
Abstract
Introduction:
The aim of the study was to present the psychometric properties of the Turkish version of the life balance inventory in individuals with multiple sclerosis.
Methods:
Life balance inventory was translated and adapted considering common suggestions. Participants were cross-sectionally evaluated twice with life balance inventory, with a 1-week interval. Expanded Disability Status Scale, Beck Depression Scale, and Short Form-12 were used to assess the convergent validity.
Results:
A total of 113 individuals with multiple sclerosis were enrolled in the study. Test-retest reliability of the total score and all subscores of the life balance inventory were excellent (intraclass correlation coefficient > 0.80). The internal consistency of the life distress inventory was excellent (α = 0.73–0.95). The correlation of Expanded Disability Status Scale with life balance inventory and its subscores was low in the scope of divergent validity, as expected (r < 0.35). The correlation between life balance inventory total score and Expanded Disability Status Index was −0.337 (p < 0.01). Life balance inventory scores were moderately correlated (p < 0.01), except life balance inventory health score. Life balance inventory scores were correlated with SF-12 physical-subscales and mental-subscales, in a low and moderate degree, respectively. The life balance inventory total score was highly correlated with the life balance inventory subscores (r = 0.69–0.96, p < 0.01).
Conclusion:
The Turkish life balance inventory is a reliable and valid inventory in patients with multiple sclerosis. Life balance inventory comprehensively evaluates the life balance parameters of multiple sclerosis patients.
Introduction
Multiple sclerosis (MS) is an autoimmune neurodegenerative disease of the central nervous system. MS characteristically begins at the age of 20–30 and causes physical and cognitive impairments in individuals, resulting in a decrease in quality of life (McGinley et al., 2021). Accordingly, individuals with MS may have difficulties in participating in activities of daily life (Barin et al., 2018; Matuska and Erickson, 2008). If there are obstacles to participation in daily life, health and well-being are adversely affected (Matuska and Bass, 2016). The life balance structure, which includes many dimensions of life, has been described in a narrow and broad sense by different authors (Matuska and Christiansen, 2008; Pentland and McColl, 2008; Sheldon et al., 2010). Life balance is defined as “a satisfactory pattern of activity that is sustainable and meaningful in one’s living conditions.” Life balance refers to a healthy form of activity that involves the proportional use of different aspects of life (e.g., self-care, work, rest, leisure) (Wagman et al., 2011).
People with MS have reported life imbalance because of the disconnect between what they do and want to do. The presence of multiple different symptoms causes difficulties and obstacles in continuing patients’ profession (Matuska and Erickson, 2008). On the other hand, it has been found that the depressive state seen in individuals with MS is associated with less participation in recreational activities (Matuska and Erickson, 2008; Voss et al., 2002). There are several studies on life balance in the literature (Matuska, 2010; Matuska, 2012b; Matuska and Bass, 2016; Matuska and Christiansen, 2008; Matuska et al., 2013). However, studies including individuals with MS are limited. A phenomenological study addressed experiences and perceptions about lifestyle balance in individuals with MS through a focus group discussion. It was stated that the participants emphasized their desire to be physically active with minimum stress (Matuska and Erickson, 2008). The authors emphasized the importance of rewarding and stimulating activities in achieving this goal. In addition, individuals expressed their concerns about managing their energy and fatigue. Another recent qualitative study underlined the importance of physical and mental life balance for daily living activities and work life in individuals with MS (Vijayasingham et al., 2017).
In this respect, assessment tools are needed to evaluate the living habits of individuals with MS who have disabilities at different levels. In the literature, there is the Juhnke–Balkin Life Balance Inventory (JBLI) (Davis et al., 2014) consisting of 91 items, and the Life Balance Inventory (LBI) (Matuska, 2012a) consisting of 53 items in short. LBI is a self-report tool that evaluates the perceived fit between the time individuals want to spend in different activities in daily life and how much time they spend in real life (Matuska, 2012a, 2012b). Owing to LBI, it is possible to determine the activities of the individual in daily life and other activities that they want to participate. LBI is a scale consisting of four sub-dimensions: health, identity, relationship, and challenge/interest. It evaluates 53 activities (instrumental activities of daily living, education, work, play, rest, social, and leisure participation) in different fields. The American version of LBI was demonstrated to be valid and reliable (Matuska, 2012a, 2012b).
