
Abstract
Background
Diagnosing headache in children and adolescents is challenging because clinical features vary with age, primary and secondary forms may overlap and the use of investigations is often inconsistent.
Methods
We conducted a scoping review following PRISMA guidelines. PubMed, Ovid MEDLINE, Scopus and the Cochrane Library were searched for studies on headache diagnosis in individuals aged 1–18 years (2018–2025). Of 126 records identified, 36 met eligibility criteria and were included.
Results
Several studies indicate that ICHD-3 criteria, developed mainly in adults, may not fully reflect paediatric presentations, contributing to diagnostic uncertainty. Evidence clarifies the value of some red flags while challenging others. Neuroimaging demonstrates low diagnostic yield except in selected cases. Common pitfalls include overdiagnosis of sinusitis, inappropriate EEG use and unnecessary ophthalmologic or allergologic testing.
Conclusions
Accurate diagnosis relies on careful history taking, recognition of age-specific patterns and judicious use of investigations. Paediatric-focused diagnostic pathways are needed. Emerging digital tools and biomarkers may support earlier and more precise diagnosis.
This is a visual representation of the abstract.
Introduction
Headache is one of the most common neurological complaints in childhood and adolescence and a frequent reason for referral to paediatrician.1,2 A recent global systematic review and meta-analysis including 48 school-based and population-based studies from Europe, Asia, North and South America, Africa and Oceania estimated a pooled prevalence of 11% for migraine and 17% for tension-type headache in young people, underscoring the substantial burden of primary headache disorders worldwide. 3 Despite this high prevalence, diagnosing headache in children remains challenging. Clinical manifestations often differ from those observed in adults, and key features required by International Classification of Headache Disorders (ICHD-3) criteria 4 may be difficult to elicit or inconsistently reported, particularly in younger patients, leading to incomplete or atypical phenotypes rather than truly distinct headache entities.5,6
Distinguishing primary from secondary headaches also presents difficulties. Although most headaches in children are benign, clinicians must balance the need to promptly identify potential secondary causes with the risk of over-investigating, especially in the presence of nonspecific symptoms. 7 The interpretation of red flags, indications for neuroimaging, and the use of ancillary tests vary widely across clinical settings and are frequently influenced by persistent misconceptions rather than evidence-based risk stratification.7,8 Consequently, unnecessary investigations and incidental findings are common, while clinically meaningful indicators of secondary headache may be under-recognized. 9 Over the past decade, emerging evidence has refined the diagnostic value of individual warning signs, questioned the specificity of several traditionally cited red flags, and clarified the limited yield of neuroimaging in neurologically normal children.7–9 However, these advances remain scattered across different clinical domains and have not been systematically integrated into a paediatric-focused diagnostic framework.
This scoping review aims to synthesise recent findings on the diagnosis of headache in children and adolescents, focusing on the applicability of ICHD-3 criteria, the diagnostic value of clinical indicators, the role of investigations and the main sources of misdiagnosis. By mapping current evidence, we highlight practical tools for clinicians and identify areas in which paediatric-focused diagnostic criteria and pathways are most needed.
Methods
Study design. This review was conducted according to the Preferred Reporting Items for Scoping Reviews (PRISMA-ScR) guidelines. A scoping approach was chosen to map the breadth of available evidence on the diagnosis of headache in children and adolescents, to identify gaps in current knowledge and to summarise emerging diagnostic themes across heterogeneous study designs.
Search strategy. A comprehensive literature search was performed in PubMed, Scopus, and Web of Science. The search strategy was built around three conceptual groups of terms. The first group included headache-related terms (headache, migraine, primary headache, secondary headache). The second group captured the paediatric population (child, children, paediatric, adolescent). The third group focused on diagnostic concepts and included diagnosis, diagnostic criteria, clinical assessment, differential diagnosis, red flags, neuroimaging, misdiagnosis, and evaluation. Terms related to specific diagnostic tools or domains (e.g., neurophysiology, ophthalmologic assessment, sinus disease, allergic conditions) were captured within the diagnostic concept framework rather than searched as standalone entities. These groups were combined to retrieve studies specifically addressing the diagnosis of headache in individuals aged 1 to 18 years. To reduce retrieval of non-relevant records, we excluded articles whose main focus was treatment, management, prophylaxis, drug interventions or basic science involving animal models. The search was limited to articles published in English from 1 January 2018, corresponding to the release of the third edition of the ICHD-3, to 31 December 2025. Equivalent keyword combinations and filters were applied in all databases. A scoping review methodology was chosen to map and critically appraise the breadth of diagnostic approaches and challenges in paediatric cohort, an area characterized by methodological heterogeneity and limited comparative studies.
