
Abstract
Introduction
This study aimed to clarify factors associated with post-stroke depression in patients with acute stroke within 2 weeks of onset.
Method
Eighty-eight patients with stroke were divided into post-stroke depression (n = 49) and non-post-stroke depression (n = 39) groups based on their Hamilton Depression Rating Scale scores. We evaluated stroke severity, upper limb function, activities of daily living, frontal lobe/cognitive function, and level of apathy. Activity levels were measured using an ActiGraph GT9X Link system. Mann–Whitney U-tests were used to determine differences between the two groups. Spearman’s rank correlation and logistic regression analyses were also performed.
Results
The post-stroke depression and non-post-stroke depression groups exhibited significant differences in National Institutes of Health Stroke Scale scores at admission and discharge; Functional Independence Measure exercise items, cognitive items, and total items at admission; Fugl-Meyer Assessment scores; and Apathy Rating Scale scores. Logistic regression indicated that Fugl-Meyer Assessment scores were associated with post-stroke depression.
Conclusion
Stroke severity, paralysis, and physical function/activities of daily living ability are associated with post-stroke depression in the acute phase. Our findings suggest that increases in physical impairment severity are associated with increased post-stroke depression risks. Rehabilitation professionals should focus on identifying post-stroke depression in early post-stroke stages.
Introduction
Of the 56,900,000 deaths worldwide in 2016, ischaemic heart disease and stroke represented the leading causes, accounting for 15,200,000 total deaths (26.7%). In addition, these diseases have been the leading causes of death worldwide for the past 15 years (World Health Organization, 2018). In 2015, the total number of patients with cerebrovascular disease in Japan was 1,179,000, with more than 290,000 new strokes occurring annually. Moreover, researchers have predicted that the total worldwide number of patients with stroke will exceed 3,000,000 by 2020 (Takashima et al., 2018).
Although stroke is associated with various sequelae, patients exhibiting depressive symptoms following stroke are considered to have post-stroke depression (PSD). According to the World Health Organization (WHO), the overall prevalence of depression is 3% worldwide. While the frequency of PSD varies by report, reviews by Ayerbe et al. (2013) and Hackett and Pickles (2014) have suggested that it occurs in 29% and 31% of patients with stroke, respectively. Wassink-Vossen et al. (2014) found that people over 60 years of age with depression have lower physical activity than those without depression, and that high physical activity reduces the risk of depression in older people (Wassink-Vossen et al., 2014). A depressed mood and reduced motivation due to PSD are related to an individual’s level of physical activity and participation in rehabilitation (George et al., 2001).
Furthermore, low levels of physical activity and motivation are known to hinder improvement in motor paralysis, sensory disturbance, higher brain dysfunction, and impairment in activities of daily living (ADL) (Kutlubaev and Hackett, 2014; Shimoda and Robinson, 2016). Mortality rates can be up to 10 times higher in patients with PSD than in those without (Miranda et al., 2018). According to a systematic review of previous studies, the reported prevalence of depression was 29%, with a cumulative incidence of 39–52% within 5 years of stroke (Ayerbe et al., 2013). In addition, PSD 3 months after its onset has been associated with poor functional outcomes at the 1-year follow-up (Wade et al., 1987). In other words, the longer it takes to start appropriate treatment, the worse the progression of depressive disorders can be. Therefore, it is important to detect and treat depression symptoms early (de Diego-Adeliño et al., 2010).
In the present study, we aimed to clarify the factors associated with PSD in patients with acute stroke within 2 weeks of onset. To achieve this, we examined levels of depression, physical function, cognitive function, and physical activity in patients with acute stroke. We believe that clarifying these factors may allow for the prediction of PSD in the acute phase, enabling rehabilitation professionals to adopt early intervention strategies.
