
Abstract
Past research has categorized the rape experiences of women attending college into types primarily based on perpetration tactics and/or survivor substance use. However, this practice may overlook key differences. Therefore, in the current study, we sought via latent class analysis (LCA) to identify types of rape using multiple assault characteristics, including survivor resistance and substance use by the survivor and perpetrator. Participants were 344 college women who experienced rape since age 14 who completed an online survey. A five-class rape typology model was the best-fit: (a) Combined force/substance-facilitated rape (16.0%), (b) Substance-facilitated rape, congruent drinking (18.0%), (c) Substance-facilitated rape, non-congruent drinking (14.0%), (d) Low force/resistance rape (25.0%), and (e) Forcible rape (27.0%). Classes differed in acknowledgment, perpetrator relationship, current psychological distress, and recent hazardous drinking. Findings showed that college women’s rape experiences fell into several distinct typologies on the basis of the presence of force/resistance as well as survivor and perpetrator substance use/substance-related impairment. Practitioners working with college rape survivors should be mindful of how multiple assault characteristics may affect survivors’ recovery trajectory. Future research should further investigate the implications of these rape typologies on adjustment, recovery, and re-victimization risk among survivors.
Unfortunately, many women attending college have a history of sexual assault. For example, approximately 16% of women enter college with a prior history of sexual assault in adolescence, including 11% with a pre-college completed rape history (Jordan et al., 2014; Krebs et al., 2009). Once enrolled in college, it is estimated that 23%–25% of women experience at least one sexual assault (e.g., Cantor et al, 2015; Jordan et al., 2014). Further, 3%–10% of women attending college experience a completed rape in a given academic year, with women in their first year of college at highest risk (Decker & Littleton, 2018; Jordan et al., 2014; Messman-Moore et al., 2009). Experiencing sexual assault prior to or during college, particularly completed rape, is associated with a host of negative outcomes, including the development of posttraumatic stress disorder (PTSD) and depression, hazardous alcohol use, suicidality, poor academic performance, and college dropout (Chang et. al., 2015; e.g., Baker et al., 2016; Jordan et al., 2014; Messman-Moore et al., 2009; Zinzow et al., 2010).
Given the prevalence of sexual assault among college women and its association with a host of negative outcomes, researchers have sought to identify factors related to assault outcomes and recovery, including whether characteristics of survivors’ assaults are related to systematic differences in outcomes and recovery. The majority of this work has focused on rape perpetration tactics and survivor substance use prior to the rape, classifying survivors’ rape experiences as representing a forcible (perpetrated using physical force), substance-facilitated (occurring when the survivor was impaired due to substances given to her by the perpetrator), or incapacitated (occurred when the survivor was incapable of consenting due to voluntary substance use) assault (e.g., Krebs et al., 2009; Zinzow et al., 2010). For example, in a national sample of college women who were rape survivors, Zinzow and colleagues (2010) found that experiencing a forcible rape was associated with the highest risk of PTSD and depression as well as a higher likelihood of rape acknowledgment, as compared to experiencing the other two types of rape. Using a slightly different assault classification approach, Littleton, Grills-Taquechel, and Axsom (2009) classified college women’s rape experiences (prior to or during college) into three types based on the survivor’s level of substance-related impairment during the assault (regardless of whether the substance use was voluntary): not impaired, impaired (e.g., had trouble walking, had trouble speaking), and incapacitated (e.g., unconscious). They found significant differences among survivors of these three assault types on rape-related stigma, self-blame, assault disclosure, and relationship with the assailant. Specifically, non-impaired survivors endorsed the lowest level of stigma and self-blame and were most likely to have been assaulted by a romantic partner. In contrast, impaired survivors were least likely to disclose the assault.
Rather than classifying assaults into different types based on a single assault characteristic, a few studies have sought to identify sexual assault typologies based on multiple characteristics although in non-college samples. Peter-Hagene and Ullman (2015) utilized cluster analysis to identify assault types among a sample of community women who experienced adolescent or adult sexual assault. Three assault type groups emerged which differed in PTSD symptom severity: an “alcohol-related” group which involved survivor alcohol use and perpetrator force, a “high-violence” group which involved severe perpetrator force and no survivor alcohol use, and a “moderate sexual assault severity” group with lower assault severity and perpetrator physical force and no survivor alcohol use. As another example, Masters and colleagues (2015) used latent class analysis (LCA) to identify sexual assault types in a sample of community women considered at elevated risk for HIV/STI infection. This analysis also yielded a three-class model: “contact or attempted” assaults characterized by experiencing a sexual assault other than rape and intoxication by the survivor, “incapacitated” assaults characterized by completed rape and survivor intoxication during the assault, and “forceful severe” assaults characterized by completed rape and force by the perpetrator. Women classified as having experienced these three different types of assault differed in anxiety, depression, trauma symptoms, and heavy episodic drinking with those in the forceful severe assault class having significantly higher scores on these variables than the other two classes. Thus, results of both studies support the potential utility of classifying sexual assaults based on multiple assault characteristics, as this may provide a fuller picture of common patterns of sexual assault experiences that are likely systematically related to post-assault adjustment patterns.
However, no study to our knowledge has sought to classify the assault experiences of college women using multiple assault characteristics. This is a significant gap in the literature given that women attending college are a high-risk group for sexual assault prior to and during college, and it is likely that key differences exist in the assault experiences of women attending college as compared to other populations (Kilpatrick et al., 2007). Therefore, in the current study, we sought to utilize LCA to identify sexual assault typologies among a sample of female rape survivors attending college. LCA was chosen over other analytic approaches (e.g., cluster analysis) due to the several advantages afforded by use of LCA, including the ability to evaluate the fit of multiple models to the data via examination of model fit indices (Wang & Hanges, 2011). We also focused specifically on the experience of completed rape survivors due to the likelihood that assault type (e.g., completed rape, attempted rape unwanted touching) would be associated with a number of assault characteristics (e.g., substance-related impairment, survivor resistance, perpetrator force). Specifically, in the current study, we sought to identify sexual assault typologies using LCA among a sample of 344 college women who had experienced completed rape since the age of 14. A number of assault characteristics were included in the LCA model, including perpetration tactics (intimidation, threats of violence, physical force) and resistance behaviors by the survivor. We chose to include resistance behaviors given evidence that survivor resistance (i.e., the extent to which the survivor engaged in clear and assertive resistance behavior) is associated with assault outcomes, including greater PTSD symptomology and greater rape acknowledgment (e.g., Cook & Messman-Moore, 2018; Littleton, 2010). Further, resistance behaviors are both a response to the perpetrator’s tactics, as well as likely influence perpetration strategies (e.g., threats of harm, intimidation, physical force) used by the perpetrator (e.g., Balemba & Beauregard, 2012). In addition, given the frequency of pre-assault alcohol and other substance use by the perpetrator and survivor among college women who experienced sexual assaults prior to or during college, and the frequency with which college women who are survivors of sexual assaults are impaired or incapacitated by substances, we included multiple substance-related variables in the LCA (e.g., Krebs et al., 2009; Littleton, Grills-Taquechel, & Axsom, 2009; Littleton et al., 2017). Specifically, we included whether the survivor and perpetrator engaged in binge or non-binge drinking, the level of substance-related impairment experienced by the survivor, and whether the survivor and perpetrator used other drugs prior to the assault.
We also sought to identify multiple correlates of membership into the identified assault type classes, including the survivor’s relationship with the perpetrator (e.g., stranger/just met, friend/acquaintance, romantic partner), whether the survivor acknowledged the rape as a crime/victimization, and their prior history of engaging in consensual sex with the perpetrator. These correlates were chosen given their association with different sexual assault typologies (e.g., forcible assault, incapacitated assault) in prior research (Littleton, Grills-Taquechel, & Axsom, 2009; McConnell et al., 2020; Zinzow et al., 2010). We also evaluated current symptoms of depression, rape-related PTSD, and hazardous drinking as correlates of assault type class membership. These three symptom classes were chosen given prior work supporting their association with sexual assault typologies (Masters et al., 2015; McConnell et al., 2020; Peter-Hagene & Ullman, 2015; Zinzow et al., 2010).
