
Abstract
Introduction
This study aimed to investigate the effect of play-based occupational therapy on symptoms and participation in daily life activities in hospitalized children with cancer undergoing chemotherapy.
Method
A total of 25 children (mean age = 9.28 ± 0.95 years, range = 7–12 years) with cancer undergoing chemotherapy were enrolled and randomly assigned to a play-based occupational therapy group (n = 12) or control group (n = 13). The intervention group received eight 1-hour play-based occupational therapy sessions, and the control group received traditional occupational therapy services. Participation in daily life activities, therapy-related symptoms, pain, anxiety, and fatigue were evaluated.
Results
Total mean scores of participation in daily life activities in the intervention group in the diversity of activities (p = 0.001, d = 1.39), intensity of participation (p = 0.001, d = 1.86), with whom done (p = 0.005, d = 1.22), enjoyment (p = 0.003, d = 1.33), and parents’ satisfaction (p = 0.003, d = 1.33) were significantly higher than the control group. Symptoms decreased in both groups; however, this trend had a significant difference in the intervention group for the therapy-related symptom checklist (p = 0.001, d = 1.68), pain (p = 0.001, d = 1.61), anxiety (p = 0.001, d = 1.58), and fatigue (p = 0.002, d = 1.39) scores.
Conclusion
A 2-week course of inpatient play-based occupational therapy is an effective approach in the reduction of cancer symptoms, therapy-related symptoms, and the participation facilitation, of children with cancer in daily life activities.
Introduction
Diagnosis of a life-threatening illness such as cancer can be a devastating event for both the child and the family. Children facing such conditions potentially experience a prolonged period of treatment, including multiple visits and hospitalizations (Compas et al., 2012). In addition to the unpleasant symptoms of the disease, the invasive, painful, and stressful nature of the treatment process, with numerous side effects, can affect the physical, emotional, and psychosocial functioning of the child. Facing such a situation can manifest both short-term and long-term problems, including sleep disorders, aggression, depression, anxiety, developmental delay, lower quality of life, disruptions in daily life activities, and limited physical, emotional, social, and school functions (Noll et al., 1999). In addition, children with cancer experience challenges in their daily occupational performance, including self-care, productivity, and play/leisure time, which indicates the need for rehabilitation interventions, particularly occupational therapy, to reduce the current challenges and improve the quality of life of such patients (Gharebaghy et al., 2018).
Play is the most important occupation of childhood. Play and playfulness are basic needs for the child to satisfy his/her internal need for participating in activities and facilitating different aspects of growth and development (Lynch and Moore, 2016). Play is a child’s whole world, and they need to play even when they are sick (Koukourikos et al., 2015). Interventions such as play therapy have been used to help children with cancer in order to better adapt to disease conditions, long-term treatments, multiple hospitalizations, and psychological problems. Previous studies have shown the effectiveness of different types of play therapy in children with chronic health conditions, such as cancer. Play therapy, through the fun and enjoyable nature of play and the therapeutic interaction between the child and therapist, encourages distraction, creates a sense of control over the situation, helps the child to express emotions, reduces the child’s tension, helps the child adapt better to the hospital environment, helps the child to cope with physical and psychological symptoms, and allows the child to accept the reality of their condition.
Occupational therapy interventions focus on meaningful activities in special contexts that can influence the physical, mental, emotional, and social abilities of clients. Pediatric occupational therapists can use/direct play to help children with cancer to reduce symptoms and improve their abilities (Huri, 2017). Occupational therapists have a unique perspective of play: play as a means (used to achieve other developmental goals) and play as an end (undertaken for its own sake). Indeed, the term “play-based occupational therapy” means the use of play to develop basic skills and abilities, facilitating playfulness and participation in daily life activities (Lynch and Moore, 2016; Rodger and Ziviani, 1999). However, limited studies have been conducted, as a case-study and single-subject design, on the effect of play-based occupational therapy on children with cancer (Chari et al., 2013; Mohammadi et al., 2017). The field of cancer is disregarded by occupational therapists due to its specific life-threatening conditions and barriers (Sleight and Stein Duker, 2016). The current study aimed at investigating the effect of play-based occupational therapy interventions on cancer symptoms, treatment complications, and participation in daily life activities in hospitalized children with cancer undergoing chemotherapy. It was hypothesized that the child’s engagement in his/her selective play activities (based on the child’s daily life routine in a safe environment to create the most child–environment interactions and best playful experiences) could control the therapy-related symptoms and increase participation in daily life activities of children with cancer.