Eligibility criteria. Studies were eligible if they focused on the diagnostic evaluation of headache or headache-related disorders in children or adolescents (0–18 years), and provided clinically relevant diagnostic information. We included only original research articles (observational studies, diagnostic accuracy/validation studies, and cohort or registry-based studies). We excluded studies primarily centred on treatment or prevention, interventional trials, adult-only populations, case reports or small case series without diagnostic implications, conference abstracts, non–peer-reviewed material, and non-English publications. For studies primarily investigating primary headache disorders, inclusion required the use of ICHD-3 diagnostic criteria. Conversely, for studies focusing on diagnostic pathways, red flags, neuroimaging practices, or comorbid conditions, formal ICHD classification was not mandatory, as their primary objective was not nosological definition but the evaluation of diagnostic reasoning and risk stratification in children and adolescents with headache.
Study selection. All records were imported into a reference management software for organisation and deduplication. Two reviewers independently screened titles and abstracts according to the predefined eligibility criteria. Full texts of potentially relevant articles were then assessed for inclusion. Any disagreements were resolved by discussion and consensus. The study selection process is summarised in the PRISMA-ScR flow diagram (Figure 1).

PRISMA-ScR flow diagram of study selection. Flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies in accordance with PRISMA-ScR guidelines.
Data extraction and synthesis. Data extraction was conducted independently by two authors using a predefined data-charting form. Extracted variables included: study design, population characteristics and age range, headache type and diagnostic framework (including use of ICHD criteria when applicable), clinical focus (e.g., diagnostic criteria, red flags, neuroimaging, comorbidities), key diagnostic findings, and main conclusions relevant to headache diagnosis. All extracted data were cross-checked by a second reviewer to ensure accuracy and consistency. Given the scoping review design, no quantitative synthesis or meta-analysis was performed.
Results
Study selection. The database search identified 126 records in PubMed. Equivalent searches conducted in Ovid MEDLINE, Scopus and the Cochrane Library yielded overlapping results and did not provide additional unique studies. After deduplication, all 126 records underwent title and abstract screening. Based on the predefined eligibility criteria, 69 records were excluded because they did not address diagnostic aspects of headache, focused primarily on epidemiology, comorbidities or treatment, involved adult or mixed age populations or lacked sufficient methodological detail.
A total of 57 full text articles were assessed for eligibility. Of these, 21 were excluded because they were not focused on diagnosis (n = 10), involved predominantly adult or mixed age populations (n = 4), were mainly treatment oriented (n = 3), were case reports without diagnostic implications (n = 2) or provided insufficient clinical information (n = 2).
Ultimately, 36 studies met all inclusion criteria and were incorporated into the qualitative synthesis (Table 1). The selection process is summarised in the PRISMA-ScR flow diagram (Figure 1).
Studies included in the qualitative synthesis (n = 31). Articles with overlapping diagnostic contributions are grouped.