We made several hypotheses. Specifically, we hypothesized that the LCA would support the existence of multiple assault type classes, differentiated by combinations of perpetration tactics, survivor resistance behaviors, substance use by the survivor and perpetrator, and level of substance-related impairment by the survivor (Masters et al., 2015; Peter-Hagene & Ullman, 2015). We also hypothesized that some assault type classes would be differentiated by the probability of inclusion of perpetrator force, survivor impairment/incapacitation, and both (Peter-Hagene & Ullman, 2015). In addition, we hypothesized that some assault type classes would be differentiated by the probability of inclusion of perpetrator substance use (Zinzow & Thompson, 2014).
With regard to correlates of class membership, we hypothesized that survivors of assault types involving a greater probability of inclusion of substance use/impairment by the survivor at the time of the assault would be associated with more current hazardous drinking (Messman-Moore et al., 2015). We also hypothesized that survivors of assault types involving a greater probability of survivor resistance behaviors would be associated with a greater likelihood of acknowledgment (e.g., Cook & Messman-Moore, 2018). Finally, we hypothesized that survivors of assault types involving a greater probability of inclusion of physical force tactics by the perpetrator would be associated with more current distress (depression and PTSD symptoms; Zinzow et al., 2010).
Method
Participants
Participants were 344 cisgender women (19.2% of the full sample) who indicated on a voluntary online survey that they experienced a completed rape since age 14, drawn from a larger sample of 1,791 undergraduate women attending a large Southeastern university. Participants were primarily first (80.8%) or second (14.0%) year students. When asked to select all racial or ethnic categories that described themselves, the majority selected White/European American (84.3%), with 14.2% selecting African American, and 5.2% Hispanic/Latina. Fewer women selected Asian American (2.9%), Native American (1.7%), Caribbean Islander (1.5%), Pacific Islander (0.6%), North African/Middle Eastern (0.3%), or multi-ethnic (2.0%). A total of 93.0% of participants described themselves as heterosexual, 4.9% as bisexual, 1.5% as lesbian, 0.3% as pansexual, and 0.3% as asexual. Participants were 18.4 years of age on average (SD = 1.0 years).
Procedures
Undergraduate women were recruited from a psychology department participant pool of individuals enrolled in Introduction to Psychology (a general education requirement at the university often completed in students’ first year of college) to complete a voluntary self-report confidential online study of “unwanted sex, sexual behaviors, adjustment, and sexual functioning” for course credit, described as being open to all women over the age of 18.
Participants were recruited over the course of three academic semesters: Fall 2016, Spring 2017, and Fall 2017. Participants completed a confidential online survey of their history of rape victimization, characteristics of the assault, hazardous drinking, psychological adjustment, and other measures not utilized in the current study (e.g., sexual functioning, sexual motives, sexual risk behaviors). A total of 1,930 survey responses were received out of a planned 1,900 (to ensure a sample size of at least 300 women with a history of completed rape). Of these responses, 94 were deleted for extensive missing data (over 50% missing), 32 represented duplicate responses, and 13 represented a pattern of invalid responding (e.g., indicating they consumed 50 drinks prior to their sexual assault, marking all 3s on the PTSD measure). The study was approved by the East Carolina University IRB and all participants were provided information about area free and low-cost mental health resources, including those for survivors of sexual assault.
Measures
Adolescent/adult rape history
Participants were screened for adolescent/adult rape experiences (since the age of 14) using three yes-no behaviorally specific items derived from the Sexual Experiences Survey-Revised (SES-R; Koss et al., 2007). Items assessed completed rape (oral, vaginal, or anal sex) that occurred via (a) threats of physical harm to the participant or someone close to them, (b) use of physical force such as holding the individual down or having a weapon, or (c) taking advantage of the fact that the participant was incapable of consenting following substance use. Participants endorsed at least one of these three items.
The SES-R is the most widely used screening measure for rape because of item agreement with research and legal definitions (Koss & Gidycz, 1985). Supporting reliability, over 70% of a sample of primarily White college women reported the same type of sexual assault experience over two assessments, 2 weeks apart (Johnson et al., 2017). Additionally, among a sample of primarily White college women, endorsement of SES-R rape items demonstrated moderate agreement across two assessments (1–4 weeks; κ = .60; Littleton et al., 2019).
Supporting the measure’s validity, SES-R scores have been moderately associated with scores on measures of psychological distress, trauma symptoms, hazardous drinking, and relationship abuse history (Davis et al., 2014; Johnson et al., 2017; Littleton et al., 2019).
Assault characteristics
To obtain information about the characteristics of participants’ rape experience, they were asked to complete a 20-item assault characteristics questionnaire with regard to their “unwanted sexual experience” or self-assessed worst experience if they had a history of multiple sexual assaults (Littleton et al., 2006). This questionnaire was initially developed by Koss (1985) and then modified by Layman and colleagues (1996); it was later expanded by Littleton and colleagues (2006). Responses to these items were coded using the categories developed in later work (Littleton et al., 2017).
Specifically, participants were asked to indicate their relationship with the assailant, which was coded as romantic (e.g., casually dating, romantic partner), friend/acquaintance, or stranger (i.e., stranger, just met). They were also asked to indicate the gender of the perpetrator(s): man, woman, both men/women, or other. Participants were asked to indicate all the tactics used by the perpetrator to obtain sex from a list, which were coded into the following categories: non-verbal threats/intimidation, verbal threats, moderate physical force (holding the participant down, using their body weight), and severe physical force (hitting, choking, beating, using/showing a weapon). Participants endorsed all the strategies they used to indicate they did not want to engage in sexual activity from a provided list, which were coded into the following categories: low assertive resistance (turned cold, cried), moderately assertive resistance (said “no” or “stop,” tried to reason or plead with them), and strongly assertive resistance (ran away, physically struggled, screamed for help, hit/kicked/punched/scratched/bit them).
Participants were also asked to estimate the number of standard alcoholic drinks they and the perpetrator consumed prior to the assault, with participants who reported consuming four or more drinks coded as binge drinking, and perpetrators described as having consumed five or more drinks coded as binge drinking (95.6% described their perpetrator[s] as being a man or men and no participants who reported the perpetrator was a woman reported she consumed four drinks exactly; National Institute on Alcohol Abuse and Alcoholism, 2006). Survivors who reported consuming one to three drinks were coded as non-binge drinking, as were perpetrators described as having consumed one to four drinks. Participants also indicated if they and the perpetrator had used other drugs prior to the assault. Participants indicated their substance-related impairment from a provided list, coded into the following categories: asleep, unconscious, impaired (i.e., had trouble speaking, had trouble walking, had trouble moving limbs). They also indicated if they had engaged in consensual sex (oral/vaginal/anal sex) with the perpetrator prior to the assault. Additionally, they were asked how old they were when the assault occurred and how many experiences with unwanted sex they had since they turned 14 years old. Finally, participants were asked to indicate which term they thought “best described their experience”; those who selected a victimizing label (rape, attempted rape, sexual assault, some other type of crime) were coded as acknowledged and those who did not choose a victimizing label (miscommunication, bad sex, hook-up, seduction, not sure) were labeled as unacknowledged.
Because of the way many items were administered (i.e., mark all that apply from a list), it was not possible to calculate the percentage of missing data on the majority of assault characteristics assessed. For those items on which missing data could be calculated, it was generally rare, ranging from 0.0% (drug use by the perpetrator) to 3.2% (term that best described their experience). Similarly, items that required participants to respond to an open-ended prompt were associated with mostly minimal missing data (approximately 3%), primarily due to a few individuals not providing codable responses (e.g., not sure). However, 21.8% did not respond to or did not provide a codable response to the open-ended item querying them regarding their age when the assault occurred, and 8.7% did not respond to or did not provide a codable response to the open-ended item querying them regarding how many assaults they had experienced.