Methods
Research design
The current randomized single-blind (assessors) clinical trial was conducted on patients referring to the blood and oncology department of Ali Asghar Children’s Hospital in Tehran, Iran, from March to February 2016. The eligible patients were selected by convenience sampling and randomly assigned 1:1 to the intervention or the control group. The allocation was done by an independent biostatistician based on a computer-generated table of random numbers.
Participants
A total of 25 children with cancer undergoing chemotherapy were enrolled in the study (see Figure 1). The inclusion criteria were age 7–12 years, receiving a type of childhood cancer diagnosis, a history of chemotherapy in hospital, readmission to the oncology department for chemotherapy, obtaining a minimum score of 4 in pain and fatigue and 3 in anxiety for children, as well as parents’ reading and writing ability and fluency in speaking Persian. The exclusion criteria were any changes in the chemotherapy protocol and unwillingness to cooperate with the study for more than two treatment sessions.
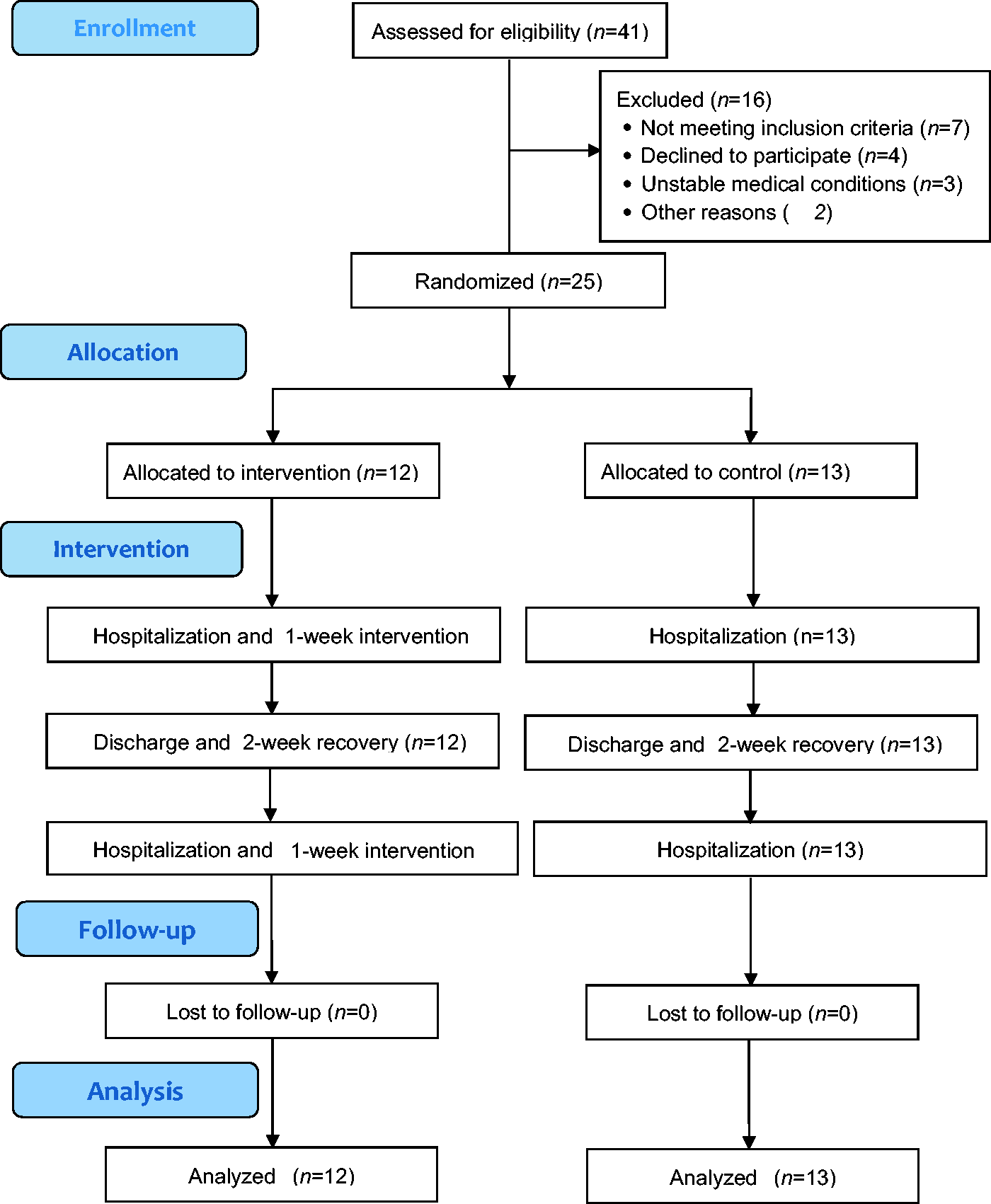
Flow diagram of the study.