LBI was also validated in adults with obesity (Matuska and Bass, 2016), women with and without personality disorders (Larivière and Levasseur, 2016), individuals with chronic stroke (Van Gils et al., 2020), individuals with and without physical disability (Larivière and Levasseur, 2016) and young adults (Kim et al., 2018). It has been stated that the life balance related to the challenge is primarily affected in individuals with stroke (Van Gils et al., 2020). In obese individuals, it was stated that the most “health” subscore had low life balance (Matuska and Bass, 2016). This shows that the affected life balance parameter may vary in different populations. In this respect, the life balance parameter that is most affected in individuals with MS is an additional curiosity. Moreover, different language versions (Dutch, Flemish, Slovenian, and Spanish versions) were found to be valid and reliable in individuals with MS living in Europe via the European Network for Best Practice and Research in Multiple Sclerosis Rehabilitation (RIMS). It has been reported that it can be used as a supportive instrument in determining rehabilitation goals. This study observed that the challenge scores were low in Dutch and Slovenian populations, and the identity scores were low in Flemish and Spanish (Kos et al., 2020). In this respect, in our study, it will be possible to observe which dimension of life balance is most affected in individuals with MS in Turkish society. We believe that LBI will be a preferred scale among physiotherapists, occupational therapists and other rehabilitation professionals. The aim of this study is to investigate the psychometric properties of the Turkish version of LBI in individuals with MS.
Method
Translation and adaptation procedures
After obtaining permission to translate the LBI into Turkish, the adaptation process was conducted according to the international guidelines (Beaton et al., 2000; Guillemin et al., 1993). The first stage of the translation procedure was “Forward-translation.” At this stage, two researchers (physiotherapist academicians) who were native Turkish and also had excellent academic English translated the LBI separately. The second stage of the procedure includes the synthesis of the independently translated two versions in the first stage. At this stage, two translations were compared, and a single “forward translation” was obtained, which was agreed upon in terms of semantic integrity. In the third stage of the procedure, “back-translation” was carried out. A native English translator (fluent in Turkish) back-translated the LBI. In the fourth stage, an expert committee compared the original English LBI with the back-translated version. In the fifth stage, the draft version was tested with 30 randomly selected people with MS (21 women, nine men, the median age is 38) regarding comprehensibility. Individuals with MS (native Turkish speakers) who came to the neurology department were informed about the pilot study and obtained their consent. These individuals were not included in the study sample. Comprehensibility was assessed for each item on a Likert-type scale (1: very weak, 2: weak, 3: moderate, 4: good). The median value of the individuals’ comprehensibility score was 4 for all items. The participants did not report any further difficulties, and the final version of the questionnaire was created.
Sample size estimation
The calculation of the sample size was carried out with G*Power (v3, Heinrich-Heine-Universität, Düsseldorf, Germany). Based on the referenced study’s r2 value (Kos et al., 2020) was settled as effect size (0.25). Considering the 0.80 of power and 0.05 of significance level, 95 cases were required for the research (Faul et al., 2007). Another calculation was conducted for the second session of the study. “The expected intraclass correlation coefficient (ICC1)” was considered as 0.85 based on the recent psychometric analysis study of the LBI (Van Gils et al., 2020). “The minimum acceptable intraclass correlation coefficient (ICC0)” was set as 0.60, considering the relevant cut-off values. A power and significance level were accepted as 0.80 and 0.05, respectively (Bonett, 2002). Consequently, a total of 26 patients were required for the retest session.
Study design
The present study was conducted in Ege University, Department of Neurology. A total of 113 participants with MS were included in the study. MS diagnosis was conducted by a clinical neurologist regarding the revised McDonald criteria (based on the relapse history, magnetic resonance imaging and cerebrospinal fluid findings evaluation) (van der Vuurst de Vries et al., 2018). Individuals were informed about the study, and their written consent was obtained. The study protocol was approved by the ethics committee of Ege University (No: 21-5T/77). Patients who would receive routine control in the neurology outpatient clinic were included by random sampling method. The entire population was evaluated with LBI, Expanded Disability Status Index (EDSS), Short Form-12 (SF-12), Beck Depression Scale (BDS). One week later, LBI was repeated with 30 randomly selected participants from the same sample. Exclusion criteria of the research were (1) patients who had no relapse for the last 30-days, (2) bedridden patients, (3) other chronic diseases that could affect daily life, (4) cognitive deficits.
