
Abstract
While strength and balance training (SBT) programs are effective in preventing falls, older adults rarely participate. A cross-sectional study design was used to explore factors that influence their decisions to attend SBT programs. Questionnaires were collected that measured theory of planned behavior constructs from 221 community-dwelling Taiwanese older women between the age of 55 and 94. Results suggest that (a) benefits of SBT programs such as increasing independence in daily life, (b) participation approval and involvement from the older adults’ family members, and (c) SBT programs conducted in familiar places strengthened potential participants’ positive attitude, subjective norm, and perceived behavioral control, respectively. Health care professionals should consider incorporating these factors in the recruitment materials or the actual design of SBT programs to enhance older adults’ decision to attend and increase the recruitment rate of such programs.
According to the National Health Research Institutes (2007) in Taiwan, the prevalence of falling adjusted for age and sex rose from 18.7% in 1999 to 20.5% in 2005; furthermore, 84% of those who fell had one injury, and 15% of them had multiple injuries. Falls and fear of falling are often linked to restricted mobility, limited independence, and distress that may result in social alienation and increased utilization of health care and social services (Yardley, Donovan-Hall, Francis, & Todd, 2007). The majority of older adults do not realize their potential risk for falling and neglect to report falling to their physicians (American Geriatric Society, British Geriatric Society, & American Academy of Orthopaedic Surgeons Panel on Falls Prevention, 2001; Aronovitch, 2006; Hanson, Salmoni, & Doyle, 2009). Wiens, Koleba, Jones, and Feeny (2006) reported that less than two thirds of respondents felt that they were personally at risk for falls. Older adults who were informed of their risk for falling, however, were more likely to perform fall risk reduction behaviors such as having their vision checked, attending exercise programs, and eating a calcium-rich diet (Ness, Gurney, & Ice, 2003). Yardley et al. (2006) also conducted interviews to inquire about older adults’ views of fall prevention strategies and found that older adults in six European countries were motivated to attend fall prevention programs because of a range of perceived benefits (e.g., enjoyment and independence) and not just reduction of fall risks.
Strength and balance training (SBT) programs are intended to reduce older adults’ risk of falling through exercises that increase lower-extremity muscle strength and improve postural control (Yardley et al., 2007). Many studies have reported that performance of SBT programs can reduce risk and fear of falling and ultimately improve balance abilities among older adults (American Geriatric Society et al., 2001; Li et al., 2001). Yet the effectiveness of these programs depends on the rate of participation. Yardley et al. pointed out that more than half of participants in several studies refused to join SBT programs when they had opportunities to do so. Challenges for older adults to attend physical activity programs have been noted in several qualitative studies. These challenges include lack of time, the aging process, and an adverse environment (Grossman & Stewart, 2003); pain and effort (Simpson, Darwin, & Marsh, 2003); and low confidence in physical abilities (Stead, Wimbush, Eadie, & Teer, 1997). McInnes and Askie (2004) further reported a number of factors that may impede older adults’ participation to fall prevention intervention that includes SBT activities: (a) low perceived personal relevance of fall prevention, (b) unfamiliarity with the term “fall prevention,” (c) social stigma attached to the program that targets “old people,” (d) increased pain and effort in relation to the exercise program, and (e) low health expectation and low confidence in physical activities.
Other barriers to attending physical activity programs suggested by the National Council on Aging (2006) encompassed (a) reluctance to be tied down to a weekly program, (b) feeling uncomfortable in an unfamiliar environment, (c) having no friend or family members who participate in physical activities, (d) program cost, and (e) transportation problems. Taiwanese older adults reported similar challenges and the common themes between Western and Taiwanese older adults include (a) fear of increased painful symptoms, fatigue, and injury, (b) perceived poor health or physical limitations, and (c) lack of exercise companion. Taiwanese older adults also reported that environmental barriers such as no available space to exercise and terrible traffic conditions were factors that made exercise difficult (Lin, Huang, Young, & Chen, 2007).
