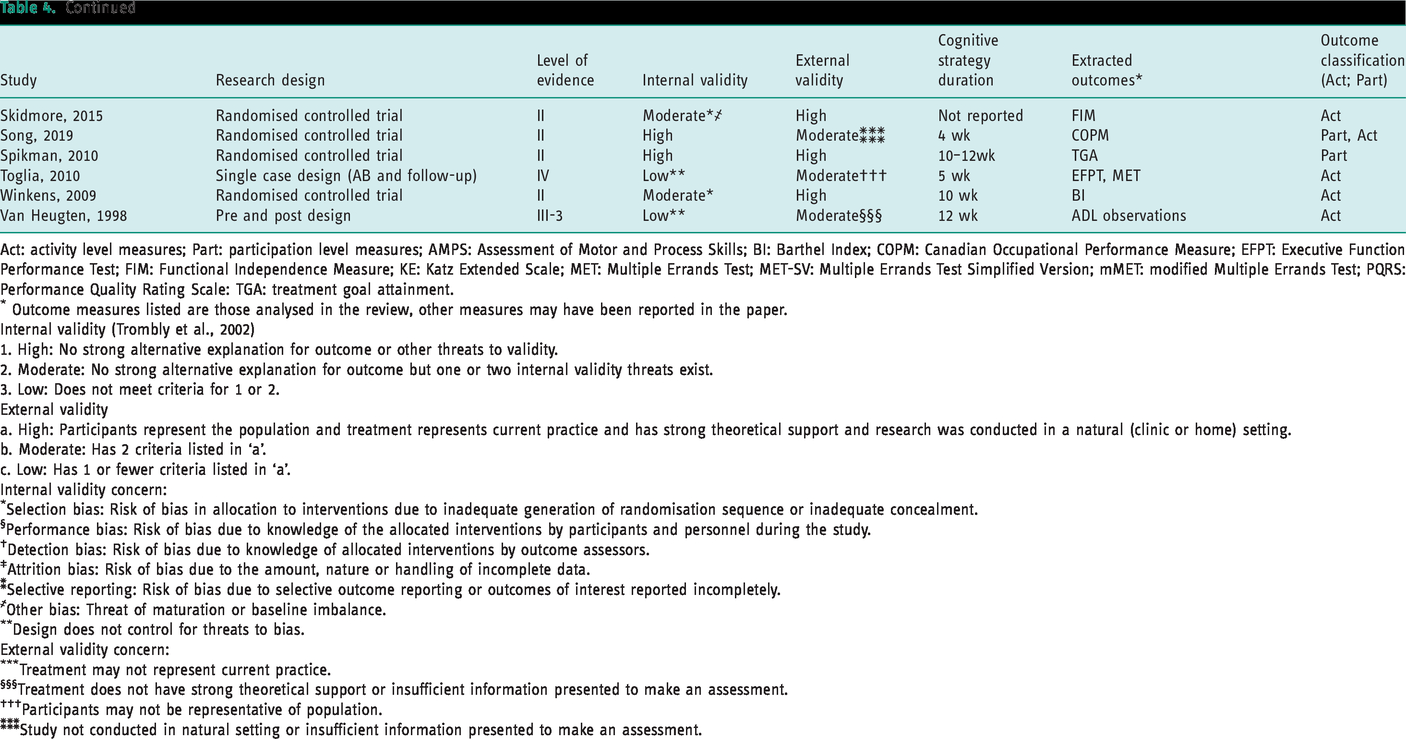
Act: activity level measures; Part: participation level measures; AMPS: Assessment of Motor and Process Skills; BI: Barthel Index; COPM: Canadian Occupational Performance Measure; EFPT: Executive Function Performance Test; FIM: Functional Independence Measure; KE: Katz Extended Scale; MET: Multiple Errands Test; MET-SV: Multiple Errands Test Simplified Version; mMET: modified Multiple Errands Test; PQRS: Performance Quality Rating Scale: TGA: treatment goal attainment.
Outcome measures listed are those analysed in the review, other measures may have been reported in the paper.
Internal validity (Trombly et al., 2002)
1. High: No strong alternative explanation for outcome or other threats to validity.
2. Moderate: No strong alternative explanation for outcome but one or two internal validity threats exist.
3. Low: Does not meet criteria for 1 or 2.
External validity
a. High: Participants represent the population and treatment represents current practice and has strong theoretical support and research was conducted in a natural (clinic or home) setting.
b. Moderate: Has 2 criteria listed in ‘a’.
c. Low: Has 1 or fewer criteria listed in ‘a’.
