
Abstract
Childhood maltreatment is a risk factor for poor physical health outcomes in later life, such as cardiovascular disease and type 2 diabetes. In order to target preventive interventions to reduce this risk, it is important to understand the biological mechanisms linking childhood maltreatment to cardiometabolic disorders. Research reviewed here suggests that maltreated children show alterations in biological systems relating to metabolism and the immune system which could, in turn, increase the risk of long-term cardiometabolic disease risk. Specifically, maltreated children show an elevated risk of obesity in adulthood and greater inflammation levels in adolescence and adulthood. These findings from observational studies of humans are consistent with evidence from experimental animal models showing the causal effects of early life stress on obesity and immune function. To help prevent maltreated children from developing cardiometabolic disease later in life, clinical assessment and treatment should focus on physical as well as mental health.
Keywords
Introduction
It is increasingly recognised that maltreated children have an elevated risk of physical health problems later in life. For example, adults with histories of childhood maltreatment show a high prevalence of clinical outcomes, such as cardiovascular disease (Suglia, et al., 2018) and type 2 diabetes (Widom, et al., 2012). These clinical findings are also supported by experimental animal models showing that early life stress can cause indicators of cardiovascular disease in rodents (Loria, et al., 2013) and type 2 diabetes in non-human primates (Kaufman, et al., 2007). In order to understand how childhood maltreatment might affect long-term cardiometabolic risk and to inform preventive strategies, it is important to investigate whether maltreated children develop physical risk factors for later-life disease.
In this article, we review the literature to describe how exposure to childhood maltreatment could lead to pre-clinical abnormalities in metabolic and immune functioning which, in turn, might affect risk for cardiometabolic disease decades after maltreatment has ceased. A growing body of research from observational studies of humans and experimental animal models suggests that childhood maltreatment and other early life stressors are associated with obesity and elevated inflammation levels. We review this research, distinguishing between studies of adults and children to gain insight into the short- and long-term correlates of maltreatment. We also outline potential mechanisms through which maltreatment could exert effects on obesity and inflammation. Finally, we discuss the clinical implications of this emerging field of research.
Childhood maltreatment and obesity
Observational studies in humans
A number of observational studies in humans have shown that childhood maltreatment is associated with obesity (body mass index [BMI] ≥ 30 kg/m2) later in life. Indeed, a meta-analysis of 41 studies (including 190,285 participants) showed that childhood maltreatment was associated with a small but significant increase in risk of obesity (odds ratio = 1.36, 95% confidence interval = 1.26–1.47) (Danese and Tan, 2014). This association was independent of a number of potential confounders, including socio-economic status, current smoking, alcohol intake and physical activity. Sensitivity analyses showed that links between maltreatment and obesity were observed across all maltreatment types, with the exception of emotional neglect. Furthermore, the association was present in adults but not in children or adolescents. The latter finding suggested the existence of an ‘incubation period’ between exposure to childhood maltreatment and the development of obesity.
Although inference on an ‘incubation period’ was initially based on multiple cross-sectional studies in the meta-analysis, subsequent findings from longitudinal studies examining developmental trajectories of body mass in maltreated and non-maltreated children were broadly consistent with this hypothesis. For example, one study assessed children exposed to substantiated maltreatment and non-maltreated controls at four time-points across late childhood and adolescence (Schneiderman, et al., 2015). The results showed that females exposed to sexual abuse or neglect had different BMI trajectories than non-maltreated females, in that they showed lower BMI in late childhood/early adolescence and higher BMI in late adolescence. Another study tested the association between childhood maltreatment and BMI measured at seven time-points from childhood to age 50 in participants from the 1958 British birth cohort/National Child Development Study (Power, Pereira and Li, 2015). Participants with reports of physical abuse and neglect (and sexual abuse in females) showed normal BMI in childhood but faster BMI gain up to age 50 and obesity in adulthood. These associations were independent of parental BMI, prenatal/infancy factors, childhood factors, education and adult health behaviours. These findings suggest that childhood maltreatment is associated with a progressive increase in risk for obesity over the life-course.