Previous research on older adults’ perceptions regarding SBT programs and intentions to attend such programs were limited to the qualitative studies mentioned previously; thus, it is important to quantitatively assess older adults’ attitudes and beliefs regarding SBT programs and examine how these perceptions relate to their intentions to participate in such programs. Though men generally are less likely to seek preventive health services (Williams, 2005) and attend health promotion programs (Engelhardt, Ahn, Cho, & Joung, 2007; Lieberman, Meana, & Stewart, 1998; Senn, Carey, Vanable, Coury-Doniger, & Urban, 2007), Yardley et al. (2007) found women and older respondents were slightly less inclined to participate in SBT programs. Therefore, it is important to focus the investigation on the attitudes and beliefs of older adult women regarding SBT programs and to examine how these relate to intentions to participate in such programs.
Theoretical Framework
We used the framework of Ajzen’s (1991) theory of planned behavior that has been shown to have efficacy in predicting a wide range of health-related behaviors such as smoking (Higgins & Conner, 2003), dieting (Nejad, Wertheim, & Greenwood, 2004), and exercising (Rhodes & Blanchard, 2006). In Ajzen’s theory, an individual’s behavior can be directly predicted by intention that, in turn, is predicted by attitude toward the behavior, subjective norm (perceived social pressure regarding the specific behavior), and perceived behavioral control (perceived ability to perform the behavior). Perceived outcomes of the behavior (behavioral beliefs) and evaluation of these outcomes determine the attitude. Subjective norm is influenced by expectations about what referent others want individuals to do (normative beliefs) and individuals’ motivation to comply with referent others. Perceived behavioral control is determined by perceived presence of factors that facilitate or hinder the action (control beliefs) and the perceived importance of each of these factors (perceived power). Perceived behavioral control can also directly predict an individual’s behavior if perceived control matches actual control. In general, with more favorable attitude and subjective norm, and greater perceived behavioral control, intention to perform the behavior will be stronger (Ajzen, 2006).
The purpose of the study was to explore the attitudes and beliefs of Taiwanese older women regarding SBT programs and how those beliefs affect their intentions to attend such programs within the framework of the theory of planned behavior. We also examined how age relates to participants’ perceptions and intentions to attend SBT programs.
Method
Participants
Participants were older adult Taiwanese students who attend the Taiwan Silver College of Presbyterian Church—Suang Lien Branch—which provides education to individuals who wish to learn in later life. The administrator of the study site distributed the flyers for the study and encouraged participation. Flyers advertising the study were also posted in the classrooms. All students from the study site who wished to participate were given questionnaires; however, they were only included in the analysis if they were cognitively intact and aged 55 or older. The age of 55 was chosen because this is the minimum age of the school enrollment.
A total of 346 respondents participated in the study. Five participants were eliminated because they had cognitive scores on the AD8 (see instrument section) exceeding 1 and thus lacked adequate cognitive abilities. Participants who responded to less than 80% of questions in the questionnaire were also eliminated. Of those remaining, participants were eliminated if they responded to less than half of the questions in any section measuring the theory of planned behavior construct, balance-maintaining confidence, or demographics. This left 248 participants. The remaining missing data were imputed with the expectation maximization (EM) algorithm in the SPSS 16 missing-data module. Among included participants, 26 (10.5%) were men, 221 (89.1%) were women, and 1 did not report gender. Because the small sample for men made comparison difficult, we decided to include only women in the analysis. The final data set consisted of 221 Taiwanese older women.
Characteristics of participants
The average age of a participant was 72 (SE = 0.56). High school or higher degrees were held by 80% of the participants. Most were married (58.4%) or widowed (35.3%). Buddhists (54.8%) and Christians (23.1%) were the most well-represented religious groups. Since the study site is a Christian-based institution, Christians are overrepresented when compared to the 4.1% of Christians living in Taiwan (Chen, 2008). Finally, the majority of the participants perceived their health status as fair (61.1%) or good (23.1%).