Life balance inventory
LBI is a self-report tool consisting of 53 activities from different areas of daily life (instrumental activities of daily living, work, rest, play, education, leisure, and social participation). The LBI includes four subscales: health, identity, relationship, and difficulty/interest. In the first step of LBI, individuals indicate whether they want to do the relevant activity or not. In the second step, the time spent on activities is scored: “always less than I want” (1 point), “sometimes less than I want” (2 points), “about right for me” (3 points), “sometimes more than I want” (2 points), “always more than I want” (1 point). The LBI total score is calculated by the arithmetic average of a person’s activities or wants to do. The total score ranges from 1.00 to 3.00. A higher score represents a better life balance (Kos et al., 2020; Matuska, 2012a, 2012b; Van Gils et al., 2020).
Expanded disability status scale
The EDSS is a clinician-applied assessment scale that evaluates the functional systems of the central nervous system. EDSS is used to describe disease progression in MS patients and evaluate the effectiveness of therapeutic interventions in clinical trials. The EDSS is considered the gold standard measure of disability in people with MS. It is an ordinal scale ranging from 0 (no disability) to 10 (death due to MS) (Kurtzke, 1983).
Short form-12
SF-12 is the short form of Short Form-36 (SF-36), which provides a more practical assessment with 12 items. SF-12 includes physical and mental composites. Factor analysis of the SF-36 indicated two factors: physical and mental. The scores of SF-36 based on two factors with SF-12’s physical and mental composite were highly correlated (r = 0.94 for the physical component, p < 0.001; r = 0.96 for the mental component, p < 0.001). Physical and mental dimension scores range from 0 to 100, with higher scores indicating better health (Jenkinson and Layte, 1997). SF-12 Turkish version was conducted by Soylu and Kütük. The authors of the Turkish version demonstrated the internal consistency (Cronbach’s alpha = 0.73 for the physical component, Cronbach’s alpha = 0.72 for the mental component) and the factor structure (two factors including the physical and mental component) of the Turkish SF-12 (Soylu and Kütük, 2021).
Beck depression scale
BDS evaluates the cognitive and physical symptoms of depression. It consists of 21 questions. Each question is scored between 0 and 3. It is evaluated over the total score, and a high one indicates the severity of depression. In the evaluation, 0–10 points normal; 11–16 points mild mood disorder; 17–20 points borderline clinical depression; 21–30 points moderate depression; a score of 31–40 is scored as severe depression, and over 40 points as very severe depression. The highest score is 63. Hisli demonstrated the reliability and validity of the Turkish version of the BDS. In this study, reliability was examined by item analysis and halving techniques, and the correlation coefficients were found to be r = 0.80 and r = 0.74, respectively. For validity, BDS was compared with Minnesota Multiphasic Personality Inventory, and Pearson correlation coefficient was found to be 0.50 (Hisli, 1988).
Statistical analysis
The software “SPSS for Windows v25.0” (SPSS Inc, Chicago, IL, USA) was used for the analysis. Mean values and standard deviation (SD) were presented for scale data and percentage (%) for nominal variables. Normality and homogeneity were observed with the “Kolmogorov–Smirnov” or “Shapiro Wilk” test. Cronbach’s alpha coefficient was calculated for the internal consistency of LBI. This value shows the consistency of the items of the questionnaire with each other. An alpha value of 0.80 and above represents excellent consistency (Portney and Watkins, 2009). In the test-retest reliability evaluation, two LBI evaluations performed 1 week apart were performed with the intraclass correlation coefficient (ICC). An ICC value of 0.8 and above indicates excellent reproducibility (Baumgartner and Chung, 2001).
“Spearman Correlation Coefficient” or “Pearson Correlation Coefficient” was used for construct validity regarding the normality analysis results. Correlation values below 0.35 indicate a low level, values between 035 and 0.50 indicate a moderate level, and values above 0.50 indicate a high level of correlation (Juniper et al., 1996). Construct validity was considered within the scope of convergent and divergent. The validity analysis was accomplished by comparing LBI with EDSS, BDS and SF-12. The aim was to observe the correlation of life balance with the abovementioned questionnaires with physical/psychological state and quality of life, respectively. A high (> 0.50) correlation was expected between the LBI total score and its subscores within the scope of convergent validity. In addition, since it is comprehended that LBI is not only an indicator of disability like EDSS, a low (< 0.35) correlation was expected within the scope of divergent validity. A moderate and high (> 0.35) correlation was predicted with BDS, except for the health subscore of LBI. A low (< 0.35) correlation was anticipated between BDS and LBI “health” subscore within the scope of divergent validity. It was also assumed that each parameter of SF-12’s physical and mental composite could be moderately and highly correlated with LBI (> 0.35).