Intervention
Given that the target group in the study was those children with cancer undergoing chemotherapy, based on the Berlin-Frankfurt-Munster (BFM) protocol, a play-based occupational therapy intervention was designed. According to this protocol, the hospitalized child receives chemotherapy drugs for 1 week and then takes a break for 2 weeks after discharge. This is continued until therapeutic goals are achieved. Accordingly, the play-based occupational therapy in the intervention group consisted of eight 1-hour sessions, corresponding to two 1-week hospitalization courses, on 4 consecutive days of a week (days 2–5 of hospitalization). In both the intervention and control groups, traditional inpatient occupational therapy services (positioning, transfer and mobility, range of motion, strengthening, and splinting) were provided upon the request of the pediatric oncologist by a different occupational therapist not involved in the study.
The sessions included 45 minutes of play-based occupational therapy and 15 minutes of free play. The play-based interventions were designed based on information extracted from interviews with parents using the Takata play history (Takata, 1969). A total of eight play activities were selected based on the child’s preferences and therapeutic goals (reducing symptoms and facilitating participation in daily life activities). Based on the interview results, a total of eight further common play activities were selected by the author to be used beside preferred plays if needed. The child chose one or two play activities in each session, and the therapist also indirectly participated in the play activities as a playmate, considering the therapeutic goals. At the beginning and the end of each session, the child shared his/her experiences of the previous and current day and the therapist gave feedback to the child. It should be noted that in the first week of the intervention (sessions 1–4) the focus was more on reducing symptoms (for example training in coping strategies or relaxation techniques during the presence of pain or anxiety through play), and in the second week (sessions 5–8) the focus was more on improving the child’s participation (for example training in adaptation strategies to improve self-care skills or participate in leisure activities during hospitalization and/or at home through play).
The play-based intervention took place in a consistent playroom (4 m×5 m) in the oncology ward with adequate space, toys, and materials to support the child’s play. The materials included a doctor kit, building blocks, a sandbox, clay, dress-up clothes, ball games, weapons, vehicles, books, crayons, colored pencils, markers, a whiteboard, a doll family, a dollhouse, and puppets. The same toys were present during all treatment sessions. The children were allowed to choose the play materials and activities.
A training session with parents was held on the last day of the first week, before the discharge of the child, to continue treatment at home. An educational pamphlet was also provided for the parents to continue the agreed play activities (at least 1 hour per day) during the 2-week break. Before the start of the second week, parents reported on the child’s play process at home.
Instruments
The main evaluations consisted of the therapy-related symptoms and participation of the child in daily life activities. Secondary evaluations included pain, anxiety, and fatigue.
The therapy-related symptom checklist (TRSC) includes 30 items categorized into seven groups of symptoms, including nutritional, psychosocial, oropharyngeal, toxicity of bone marrow, skin, nervous system, and respiratory system symptoms. The checklist is designed for children aged 5 to 17 years and evaluates the outcomes of chemotherapy based on a five-point scale (from 0 = asymptomatic to 4 = very severe symptoms). The TRSC is a reliable (internal consistency: Cronbach’s alpha = 0.83) and valid (content validity index (CVI) = 1.00) scale for children with cancer, and its comprehensiveness and face validity is considered to be appropriate (Mansouri et al., 2017; Williams et al., 2012).