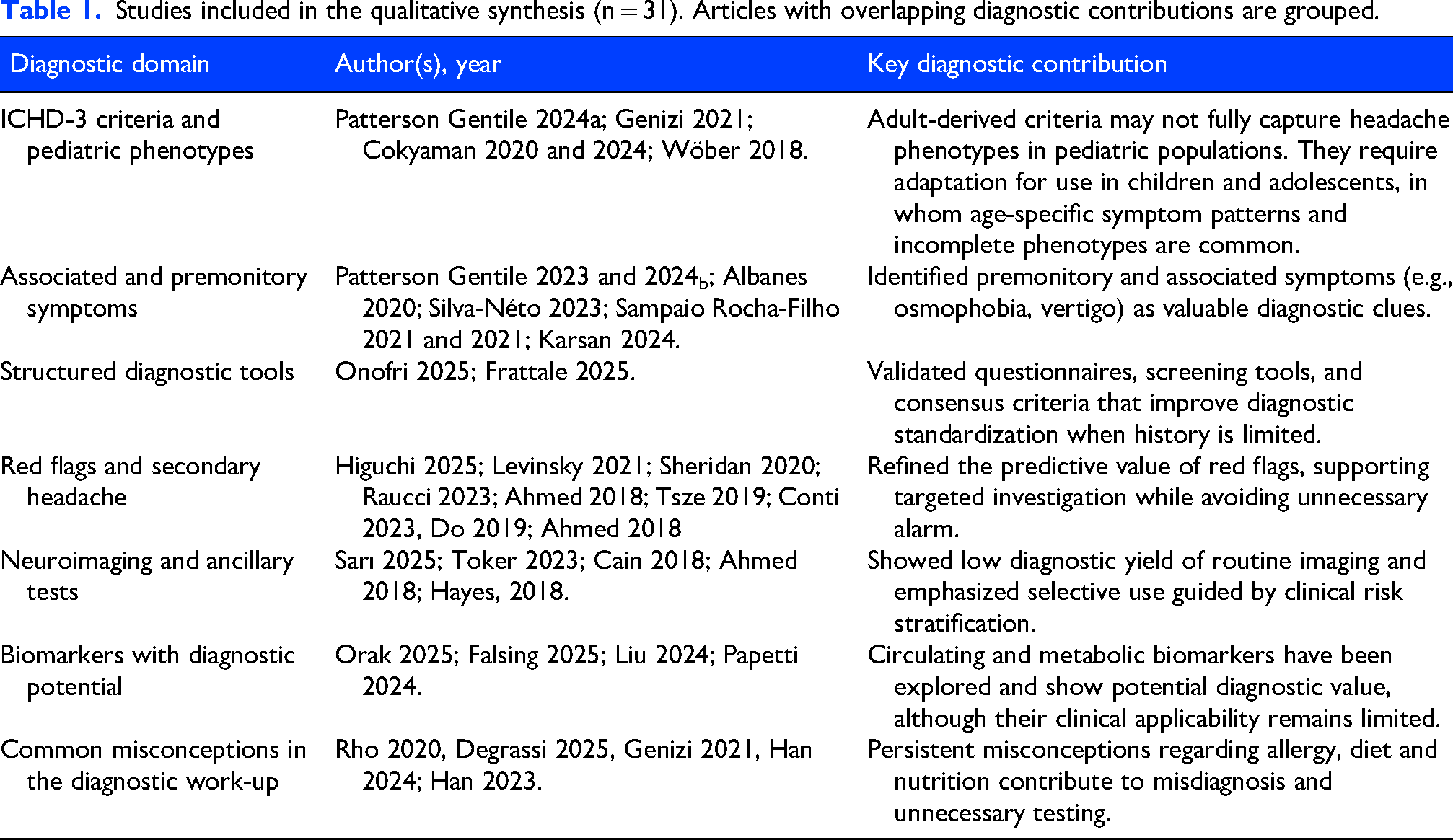
Applicability of ICHD-3 to paediatric populations
Although the ICHD-3 criteria represent the international standard for headache diagnosis, growing evidence highlights limitations when adult derived criteria are applied to children and adolescents.10–16 Migraine in paediatric population frequently differs from the adult phenotype in term of attack duration, pain location, quality, and symptom expression, particularly in younger age groups.13,15 Migraine attacks in younger children often last less than 2 h, which is below the minimum duration required by ICHD-3 4 leading to a high proportion of undetermined diagnoses.5,16,17 Evidence from preschool cohorts shows that removing or relaxing the duration criterion allows many previously unclassified headaches to meet the diagnosis of migraine.11,17
Pain characteristics also differ substantially from adult descriptions. Unilateral, pulsating pain is less common in children, in whom headache is more frequently bilateral or frontal. 13 In addition, younger children may have difficulty describing pulsating pain, photophobia or phonophobia and these features often must be inferred from behaviour rather than verbal report. 12 These factors challenge the direct application of adult symptom descriptors and underscore the risk of misclassification when criteria are applied rigidly. 11
Distinguishing migraine from tension-type headache (TTH) remains particularly challenging in pediatric populations.13,16,17 Clinical overlap between these entities is common, and longitudinal data suggest a dynamic relationship rather than clearly distinct categories, with some children initially diagnosed with tension-type headache later fulfilling criteria for migraine.16,17 This continuum further limits the discriminatory power of strictly categorical diagnostic approaches based solely on ICHD-3. Beyond core pain features, several studies indicate that migraine in children and adolescents is frequently accompanied by a broader range of associated and premonitory symptoms that are not fully represented within the current ICHD-3 framework.12,17–22 While these symptoms are increasingly recognised as clinically relevant, they are only partially incorporated into existing diagnostic criteria. 4
Similar considerations apply to other primary headache disorders, such as trigeminal autonomic cephalalgias (TACs). 11 While ICHD-3 criteria rely on attack duration, frequency, and indomethacin responsiveness for the differentiation of TACs, 4 emerging paediatric evidence suggests that clinical presentations may be more heterogeneous and not always fully captured by current criteria. 11 Recent case series indicate that, compared to adults, cranial autonomic symptoms and restlessness may be less prominent in children, contributing to diagnostic delay and frequent misclassification, often as migraine or as non-headache conditions such as ocular or dental disorders. In addition, the shorter duration of migraine attacks in children and the presence of autonomic features may further complicate the differential diagnosis between migraine and TACs.23,24
In recent years, increasing attention has been given to indomethacin responsiveness in primary paediatric headaches. 25 In hemicrania continua and paroxysmal hemicrania, response to indomethacin is considered diagnostic 6 ; however, responsiveness to this drug has also been described in a broader spectrum of primary headaches, including primary stabbing headache, primary cough headache, SUNCT, and primary exercise headache.24,25 In this context, some authors propose that a diagnostic trial with indomethacin should be considered in selected clinical scenarios, including patients with a clinical presentation suggestive of an indomethacin-responsive headache disorder, strictly unilateral side-locked headache unresponsive to standard treatments, or primary headache disorders refractory to multiple therapeutic interventions, particularly when associated with significant functional impairment. 25