In addition to victimisation by adults in the form of childhood maltreatment, victimisation by peers also appears to be associated with obesity. For example, children exposed to chronic bullying victimisation were more likely to be overweight in young adulthood than non-bullied ones (Baldwin, et al., 2016). This risk remained even after accounting for genetic risk of overweight, childhood weight, childhood mental health/cognition and other forms of environmental adversity. Furthermore, frequently bullied female children in the 1958 British Birth Cohort had an elevated risk of obesity at mid-life (Takizawa, et al., 2015), suggesting that, like childhood maltreatment, bullying victimisation may have long-lasting effects on obesity risk.
Experimental animal models
Animal models have provided important experimental evidence for a causal effect of early life stress on obesity in later life. Although animal models may be limited in generalisability to human experiences, biology and behaviour, these experimental studies are uniquely placed to address causal inference because they can manipulate the environment and randomly assign animals to stressful early experiences. This means that pre-existing differences between the animals exposed or not exposed to early life stress can be assumed to be equally distributed between groups, and any differences in obesity between groups can be attributed to differential exposure to early life stress. In contrast, because random assignment of human children to maltreatment is clearly unethical, observational human studies rely on statistically controlling for factors that are associated with childhood maltreatment and obesity and may thus act as confounders. However, many of these potential confounding factors are unknown or unmeasured in practice, which limits causal inference in human studies. The complementary strengths of experimental animal models and observational human studies allow confidence to be placed in findings that converge from both methods.
In animals, two studies of non-human primates have suggested that early life stress is causally associated with the development of obesity. First, Kaufman and colleagues (2007) exposed infant monkeys to early life stress in a paradigm known as variable foraging demand. This involved imposing food insecurity on their mothers for 16 weeks during nursing, which has been shown to impair maternal care and evoke stress responses in the offspring (Andrews and Rosenblum, 1994). The results showed that peripubertal primates who had been exposed to prolonged maternal food insecurity exhibited greater weight, BMI and abdominal circumference than normally reared controls. Second, Conti and colleagues (2012) carried out a study in which newborn rhesus monkeys were either reared by their mothers (the control condition) or removed from them and reared alongside their peers (the stress condition). In later life, female peer-reared monkeys exhibited greater weight than monkeys reared by their mothers. These experimental findings support evidence from observational human studies showing an association between early life stress and later obesity.
How could childhood maltreatment lead to obesity?
Childhood maltreatment and other early life stressors could increase obesity risk by giving rise to a ‘thrifty' phenotype, characterised by increased energy intake and storage and/or decreased energy expenditure (Danese and Tan, 2014). This could occur via interacting biological and behavioural mechanisms affecting energy intake and expenditure.
Childhood maltreatment and increased energy intake
Maltreated children may eat more food than non-maltreated children due to alterations in reward processing, the neuroendocrine stress system and executive function. With regard to reward processing, maltreated children show reduced sensitivity to reward, described both at a behavioural level by poorer reward-related task performance (Guyer, et al., 2006) and at the neural level by weaker activation of reward-related brain regions in the basal ganglia during reward anticipation (Mehta, et al., 2010). In turn, low reward sensitivity could result in maltreated children overeating high-calorie food in order to satisfy a reward deficit. With regard to the neuroendocrine stress system, maltreated children show chronic over-activation of the central stress response system – the Hypothalamic-Pituitary-Adrenal (HPA) axis (De Bellis, et al., 1999) and associated mental and physical symptoms of anxiety (Tarullo and Gunnar, 2006). Given that high-calorie food can reduce HPA axis activation (Pecoraro, et al., 2004) and anxiety (Prasad and Prasad, 1996), maltreated individuals may ‘self-medicate’ with high-calorie food. With regard to executive function, maltreated children show impulsivity and impairments in inhibitory control (Guyer, et al., 2006) which might arise due to smaller volume of the prefrontal cortex, a brain region involved in these functions (Lim, Radua and Rubia, 2014). In turn, poor inhibitory control over food intake could result in maltreated individuals overeating (Wonderlich, et al., 2001). These proposed mechanisms are consistent with evidence linking childhood maltreatment to excessive eating (Tarren-Sweeney, 2006) and clinical disorders involving overeating, such as food addiction (Mason, et al., 2013) and binge eating disorder (Striegel-Moore, et al., 2002).