The Children Participation Assessment Scale (CPAS) is a 71-item questionnaire used to assess the participation of children in eight areas of basic and instrumental daily life activities, play, leisure, social participation, education, work, and sleep/rest. This tool examines the daily life activities of the child in the five domains of the diversity of activities, intensity of participation, with whom done, level of enjoyment, and level of parents’ satisfaction. The scale is designed for children aged 6 to 12 years and is available in two child and parent versions. In order to collect information on participation, Children Participation Assessment Scale-parent version (CPAS-P) was used. The CPAS-P is a reliable (inter-rater reliability: ICC = 0.87–0.91, test–retest reliability: ICC = 0.97–0.99) and valid (CVI ≥ 0.88) scale for children with cancer (Amini et al., 2015).
The Wong–Baker faces pain rating scale (FPS) is designed for children over 3 years old and includes graphic and numeric parts. The numeric scale is a 10cm line: the greater the number, the more severe the pain. The graphic scale has six cartoon faces, each showing a degree of pain intensity. The left image indicates “no pain” and the right image indicates the “worst possible pain.” The Wong–Baker Faces Pain Scale has been extensively studied, and its reliability (test–retest reliability: r = 0.90, Cronbach’s a = 0.93) and validity (concurrent validity with visual analogue scale: r = 0.74–0.78) have been confirmed in children aged 3 to 18 years (Tomlinson et al., 2010).
The visual analog scale – fatigue (VAS-F) also consists of a numeric part (10cm linear scale) with five cartoon faces measuring the level of fatigue from “I am not tired at all” (0) to “I am totally exhausted” (10) in children over 7 years old. The VAS-F is a valid (convergent validity with Rhoten Fatigue Scale: r = 0.80) and reliable (internal consistency: ICC = 0.88) measure (Khoshknabi et al., 2011; Mahdizadeh et al., 2017).
The faces anxiety scale (FAS) is designed for children aged 6–12 years and consists of five cartoon faces measuring the level of anxiety and stress in the child from 1 (no anxiety) to 5 (very severe anxiety). The reliability and validity of VAS-F have been reported in previous studies (Buchanan and Niven, 2002; Quiles et al., 2013; Schlegelmilch et al., 2019).
Takata’s play history is a semi-structured interview conducted with the child’s parents. It evaluates the interests, experiences, and play opportunities in four areas of play, including materials, actions, playmates, and the time/place. This instrument is usually used as an intervention guideline in research and clinical practice. The qualitative data from the play history were used to understand the participants’ play characteristics to plan the intervention sessions (Takata, 1969).
After obtaining written consent for participation in the study and performing random allocation, the demographic information of the children and their parents, including age, gender, education level, occupational status, and diagnostic/therapeutic information, were collected. The demographic form and children’s participation assessment scale were completed with parents in a 1-hour interview session at the time of the first admission. Furthermore, therapy-related symptom checklist, pain, anxiety, and fatigue data were obtained from the children in a half-hour session in a playroom after the first admission (first day of hospitalization). This session was to familiarize the child with the therapist and playroom, as well as to gather data.
Assessments of TRSC, pain, anxiety, and fatigue were done four times (before and after each phase). Assessment of CPAS was done three times (before the first and second phase, and 2 weeks after the second phase). The reason for different CPAS assessment times was related to the nature of the tool. Given that the CPAS evaluates participation in daily life activities, the child needs to be at home for at least 1 week for the evaluation results to be valid and interpretable. All the outcome measures were assessed by a different occupational therapist who was blind to the study groups.
Statistical analysis
The optimum sample size was considered to be 10 in each group, according to the study by Williams et al. (2015) (results of therapy-related symptoms checklist, type 1 error 5%, and type 2 error 20%). With a 20% probability of dropouts, the sample size was set at 12 in each group. It should be noted that all participants completed the study, and there was no need to analyze intention-to-treat and use the per-protocol analysis.