Literature review
Because previous research has indicated that PSD is associated with subsequent decreases in the quality of life of patients with acute stroke (Kim et al., 2018), it is important to first evaluate PSD in the acute phase (Kneebone et al., 2010). In addition, by detecting PSD from an early stage, the effect of PSD may be reduced with treatment, which may contribute to improving the prognosis of stroke. PSD can be treated with pharmacotherapy and non-pharmacotherapy options. Pharmacological and psychosocial interventions have been shown to reduce the likelihood of developing PSD and improve the depressive symptoms of PSD (Towfighi et al., 2017). In recent years, it has been suggested that occupational therapists should be involved in non-drug therapies that can be as effective as drug treatment. Therefore, it is important that occupational therapists are involved in the detection of PSD early after stroke.
Although PSD usually develops within the first few months after stroke (Dafer et al., 2008), only 12% of patients exhibit depressive symptoms within the first 12 months (Berg et al., 2003). Indeed, several previous reports have discussed cases of PSD occurring within the first 3 months after stroke (Espárrago Llorca et al., 2015). However, the precise period within which PSD develops during this 3-month window remains to be determined, and no previous studies have examined PSD rates within 2 weeks of stroke onset. Furthermore, PSD is the main factor that limits patient recovery and rehabilitation, thereby increasing morbidity and mortality. However, the precise mechanisms underlying the development of PSD remain unknown, along with the most appropriate methods for evaluation and treatment (Gaete and Bogousslavsky, 2008).
Methods
Patients
The present study included 88 inpatients (56 men; mean age ± standard deviation: 72.7 ± 11.9 years) with stroke that were admitted to Nagasaki University Hospital between May 2017 and June 2018. The average duration of admission among these 88 patients was 18.65 ± 5.95 days. At the beginning of rehabilitation, we assessed cognitive function using the 11-item Mini-Mental State Examination (MMSE). We excluded inpatients with severe aphasia and higher brain function, based on an MMSE score of <23 points, in consultation with their attending neurologist. Further, we investigated the patient’s drug history and medical records related to depression, and excluded those with depression. In the included patient sample, 42 cases of stroke occurred on the left side, and 46 occurred on the right side. The sample included 66 patients with cerebral infarction and 22 patients with cerebral haemorrhage (Table 1).
Demographic and clinical features of the stroke group (n = 88).
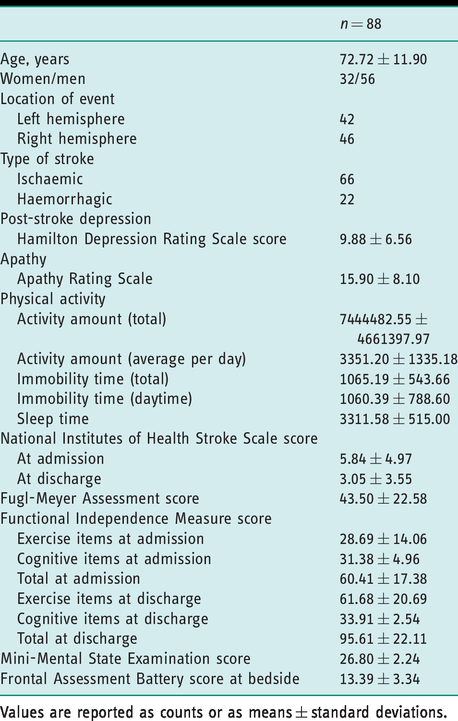
Values are reported as counts or as means ± standard deviations.
This study was approved by the local ethics committee (2016). All experimental procedures were conducted in accordance with the Declaration of Helsinki. All included patients provided written informed consent prior to participation in the study.
Measures
Patient data was collected, including age, sex, stroke side, and stroke type. Patients were classified into a PSD and a non-PSD group using the Hamilton Depression Rating Scale (HAMD) (Carod-Artal, 2006). In addition, to examine the factors associated with PSD, we evaluated stroke severity, upper limb function, ADL ability, frontal lobe/cognitive function, and levels of apathy. We also measured activity levels using a GT9X Link system (ActiGraph, Pensacola, Florida, USA). All assessments were conducted within 2 weeks after admission.