Childhood maltreatment and decreased energy expenditure
In addition to increased energy intake, maltreated children may have decreased energy expenditure due to alterations in metabolic hormones, mental health problems and abnormal immune functioning. With regard to metabolic hormones, initial evidence suggests that childhood maltreatment and other early life stressors are associated with low basal and stimulated levels of leptin (Danese, et al., 2014; Panagiotaropoulos, et al., 2004). Given that leptin promotes lipolysis (the breakdown of fat into energy), leptin deficiency in maltreated children could reduce energy expended through this basal metabolic process. With regard to mental health problems, maltreated children have an elevated risk of developing depression (Widom, DuMont and Czaja, 2007) which is associated with physical inactivity. Therefore, children exposed to maltreatment might engage in less exercise due to depression. With regard to the immune system, as is discussed later in this review, maltreated children are at risk of developing high inflammation levels (Danese, et al., 2007). Because inflammation can induce fatigue (Dantzer, et al., 2008), high levels could result in maltreated individuals being less physically active. The latter two mechanisms are consistent with evidence showing that adults with a history of childhood maltreatment report engaging in less physical activity than non-maltreated individuals (Power, Pereira and Li, 2015).
Taken together, these findings suggest that childhood maltreatment may increase risk of obesity in adult life via plausible (but largely untested) biological and behavioural mechanisms. In turn, elevated rates of obesity in individuals with a history of childhood maltreatment could at least partly contribute to their increased risk of later cardiometabolic disease.
Childhood maltreatment and inflammation
Observational studies in humans
Inflammation is part of the innate immune response to infection and physical injury. Although timely activation of the inflammatory response is a vital defensive mechanism, the inflammatory response is non-specific and can also mistakenly target parts of the body and cause damage when chronically activated. Evidence suggests that childhood maltreatment is associated with chronic low-grade inflammation, as reflected in high levels of inflammation biomarkers, such as the acute phase protein C-reactive protein (CRP) and pro-inflammatory cytokines like tumour necrosis factor alpha (TNF-α) and interleukin 6 (IL-6). For example, children exposed to maternal rejection, harsh discipline, disruptive caregiver changes, physical abuse or sexual abuse showed higher levels of CRP than non-maltreated children at age 32 (Danese, et al., 2007). This association also generalised to other inflammation biomarkers such as fibrinogen and white blood cell count. Furthermore, the association was independent of the influence of low birth weight, childhood family socio-economic disadvantage and low IQ. Since these initial findings, more than two dozen studies have investigated the association between childhood maltreatment and inflammation in adulthood, with qualitative and quantitative reviews showing that adults with histories of childhood maltreatment have a small elevation in CRP, TNF-α and IL-6 (Baumeister, et al., 2015; Danese and Baldwin, 2017). These long-term effects of maltreatment have generalised to other forms of early life stress, such as bullying victimisation, which also predict high inflammation levels in midlife (Takizawa, et al., 2015).
To understand the emergence of the effect of childhood maltreatment on cardiometabolic disease risk, studies have also examined whether maltreated children already showed high inflammation levels in early life. Evidence suggests that childhood maltreatment is associated with a very small elevation in inflammation levels in young people (Kuhlman, et al., 2019), though effects can vary according to differing methodological approaches, co-occurring psychopathology or gender. For example, maltreated children with depression showed elevated CRP levels at age 12, compared to non-maltreated children matched for sex, socio-economic status and zygosity (Danese, et al., 2011). Furthermore, children exposed to multiple victimisation types (including physical abuse, sexual abuse, emotional abuse and neglect, physical neglect, domestic violence and bullying victimisation) showed elevated levels of CRP at age 18 (Baldwin, et al., 2018). Notably, this association was present only in females and not in males. In females, the association was independent of genetic risk for inflammation, socio-economic disadvantage, obesity and body temperature. Consistent with findings in adults, these results linking childhood maltreatment to inflammation in young people also generalise to other forms of victimisation: for example, children exposed to cumulative bullying victimisation showed elevated CRP levels in adolescence and greater increases in CRP levels from adolescence to young adulthood (Copeland, et al., 2014).