PTSD symptoms
Rape-related PTSD symptoms were assessed with the PTSD Symptom Scale–Self-Report (PSS-SR; Foa et al., 1993), a brief 17-item measure of symptoms consistent with DSM-IV diagnostic criteria for PTSD. Participants were asked to indicate how often they experienced each symptom in the past 2 weeks in relation to their experience of unwanted sex on a 4-point scale anchored by 0 (not at all) and 3 (five or more times per week/very much/always). Scores on all items are summed and can range from 0 to 51 with a recommended cutoff for likely PTSD of 14 or above (Coffey et al., 2006). The PSS-SR was found to have a 62% sensitivity and 100% specificity for a diagnosis of PTSD obtained via structured clinical interview among a sample of primarily African American women rape survivors recruited from the community (Foa et al., 1993). Further, scores were strongly correlated with scores on other self-report measures of trauma and anxiety symptoms (Foa et al., 1993). Scores on the measure have also demonstrated good internal consistency among rape survivors, including among White and African American college and community-recruited rape survivors (α = .93; Foa et al., 1993; Littleton, Axsom, & Grills-Taquechel, 2009). Cronbach’s α was .96 in the current study. A total of 2.0% (n = 7) of participants had missing data on this measure.
Depression symptoms
Depression symptoms were assessed with the depression subscale of the 21-item Depression Anxiety Stress Scales (DASS-21; Crawford & Henry, 2003; Lovibond & Lovibond, 1995). For each item, participants were asked to indicate how much it applied to them over the past week on a 4-point scale anchored by 0 (did not apply to me at all) and 3 (applied to me very much or most of the time). Scores on all items are summed and then doubled and can range from 0 to 42, with a recommended score range for moderate depression of 14 to 20 and a score of 21 or above for severe depression (Lovibond & Lovibond, 1995). A prior confirmatory factor analysis utilizing a large sample of British adults supported the three-factor structure of the measure as well as strong correlations of depression subscale scores with other self-report measures of depression and psychological distress (Henry & Crawford, 2005). In a sample of primarily White United States (U.S.) college students, Cronbach’s α was .85 for the scores on the depression scale (Osman et al., 2012) and in the current study was .91. A total of 0.3% (n = 1) of participants had missing data on this measure.
Hazardous alcohol use
Hazardous alcohol use in the past 6 months was assessed using the five-item version of the Alcohol Use Disorders Identification Test (AUDIT-5; Babor et al., 2001; Miles et al., 2001). The AUDIT-5 assesses drinking behaviors (drinking frequency, number of drinks consumed on a typical day) and drinking-related problems (e.g., difficulty stopping drinking) and is scored by summing the five items (all of which are scored on a 0–4 scale), with a maximum score of 20 points, and a cutoff score of 5 or above for hazardous alcohol use (Miles et al., 2001). A sample item is, “How often during the past six months have you found that you were not able to stop drinking once you started?,” with response options of never (0), less than monthly (1), monthly (2), weekly (3), and daily (4). Among a sample of British college students, the measure demonstrated a sensitivity of 79% and a specificity of 97% for identifying individuals with alcohol problems (Miles et al., 2001). Supporting the measure’s validity, scores were also associated with self-reported drinking frequency and alcohol-related consequences (Miles et al., 2001). Cronbach’s α among a sample of racially/ethnically diverse U.S. university women was .77 (Littleton et al., 2014) and in the current study was .68. A total of 30 women (8.7%) reported no alcohol use in the past 6 months and were not administered the AUDIT-5. No additional participants had missing data on this measure.
Analysis Plan
An LCA was conducted in MPlus version 8.0 (Muthén & Muthén, 1998–2017). The LCA was run utilizing the default settings in MPlus, which utilizes all available data under missing data theory, which assumes that data are missing at random, and a total of 100 random starts were specified. The LCA was conducted using the following 16 dichotomous assault characteristic items: force tactics (non-verbal intimidation, verbal threats, moderate force, and severe force), resistance strategies (low, moderate, and high assertive resistance), drinking by the survivor and perpetrator (binge drinking and non-binge drinking), drug use by the survivor and perpetrator, and substance-related impairment of the survivor (asleep, unconscious, and impaired). For each of these assault characteristics, the presence of that assault characteristic was coded as 1, and the absence of that assault characteristic was coded as 0. LCA is an empirically driven procedure that defines taxonomies or profiles of individuals based on common characteristics. LCA uses all observations of the dependent variables (assault characteristics) to define these profiles via maximum likelihood estimation (Merz & Roesch, 2011). The estimated probability that an individual was properly classified, which ensures each individual to be placed into the best-fitting class, is estimated simultaneously with the overall model (Merz & Roesch, 2011). Models are estimated with classes added sequentially to determine which model best fits the data (Merz & Roesch, 2011).
In order to determine the optimal number of classes for the data, three statistics were calculated and compared: the bootstrapped likelihood ratio test (BLRT), the Bayesian information criteria (BIC), and the sample size-adjusted Bayesian information criteria (sBIC). The BLRT compares the fit of the target model to a comparison model with one fewer class. The p value generated for this procedure evaluates whether the solution with more classes (p < .05) or fewer classes (p > .05) is a better fit (Merz & Roesch, 2011). The BIC and sBIC are descriptive fit indices, where lower relative values suggest better model fit (Schwarz, 1978; Sclove, 1987). These three fit indices were chosen given data from simulation studies suggesting that these indices have the lowest type I error rate and most power when conducting LCA (Nylund et al., 2007). It also has been suggested that small profiles (containing less than 5% of the sample) are typically considered spurious profiles; therefore, profile size was also considered when deciding on the best model (Merz & Roesch, 2011). In addition to these indices, each model was evaluated on interpretability to determine whether the profiles ultimately represent different categories (Merz & Roesch, 2011). Additionally, Nylund and colleagues (2007) found that a “flattening out” of fit indices can occur when continuing to add additional classes; therefore, this was also evaluated when determining the best fitting model. Finally, another way to examine how well individuals have been classified is to look at the entropy of the latent class model (Clark & Muthén, 2009). Entropy can be considered a measure of variability within latent classes with higher values (closer to 1.0) indicative of better model fit (Larose et al., 2016).
Power of LCA is dependent on multiple factors including sample size, number of indicators, and class separation, with class separation being most influential, with very large sample sizes necessary to obtain adequate power if there is small-sized separation among classes (Tien et al., 2013). Therefore, we examined the odds ratios of item probabilities between classes to evaluate class separation, with odds ratios of > 5.0 and < 0.20 used as thresholds for indication of a large separation between classes (Nylund-Gibson & Choi, 2018).
The three-step procedure developed by Vermunt (2010) was conducted to examine dichotomous covariates of class membership. In this approach, the latent class model is first estimated using LCA indicator variables. Next, the most likely class variable is created using the latent class posterior distribution. Finally, a multinomial logistic regression is conducted using most likely class membership, taking into account the misclassification at Step 2 (Asparouhov & Muthén, 2014). For these analyses, rape acknowledgment, relationship with perpetrator, and prior consensual sex were entered as predictors.
The BCH approach (Bakk et al., 2016) was used to examine continuous covariates of class membership (Asparouhov & Muthen, 2014). The BCH approach involves first estimating the latent classes, then assigning observations to latent classes, and finally testing weighted differences across classes in standing on the auxiliary variable, assigning weights to reflect the measurement error of the latent class variable (Asparouhov & Muthen, 2014; Bakk et al., 2016). This procedure first produces a test of the overall model for each covariate of class membership. If this overall test is significant, differences in weighted means are examined among each pair of latent classes. Auxiliary variables examined by the BCH approach were DASS-21 depression, PSS-SR, and AUDIT-5. A modified Bonferroni adjustment utilizing the Holm procedure was employed to evaluate statistical significance for the two sets of auxiliary analyses (dichotomous covariates and continuous covariates) utilizing the Gaetano (2013) calculator (Holm, 1979; Olejnik et al., 1997).
Results
Assault Characteristics and Adjustment
Assault characteristics for the overall sample are summarized in Table 1. The majority of survivors reported that the perpetrator used physical force, with moderate physical force being the most common type of force reported, as well as that they engaged in resistance, with moderately assertive resistance most commonly reported. Binge drinking by the survivor and perpetrator were frequently reported, as was substance-related impairment. One third of participants (33.7%, n = 116) were romantically involved with the assailant and nearly half (48.8%, n = 168) acknowledged the assault. A total of 13.1% (n = 45) were 14–15 years old when the rape occurred, 39.2% (n = 135) were 16–17, 22.7% (n = 78) were 18, and 3.2% (n = 11) were 19 or older (21.8%, n = 75 missing/not codable). Finally, 50.0% (n = 172) indicated that they had experienced multiple assaults.