Patients completed the 17-item HAMD within 1 week from the time they were able to leave their bed. Total HAMD scores range from 0 to 53 points and are categorised as follows: ≥23 points (most severe), 19–22 points (severe), 14–18 points (moderate), 8–13 points (mild), and ≤7 points (no depression).
Patients also completed the 11-item National Institutes of Health Stroke Scale (NIHSS) to determine the severity of stroke at the time of admission and discharge. Total scores range from 0 to 42 points, with higher scores indicative of more serious impairment.
Upper limb paralysis was assessed at the beginning of rehabilitation using the relevant items of the Fugl-Meyer Assessment (FMA). The FMA consists of five items for each of the upper and lower limbs: motor function, sensory function, balance function, range of joint motion, and arthralgia. Scores for the shoulder, elbow, forearm, wrist, hand/finger, and cooperation of upper extremities range from 0 to 2 points. Total scores range from 0 to 66 points, with lower scores indicative of more serious impairment.
ADL abilities were assessed at admission and discharge using an 18-item Functional Independence Measure (FIM). The FIM contains 13 items related to exercise and five items related to cognitive function. Item scores range from 1 to 7 points, with total scores ranging from 18 to 126 points. Lower FIM scores are indicative of more serious impairment.
Frontal lobe function was assessed at the beginning of rehabilitation using the six-item Frontal Assessment Battery (FAB). Items are scored from 0 to 3 points, with total scores ranging from 0 to 18 points. Lower FAB scores are indicative of more serious impairment.
Apathy alone may occur in 29.5%–40.2% of patients following stroke, making it easy to confuse it with PSD (van Dalen et al., 2013). Because both apathy and PSD can result in reduced physical function and ADL abilities, we used the 14-item Apathy Rating Scale (ARS) to evaluate levels of apathy within 1 week from the day the patients were able to leave their beds. Total ARS scores range from 0 to 42 points, with scores of 16 points or more considered indicative of apathy.
Levels of physical activity were assessed using an ActiGraph GT9X Link wrist-worn activity meter (ActiGraph, Florida, USA), which integrated and measured all accelerations that occurred using a three-axis accelerometer. The amount of physical activity recorded by the activity meter was quantified as an arbitrary acceleration integration unit, specific to the ActiGraph GT9X Link, called an ‘activity count’. Several previous studies have reported that this waterproof device is highly reliable for measuring levels of physical activity (O’Dwyer et al., 2014). With three-axis solid state acceleration, it can measure continuous data for a battery life of approximately 14 days. Measurements of physical activity began within 1 week from the day the patients were able to leave their beds. We measured the total amount of physical activity for each week, the average amount of physical activity for each day, total immobility time during the week, average immobility time during the day, and time spent sleeping during the week.
Statistical analysis
Based on the results of the HAMD, patients were divided into two groups, a PSD group and a non-PSD group, and analysed. We examined correlation in sex, age, stroke type, stroke side, physical activity levels, immobility time, NIHSS scores at admission and discharge, FMA scores, FIM scores at admission and discharge, and MMSE scores between the two groups using Mann–Whitney U-tests (univariate analysis). Next, to avoid the influence of multiple collinearity, we performed Spearman’s rank correlation analysis to evaluate items exhibiting significant associations in the univariate analysis. We then extracted independent variables from the evaluated items, and performed logistic regression analysis using the stepwise variable reduction method, with PSD as the dependent variable.
All statistical analyses were performed using SPSS version 22.0 (IBM, USA). The level of statistical significance was set at p < 0.05.
Results
Among the 88 included patients, there were 71 cases of cerebral infarction and 17 cases of cerebral haemorrhage. The PSD group included 49 patients (55.7%; 29 men), with an average age of 74.0 ± 12.9 years and an average hospital stay of 18.90 ± 5.07 days. Among these 49 patients, there were 37 cases of cerebral infarction and 12 cases of cerebral haemorrhage. The non-PSD group included 39 patients (44.3%; 27 men), with an average age of 71.1 ± 10.4 years and an average hospital stay of 18.33 ± 6.96 days. Among these 39 patients, there were 34 cases of cerebral infarction and five cases of cerebral haemorrhage.