In addition to an association between childhood maltreatment and elevated baseline inflammation levels, maltreated individuals also show greater pro-inflammatory responses to subsequent stressors. For example, adults with a history of childhood maltreatment showed a greater inflammatory response to an acute psychosocial stress test than non-maltreated controls (Carpenter, et al., 2010). Maltreated individuals also showed heightened inflammatory responses to daily stressors and caregiving stress in older adulthood (Gouin, et al., 2012). Furthermore, depressed adults reporting childhood maltreatment showed an elevated inflammatory response to acute stress, relative to controls (Pace, et al., 2006).
Experimental animal models
A number of experimental animal studies have investigated whether early life stress has causal effects on immune function and development. An extensive review of these studies is beyond the scope of this article but interested readers may refer to Ganguly and Brenhouse (2015). In brief, results vary according to the type of stressor and immune system measure used, though several studies have reported elevated inflammation levels in animals exposed to early maternal separation. For example, Cole and colleagues (2012) assessed inflammatory gene expression profiles of rhesus monkeys either reared maternally or removed from their mothers and reared with peers. Relative to monkeys reared by their mothers, maternally-deprived monkeys showed enhanced expression of genes involved in inflammation. This suggested that early life stress can increase inflammatory gene expression in the first few months of life in non-human primates. These findings are consistent with experimental findings from rodent studies showing that maternal separation increases inflammatory markers (O’Mahony, et al., 2009).
How could childhood maltreatment affect inflammation?
Maltreated children may develop high inflammation levels via a number of biological and behavioural mechanisms.
Biological mechanisms. At least three potential biological pathways could link childhood maltreatment to inflammation. First, maltreated children show reduced sensitivity to cortisol (a hormone with anti-inflammatory properties) which could, in turn, result in chronically elevated inflammation levels. Indeed, a longitudinal study found that female adolescents from harsh families showed decreasing sensitivity to cortisol’s anti-inflammatory properties and greater inflammatory responses to stressors over time (Miller and Chen, 2010). Similarly, adolescents exposed to early life stress showed resistance to cortisol and increased levels of inflammation biomarkers (do Prado, et al., 2017). Second, childhood maltreatment is associated with elevated risk of infections, which could impact immune development. For example, maltreated children are more likely to be exposed to infections and injury (Gilbert, et al., 2009) and may also be more susceptible to infection (Shirtcliff, Coe and Pollak, 2009). In turn, exposure to multiple infections could result in chronic inflammation. Third, childhood maltreatment could increase inflammation levels due to alterations in the microbiome. For example, early life stress in animals can cause alterations in the colonisation and composition of the gut microbiota (O'Mahony, et al., 2009). In turn, alterations in the gut microbiome during sensitive periods in early life could affect immune system development and lead to chronic inflammation (Cryan and Dinan, 2012).
Behavioural mechanisms. As well as biological pathways between childhood maltreatment and inflammation, several broader behavioural mechanisms may operate. First, disruption of sleep patterns could partly mediate the association between childhood maltreatment and high inflammation levels. Maltreated children have an elevated risk of sleep problems (Cecil, et al., 2015) and experimental studies have shown that sleep deprivation can cause increased inflammation levels (Meier-Ewert, et al., 2004). Second, obesity is likely to play a role in the association between childhood maltreatment and inflammation. As discussed, maltreated children have an elevated risk of obesity (Danese and Tan, 2014) and obesity is linked to a chronic inflammatory state due to production of pro-inflammatory cytokines by adipose (fat) tissue (Gregor and Hotamisligil, 2011). Notably, one study showed that the relationship between reports of childhood maltreatment and CRP levels in females was mediated through obesity (Matthews, et al., 2014), though other studies found that the association was independent of obesity (Baldwin, et al., 2018; Danese, et al., 2007; 2011). Third, maltreated children may develop high inflammation levels due to consuming addictive substances. Adults with histories of childhood maltreatment are particularly likely to smoke and abuse alcohol and drugs (Felitti, et al., 1998), which can increase inflammation levels. These addictive behaviours may, therefore, partly explain the high inflammation levels seen in victimised children and adolescents but may contribute to sustained high inflammation levels in adults exposed to childhood maltreatment (Danese and Baldwin, 2017).