Overall, converging evidence indicates that rigid adherence to adult-derived ICHD-3 thresholds may contribute to underdiagnosis or diagnostic uncertainty in children and adolescents.5,12–20 A more flexible interpretation of criteria, integration of behavioural indicators, and development of paediatric-focused diagnostic refinements appear essential to improve diagnostic accuracy in this population.
Associated and premonitory symptoms as diagnostic modifiers
Beyond core headache features, increasing evidence indicates that associated symptoms substantially contribute to the diagnostic characterization of headache in children and adolescents.19–21 While the ICHD-3 criteria include nausea, vomiting, photophobia and phonophobia as accompanying features of migraine attacks, several studies suggest that this framework does not fully capture the breadth of symptoms commonly reported in younger patients.19,20 Data-driven approaches such as cluster analysis of migraine associated Symptoms (CAMS) have shown that migraine in children and adolescents is characterized by reproducible symptom clusters extending beyond pain and sensory sensitivity, often incorporating dizziness, impaired concentration, fatigue, and subtle autonomic features. 19 Among associated symptoms vertigo are frequently reported in migraine in children and adolescents and may represent key diagnostic clues, particularly in patients with atypical pain features or short-lasting attacks. 21 These symptoms often overlap with vestibular migraine phenotypes and may complicate differential diagnosis with other primary headache disorders if not systematically assessed.4,21
Osmophobia, although not required by ICHD-3, has been shown to have high diagnostic specificity for migraine in paediatric populations and may support diagnosis in otherwise equivocal cases.22,25 Mild autonomic manifestations such as lacrimation, nasal congestion, facial flushing and sweating are increasingly recognized in migraine in children and adolescents and are typically bilateral or poorly lateralized. 20 In contrast to TACs, these symptoms are usually less intense and lack strict ipsilateral concordance with headache pain. 4 Nevertheless, when autonomic signs are prominent or headache attacks are short lasting, especially in younger children with limited symptom reporting, they may still generate diagnostic uncertainty if interpreted in isolation. 20
Some studies highlight the importance of distinguishing associated symptoms from premonitory symptoms, which may precede headache onset by hours or days.26,27 In children and adolescents, premonitory symptoms commonly include fatigue, mood changes, irritability, difficulty concentrating, neck discomfort and increased sensory sensitivity. 26 Extended phenotyping studies confirm that these symptoms are frequent but often under recognised, particularly when headache features are not yet fully developed. 27 Because premonitory symptoms are frequently misinterpreted as triggers or comorbid conditions, their systematic assessment may improve diagnostic accuracy, especially in younger children who more readily report behavioural or functional changes than headache characteristics.27,28
Diagnostic tools and structured assessments
Diagnosis of headache in children and adolescents is primarily clinical, but history taking may be limited by age related communication difficulties, recall bias and inconsistent symptom reporting, particularly in younger children.12,17 To address these challenges, structured diagnostic tools and standardized questionnaires have been increasingly adopted as adjuncts to clinical assessment, allowing systematic collection of headache characteristics, associated symptoms and functional impact, and improving diagnostic consistency, especially when headache features are atypical or incompletely expressed.17,20