Results
A total of 113 individuals with MS (40.6 ± 10.9 years, 70.8% Women, 29.2% Men) were enrolled in the study. The average MS duration of the patients was 8.7 ± 5.9. Most of the MS patients were married (60.2%) and educated in university (58.6%). 77% of the participants did not have any comorbid diseases. The demographic characteristics of the individuals with MS are presented in Table 1. The clinical assessment values of the participants are presented in Table 2. Our population’s lowest life balance subscores were challenge and identity (mean score of 1.4).
The demographic characteristics of the individuals with MS.
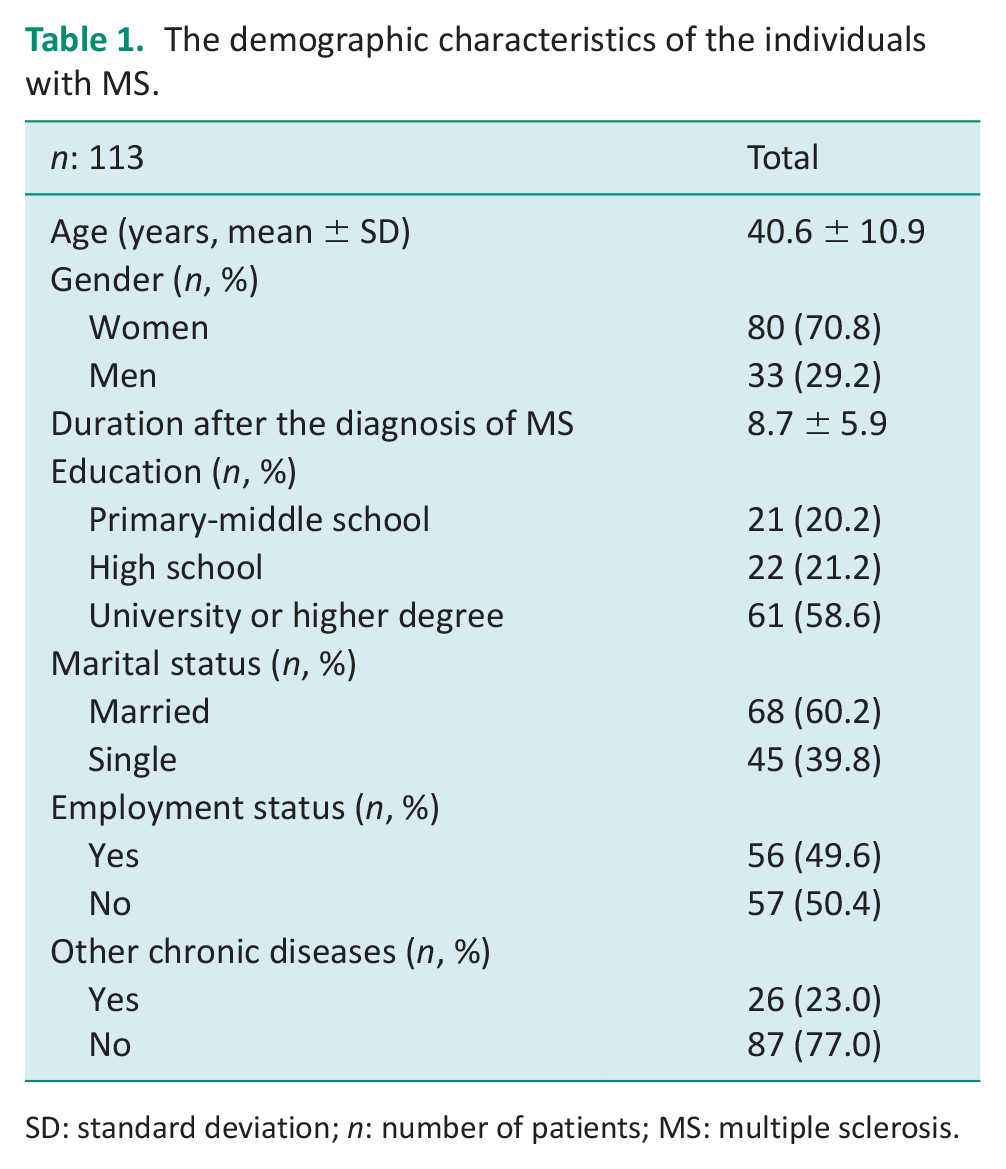
SD: standard deviation; n: number of patients; MS: multiple sclerosis.