Discussion
Maltreated children show a higher risk of developing obesity and higher inflammation levels than non-maltreated children. These effects appear to progressively emerge throughout adolescence and become established by adulthood (Baumesister, et al., 2015; Power, Pereira and Li, 2015). Because these metabolic and immune abnormalities after exposure to early life stress in humans appear to be conserved across other species with distant common ancestors (e.g. non-human primates), it is possible that excess weight and inflammation may be adaptive in the face of early life stress (Danese and Baldwin, 2017). For example, larger bodyweight could help abused children to better defend or protect themselves against violence and sexual victimisation. In addition, high levels of body fat could help ensure that neglected children have adequate energy supply during periods of malnutrition. Furthermore, high inflammation levels could accelerate wound repair and prevent infections in children with injuries from violence and infection due to unsanitary environments.
Despite these potential adaptive advantages of obesity and inflammation in the context of childhood maltreatment, when maltreated individuals escape abusive and neglectful environments and priorities shift from survival to long-term health, obesity and inflammation will become maladaptive by conferring disease risk (Danese and Baldwin, 2017). Both obesity and inflammation are major independent risk factors for cardiovascular disease (Ridker, et al., 1997) and type 2 diabetes (Reilly and Kelly, 2011). Because these clinical outcomes are more prevalent in adults with histories of childhood maltreatment, it is possible that obesity and high inflammation might help explain why childhood maltreatment is associated with increased disease risk in later life. Though future research is required to test whether obesity and inflammation mediate the effects of childhood maltreatment on later disease risk, the current findings reviewed here have clinical implications.
Clinical implications
Given that maltreated children are at higher risk for physical health problems as well as mental health problems, professionals working with them need to be aware of the potential for poor physical health and integrate its management in their practice. To detect risk of poor physical health in maltreated children, professionals should adopt more holistic approaches to assessment. For example, such children could be assessed for BMI, blood pressure, heart rate, immune-related conditions (e.g., asthma, allergies) and routine blood tests, as well as mental health and psychosocial needs. Notably, looked after children do undergo regular physical health screenings and the findings above suggest that this screening would benefit all maltreated children regardless of care arrangements. Professionals and carers are in the position to put in place interventions to prevent maltreated children from developing physical health problems. It is still unclear which interventions may be effective in preventing physical health outcomes among maltreated children. However, we have summarised the hypothesised pathways from childhood maltreatment to adult clinical outcomes in Figure 1, and these pathways suggest potential targets for interventions. Building on some of these targets, professionals and carers could support maltreated children in engaging in healthy behaviours, such as eating sensibly, exercising and abstaining from smoking, alcohol and drugs, which can have a substantial impact on physical health. Given that health behaviours during early life track into adulthood, establishing healthy habits in maltreated children could reduce their future risk of physical health problems and potentially also improve mental health outcomes. Furthermore, professionals and carers have an important role in promoting mental health, and emerging evidence suggests that treatments for mental health problems can lower pre-clinical physical health risks in maltreated children (Bower and Irwin, 2016; Pace, et al., 2013).