The HARDSHIP (Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) questionnaire represents a significant advance in standardized headache assessment in children and adolescents. This tool demonstrated good reliability and diagnostic accuracy, facilitating structured evaluation of headache frequency, associated symptoms and headache related disability across different age groups and clinical contexts. Its use supports both clinical decisions making and epidemiological research by improving comparability of diagnostic data. 29
Similarly, the paediatric validation of the ID Migraine screening tool confirms that brief symptom-based questionnaires can effectively support migraine diagnosis in children and adolescents when appropriately adapted. 30 Although originally developed for adults, ID Migraine retained good diagnostic performance in paediatric populations, particularly through the assessment of key associated symptoms such as nausea and sensory sensitivity. This tool may be especially useful as a first line screening approach in busy clinical settings or when migraine characteristics are not yet fully established. 30
While they do not replace comprehensive clinical evaluation, standardized questionnaires may enhance diagnostic confidence, reduce misclassification and promote a more developmentally sensitive approach to headache diagnosis in children and adolescents.
Red flags and neuroimaging: refined evidence
Although red flags remain central to headache assessment in children and adolescents, increasing evidence shows that many traditionally cited warning signs lack specificity for secondary headache when considered in isolation.31–35 Reliance on single symptoms may lead to overestimation of risk and unnecessary investigations, particularly in neurologically normal children, supporting current recommendations that prioritize clinical context and neurological examination over symptom-based triggers alone when deciding on neuroimaging.36,37
Younger age at headache onset has historically been regarded as a warning sign for secondary headache. Contemporary data, however, show that primary headache disorders are common even in preschool children, and that age alone does not reliably predict intracranial pathology in the absence of additional concerning features.17,33,38 Similarly, headache on awakening or headache waking the child from sleep has long been interpreted as suggestive of raised intracranial pressure. However, recent prospective and retrospective studies demonstrate that nocturnal awakening is frequently reported in children with primary headache disorders and, in neurologically normal patients, is not independently associated with serious intracranial disease, questioning its value as a stand-alone red flag for neuroimaging.34,39–42
A positive family history of headache is common in primary headache disorders and may support diagnostic confidence. However, family history is frequently underreported, and its absence has not been shown to reliably predict secondary or life-threatening headache, nor to discriminate between benign and serious conditions in paediatric populations.40,43 Occipital pain localization has also traditionally been considered a red flag in paediatric age. Emerging evidence indicates that occipital headache is commonly reported in children with migraine and tension-type headache and does not, by itself, discriminate between primary and secondary causes.31,32 In contrast, red flags that consistently retain diagnostic relevance across settings include abnormal neurological examination, focal neurological deficits, progressive worsening of headache over time, signs of raised intracranial pressure such as persistent vomiting or papilledema, thunderclap or rapidly evolving headache onset, and systemic features including fever, weight loss, immunosuppression, or prothrombotic conditions.37,39,40 The presence of these findings, particularly when occurring in combination, is associated with a substantially higher likelihood of secondary headache and justifies prompt neuroimaging and further diagnostic work-up.38,41