Internal validity concern:
Selection bias: Risk of bias in allocation to interventions due to inadequate generation of randomisation sequence or inadequate concealment.
Performance bias: Risk of bias due to knowledge of the allocated interventions by participants and personnel during the study.
Detection bias: Risk of bias due to knowledge of allocated interventions by outcome assessors.
Attrition bias: Risk of bias due to the amount, nature or handling of incomplete data.
Selective reporting: Risk of bias due to selective outcome reporting or outcomes of interest reported incompletely.
Other bias: Threat of maturation or baseline imbalance.
Design does not control for threats to bias.
External validity concern:
Treatment may not represent current practice.
Treatment does not have strong theoretical support or insufficient information presented to make an assessment.
Participants may not be representative of population.
Study not conducted in natural setting or insufficient information presented to make an assessment.
Of the 22 RCTs and quasi-RCTs, 16 were included in the meta-analysis (Ahn, 2019; Ahn et al., 2017; Bertilsson et al., 2014; Dawson et al., 2013; Donkervoort et al., 2001; Goverover et al., 2007; Kessler et al., 2017; Liu and Chan, 2014; Liu et al., 2004a; McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Skidmore et al., 2015; Song et al., 2019; Spikman et al., 2010; Winkens et al., 2009). Six studies were not included for the following reasons: Guidetti et al. (2010) reported median and interquartile range and subsequently data could not be pooled in the meta-analysis. Two studies presented long-term outcomes from previously reported trials (Guidetti and Ytterberg, 2011; Guidetti et al., 2015) and one study conducted additional analysis of data from the original trial (Geusgens et al., 2006). When possible data from these studies were analysed together with the original study. Two studies compared cognitive strategy interventions in both intervention and control conditions (Bertens et al., 2015; Ownsworth et al., 2008). Consequently, these studies were not included in the meta-analysis.
Characteristics of included studies
Methodological quality
Study quality scores using PEDro scale for included RCTs and quasi-RCTs (n = 16 studies).
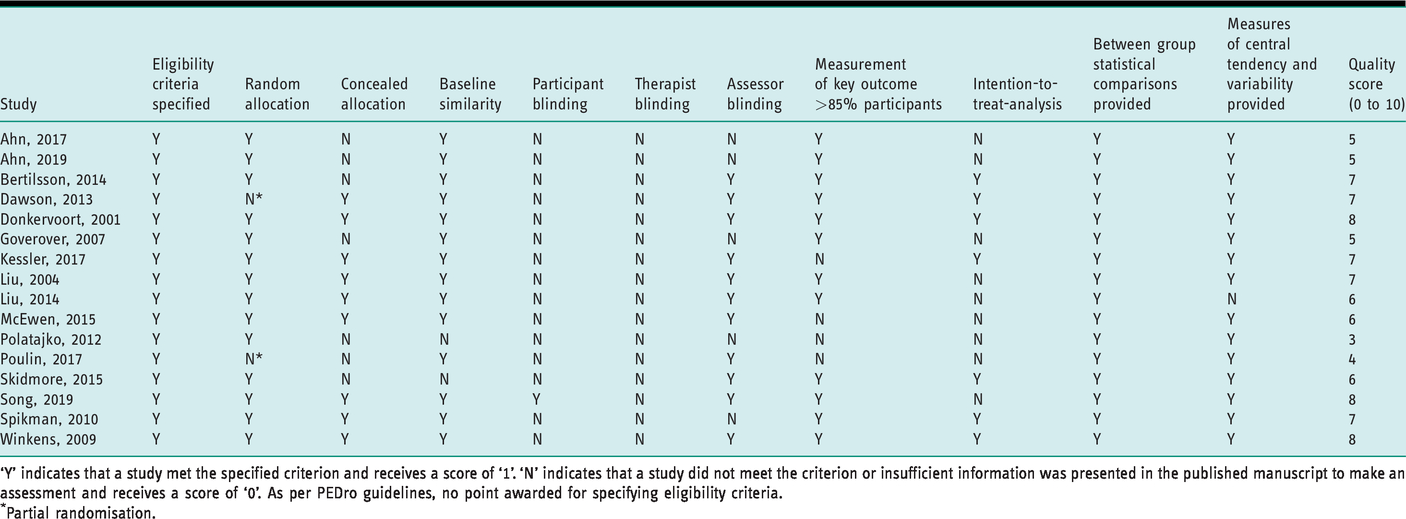
‘Y’ indicates that a study met the specified criterion and receives a score of ‘1’. ‘N’ indicates that a study did not meet the criterion or insufficient information was presented in the published manuscript to make an assessment and receives a score of ‘0’. As per PEDro guidelines, no point awarded for specifying eligibility criteria.