The PSD and non-PSD groups exhibited significant differences in NIHSS scores at admission (p = 0.002), NIHSS scores at discharge (p = 0.009), FIM exercise items at admission (p = 0.001), FIM cognitive items at admission (p = 0.002), total FIM items at admission (p = 0.0001), FMA scores (p = 0.001), and ARS scores (p = 0.031) (Table 2). NIHSS scores, ADL abilities, upper limb functions, and ARS scores indicated that impairments were more severe in the PSD group than in the non-PSD group.
Comparison of outcome measures between the PSD and non-PSD group.
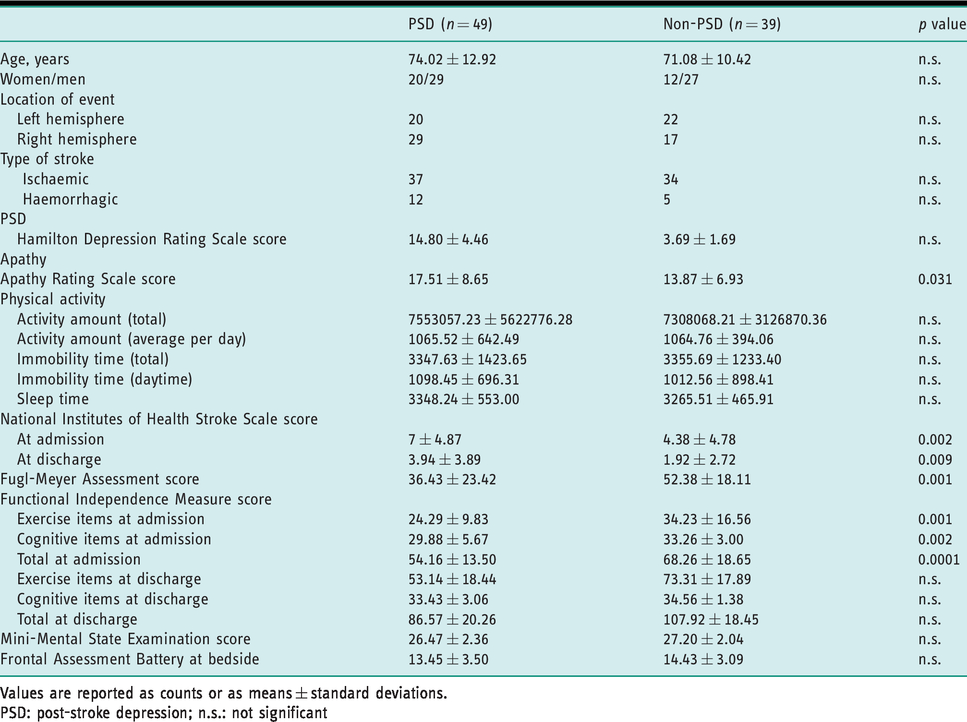
Values are reported as counts or as means ± standard deviations.
PSD: post-stroke depression; n.s.: not significant
In addition to NIHSS scores at admission, NIHSS scores at discharge, FMA scores, and ARS scores, we adopted the total amount of physical activity for 1 week and the average amount of physical activity for 1 day as explanatory variables. Although the PSD and non-PSD groups exhibited significant differences in FIM scores, there was a strong correlation between the FIM and the non-PSD group. Because logistic regression revealed multicollinearity, FIM was excluded from the explanatory variables. Based on the results of our analysis, we adopted the FMA score (p = 0.004, Exp = 3.780) as a significant variable (Table 3).
Odds ratios for post-stroke depression in patients with acute stroke.