Data analysis was performed using SPSS version 18; the significance level was 0.05. In the descriptive statistics, central tendency and dispersion indices were used. The independent T-test was used to analyze the quantitative data and the mean and standard deviation, as well as to assess their homogeneity. The chi-squared test was used to analyze the qualitative data, frequency, and percentage, as well as to assess their homogeneity. The normal distribution of the data was assessed using the Kolmogorov–Smirnov test (p > 0.005). The effect sizes were calculated based on the Cohen’s d for intergroup comparisons (0.2 as small, 0.5 as medium, and 0.8 as large) and partial eta squared for intragroup comparisons (0.02 as small, 0.13 as medium, and 0.26 as large). In the statistical analyses, to assess the efficacy of treatment and compare the results of each group in term of participation in daily life activities (3 time points × 2 groups), besides therapy-related symptoms, pain, anxiety, and fatigue (4 time points × 2 groups), the repeated measures analysis of variance (ANOVA), Bonferroni post-hoc test, and independent T-test in each time point were used. The children’s symptoms on each scale of TRSC, FPS, FAS, and VAS-F were compared for the two groups using a repeated measure ANOVA with time (T1: before week 1 (baseline); T2: immediately after week 1; T3: before week 2; T4: immediately after week 2) as the within-subjects effects and group (intervention/control) as the between-subjects effects. The children’s participation on each subscale of CPAS was compared for the two groups using a repeated measure ANOVA with time (T1: before week 1 (baseline); T2: before week 2; T3: 2 weeks after week 2) as the within-subjects effects and group (intervention/control) as the between-subjects effects.
Results
Of the 25 children participating in the study, 13 were assigned to the control group and 12 to the intervention group. Table 1 shows the demographic characteristics of the participants in the two groups. Data analysis indicated the normal distribution of all studied variables.
Participant characteristics.

* Mean (SD).
Tables 2 and 3 compare the results of participation and symptoms within and between the two groups to evaluate the main effects of time, group, and group by time interaction. The repeated measure ANOVA showed a significant effect of time on the diversity of activities, TRSC, pain, anxiety, and fatigue (p < 0.05). In other variables, the effect of time was not significant (p > 0.05). The repeated measure ANOVA also showed a significant effect of the group on the diversity of activities, intensity of participation, TRSC, pain, and anxiety (p < 0.01). The effects of group on with whom the activity was done, enjoyment, satisfaction, and fatigue were not significant (p > 0.05). The results demonstrated a significant effect of the group by time interaction on all study variables (p < 0.05). Given that the interaction between time and group was significant in all variables, independent T-testing was used to compare mean scores at each time point.
Intragroup/intergroup comparisons of participation variables.

* Mean (SD); ** Independent T-test for intergroup comparison (p-value, Cohen’s d); *** Repeated measure ANOVA for main effect of time (p-value, ηp2).
Intragroup/intergroup comparisons of symptoms variables.
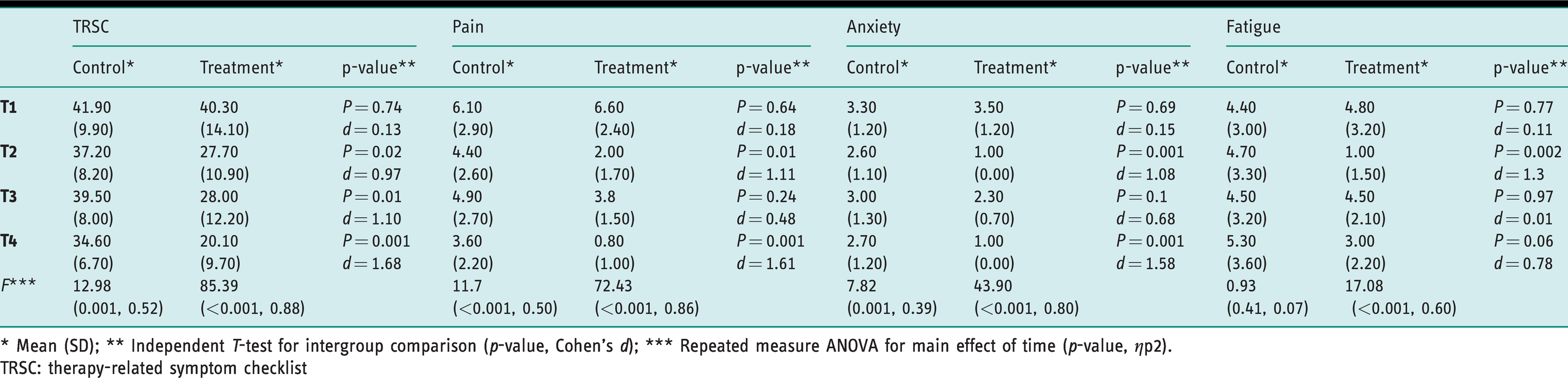
* Mean (SD); ** Independent T-test for intergroup comparison (p-value, Cohen’s d); *** Repeated measure ANOVA for main effect of time (p-value, ηp2).