Partial randomisation.
Participants
The included trials recruited 889 participants, 811 (91%) of whom completed post-intervention assessment (Table 3). Sample sizes varied considerably across trials; five studies (31%) recruited sample sizes of less than 25 participants, eight (50%) studies recruited sample sizes of less than 50 participants, one study (6%) recruited less than 100 participants and only two studies (12%) involved sample sizes greater than 100 participants. Overall, studies included 796 (91%) participants with stroke, 65 (7%) with TBI and 10 (1%) were diagnosed with other causes of neurological injury (for example, post-revision of low-grade brain tumour). Participants were predominantly working age adults, with the mean age of participants ranging from 39 to 72 years. The length of time since the onset of neurological condition ranged from under 7 days to 10 years.
Intervention
Ten different cognitive strategy interventions were used across included trials (Table 3): client-centred ADL intervention (Bertilsson et al., 2014), cognitive orientation to daily occupational performance (Ahn et al., 2017; Dawson et al., 2013; McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Song et al., 2019), metacognitive strategy training (Goverover et al., 2007), multifaceted strategy training (Spikman et al., 2010), occupation-based intervention (Ahn, 2019), occupational performance coaching – stroke (Kessler et al., 2017), self-regulation for promoting function (Liu and Chan, 2014; Liu et al., 2004a), strategy training (Skidmore et al., 2015), strategy training for apraxia (Donkervoort et al., 2001) and time pressure management (Winkens et al., 2009). Interventions were predominantly delivered in the outpatient or inpatient rehabilitation settings, and only provided in the participants’ home or relevant community settings in three studies. Cognitive strategy interventions were delivered by an occupational therapist in 10 (63%) studies, trained rehabilitation personnel or therapists in four (25%) studies, by either an occupational therapist or neuropsychologist in one (6%) study and by a neuropsychologist in one (6%) study. The intensity (minutes/session), frequency (days/week) and overall duration (weeks) of intervention varied across studies. Interventions ranged from 30-minute sessions to 120-minute sessions, at varied frequencies of between 1 and 5 days per week, with an intervention duration from 1 to 16 weeks.
Comparison interventions
Most studies compared cognitive strategy training with a comparable control intervention (Table 3). Comparative interventions included ‘standard’ or ‘usual’ occupational therapy (Ahn et al., 2017; Bertilsson et al., 2014; Donkervoort et al., 2001; Liu and Chan, 2014; Liu et al., 2004a; Polatajko et al., 2012), attention control in addition to usual care (Skidmore et al., 2015), usual care without (no) occupational therapy (Kessler et al., 2017), action focusing intervention (Ahn, 2019), task-specific retraining (Song et al., 2019), conventional task practice or functional retraining (Goverover et al., 2007), conventional cognitive rehabilitation (Winkens et al., 2009) and computer-based cognitive retraining (Poulin et al., 2017; Spikman et al., 2010). Only one study used a no intervention control group (Dawson et al., 2013). The majority of studies provided limited information detailing the procedures and contents of comparator interventions.
Outcome measures
Performance of ADL was measured using a variety of outcome measures (Table 3) including: Canadian Occupational Performance Measure Performance scale (eight comparisons), Treatment Goal Achievement Scale (one comparison), the Barthel Activity of Daily Living index (four comparisons), the Functional Independence Measure (three comparisons), Assessment of Motor and Process Skills (three comparisons), ADL observations (one comparison), everyday task performance rating (one comparison), Everyday Information Intake Task (one comparison), Performance Quality Rating Scale (four comparisons), Katz Activity of Daily Living Inventory (one comparison) and Frenchay Activities Index (one comparison). Due to the heterogeneity of outcome measures, it was not possible to include all outcomes in the analyses. Outcomes were measured immediately post-intervention in 14 studies. Post-intervention outcome assessment was conducted at 2–3 months in three studies. Follow-up data were presented in seven studies and the time interval varied from 1 to 12 months.