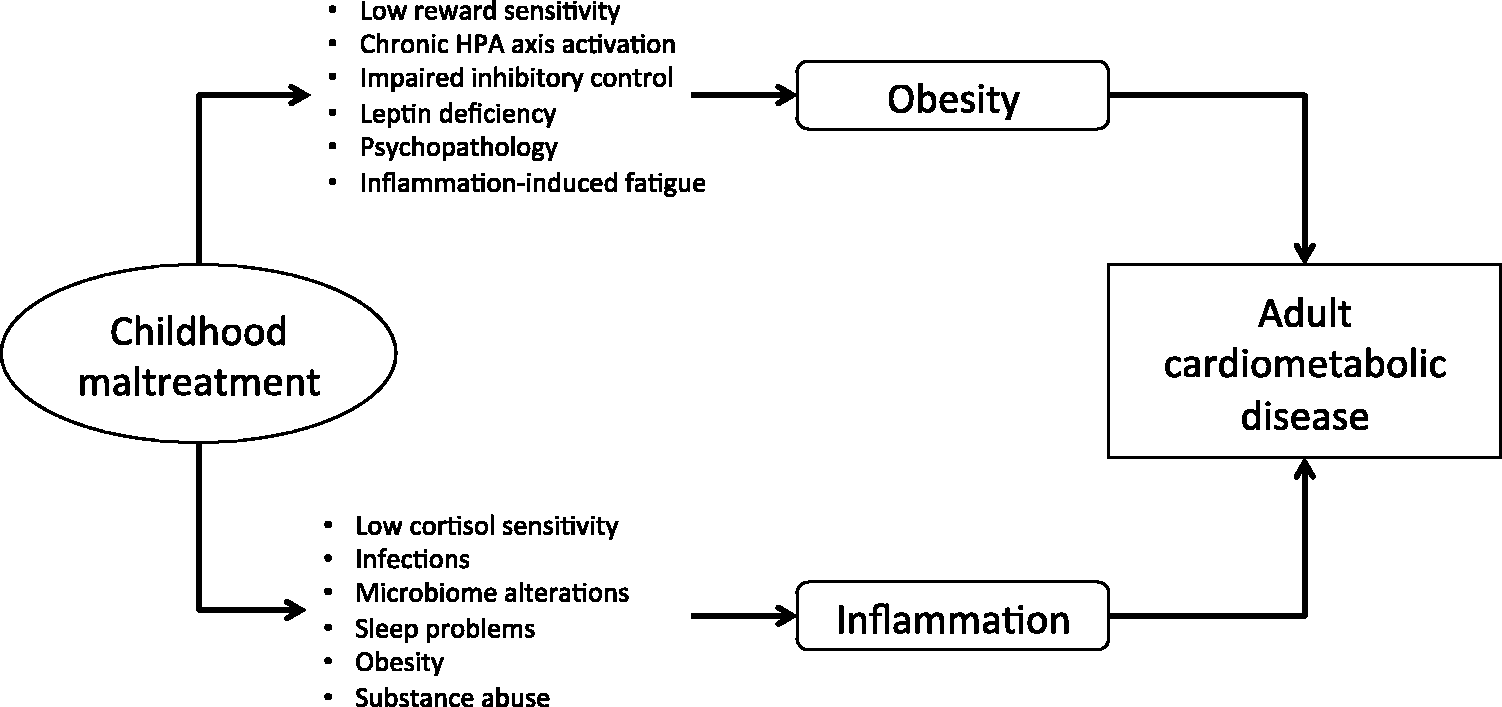
Hypothesised pathways from childhood maltreatment to adult clinical outcomes.
Conclusion
Research reviewed here suggests that childhood maltreatment may confer long-term risk to cardiometabolic disease through biological pathways involving abnormalities in metabolism and the immune system (Suglia, et al., 2018). Specifically, children exposed to maltreatment show a heightened risk of obesity and an elevation in inflammation levels, which are apparent in adulthood but may start emerging earlier in adolescence. To prevent maltreated children from becoming obese and developing high inflammation levels, professionals working with them need to recognise the long-term value of regularly assessing their physical health and helping them to establish long-term healthy habits. Future research should also further characterise the mechanisms through which maltreated children develop risk of obesity and high inflammation levels, so that targeted interventions can be developed to reduce their long-term disease risk.