The average values of the evaluations.
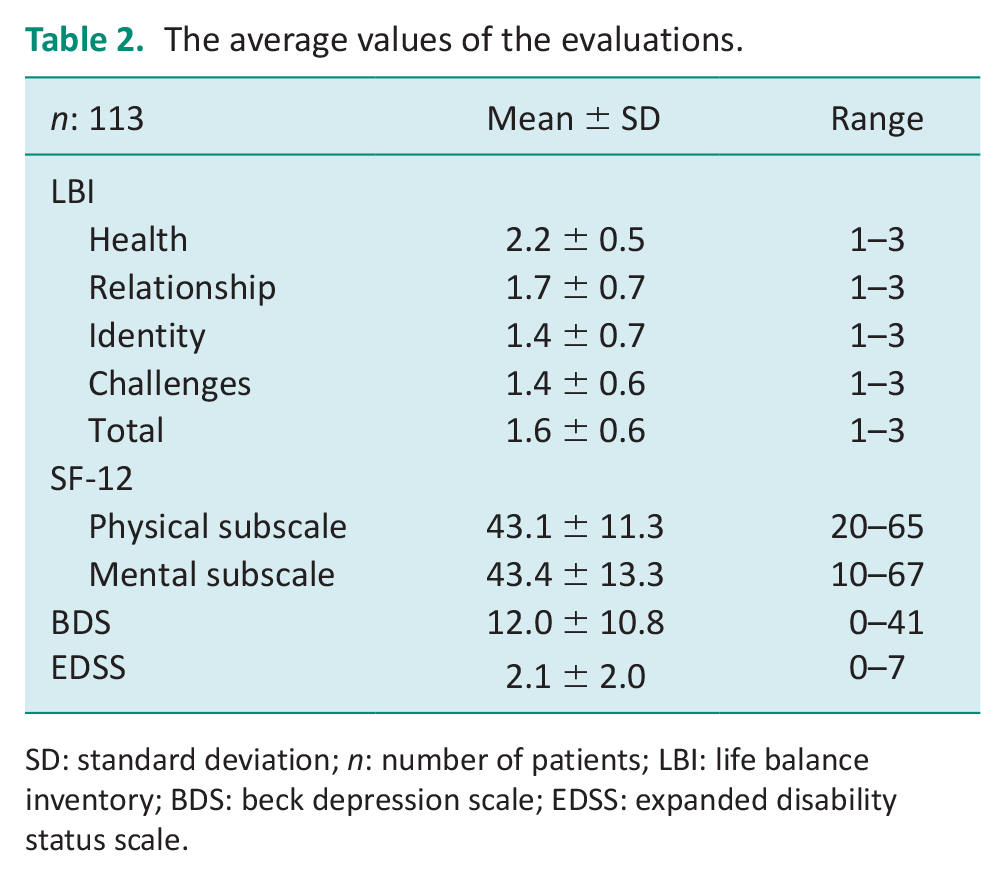
SD: standard deviation; n: number of patients; LBI: life balance inventory; BDS: beck depression scale; EDSS: expanded disability status scale.
Table 3 presents the reliability results of the LBI and its subscales. All subscores and the total score of the LBI’s alpha value were greater than 0.70. The internal consistency of the Life Distress Inventory (LDI) was excellent (α = 0.73–0.95). Test-retest reliability of the total score and all subscores of the LBI was excellent (ICC > 0.80). The ICC value of the total score of the LBI was 0.928 (CI: 0.85–0.96).
Reproducibility and consistency of the LBI.

n: number of patients; ICC: intra-class correlation coefficient; CI: confidence interval; α: Cronbach’s alpha; LBI: life balance inventory.