Intervention effects
To quantify the effects of cognitive strategy training we conducted separate random effects meta-analyses to understand activity performance outcomes for all participants, and for stroke-only participants which allowed determination of response variation across populations, and for timing of the intervention delivery.
Activity performance outcomes: all cognitive strategy training approaches
The immediate effect of cognitive strategy training compared to any other comparative intervention or no intervention was examined using a random effects model from 16 studies, involving 833 participants with non-progressive brain injury (Ahn, 2019; Ahn et al., 2017; Bertilsson et al., 2014; Dawson et al., 2013; Donkervoort et al., 2001; Goverover et al., 2007; Kessler et al., 2017; Liu and Chan, 2014; Liu et al., 2004a; McEwen et al., 2015; Polatajko et al., 2012; Poulin et al., 2017; Skidmore et al., 2015; Song et al., 2019; Spikman et al., 2010; Winkens et al., 2009). Cognitive strategy training improved activity performance outcomes for participants immediately after the intervention period (SMD 0.79, 95% CI 0.49–1.09) (Figure 2
Standard mean difference (SMD) (95% confidence interval (CI)) of the effect of cognitive strategy training compared with any comparative intervention or no intervention on activity performance outcomes immediately after intervention for people with non-progressive brain injury. *Incomplete data presented in the paper. Data estimated statistically.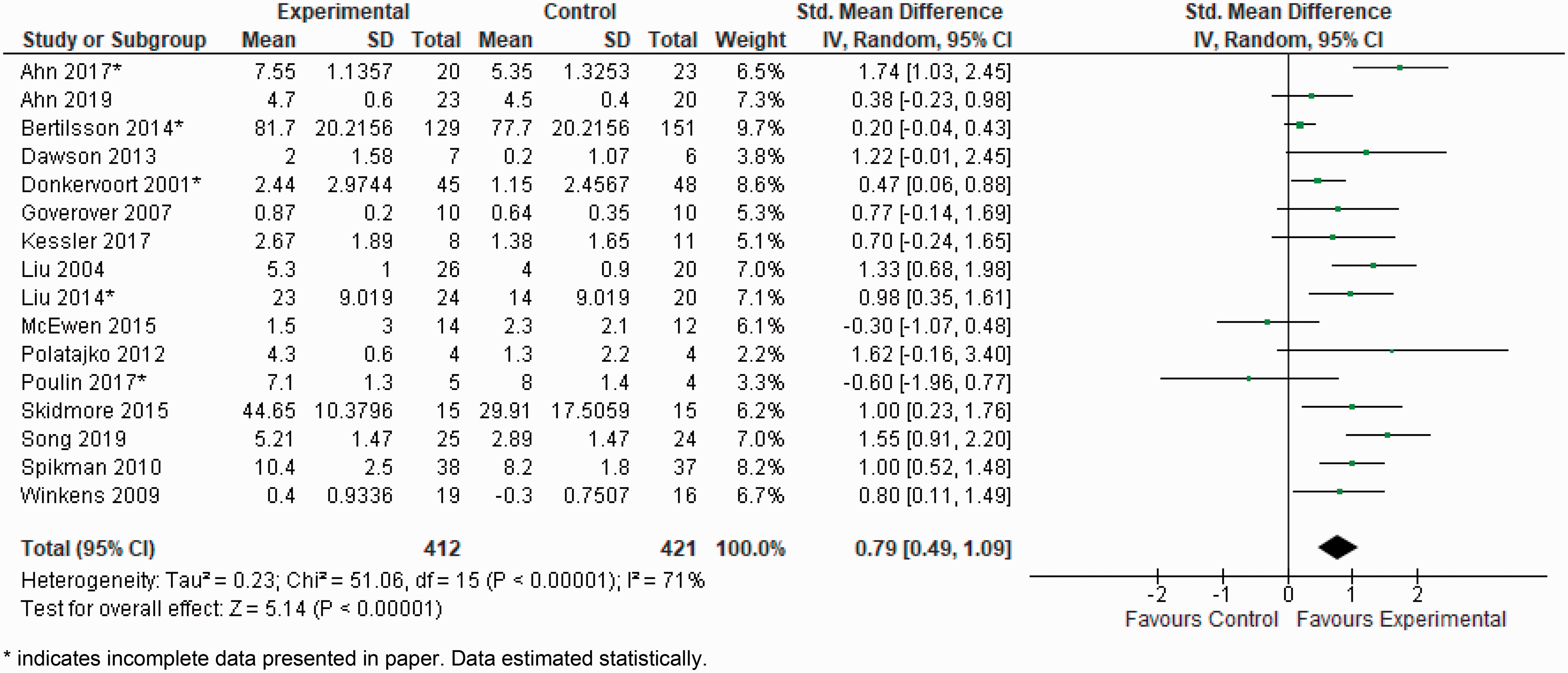
Seven studies, with 269 participants, presented follow-up data (i.e. >4 weeks and <12 months following post-intervention assessment) for this same comparison (Donkervoort et al., 2001; Kessler et al., 2017; McEwen et al., 2015; Poulin et al., 2017; Skidmore et al., 2015; Spikman et al., 2010; Winkens et al., 2009). Cognitive strategy training improved activity performance compared with usual care at the follow-up timepoint (SMD 0.41, 95% CI 0.13–0.70) (Figure 3