Assault Characteristics Among Rape Survivors.
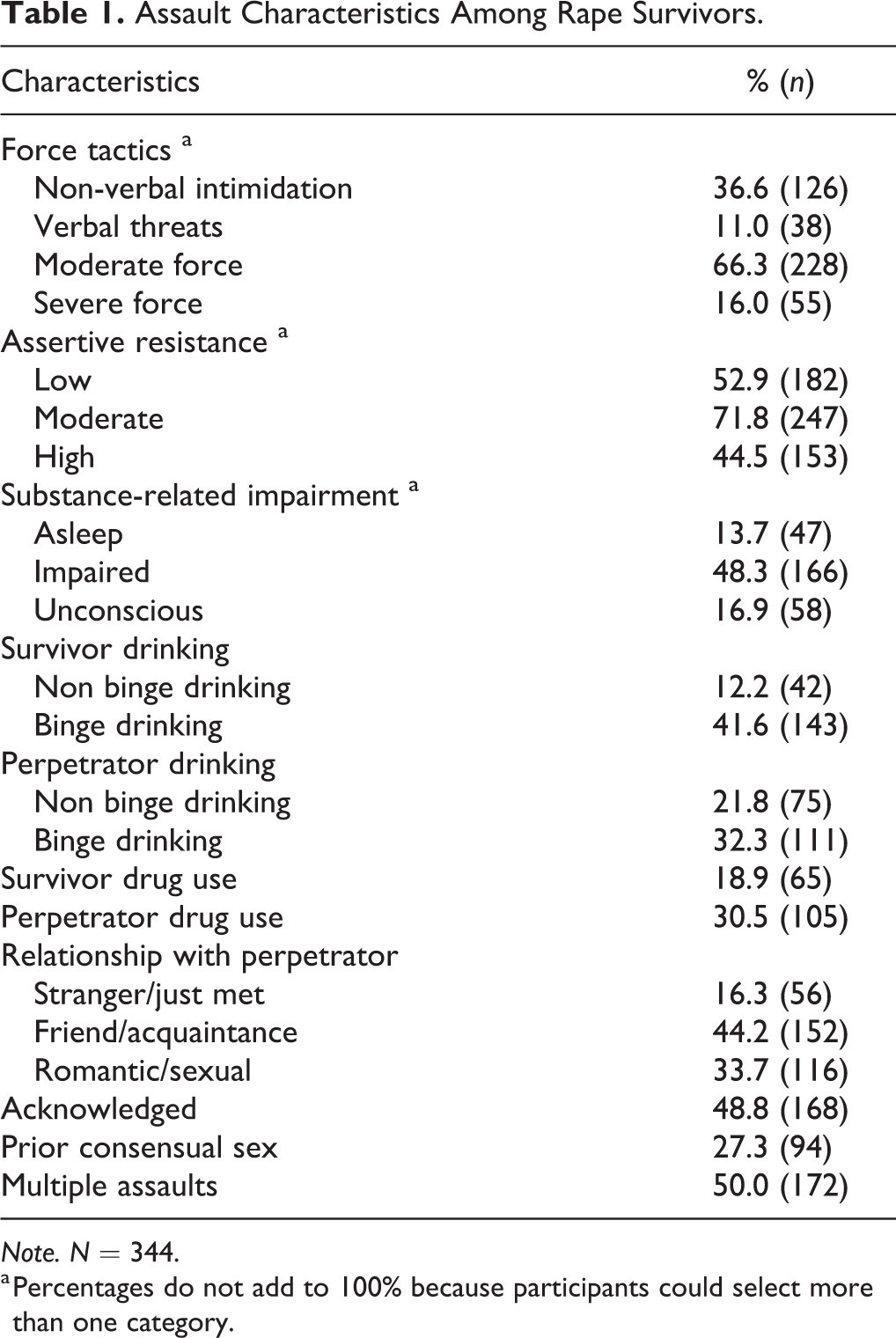
Note. N = 344.
a Percentages do not add to 100% because participants could select more than one category.
As far as current adjustment, 33.9% of participants scored above the cutoff for current rape-related PTSD, 16.6% scored above the cutoff for moderate depression, and an additional 14.8% above the cut-off for severe depression. Finally, 47.7% scored above the cutoff for current hazardous alcohol use, which represented 56.4% of participants who reported they drank alcohol in the past year.
Latent Class Analysis of Assault Types
Summary of the fit statistics for the LCA are reported in Table 2. A “flattening out” in the fit indices occurred after five classes. Specifically, the BIC values for the six-, seven-, and eight-class models were larger than that of the five-class model; at the same time, there were only small decreases in SSABIC from five to eight classes, and small increases in entropy. In addition, examination of the six-, seven-, and eight-class models demonstrated that these models were often splitting one larger class into two smaller classes on the basis of a single assault characteristic. Further, the eight-class model had one class with less than 5% of observations. Thus, the five-class model was retained as the best fit to the data. For the five-class model, the average latent class probabilities for most likely latent class membership ranged from .89 (Class 4) to .98 (Class 3) and for incorrect classification ranged from .00 to .04.
Fit Statistics for LCA Models of Rape Typologies.
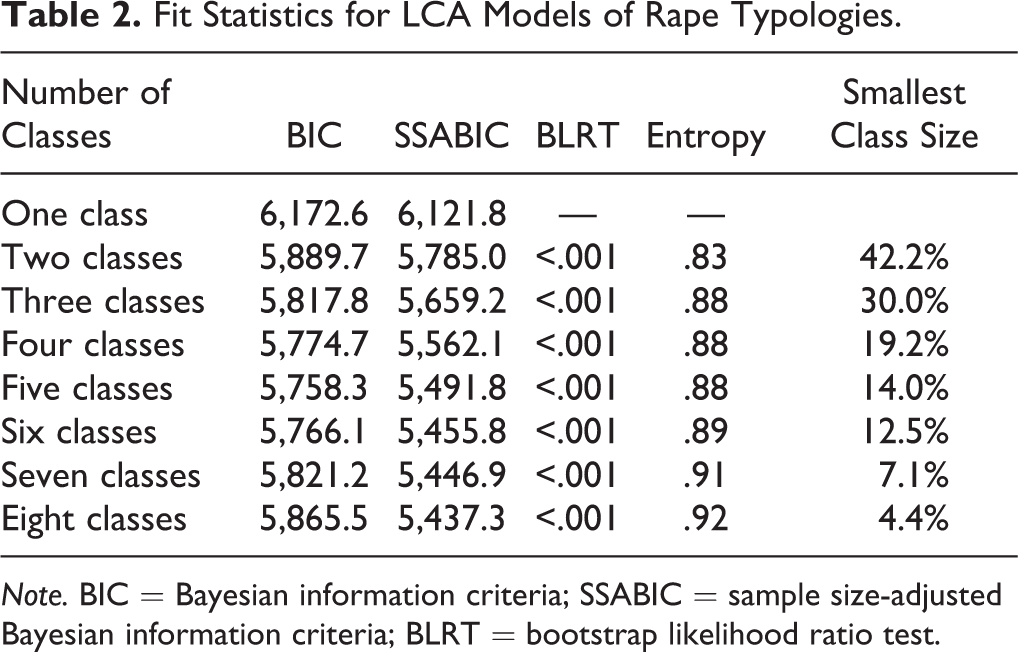
Note. BIC = Bayesian information criteria; SSABIC = sample size-adjusted Bayesian information criteria; BLRT = bootstrap likelihood ratio test.