The construct validity was considered in terms of convergent and divergent manners. First, the relationship between clinician-based EDSS with LBI total score was low in the scope of divergent validity, as expected (r = −0.337 to −0.182). Second, LBI scores were moderately correlated in the scope of convergent validity with the BDS (r = −0.354 to −0.430), except LBI health score (r = −0.280). Third, LBI scores were lowly correlated with SF-12 physical subscales, which was not the expected result regarding our expectation in the scope of convergent validity (r = 0.211 to 0.482) (Table 4). Fourth, LBI scores were correlated with SF-12 mental subscales to a moderate degree, as expected in the scope of convergent validity (r = 0.397–0.482) (Table 4). On the other hand, the LBI total score was highly correlated with the LBI subscores, as expected in the scope of convergent validity (r = 0.69–0.96) (Table 5).
Correlation between the LBI with EDSS and BDS.
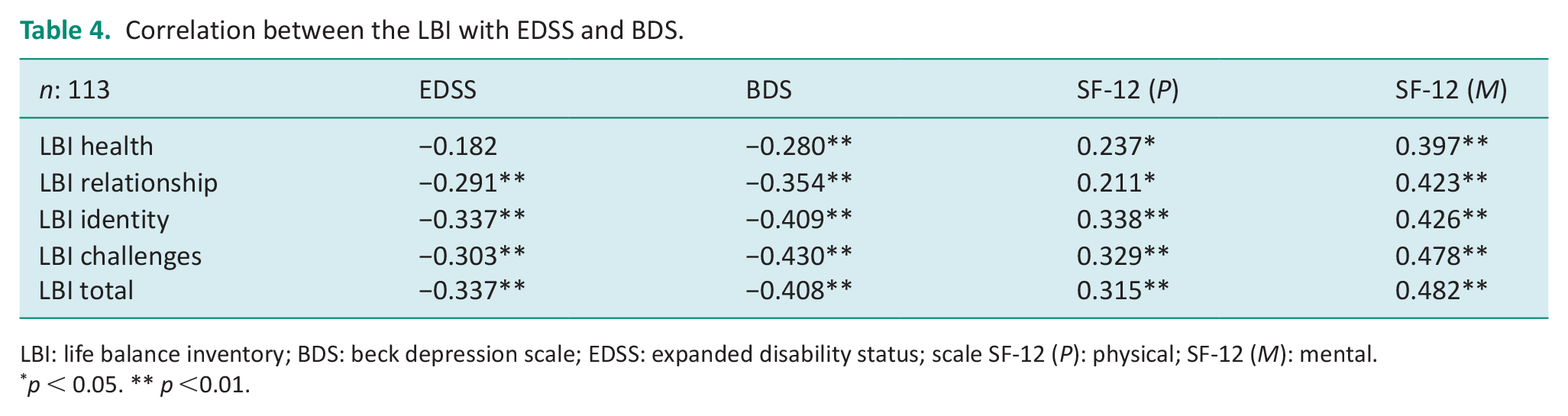
LBI: life balance inventory; BDS: beck depression scale; EDSS: expanded disability status; scale SF-12 (P): physical; SF-12 (M): mental.
p < 0.05. ** p <0.01.
Correlation between the total score of the LBI and its subscales.
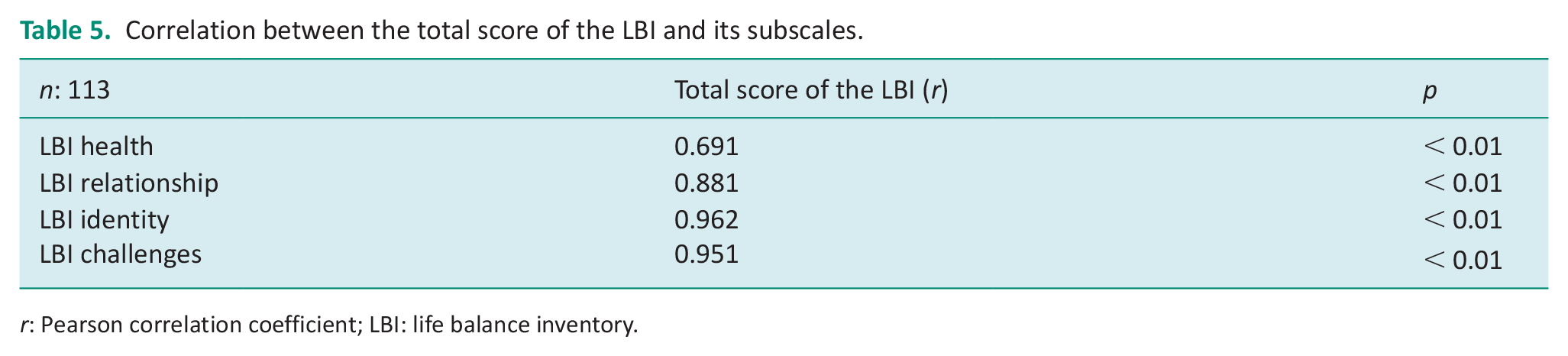
r: Pearson correlation coefficient; LBI: life balance inventory.