Standard mean difference (SMD) (95% confidence interval (CI)) of the effect of cognitive strategy training compared with any comparative intervention or no intervention on activity performance outcomes at follow-up time point for people with non-progressive brain injury.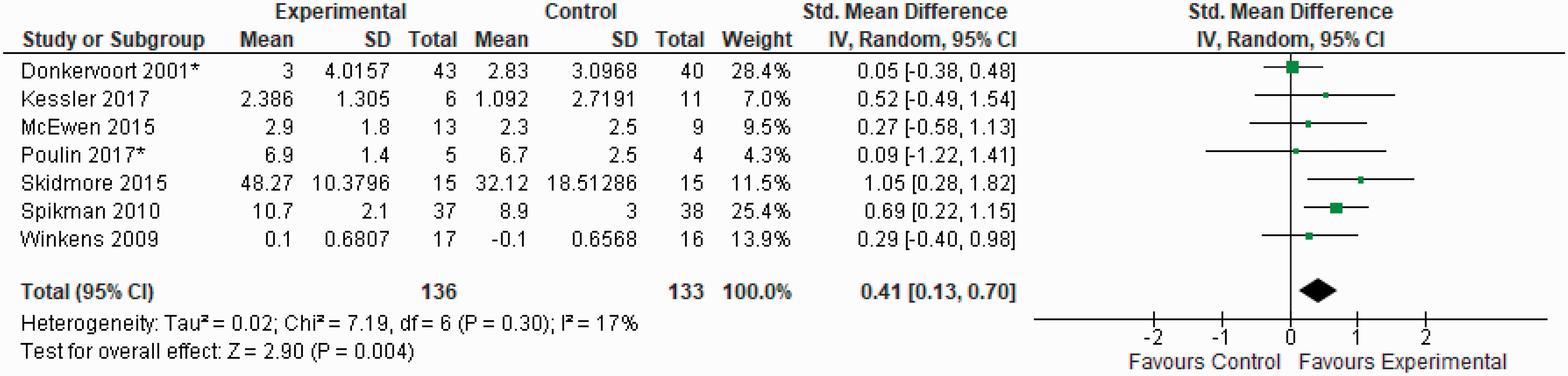
Activity performance outcomes: stroke participants only
The effect of cognitive strategy training for people diagnosed with stroke was examined by pooling post-intervention data from 13 studies, with 725 participants. Of these, five trials were conducted in early stage rehabilitation (less than 3 months since onset) (Bertilsson et al., 2014; Liu and Chan, 2014; Liu et al., 2004a; McEwen et al., 2015; Skidmore et al., 2015), seven were conducted in the chronic phase of rehabilitation (greater than 3 months following stroke) in outpatient or community rehabilitation settings (Ahn, 2019; Ahn et al., 2017; Kessler et al., 2017; Polatajko et al., 2012; Poulin et al., 2017; Song et al., 2019; Winkens et al., 2009) and one study offered the intervention to participants within 2 years of stroke onset in either inpatient rehabilitation or a nursing home setting (Donkervoort et al., 2001). Cognitive strategy training improved activity performance in stroke participants compared to usual or standard care (SMD 0.75, 95% CI 0.41–1.10) (Figure 4
Standard mean difference (SMD) (95% confidence interval (CI)) of the effect of cognitive strategy training compared with any comparative intervention on activity performance outcomes immediately after intervention for people with stroke. *Incomplete data presented in paper. Data estimated statistically.