Despite increasingly refined evidence, neuroimaging remains overused in paediatric patients with headache. Multiple studies report a low diagnostic yield of brain MRI in neurologically normal children with recurrent headache, with most abnormalities representing incidental findings rather than causative lesions.33,44,45 Findings such as white matter hyperintensities or benign structural variants are frequently detected but rarely correlate with headache characteristics or clinical course, and their identification may increase diagnostic uncertainty and parental anxiety without providing clear clinical benefit.32,35
Overall, current evidence supports a paradigm shift in the interpretation of red flags and the use of neuroimaging in children and adolescents with headache. Rather than acting as binary triggers for investigation, red flags should be interpreted as clinical signals whose relevance depends on their combination, temporal evolution, and association with objective findings.32,37,38 Isolated warning features rarely justify urgent neuroimaging, whereas the coexistence of multiple red flags or their association with abnormal neurological examination or systemic features substantially increases the likelihood of secondary headache (Table 2). In this context, the distinction between primary and secondary headache disorders should be viewed as dynamic and clinically driven. Structural abnormalities detected on neuroimaging are often incidental and not causally related to headache, emphasizing the need for careful clinic radiological correlation.44,45 At the same time, even in primary headache disorders, contributory factors and comorbidities should be considered, and selected entities, such as trigeminal autonomic cephalalgias in paediatric patients, warrant targeted neuroimaging to exclude underlying structural or vascular causes.4,11
Practical red flags to guide further investigation in children and adolescents with headache.

Diagnostic value is qualitative and intended for clinical triage; interpretation depends on age, context, and examination findings.
Legend: OCT = Optical Coherence Tomography; ED = Emergency Department; IIH = Idiopathic Intracranial Hypertension; RCVS = Reversible Cerebral Vasoconstriction Syndrome.
Biological markers as exploratory diagnostic adjuncts
Alongside advances in clinical phenotyping, several studies have explored biological markers as potential adjuncts to headache diagnosis in children and adolescents, although none currently demonstrate sufficient accuracy to support routine diagnostic use.
Among circulating biomarkers, neuropeptides involved in migraine pathophysiology have been most extensively investigated. Calcitonin gene-related peptide (CGRP) has been consistently reported at higher serum levels in children and adolescents with migraine compared with healthy controls.46,47 However, both studies showed a wide overlap between patients and controls, with no reliable diagnostic cut-off values, limiting the individual discriminatory value of CGRP. In addition to CGRP, substance P, vasoactive intestinal peptide (VIP) and neuropeptide Y were evaluated in paediatric cohorts but results were heterogeneous and inconsistent, and none of these neuropeptides demonstrated sufficient sensitivity or specificity for diagnostic purposes. 47
Beyond circulating neuropeptides, metabolic and gut-related pathways have gained increasing attention. Altered tryptophan metabolites and differences in gut microbiota composition have been described in children and adolescents with migraine, suggesting a potential involvement of the gut–brain axis in migraine expression rather than diagnosis.48,49 At present, methodological heterogeneity, lack of standardization and overlap with non-headache populations preclude clinical diagnostic application.
Overall, current evidence indicates that biological markers in headache should be regarded as pathophysiological correlates and research tools, rather than diagnostic instruments. Common Misconceptions in the diagnostic work up.