Instruments
A two-stage protocol suggested by Ajzen (2006) was followed to construct the questionnaire. First, a set of nine open-ended questions were used to elicit positive, negative, and neutral behavioral, normative, and control beliefs regarding the attendance of SBT programs. An example of the open-ended positive behavioral belief question is, “What do you believe are the advantages of attending SBT programs?” A negative normative belief question is, “Are there any individuals or groups who would not approve your attendance at SBT programs?” A neutral control belief question is, “Are there any other issues that come to mind when you think about the difficulty of participating in an SBT program in the next six months?” A convenience sample of 12 older adult students (6 men and 6 women) in 2 focus groups responded to these questions. Subsequently, results of a content analysis on responses to the focus group questions were used to compose behavioral, normative, and control belief questions in the questionnaire. For example, the focus group respondents indicated that one of the advantages of the SBT program is that it might help them become more independent on their daily tasks; thus, we asked participants to rate the following behavioral belief statements: (a) “My attendance at an SBT program in the next six months will help me become more independent on my daily tasks” (1 = extremely unlikely, 8 = extremely likely), and (b) “Becoming more independent on my daily tasks is . . .” (1 = extremely bad, 8 = extremely good).
In the second stage, the questionnaire was created. It consisted of four major sections: (1) the AD8 (Galvin et al., 2005) used to screen for participants’ cognitive ability, (2) a theory of planned behavior section including semantic differential scales and Likert-type scales to evaluate theory of planned behavior variables regarding attending an SBT program, (3) the Activities-Specific Balance Confidence Scale-Chinese (Mak, Lau, Law, Cheung, & Wong, 2007), and (4) a general section regarding participants’ demographic characteristics, falling history, and SBT/Tai-Chi exercise attendance. The ABC-C scale assesses individuals’ confidence in performing 16 activities of daily living without losing their balance or becoming unsteady. A higher score indicates greater confidence in maintaining balance. Cronbach’s alpha was .97 in our sample.
The questionnaire was pilot-tested on a convenience sample of 15 students from the study site. Respondents were asked to provide comments regarding the format and content of the initial questionnaire. The questionnaire was finalized according to these suggestions. The questionnaire was first written in English and translated into Chinese. We implemented the back translation process described in Jones, Lee, Phillips, Zhang, and Jaceldo (2001) to ensure the clarity and equivalence of translated contents. It took participants about 35 to 40 min to complete the final 18-page questionnaire.
Theory of Planned Behavior Assessment
Intention to attend SBT programs
Intention was measured with three Likert-style items, for example, “I intend to attend an SBT program in the next 6 months if there is an opportunity” (1 = strongly disagree, 8 = strongly agree). The intention score was calculated by the mean of all complete intention items. Figure 1 shows a general structure of the theory of planned behavior. Intention scores represented by the rightmost panel (intention to attend SBT programs) can be predicted by participants’ scores on attitude, subjective norm, and perceived behavioral control. Cronbach’s alpha was .91 in our sample.

A path diagram that depicts how theory of planned behavior constructs relate to intention to attend SBT programs N represents numbers of participants with complete data. For explanation of the derivation of the r and β in these regressions, see the analysis section.
Attitude
Attitude, subjective norm, and perceived behavioral control toward SBT programs were assessed with either semantic differential scales or Likert-type scales. Ajzen (2006) specified two types of attitude items: instrumental (usefulness of the specific behavior), and experiential (feeling toward the behavior); for example, instrumental attitude: “Attending an SBT program is . . .” harmful (1) to beneficial (8), and experiential attitude: “Attending an SBT program is . . .” unenjoyable (1) to enjoyable (8). Cronbach’s alpha was .96 in our sample.