Timing of providing cognitive strategy interventions
The effect of cognitive strategy training conducted in an early phase of rehabilitation (less than 3 months from onset) compared with usual care was examined by pooling post-intervention data from five studies, with 426 participants (Bertilsson et al., 2014; Liu and Chan, 2014; Liu et al., 2004a; McEwen et al., 2015; Skidmore et al., 2015). Cognitive strategy training improved activity performance compared to usual or standard care (SMD 0.63, 95% CI 0.07–01.19); however, again heterogeneity was high (I2 = 80%). The effect of cognitive strategy training conducted in the chronic stage of recovery (greater than 3 months from onset) was explored by pooling data from 10 studies with 314 participants (Ahn, 2019; Ahn et al., 2017; Dawson et al., 2013; Goverover et al., 2007; Kessler et al., 2017; Polatajko et al., 2012; Poulin et al., 2017; Song et al., 2019; Spikman et al., 2010; Winkens et al., 2009). The results also favoured cognitive strategy training (SMD 0.95, 95% CI 0.59–1.32); heterogeneity between studies was moderate (I2 = 49%).
Discussion
This systematic review sought to understand the benefit of using a cognitive strategy training approach to improve activity performance for adults with non-progressive neurological conditions, including TBI and stroke. While different cognitive strategy training approaches were identified across studies, there was sufficient similarity between intervention approaches to permit meta-analysis. Our findings indicate that cognitive strategy training resulted in greater improvements in activity performance when compared to conventional or standard care, which mostly included occupational therapy of unspecified dose or approach.
While we report a positive effect for cognitive strategy training in improving activity performance, these findings need to be interpreted with caution. Many of the included studies were limited by small sample sizes that did not have sufficient power to detect clinically meaningful effects of intervention. Furthermore, there was considerable variability between studies in outcome measures used to measure changes in activity performance, as well as the timing and intensity of cognitive strategy interventions. Taking all this into account, our conclusion is that the evidence-base for cognitive strategy training is currently insufficient and no strong conclusions can be drawn to guide clinical practice.
Limited consensus exists in the rehabilitation literature on the most appropriate outcome measures to measure changes in activity performance and participation for adults with neurological conditions, and considerable variability was evident in the outcome measures used across included studies. Many existing studies used outcome assessments limited to self-care performance outcomes or used observational measures of activity performance with limited psychometric properties. Consistent with the review of Chung and colleagues (2013), our review applied their stricter definition of activity performance and we did not include measures of error frequency (e.g. number of errors made during task performance) or completion of steps (e.g. omission of essential task steps or addition of unnecessary steps) as a measure of activity performance, instead appraising these outcomes as being at the body function and structures level of the International Classification of Functioning, Disability and Health (ICF) (World Health Organization, 2001). It remains unclear to what extent changes to these outcomes reflect actual improvements in everyday task performance (Cramm et al., 2016). The primary goal of rehabilitation is to improve the individual’s ability to participate in meaningful everyday activities. It is essential therefore that future studies use outcome measures that more accurately reflect the performance of a broader range of everyday tasks that are relevant and meaningful to individuals with neurological conditions, for example the Canadian Occupational Performance Measure (Law, 1998) or the Assessment of Motor and Process Skills (Fisher and Jones, 2012).
The optimal timing of cognitive strategy training is not currently well understood, and variability in the timing of intervention across studies was evident. Our review included studies conducted in all stages of rehabilitation, from acute inpatient to chronic community rehabilitation settings. Only one included study recruited participants in the subacute stage of rehabilitation (McEwen et al., 2015). This is surprising given that there is consensus that rehabilitation provided early following neurological injury has a greater effect on longer term functional outcomes (Wolf et al., 2015). This is an important gap that needs to be addressed by future research.