TRSC: therapy-related symptom checklist
Table 2 presents the mean, standard deviation, repeated measure ANOVA, and independent T-test of the intervention and control groups at different time points for participation variables. Accordingly, an increasing trend was observed in all areas of participation in the intervention group (increased mean scores of participation); however, a decreasing trend was found in the control group (decreased mean scores of participation). Further, comparison of mean scores in the T1 and T2 time points showed no significant difference in the means of participation variables (p < 0.05); however, in the T3 time point, a significant difference was seen in diversity of activities, intensity of participation, with whom done, enjoyment, and parents’ satisfaction, with large effect sizes for all variables. Also, despite the large effect sizes in both groups, these values were higher in the intervention group than the control group.
The results of the Bonferroni post-hoc test for the intervention group for the diversity of activities and intensity of participation showed a significant difference from T1 to T3 and T2 to T3, with an increasing trend in means. The same trend was observed for the variable “with whom done” from T1 to T2 and T1 to T3. For the variables of enjoyment and parents’ satisfaction, despite the increasing trend in means, no significant difference was observed between the different time points. The results of the Bonferroni post-hoc test for the control group showed no significant differences at different time points.
Table 3 presents the mean, standard deviation, repeated measure ANOVA, and independent T-test of the intervention and control groups at different time points for each symptom variable. Accordingly, the mean scores of TRSC, pain, anxiety, and fatigue in the intervention group had a decreasing trend during the study (decreased mean scores of symptoms). This trend was also observed in the control group for all the variables, including TRSC, pain, and anxiety, except for fatigue. However, the reductions in mean scores of TRSC, pain, anxiety, and fatigue were larger in the intervention group. The comparison of mean scores of TRSC, pain, and anxiety demonstrated a significant difference at T2 and T4 time points with a large effect size; however, there was no significant difference between groups at T1 and T3 time points for TRSC, pain, and anxiety (p > 0.05). The comparison of mean scores of fatigue demonstrated a significant difference only at T2. Despite the large effect size in both groups, these values were higher in the intervention group than the control group. The only exception is the fatigue variable, which had a small effect size.
According to the results of the Bonferroni post-hoc test for the intervention group, with the exception of the T2–T3 time point, a significant difference was observed for TRSC scores among the assessment time points, and the mean scores had a decreasing trend. Regarding pain, except for T2–T4, a significant difference was observed among the assessment time points, with a decreasing trend. With regard to anxiety, a significant difference with a decreasing trend in symptoms was observed at all assessment times. However, the results for the fatigue variable were somewhat different: despite a decreasing trend, a significant difference was observed only at the T2–T3 assessment time point (P < 0.05).
Discussion
The results of the current study showed that play-based occupational therapy could effectively reduce therapy-related symptoms and control pain, anxiety, and fatigue. Several previous studies have reported the effect of various interventions on symptom control in children with cancer, but no study has been conducted on the efficacy of play-based interventions in reducing therapy-related symptoms. Chari et al. (2013) investigated the effects of play therapy on a 4-year-old girl with acute lymphoblastic leukemia (ALL). The protocol of this case study consisted of 20 30-minute sessions of non-directive play therapy, and the results showed better compliance of the subject with the disease and hospital conditions, reduced negative behaviors, and improved mental health. The authors stated that the relationship between play and distress is bi-directional such that while distress impacts play quality, play also simultaneously facilitates distress alleviation (Chari et al., 2013). This study aligned with these results in that play-based occupational therapy reduced symptoms and improved control of pain and fatigue through better distress management and disease adjustment.