Next, the bivariate residuals between variables were inspected to assess for possible violations of the assumption of conditional independence. Of the 120 bivariate residuals inspected, 11 were significant, suggesting a possible issue with violations of the assumption of conditional independence. The LCA models were then re-run modeling shared covariances between these 11 pairs of assault characteristic indicators. Results of these analyses were identical to the initial LCA in that the five-class model demonstrated the best fit to the data. Further, the obtained latent classes were largely identical to those obtained in the initial LCA. Thus, the results of the initial LCA were retained given that there was no evidence that the initial LCA model resulted in the over identification of latent classes due to poor model fit indices of models with fewer classes, which is considered the most significant issue if violations of conditional independence occurred (Oberski, 2016).
The item response probabilities of the assault characteristics for the five latent classes are summarized in Table 3 and Figure 1. Class 1 (16.0%, n = 55) “Combined force/substance-facilitated rape” was characterized by the second highest probability of including the different types of force and resistance of all the latent classes, as well as a moderate absolute probability of including binge drinking by the survivor and a high absolute probability of including binge drinking by the perpetrator. This class also had the second highest probability of including survivor impairment of all the latent classes. Finally, assaults in this class had the second highest probability of including survivor drug use, and the highest probability of including drug use by the perpetrator of all the latent classes.
Proportion of Assaults Containing Each Assault Characteristic Stratified by Class Membership.
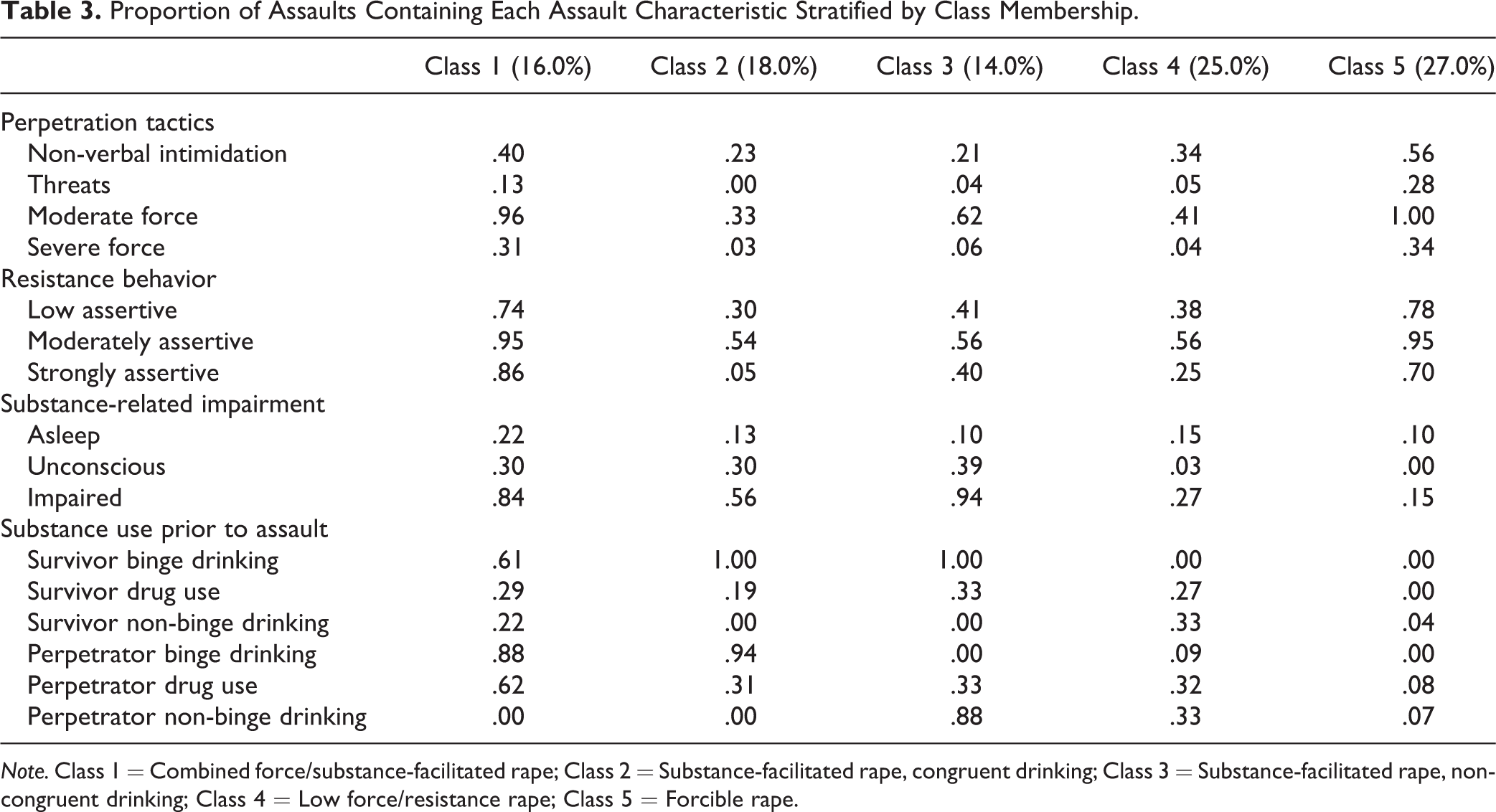
Note. Class 1 = Combined force/substance-facilitated rape; Class 2 = Substance-facilitated rape, congruent drinking; Class 3 = Substance-facilitated rape, non-congruent drinking; Class 4 = Low force/resistance rape; Class 5 = Forcible rape.
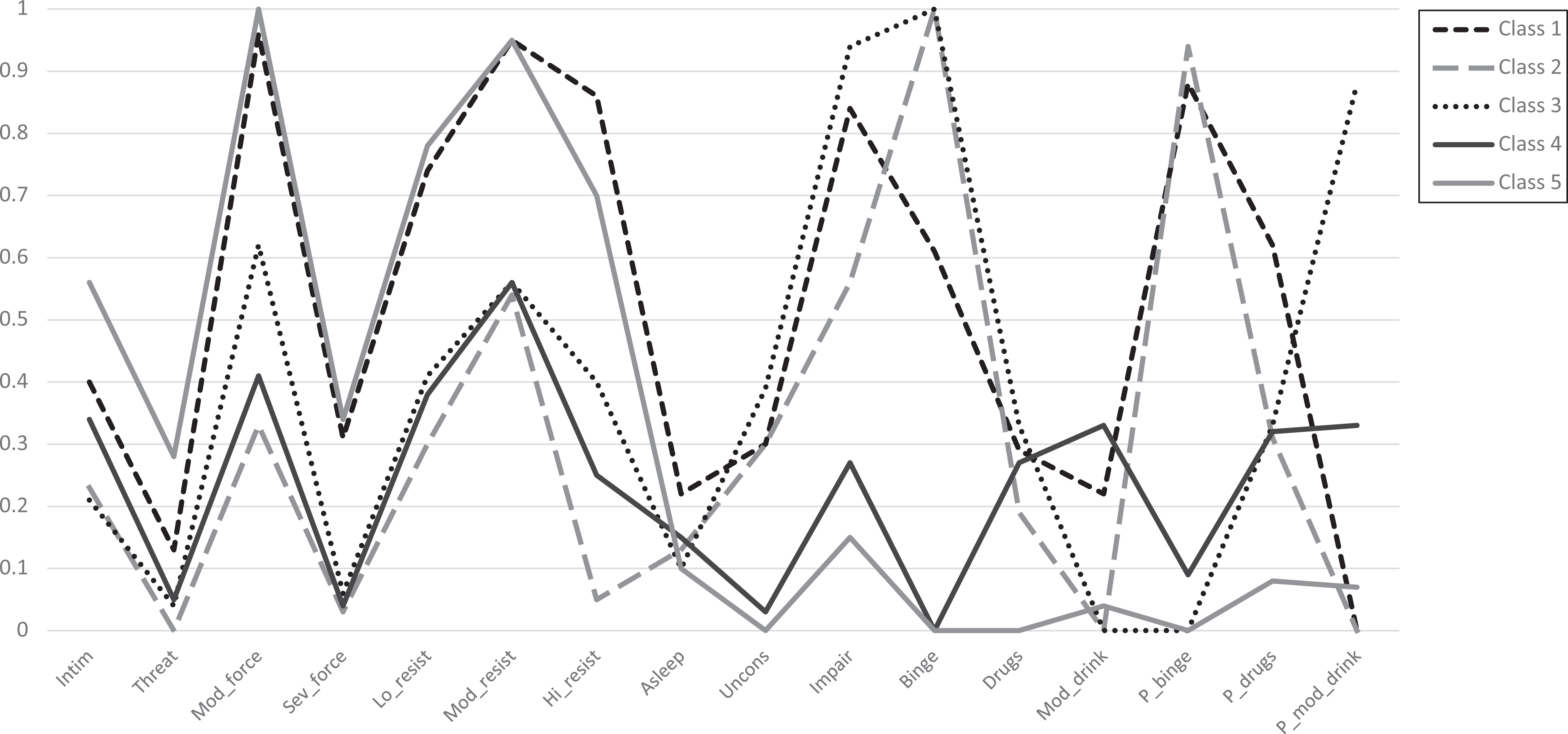
LCA Plot of Rape Typologies.