There was considerable variability in how cognitive strategy training interventions were delivered with respect to intensity, frequency and duration across the trials. Cognitive strategy training interventions were also inconsistently conducted in conjunction with other occupational therapy and/or psychology treatments. As such, we are unable to comment on optimal protocols or doses for cognitive strategy training. Many studies lacked detail about the content of conventional or standard care being compared to cognitive strategy training interventions, and few studies published an intervention guide or protocol that would facilitate replication. We acknowledge the improvement in study reporting with the release of the updated CONSORT statement (Schulz, Altman and Moher, 2010) and the TIDieR checklist as an extension of the CONSORT statement (Hoffmann et al., 2014). Future trials must adhere to these reporting recommendations to enable future synthesis and allow for accurate comparisons, as well as researchers and clinicians alike to be able to understand the nature of the interventions delivered. This is important to enable clinicians to make informed decisions on the suitability of cognitive strategy training for their client population and clinical setting.
Every effort was made throughout all stages of the systematic review to limit potential sources of bias. However, there are some limitations that need to be considered when interpreting the findings. The meta-analysis may have been affected by small study bias; over one-third (36%) of studies included a sample size of less than 25 participants per study. The authors additionally experienced incomplete data reporting in included studies. Consequentially, data were estimated statistically, which may impact on the precision of pooled results.
Implications for practice and future research
Limited evidence currently exists regarding the effectiveness of cognitive strategy interventions for improving activity performance for adults with non-progressive neurological conditions, such as brain injury or stroke. No strong conclusions can be drawn to guide occupational therapy practice on the optimal cognitive strategy intervention approach or on dosage, intensity or timing of cognitive strategy intervention approaches. Larger, well-conducted RCTs that eliminate potential risks of bias are required to provide stronger evidence to support the use of cognitive strategy training. It is important that the feasibility and acceptability of future RCTs be carefully considered to ensure that a sufficient number of participants can be recruited to and retained within the trial. In addition, researchers should use objective and methodologically robust outcome measures of activity and performance. Furthermore, there is a need to consider participants’ perspectives on the acceptability and suitability of cognitive strategy training interventions. This is an area that is largely unexplored and requires consideration because participant perspectives are likely to influence levels of engagement and may even influence the potential success of interventions (Gillespie et al., 2015).
Key findings
Cognitive strategy training approaches demonstrated a positive benefit on activity performance for adults with non-progressive neurological conditions compared to conventional or standard care, but the strength of these findings are limited by a high degree of variability between studies. No strong conclusions can be drawn to guide clinical practice on the optimal approach or dosage, intensity or timing of intervention delivery. More high quality research is needed to determine the efficacy of cognitive strategy training interventions on improving activity performance and participation.
What the study has added
This systematic review presented the current evidence on cognitive strategy interventions for improving activity performance in adults with non-progressive neurological conditions. Future research should better define comparsion interventions, include a larger sample size and use objective and methodologically robust measures of activity performance and participation.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620933095 - Supplemental material for Cognitive strategy training for adults with neurological conditions: a systematic review and meta-analysis exploring effect on occupational performance
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620933095 for Cognitive strategy training for adults with neurological conditions: a systematic review and meta-analysis exploring effect on occupational performance by Ruth Swanton, Louise Gustafsson, Elspeth Froude, Tenelle Hodson, Michelle McInerney, Liana S Cahill and Natasha A Lannin in British Journal of Occupational Therapy
Footnotes
Acknowledgements
Acknowledgements are extended to Ms Jennifer Crosbie and Ms Samantha Fernandez, Librarians, Australian Catholic University, Sydney, Australia, for providing guidance and assistance with literature search strategies and database searches.
Research ethics
Ethics approval was not required for this study.
Consent
Consent was not applicable to this systematic review as no human subjects were involved.
Declaration of conflicting interests
The author(s) confirm that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. NAL is supported by National Heart Foundation of Australia Future Leaders Fellowship (GNT102055). LC is supported by La Trobe University Postgraduate Scholarship.
Contributorship
RS, LG, EF and NAL conceptualised and designed the review; RW and NAL developed the search strategy; RS undertook database searches; RS and TH screened studies for eligibility, and RS, TH and MM conducted methodological assessment of included studies; RS, LC and NAL completed statistical analyses; RS and NAL drafted the manuscript; and all authors assisted in interpretation of findings and critically reviewed the manuscript.
Systematic review registration
PROSPERO CRD42016033728
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.