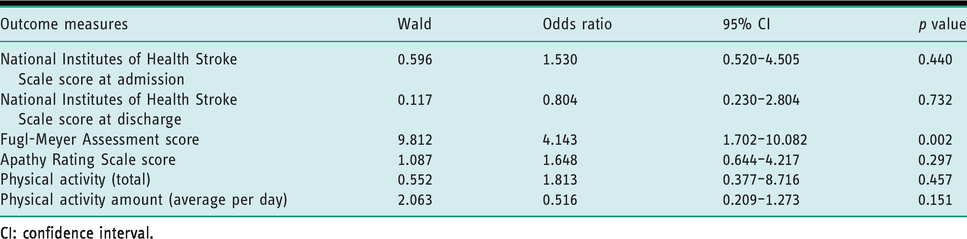
CI: confidence interval.
Discussion and implications
Incidence of PSD
In the present study, we aimed to clarify factors associated with PSD in patients with acute stroke. It is well known that PSD profoundly affects prognoses, and it is important for occupational therapists to check for the presence of PSD in the acute post-stroke phase. Previous studies in acute stroke patients have reported that the incidence of PSD between 10 and 20 days after the onset of stroke is 38% (Morrison et al., 2005), and 52% 3 weeks after the onset of stroke (Nys et al., 2005). One month after the onset of stroke, the incidence of PSD has been reported as 33% (Hackett et al., 2005), and this is reduced to 18% 2–4 months after the onset of stroke (Kim and Choi-Kwon, 2000). In our study, the incidence of PSD was 55.7%, evaluated within 2 weeks after the onset of stroke. Therefore, these results suggest that PSD is more likely to occur near the onset of stroke.
In contrast, high incidence of PSD has been reported even in the chronic phase (1–2 years after onset) (Arwert et al., 2018). Such findings suggest the involvement of psychosocial factors such as physical changes, psychological stress after the onset of stroke, and anxiety regarding future life (Ayerbe et al., 2013). As described above, there are various causes of PSD; its occurrence is considered to fluctuate. We suggest that the strong psychological stress caused by the onset of stroke might increase the incidence of PSD in the acute phase.
Factors related to PSD
In the present study, we aimed to clarify factors influencing PSD within 2 weeks of stroke onset. The PSD and non-PSD groups exhibited significant differences in FMA scores, NIHSS scores at admission, NIHSS scores at discharge, FIM exercise items at admission, FIM recognition items at admission, FIM total items at admission, and ARS scores. In accordance with our findings, previous studies have reported that the risk of PSD increases along with the severity of stroke (Tieges et al., 2015). We also observed significant differences in upper limb function as measured using the FMA, similar to findings described by Desrosiers et al. (2006), who also reported that upper limb function is a long-term predictor of participation in rehabilitation following stroke.
Severe upper limb paralysis not only affects ADL ability, but has also been associated with PSD. In accordance with the findings of previous studies, our results indicate that PSD influences the recovery of ADL abilities (Amaricai and Poenaru, 2016). Taken together, these findings suggest that PSD risk is influenced by the severity of stroke, the degree of paralysis, and decreases in ADL ability. However, we observed no significant differences in FIM scores at discharge between the groups, suggesting that ADL exert a greater effect on PSD at the time of admission.
Many previous studies have reported that female sex and older age are risk factors for PSD, and that morbidity rates are higher among older adults (Lökk and Delbari, 2010). However, in this study there were no significant differences in sex or age between groups, suggesting that factors other than sex or age exert a greater effect on PSD within the first 2 weeks after stroke onset. In addition, many older adults are not diagnosed with PSD because stroke and older age are considered to represent the cause of symptoms (Dafer et al., 2008), and 50%–80% of all patients with PSD do not receive relevant treatment (Robinson and Jorge, 2016). Therefore, it is important to clarify factors other than age and sex that influence PSD during the period immediately after stroke onset. To identify these factors, we performed a logistic regression analysis using the HAMD score as the dependent variable. This analysis identified the FMA score as a significant explanatory variable, suggesting that stroke severity and levels of physical functioning are major contributors in the development of PSD.