Class 2 (18.0%, n = 62) “Substance-facilitated rape, congruent drinking” had the highest probability of inclusion of binge drinking by the survivor and perpetrator of all the latent classes. Conversely, it had the second lowest probability of inclusion of drug use by the survivor and perpetrator of all the latent classes. Assaults in this class had a moderate absolute probability of inclusion of survivor impairment and incapacitation. Finally, assaults in this class had the lowest probability of inclusion of the different types of force and resistance of all the latent classes.
Class 3 (14.0%, n = 48) “Substance-facilitated rape, non-congruent drinking” had the highest probability of inclusion of binge drinking and drug use by the survivor, as well as survivor impairment and incapacitation, of all the latent classes. There was a 0% probability of inclusion of perpetrator binge drinking but a high absolute probability of inclusion of perpetrator non-binge drinking. These assaults had a moderately high absolute probability of inclusion of moderate force but a low absolute probability of inclusion of the other types of force tactics. Finally, assaults in this class had a moderately high absolute probability of inclusion of the different resistance tactics.
Class 4 (25.0%, n = 86) “Low force/resistance rape” had a low absolute probability of inclusion of inclusion of the different types of force and resistance tactics. Assaults in this class had a 0% probability of inclusion of binge drinking by the survivor and a very low absolute probability of inclusion of binge drinking by the perpetrator. Conversely, assaults in this class had the highest probability of inclusion of non-binge drinking by the survivor of all the latent classes, and a moderate absolute probability of inclusion of non-binge drinking by the perpetrator. Finally, assaults in this class had the second lowest probability of inclusion of survivor impairment and incapacitation of all the latent classes.
Class 5 (27.0%, n = 93) “Forcible rape” had the highest probability of inclusion of the different types of force of all the latent classes and a high absolute probability of inclusion of the different types of resistance. This latent class had a 0% probability of inclusion of survivor binge drinking, perpetrator binge drinking, and survivor drug use, as well as very low absolute probability of inclusion of survivor non-binge drinking, perpetrator non-binge drinking, and perpetrator drug use. It also had the lowest probability of inclusion of survivor impairment or incapacitation of all the latent classes.
Examination of the odds ratios of the item probabilities between classes supported large separation between classes on multiple indicators. The classes with the most indicators with large separations were Classes 4 (Low force/resistance rape) and 5 (Forcible rape; 11 of 16 indicators), and Classes 2 (Substance-facilitated rape, congruent drinking) and 5 (Forcible rape; 11 of 16 indicators). The classes with the fewest indicators with large separation were Classes 2 (Substance-facilitated rape, congruent drinking) and 3 (Substance-facilitated rape, non-congruent drinking; four of 16 indicators), Classes 3 (Substance-facilitated rape, non-congruent drinking) and 4 (Low force/resistance rape; five of 16 indicators), and Classes 2 (Substance-facilitated rape, congruent drinking) and 4 (Low force/resistance rape; five of 16 indicators). For the remaining comparisons, there was large separation between classes for between six and 10 indicators. Thus, results supported large separation between classes on multiple indicators, indicating adequate power to identify the latent classes.
Multinomial Regression Analyses of Dichotomous Auxiliary Variables
Results of the multinomial regression analyses (see Table 4) supported that membership in Class 3 (Substance-facilitated rape, non-congruent drinking) was associated with lower odds of being an acknowledged victim than Class 4 (Low force/resistance rape) or Class 5 (Forcible rape). Membership in Class 3 (Substance-facilitated rape, non-congruent drinking) was also associated with lower odds of being assaulted by a romantic partner than Class 4 (Low force/resistance rape). Finally, membership in Class 3 (Substance-facilitated rape, non-congruent drinking) was associated with lower odds of having had consensual sex with the perpetrator previously as compared to Class 5 (Forcible rape).
Multinomial Regression Analysis With Dichotomous Auxiliary Variables.
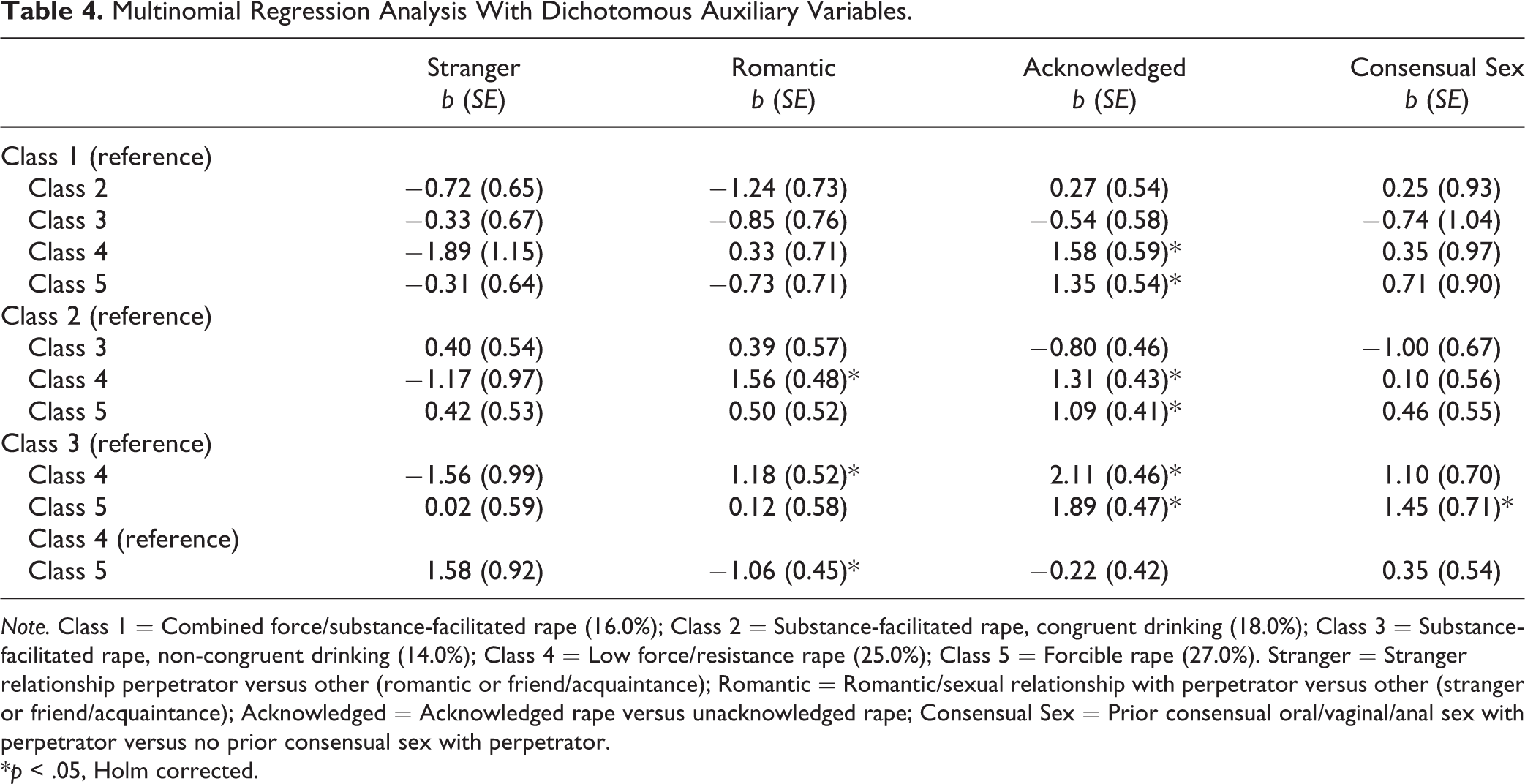
Note. Class 1 = Combined force/substance-facilitated rape (16.0%); Class 2 = Substance-facilitated rape, congruent drinking (18.0%); Class 3 = Substance-facilitated rape, non-congruent drinking (14.0%); Class 4 = Low force/resistance rape (25.0%); Class 5 = Forcible rape (27.0%). Stranger = Stranger relationship perpetrator versus other (romantic or friend/acquaintance); Romantic = Romantic/sexual relationship with perpetrator versus other (stranger or friend/acquaintance); Acknowledged = Acknowledged rape versus unacknowledged rape; Consensual Sex = Prior consensual oral/vaginal/anal sex with perpetrator versus no prior consensual sex with perpetrator.