The results of the current study showed that play-based occupational therapy could be effective in reducing pain, anxiety, and fatigue in hospitalized children with cancer undergoing chemotherapy. These findings are in line with those of the preliminary study by Mohammadi et al. (2017), in which two children with cancer received a play-based occupational therapy intervention within eight 1-hour sessions, and the results indicated the reduction of symptoms, including pain, anxiety, and fatigue, in the subjects (Mohammadi et al., 2017). Landier and Tse (2010) stated that complementary interventions (for example play, music, art, watching TV) accompanied by drug therapies could better reduce and manage pain in children with cancer. The results of this study showed that such interventions were effective for pain relief because they reduced the child’s focus of attention during painful therapeutic procedures and declining analgesic consumption (Landier and Tse, 2010). According to the results of the study by Scarponi and Pession (2016), group play therapy was effective in controlling the physical and psychosocial factors of pain in children who were inpatients in the oncology department (Scarponi and Pession, 2016). Anxiety, like pain, had a decreasing trend in both groups, although it was more significant in the intervention group than the control. Anxiety also decreased over time and during the treatment process. Marcus (2012) and Surbone et al. (2010) believed that these changes resulted from child compliance, the use of adaptive mechanisms, and more control over environmental conditions (Marcus, 2012; Surbone et al., 2010). It seems that the involvement of the child in a fun and purposeful activity such as play can speed up the reduction of symptoms. Furthermore, ill children usually play games that evacuate their negative emotions and help them to express and control safely unpleasant and annoying experiences. Contrary to the results of their study, Li et al. (2011) evaluated the depression and anxiety of children with cancer using virtual reality games and showed that, despite a significant decrease in depression symptoms in a 7-day therapeutic intervention, the level of anxiety had no significant difference between the intervention and control groups (Li et al., 2011). The possible reason for this lies in difficulty in determining whether children’s anxiety could be expected to respond to selected virtual games, which had a more precise effect on reducing children’s depressive symptoms, while anxiety might be less responsive to such intervention. Additionally, the results of effect size and power of study suggest that the relationship between the type of intervention and children’s anxiety were affected by the limited sample size. Another possible reason is the nature of the play used in play-based occupational therapy and video games. Most of the time, video games are competitive, with limited time and restricted control over some aspects of play. But, in play-based occupational therapy, the child, by choosing enjoyable and meaningful play, tries to progress the play and control influencing factors, which can facilitate self-control and control over the environment, features that cannot be found in video games.
The results of the current study indicated that play-based occupational therapy was effective in reducing the fatigue of hospitalized children with cancer. Diorio et al. (2015) and Jacobs (2014) reported the efficacy of complementary interventions (such as yoga, massage, biofeedback, and energy therapy) in the reduction of fatigue in patients with cancer (Diorio et al., 2015; Jacobs, 2014). However, the results of the study by Bar-sela et al. (2007) showed no significant difference between the pretest and posttest fatigue scores in children with cancer following the implementation of an art therapy intervention (despite the decreasing trend of fatigue in the intervention group) (Bar-Sela et al., 2007). It seems that the type of intervention and different changing trends in fatigue over time may explain the difference in results. Unlike therapy-related symptoms, pain, and anxiety, fatigue had an increasing trend in the control group. Evidence showed the increasing trend of fatigue over time in hospitalized children undergoing chemotherapy. Perdikaris et al. (2008) also reported the increasing trend of fatigue in 7–12-year-old children with cancer admitted to the hospital (Perdikaris et al., 2008). It seems that the administered treatments and the atmosphere of the hospital are the main causes of the obtained results.
According to the results of this study, play-based occupational therapy, due to its familiar/meaningful/goal-directed nature, increases the child’s motivation and engagement in the treatment process in addition to its therapeutic effects. It seems that playful intervention planning and goal-setting can increase the therapeutic effects of play and be a successful intervention for reducing symptoms in children with cancer (Moore and Lynch, 2018).