Previous studies have categorised PSD into organic and secondary forms. In patients with stroke, the frontal pole of the left hemisphere is strongly related to the frequency and severity of PSD (Shimoda and Robinson, 1999). However, in a meta-analysis conducted by Carsonn and MacHale (2000), the authors reported no association between the lesion or disease side and the risk of developing PSD. The relationship between such lesions and PSD remains to be fully elucidated, along with other relevant organic factors (Bhogal et al., 2004). Although we did not directly investigate the causative lesions, we observed no associations between FAB scores and stroke side. Therefore, although it is impossible to exclude organic factors in the development of PSD, it is likely that secondary factors were involved in the present study.
In our study, isolated apathy was observed in 44 of 88 patients (50%). Previous studies have reported that apathy interacts with PSD to influence recovery following stroke (Kim et al., 2018). Such studies have demonstrated that apathy occurs in 20%–50% of patients with stroke, and it also decreases physical function and ADL ability, similar to the findings observed in the present study (Hama et al., 2007). Among those in the PSD group, 28 patients (57.1%) exhibited apathy. Although the mechanisms underlying the development of both apathy and PSD in patients with stroke remain unclear, these results highlight the importance of evaluating PSD in the acute phase of stroke.
Although PSD is difficult to diagnose, we believe that occupational therapists should test for the presence of PSD, because it is often overlooked. It has been reported that the longer it takes to start appropriate treatment, the worse the progression of depressive disorders; improved results can be obtained by detecting and treating depressive symptoms early (de Diego-Adeliño et al., 2010). Therefore, predicting PSD early after the onset of stroke would benefit patients and enable rehabilitation professionals to adopt early intervention strategies.
Limitations
The present study has several limitations of note. First, we were required to determine the presence or absence of PSD during a single evaluation. Furthermore, although evaluations were performed within 1 week from the time participants could leave their beds, evaluation times varied among individuals. Therefore, it may be necessary to control evaluation times more strictly to improve the accuracy of PSD evaluations. In addition, to further ensure the accuracy of PSD assessments, we excluded patients with severe complications such as communication disorders or higher brain dysfunctions. In addition to decreasing the sample size, this might have led us to exclude some patients with PSD. Moreover, because this study was a cross-sectional study, we were unable to investigate the post-discharge course or PSD cases that appeared 14 days after the onset of stroke. Therefore, in the future, it will be necessary to increase the number of samples, perform follow-up evaluations of patients discharged from hospitals, and further investigate the appearance and predictors of PSD. Furthermore, we did not consider relationships between PSD and causative lesions in patients with acute stroke, and further research in this area is necessary.
Conclusion
The results of the present study demonstrate that stroke severity, paralysis, and physical function/ADL ability are associated with PSD in the acute phase. Our findings suggest that increases in the severity of physical impairment are associated with increases in PSD risk. Therefore, rehabilitation professionals should focus on identifying PSD in the early stages following stroke.
Key findings
Stroke severity, paralysis, physical dysfunction, and impairments in activities of daily living are associated with post-stroke depression. These factors can be used to predict post-stroke depression.
What the study has added
This study’s findings suggest that greater physical impairment severities are associated with increased PSD risks, and occupational therapists should use this information to help identify cases of acute-phase PSD.
Footnotes
Acknowledgements
We would like to thank the rehabilitation staff at Nagasaki University Hospital for their help in collecting data for this study, and all the patients who participated in this study.
Research ethics
This study was approved by the ethics committee of Nagasaki University Hospital at 2016 (No. 16072513). All experimental procedures were conducted in accordance with the Declaration of Helsinki.
Consent
All included patients provided written informed consent prior to participation in the study.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship
WM, TH, TM, MK, YH, MO, HS, and AT conceived and planned the study design. WM, TM, YH, YT, HS, and AT carried out the study. WM, YT, HS, and AT contributed to sample preparation. WM, TH, SH performed the analytic calculations and performed the numerical simulations. WM, TH, TM, SH, AT contributed to the interpretation of the results. WM, TH took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.