*p < .05, Holm corrected.
Membership in Class 4 (Low force/resistance rape) was associated with greater odds of acknowledgment than Class 1 (Combined force/substance facilitated rape) or Class 2 (Substance-facilitated rape, congruent drinking). Additionally, membership in Class 4 (Low force/resistance rape) was associated with greater odds of being assaulted by a romantic partner than Class 2 (Substance-facilitated rape, congruent drinking) or Class 5 (Forcible rape). Finally, membership in Class 5 (Forcible rape) was associated with greater odds of acknowledgment than Class 1 (Combined force/substance-facilitated rape) or Class 2 (Substance-facilitated rape, congruent drinking).
BCH Analyses of Continuous Auxiliary Variables
Results of the overall model tests for the BCH analyses (see Table 5) for all three psychological adjustment variables (PSS-SR, DASS-21 depression, AUDIT) were significant. Examining differences in weighted means across pairs of classes supported that membership in Class 4 (Low force/resistance rape) was associated with significantly higher depression and PTSD scores than membership in Class 1 (Combined force/substance facilitated rape), Class 2 (Substance-facilitated rape, congruent drinking), and Class 3 (Substance-facilitated rape, non-congruent drinking). Additionally, membership in Class 3 (Substance-facilitated rape, non-congruent drinking) was associated with significantly lower depression and PTSD scores than membership in Class 5 (Forcible rape).
Results of BCH Auxiliary Analyses With Continuous Variables.
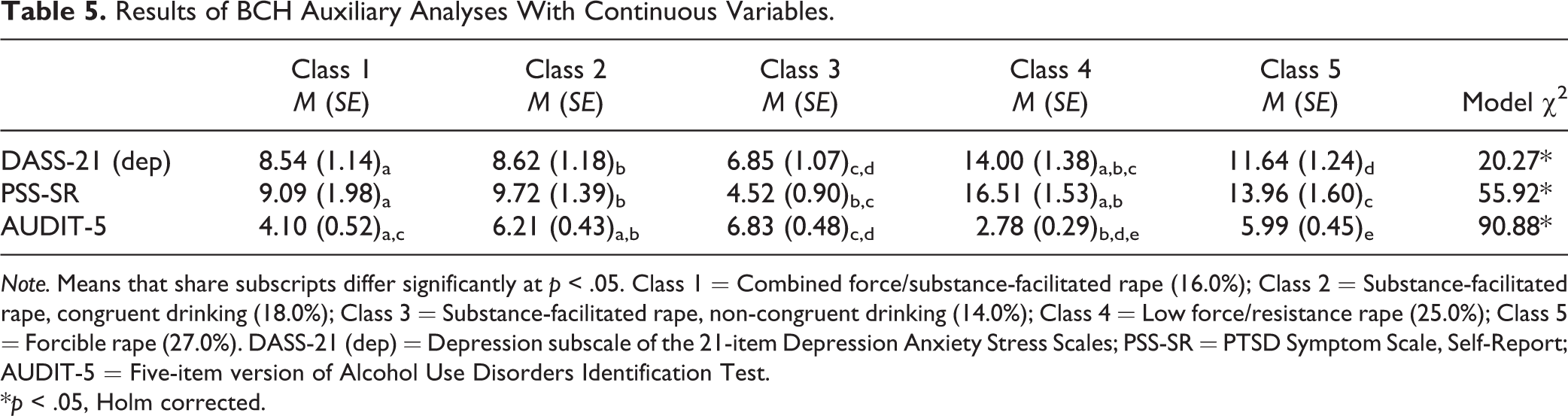
Note. Means that share subscripts differ significantly at p < .05. Class 1 = Combined force/substance-facilitated rape (16.0%); Class 2 = Substance-facilitated rape, congruent drinking (18.0%); Class 3 = Substance-facilitated rape, non-congruent drinking (14.0%); Class 4 = Low force/resistance rape (25.0%); Class 5 = Forcible rape (27.0%). DASS-21 (dep) = Depression subscale of the 21-item Depression Anxiety Stress Scales; PSS-SR = PTSD Symptom Scale, Self-Report; AUDIT-5 = Five-item version of Alcohol Use Disorders Identification Test.
*p < .05, Holm corrected.
As far as hazardous drinking, membership in Class 1 (Combined force/substance-facilitated rape) was associated with significantly lower hazardous drinking scores than membership in Class 2 (Substance-facilitated rape, congruent drinking) and Class 3 (Substance-facilitated rape, non-congruent drinking). Additionally, membership in Class 4 (Low force/resistance rape) was associated with significantly lower hazardous drinking scores than membership in Class 2 (Substance-facilitated rape, congruent drinking), Class 3 (Substance-facilitated rape, non-congruent drinking), or Class 5 (Forcible rape).
Discussion
In the current study, we sought to identify assault typologies experienced by female rape survivors attending college. Further, we evaluated whether there were systematic differences in distress, hazardous alcohol use, and assault correlates among survivors who experienced these different types of assault. We identified five distinct rape type classes using LCA, which differed along a number of key assault correlates, as well as adjustment. Some of the rape type classes found mapped on to prior studies seeking to classify rape and sexual assaults into distinct types, whereas others represented subtypes not previously identified in prior work in this area. Importantly, findings supported the importance of several assault characteristics not previously examined in the literature, including perpetrator substance use (e.g., binge drinking, non-binge drinking, drug use) and survivor resistance behaviors, in differentiating assault types. Further, assault types that previously would have been collapsed into a single category differed in both key correlates and assault outcomes, suggesting prior studies may have missed key differences in the experiences of survivors of these assaults.
First, as hypothesized, substance use–related characteristics of the assaults differentiated several of the assault type classes identified, with 48% of assaults falling into one of the three substance-related assault type classes. Of note, there existed two substance-facilitated assault type classes characterized by a high probability of inclusion of binge drinking/substance-related impairment by the survivor and a low to moderate probability of inclusion of force or resistance in the assault, as well as a combined force/substance-facilitated class characterized by both a high probability of inclusion of binge drinking/substance-related impairment by the survivor and perpetrator and a high probability of inclusion of the different types of force by the perpetrator and resistance by the survivor. This is consistent with McConnell and colleagues (2020) who classified the rape experiences of a community-recruited group of young adults into forcible, substance-facilitated (impaired or incapacitated), and combined forcible/substance-facilitated types. It is also similar to Peter-Hagene and Ullman (2015) who found a combined forcible/substance facilitated assault group (labeled as alcohol-related).
Interestingly, membership in the combined force/substance-facilitated assault type class was associated with lower current hazardous drinking than the other two substance-related assault type classes. One possible explanation of this finding is that survivors of combined force/substance-facilitated assaults may have had less problematic established drinking patterns prior to the rape than survivors of other forms of substance-related assaults, and as such, their current lower hazardous drinking (relative to survivors of other types of substance-related assaults) represents a continuation of their pre-assault drinking pattern. However, pre-assault drinking patterns were not assessed in the current study and so this hypothesis could not be tested. Another possibility is that survivors of this type of assault may be more likely to reduce their drinking behavior post-assault as compared to survivors of other types of substance-related assaults, perhaps because, at least for some, they attributed their inability to effectively stop the assault (despite attempting to do so, as indicated by their having engaged in a number of resistance behaviors) at least in part to their substance-related impairment.