A frequent misconception in the diagnostic evaluation of headache in children and adolescents is the attribution of symptoms to incidental findings or low-yield investigations. Electroencephalography (EEG) is still frequently requested in children presenting with headache, despite limited diagnostic yield. Large observational and multicentre studies confirm that routine EEG rarely contributes to headache diagnosis and does not distinguish primary headache disorders from secondary causes.12,50 EEG may be appropriate only in selected clinical contexts, such as when headache is associated with paroxysmal visual symptoms suggestive of epileptic phenomena, brainstem aura mimicking seizures, or when headache coexists with a known or suspected seizure disorder.48,49 Visual symptoms in migraine with aura typically have a gradual onset and progressive spread over several minutes and include both positive phenomena (such as scintillating scotoma, zig-zag lines, flashing lights) and negative symptoms (visual field defects or scotomas), with a total duration of 5–60 min. 3 In contrast, visual symptoms related to epileptic seizures are abrupt in onset, brief (seconds to minutes), highly stereotyped, and usually consist of simple positive visual phenomena. 51
Another common misconception concerns routine ophthalmological referral. Although selected secondary headache disorders may be related to ocular pathology, these conditions are usually associated with specific ocular symptoms and signs. 52 In children and adolescents with primary headache disorders such as migraine, visual acuity is typically preserved and correction of refractive errors does not influence headache frequency or severity. Recent paediatric ophthalmology reviews emphasize that routine ophthalmological assessment is not indicated in the absence of visual impairment, ocular pain, redness or diplopia.52,53
Cranial autonomic symptoms during headache, including nasal congestion, rhinorrhoea, and lacrimation, are frequently misinterpreted as indicators of sinus disease, leading to unnecessary neuroimaging. However, autonomic features are increasingly recognized as part of the migraine spectrum and may also occur in trigeminal autonomic cephalalgias in children and adolescents.20,54 Radiological abnormalities of the paranasal sinuses are common incidental findings in otherwise healthy children, and spontaneous improvement without antibiotic therapy is frequently observed, supporting a non-causative role in many cases. 55
Current evidence indicates that the association between headache and allergic disorders in paediatric patients reflects comorbidity rather than causality; therefore, allergological testing should not be performed routinely and is warranted only in the presence of suggestive symptoms. 56 Moreover, although dietary factors may act as individual headache triggers the indiscriminate elimination diets are not recommended and may increase unnecessary dietary restrictions without clinical benefit.57,58
Limitations
This scoping review was not designed to provide quantitative synthesis or formal risk-of-bias assessment. Included studies were heterogeneous in design and diagnostic focus, and formal ICHD-3 classification was not uniformly applied in studies addressing diagnostic pathways, red flags, or neuroimaging. Only English-language publications were included. These limitations are inherent to the scoping methodology but are balanced by the comprehensive mapping of clinically relevant diagnostic evidence.
Conclusions
Diagnosing headache in children and adolescents remains primarily clinical, yet recent literature highlights persistent heterogeneity in diagnostic approaches and frequent overuse of investigations.8,10 Evidence published since the introduction of ICHD-3 supports its role as the reference framework, 4 while also underscoring limits in its applicability to paediatric populations, particularly due to age-related variations in headache duration, pain localization, and associated symptoms.5,6,11 These challenges extend beyond migraine to other primary headache disorders, including TACs which may present with atypical features and overlap with more common conditions.
Rather than introducing new definitive tests, recent studies refine the relative weight of clinical features, validated screening tools, and risk-based investigation strategies, emphasizing the need for standardized, evidence-informed diagnostic pathways tailored to children and adolescents.
This scoping review underscores that careful clinical history and neurological examination remain central to diagnosis, whereas many commonly used investigations have low diagnostic yield when applied without clear indications. Misinterpretation of nonspecific symptoms and incidental findings frequently leads to over-investigation. Adoption of age-adapted diagnostic approaches and more judicious use of ancillary tests may improve diagnostic accuracy and reduce unnecessary procedures in paediatric headache care.
Clinical implications
Prioritize clinical history and focused neurological examination. Avoid routine low-yield tests without red flags or focal signs. Recognize paediatric headache phenotypes may differ from adult criteria. Prevent misdiagnosis by distinguishing incidental autonomic, sinus, allergic, and dietary findings from causal factors.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
All authors consent to the publication of this manuscript.
Author contributions
LP: Conceptualization, Writing the original draft, Supervision. AB: Investigation, Writing, review & editing, Visualization. CG: Investigation, Writing, review & editing, Visualization. FU: Investigation, Writing, review & editing. GS: Investigation, Writing, review & editing. MV: Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health (Current Research funds) and by the project MNESYS (PE0000006 – A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author, upon a reasonable request.
Open practices
None.
Supplemental material
Supplemental material for this article is available online.