Discussion
The present study investigated the reliability and validity of the Turkish version of the LBI in patients with MS. The adaptation and translation conducted in terms of linguistic and grammatical specifications of Turkish (Beaton et al., 2000; Guillemin et al., 1993). Considering an international methods, test-retest reliability, internal consistency and construct validity of the LBI was analyzed (Mokkink et al., 2010). The results indicated that Turkish version of the LBI is a reliable and valid inventory to assess MS patients’ life balance. MS symptoms might affect the life conditions of the patients in terms of social relationships, individual life, several living activities, in addition to health-related quality of life. Evaluation of life balance would provide clinicians to gauge a clear understanding of patients’ well-being, therefore allowing for more targeted clinical care.
The LBI provides a comprehensive assessment that includes four subscales: health, relationship, identity, and challenge. It is known that depression, anxiety and stress are common in MS patients (Matuska, 2012a, 2012b). Since it is known that life balance disorders are associated with perceived stress levels, determining the level of LBI may be valuable in seeking ways to cope with stress in MS patients (Matuska et al., 2013). Our sample consists of individuals who work more, and it can affect the work-life balance of individuals with MS, who consist of a young and active population. As a matter of fact, one review emphasized that workaholism is a condition that affects life balance (Matuska, 2010).
The lowest life balance subscores in our population were challenge and identity. This outcome allowed us to observe more detailed outcomes of LBI in the Turkish population. Regarding the RIMS study, it was observed that life balance showed similar results in different landscapes since it was known that the Dutch and Slovenian populations had low challenge scores. The Flemish and Spanish had low identity scores (Kos et al., 2020). This outcome shows that, specifically in individuals with MS, their life balance is affected due to psychological problems. Considering the low disease durations and the low average age of the individuals, it can be deduced that physical problems do not predominantly affect their daily activities. Therefore, further focusing on psychosocial issues in individuals with MS in balance problems may be helpful.
In our study’s translation and cultural adaptation process, modifications were not required apart from grammatical changes. Comprehensibility was excellent in the pilot study. As a matter of fact, the test-retest reliability results also support the intelligibility issue. So far, three different language versions (Dutch, Korean, French) have validated the LBI, apart from the LBI development study (Kim et al., 2018; Larivière and Levasseur, 2016; Matuska, 2012a; Van Gils et al., 2020).
Flemish version examined the validity and reliability of LBI in individuals with stroke, a group of neurological cases with a high disability level (ICC = 0.88) (Van Gils et al., 2020). This value is relatively lower than our study (0.95). The fact that the mean age of our sample was approximately 40 years and 61 in stroke validation may indicate cognitive differences, and different answers may have been given in the retest. The correlation between Hospital Anxiety and Depression Scale and Flemish LBI was −0.340 (p = 0.61). Our study found the coefficient for the LBI and BDS as −0.408. Close scores clearly reveal the relationship between life balance and psychological state. This situation is supported by the fact that the SF-12 mental subscore has a higher correlation coefficient than the physical subscore in our study. It is necessary to underline the importance of the mental and psychological state in life balance.
Since the French and Korean version studies were written in the mother tongue, we could not make a detailed comparison (Kim et al., 2018; Larivière and Levasseur, 2016). In the development study, Matuska performed a psychometric analysis of LBI in adults. Matuska confirmed the internal consistency of the questionnaire with an alpha value between 0.89 and 0.97 (Matuska, 2012a). In our study, however, we encounter a relatively low internal consistency between 0.73 and 0.95. In a pathological group with specific symptoms, it may be considered natural for the questionnaire to give different responses. For example, it can be thought that the power of each item of the health subscore of the LBI to evaluate symptoms within the scope of MS life balance may not be highly consistent. However, it should be emphasized that our alpha results are within acceptable limits and that all subscores and total scores can consistently assess life balance in individuals with MS.