Notably, one of the two substance-facilitated classes was characterized by the highest probability of inclusion of substance-related impairment and incapacitation of the survivor during the assault as well as a 0% probability of inclusion of perpetrator binge drinking prior to the assault (in contrast to the two other substance-facilitated classes which were characterized by a high probability of inclusion of perpetrator binge drinking). In addition, in auxiliary analyses, membership in this assault type class was associated with a lower probability of being assaulted by a romantic partner or having had prior consensual sex with the perpetrator. Membership in this class was also associated with a lower probability of rape acknowledgment than several of the other classes. Overall, this assault type class potentially reflected sexual assaults where a perpetrator with whom the survivor did not have a prior romantic or sexual relationship either purposely intoxicated the survivor to commit the assault (while moderating their own drinking) or took advantage of her incapacitated or highly impaired state (such as when the survivor passed out or fell asleep after drinking at a party or bar) to commit the assault. Of note, some of these findings paralleled those of Littleton, Grills-Taquechel, and Axsom (2009) who found that survivors who were incapacitated from substance use during the assault were significantly less likely than non-impaired survivors to have been assaulted by a romantic partner.
As hypothesized, two force-related assault type classes also emerged. The first of these, the “forcible rape” type class had a high probability of inclusion of all the types of perpetrator force and survivor resistance and a low to zero probability of inclusion of binge drinking by the survivor and perpetrator and thus was highly similar to the forcible rape type identified in prior research with college and non-college samples (e.g., Masters et al., 2015; Peter-Hagene & Ullman, 2015; Zinzow et al., 2010). As hypothesized, membership in this assault type class was associated with a high probability of acknowledging the rape. The second forcible assault type class was the “low force/resistance” class and had a low probability of inclusion of all the forms of force and resistance, a low probability of inclusion of binge drinking by the survivor and perpetrator, a moderately high probability of inclusion of non-binge drinking by the survivor and perpetrator, and a low probability of inclusion of substance-related impairment or incapacitation by the survivor. Membership in this class was associated with the highest probability of being assaulted by a romantic partner and a high probability of acknowledging the rape as compared to several of the other assault type classes.
Inconsistent with the hypothesis that assaults associated with the highest probability of inclusion of severe physical force would be associated with the highest level of distress, membership in the low force/resistance class was associated with the highest levels of depression and PTSD symptoms as compared to the other assault type classes, not membership in the forcible rape class, although it should be noted that there were no significant differences in depression and PTSD between these two force-related classes. The low force/resistance class appeared to represent incidents where the survivor was assaulted by someone with whom she likely had an ongoing romantic relationship, in a situation where neither she nor the perpetrator had been drinking heavily or were impaired by substances. As such, survivors of this type of assault were likely able to engage in resistance behavior, had a clear memory for the incident, and could not attribute the perpetrator’s behavior to his heavy use of substances. These three factors likely accounted for the association of membership in this class with acknowledging the assault. Further, it seems possible that feelings of being betrayed by a trusted individual (e.g., a romantic partner) may have in part accounted for the association of membership in this class with the highest level of depression and PTSD symptoms (Kelley et al., 2012). It also seems probable that for some survivors of this type of assault, the rape occurred within the context of other forms of relationship abuse/violence (Kennedy et al., 2018), which may further explain the association of membership in this class with elevated depression and PTSD symptomology, as well as the high probability of acknowledgment. However, this possibility could not be evaluated in the current study as other forms of relationship violence experiences were not assessed.
Limitations
This study is not without its limitations. The LCA conducted in the current study was exploratory. Thus, it will be important to replicate these findings in future studies. Another limitation of the current study was the use of a cross-sectional design, which makes it difficult to draw conclusions regarding differences in adjustment trajectories and outcomes among women who experienced different assault types. Additionally, participants were predominately White and heterosexual cisgender women, which precluded examination of the extent to which racial/ethnic/gender and sexual minority status is associated with risk for the different types of rape. In addition, the study only examined the experiences of women who experienced completed rape and did not include the experiences of women who experienced other forms of sexual assault (e.g., attempted rape) or other forms of non-consensual sex (e.g., coercion).
It also should be noted that many women’s experiences likely occurred prior to their enrollment in college, and it is not known whether the same assault types or same frequency of assault types would have been found if the study focused only on rape experiences that occurred while in college. It is also not known whether there were systematic differences in time since assault across assault types. Relatedly, participants were queried to describe their “worst” assault if they had experienced multiple assaults, and as such, certain rape typologies might have been over- or underrepresented in the sample. Finally, assault characteristics were retrospectively assessed via self-report, and thus, it is not known the extent to which recall bias affected women’s reports of the characteristics of their assault, which may be particularly salient for women whose recall may have been negatively affected by substance use at the time of the assault.
Practice Implications
Results have several implications for practitioners working with survivors of rape in adolescence and college, as well as those seeking to develop prevention programming for this population. For one, practitioners seeking to understand the experiences of rape survivors should consider discussing multiple aspects of their assault experience, including substance use by both the survivor and perpetrator(s), as well as the survivor’s resistance behaviors. Having this fuller picture of the survivor’s assault experience could be helpful in identifying potential barriers to recovery, such as feelings of betrayal, self-blame for not resisting or for not resisting more forcefully, and anger/blame toward the perpetrator. Relatedly, practitioners may wish to be mindful of the possibility that there are multiple typologies of sexual assault experienced by adolescent and young adult survivors. As such, they should be careful not to presume that an assault that involved heavy substance use also did not involve the use of physical force by the perpetrator, for example. As another example, practitioners should be mindful that assaults that do not involve more severe violence (e.g., physical force and resistance) can still have a lasting mental health impact on survivors. As far as prevention programming, the different patterns of perpetration tactics, resistance behaviors, and substance use by the survivor and perpetrator identified in the current study suggest a need to develop targeted programming to address these multiple typologies, including ones that may not be adequately addressed in extant programs, such as assaults that occurred following heavy alcohol use by both the survivor/perpetrator and assaults where the perpetrator used less forceful strategies to perpetrate an assault against someone with whom they were involved in an ongoing relationship.
Research Implications and Future Directions
Bearing the study’s limitations in mind, findings of the current study reinforce the need for continued attention to assessment of multiple characteristics of a sexual assault experience, beyond the presence of physical force and survivor substance use or impairment, including substance use by the perpetrator and resistance behaviors by the survivor. Due to the decontextualized assessment of rape characteristics in some prior work, less is known about how different aspects of the assault, including the presence of multiple perpetration tactics, survivor resistance behaviors, and perpetrator substance use co-occur and predict outcomes among survivors. Results supported that assaults which previously may have been collapsed into a single type (e.g., involving use of physical force by the perpetrator) may represent multiple distinct types of assault experiences associated with different outcomes. Future work should continue to examine these different assault types including additional assault outcomes and correlates of these typologies, such as survivor self-blame, stigma, betrayal, other trauma history, and other risky behaviors (e.g., risky sexual behavior, drug use). It is also critically important for future research to examine the impact of experiencing these different types of sexual assaults on adjustment and revictimization risk longitudinally, particularly given the association of assault type class membership with hazardous drinking and psychological distress.
In addition, the current study included rapes that occurred prior to and during college. Future work should seek to evaluate whether there are differences in the assault types or the frequency of assault types experienced by women during adolescence as compared to during college. Relatedly, future work may seek to utilize LCA to examine different types of sexual assault (e.g., attempted rape), as well as evaluate other forms of unwanted sexual experiences (e.g., coercion). Similarly, future studies may seek to enrich quantitative findings with qualitative studies of survivors’ narratives of their sexual assault experiences. Future work in these areas will serve to enhance our understanding of the diversity of experiences of college survivors of rape and other forms of unwanted and non-consensual sexual experiences, as well as develop targeted and effective prevention and intervention strategies for this at-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.