Moreover, the results of the current study showed that play-based occupational therapy was effective in improving the level of participation in daily life activities in hospitalized children with cancer undergoing chemotherapy. To the best of the authors’ knowledge, there has been no similar study on the effects of play-based occupational therapy on participation in daily life activities in children with cancer; however, the results were consistent with those of the study by Patil et al. (2003) concerning the effect of occupational therapy interventions on the quality of life of patients with leukemia. In their study, which mostly evaluated the neuropsychological aspects of the quality of life in 250 patients under 20 years old, the effect of interventions was examined descriptively and comparatively (Patil et al., 2003). The study by Golchin et al. (2011) also showed that training in self-care skills could improve the quality of life in children with leukemia. In their clinical trial, 488 children with ALL were provided with self-care training through question and answer sessions, as well as viewing videos and slideshows featuring children. The results of their study showed a significant improvement in the quality of life of the intervention group; however, in the control group, the quality of life decreased (Golchin et al., 2011). The results of the current study were in agreement with those of studies by Cordier et al. (2009) on the effect of play-based interventions on social play skills in children with attention deficit hyperactivity disorder (ADHD); Lo et al. (2009) on the effect of play-based interventions on self-care skills in children with autism; and Gokhale et al. (2014) on the effect of play-based occupational therapy on the playful behaviors of children with Down syndrome (Cordier et al., 2009; Gokhale et al., 2014; Lo et al., 2009).
The effect of play-based occupational therapy in improving participation can be examined from two aspects. The first is the relationship between symptoms and participation in daily life activities. Findings of descriptive cross-sectional studies by Williams et al. (2015) and Piamjariyakul et al. (2010) show a reverse relationship between the number and intensity of symptoms with a higher quality of life and self-care skills. It seems that, in the current study, reducing interfering symptoms caused by cancer diagnosis or treatment can affect the improvement of participation in daily life activities in hospitalized children with cancer. In addition to reducing symptoms, the nature of play-based occupational therapy interventions (playful goal-setting, purposeful play selection, and meaningful engagement) helps improve participation in daily life activities (Lynch and Moore, 2016; Ramugondo et al., 2018).
The study had some limitations: (a) several assessment instruments, the large number of items in the CPAS questionnaire, and the repetition of assessments at different time points could cause exhaustion and reduced accuracy in the respondents; (b) the type of assessment tools, which were mostly subjective and self-reporting with no responsiveness information (the responsiveness of the assessment tools has not been examined), increased the probability of overestimation in samples. Future studies should limit the use of objective assessment instruments to some daily life activities and/or symptoms caused by cancer and its treatment; (c) the type of disease and treatment imposed medical and health constraints on the participants so that the control of the time and number of treatment sessions, besides the environment, was challenging for the authors. In order to reduce the impact of such factors, the treatment sessions were scheduled during office hours flexibly to allow for time changes if needed; (d) it was not possible to launch a double-blind trial for both intervention and control groups, a problem common in most rehabilitation interventions. Nevertheless, the assessor-blind design was used to attempt to overcome this limitation as much as possible; (e) the small sample size due to the type and nature of the disease and its treatment protocol limits researchers when running comprehensive statistical analysis; (f) the ability to follow-up patients after the study to confirm the results and evaluate the long-term effects of interventions is advised for future studies.
Key findings
Play-based occupational therapy can be effective in increasing the level of participation in daily life activities of hospitalized children with cancer. Play-based occupational therapy can be effective in reducing therapy-related symptoms, pain, anxiety, and fatigue in hospitalized children with cancer. Eight 1-hour sessions of play-based occupational therapy can help improve the level of participation in daily life activities and reduce symptoms in hospitalized children with cancer.
What the study has added
This study confirms the effect of play-based occupational therapy in children with cancer and emphasizes the importance of using it.
Footnotes
Research ethics
The ethics committee of Iran University of Medical Sciences confirmed the study procedure (Ethic number: IR.IUMS.REC1394.9211525210).
Consent
The study purposes were explained to the participants and all of them signed the informed consent before entering the study. The authors also confirm appropriate handling of confidentiality and data security.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Iran University of Medical Sciences, Tehran, Iran.
Contributorship
All authors contributed to the initial research plan, and the methodology of the project. Dr. Mohammadi and Dr. Ansari cooperated in data gathering, and Dr. Haghani in data analysis. Also, all authors contributed in interpretation of the data, writing and editing the manuscript, and approving the final version.
Registration code for RCT:
IRCT201608829260N1