Our study obtained an output between LBI and EDSS following our hypothesis within the scope of divergent validity. The low correlation between LBI and its subscores and EDSS was an expected result because LBI is a comprehensive scale with both physical and psychosocial dimensions. EDSS is a gold standard tool that only provides information about disability (Kurtzke, 1983). On the other hand, there was a moderate relationship between LBI and BDS, as expected. Since many items of LBI are known to be related to psychological state, sufficient output was observed for validity in the context of convergent. LBI and SF-12 mental composite also had a similar correlational relationship in line with BDS (Hisli, 1988). However, the expected moderate correlation between SF-12 physical composite and LBI was not observed. This consequence may be due to the prominence of the psychological dimensions of LBI. In this respect, it shows that LBI can evaluate more psychological parameters in individuals with MS.
The relationship of the total score of the LBI with other subscores has also been a matter of interest. Because a holistic assessment of LBI, whether it represents health, identity, relationship and challenge subscores, may be an essential finding. The correlation analysis we conducted with this idea shows that the LBI total score is highly correlated with its subscales (r > 0.50). A value of 0.983 showed that the highest correlation was between total LBI and identity subscore. The identity subscore specifically includes individual indoor and outdoor activities. The fact that the subscore representing the life balance of MS patients is identity can be an important finding, especially for occupational therapists. The lowest correlation was found between LBI total score and health subscore (r = 0.691). The fact that the alpha value is the lowest in the health subscore of LBI (0.737), supports this finding. It is known that the health problems of MS patients are pervasive. The LBI health subscore, which covers the parameters of hygiene, health needs, nutrition, relaxation, regular exercise and adequate sleep, which are questioned in the health subscore in terms of life balance, does not include some essential conditions that affect the life balance of patients with MS. Specific evaluation of loss of strength and fatigue, especially in attack situations, could have provided higher internal consistency (Crayton and Rossman, 2006; Kister et al., 2013). As a matter of fact, the low test-retest reliability (0.4 to 0.7) and low correlation coefficients of the RIMS group do not recommend LBI in the validation study in individuals with MS, especially for international studies in the MS group (Kos et al., 2020). However, the Turkish version yielded very consistent results in the MS group. The fact that the patients in the pilot study reported no difficulties also supported our numerical results.
The limitations of the study need to be pointed out. First of all, different symptoms or frequency of attacks may vary in individuals with different types of MS. Therefore, the life balance of each individual with MS may be at a different level. Introducing an MS type or EDSS-based cut-off to the elimination criteria would have presented the study’s results more valuable. Second, it would be valuable to investigate construct validity by comparing LBI with another questionnaire assessing life balance (e.g., (JBLI)) (Davis et al., 2014). However, we did not choose the Turkish version of this questionnaire since it is not conducted with a neurological case group. We focus on depression and quality of life symptoms and not would like to burden the patients with too many questions. Finally, we could not perform the responsiveness analysis because this method included the patient monitoring period. It can be precious for establishing a reference value in the minimal clinical detectable change patient follow-up process.
Conclusions
Our study demonstrated the validity and reliability of Turkish LBI in individuals with MS. LBI: it consistently and reliably reveals the balance of life related to MS symptoms by categorically questioning several daily living activities such as health, identity, relationship, and challenge. More studies might examine psychometric analysis, especially in responsiveness, in the group with MS with a higher disability level.
Key Findings
The Turkish LBI is a reliable and valid inventory in patients with MS.
Further study should focus on the responsiveness of the Turkish LBI.
What the study has added
LBI consistently and reliably reveals the balance of life related to MS symptoms. LBI would be feasible to evaluate both the life-balance conditions of the MS patients of 100 million individuals around Turkey/Europe.
Footnotes
Acknowledgements
None.
Ethical approval
The permission for the translation for the Turkish version of Life Balance Inventory was acquired from the developer of the original questionnaire. The study was carried out in accordance with the ethical principles and the Helsinki Declaration. The study protocol was approved by the ethics committee of Ege University (No: 21-5T/77)
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was: Included at all stages of the research.
Consent
Informed consents of the patients were obtained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.