Subjective norm
Subjective norm has two dimensions: injunctive (whether referents approve or disapprove of the behavior) and descriptive (whether referents themselves engage in the behavior); for example, injunctive norm: “Most people who are important to me think I should participate in an SBT program” (1 = strongly disagree, 8 = strongly agree), and descriptive norm: “People who are important to me would participate in an SBT program themselves if they need it” (1 = strongly disagree, 8 = strongly agree). Cronbach’s alpha was .92 in our sample.
Perceived behavioral control
There are also two dimensions for perceived behavioral control: perceived capability (perceived difficulty in performing the behavior) and controllability (one’s belief about their control over the behavior); for example, perceived capability: “For me to participate in an SBT program would be . . .” impossible (1) to possible (8), and controllability: “How much control do you believe you have over participating in an SBT program?,” no control (1) to complete control (8). Cronbach’s alpha was .91 in our sample.
Five items were generated for each of the 2 dimensions of attitude (10 items total), and 3 items were generated for each of the 2 dimensions of subjective norm (6 items total) and for each of the 2 dimensions of perceived behavioral control (6 items total). The mean across the completed attitude, subjective norm, and perceived behavioral control items were calculated creating a total of three scales. In Figure 1, attitude, subjective norm, and perceived behavioral control scores represented by the middle panel serve as predictors of intention and were predicted by their corresponding beliefs.
Behavioral beliefs
Salient belief items were generated from focus groups and measured with 8-point, Likert-type scales. For each behavioral belief outcome, behavioral belief strength and outcome evaluation were assessed; for example, behavioral belief strength: “My attendance of an SBT program in the next six months will reduce my risk of falling” (1 = extremely unlikely, 8 = extremely likely), and outcome evaluation: “Reducing risks of falling is . . .” (1 = extremely bad, 8 = extremely good).
Normative beliefs
The assessment of normative and control belief follows the same pattern. Normative belief for a particular referent involved normative belief strength and motivation to comply. A normative belief strength example is: “My family thinks that I (1 = should not, 8 = should) participate in an SBT program. A motivation to comply item is, “When it comes to participating in an exercise program, how much do you want to do what your family thinks you should do (1 = not at all, 8 = very much)?
Control beliefs
Control belief involved the likelihood of a facilitator or inhibitor occurring (control belief strength) and the perceived power of the facilitator or inhibitor to ease or hinder attendance at an SBT program. For example, a control belief item is, “I expect that I would be able to perform strength and balance training exercises in a group setting where I could be around my peers” (1 = strongly disagree, 8 = strongly agree). A perceived power item is, “Being able to perform strength and balance training exercises in a group setting where I could be around my peers would make it. . .” (1 = much more difficult, 8 = much easier). The belief scores are represented by the leftmost panels in Figure 1, and they were used to predict their corresponding attitude, subjective norm, and perceived behavioral control.
Data Collection and Procedures
The study was approved by the Institutional Review Board at Loma Linda University. Questionnaires were administered to all potential participants. Data collection occurred at the Silver College site. On the date of data collection, the principal investigator presented a lecture focused on healthy eating and followed by an introduction of the study and guidance on informed consent completion. Subsequently, participants were presented with the definition of an SBT program (this was also available on the questionnaire itself), and photos of older adults demonstrating SBT exercises were shown on a slide to allow participants to understand what an SBT program would entail. Participants were given approximately an hour to complete the questionnaire, and they were allowed to temporarily or permanently withdraw from the study if they felt uncomfortable during data collection. All participants completed the questionnaire before the allotted time. Individuals who completed the questionnaire earlier were permitted to leave and drop off their questionnaires on the podium.
Data Analysis
Multiple linear regressions were used to assess the correlation among intention, the primary theory of planned behavior variables (attitude, subjective norm, and perceived behavioral control), and their respective belief items. Age was added as a control factor to the regression in which intention was explained by the three primary variables of theory of planned behavior. Interactive effects of age and attitude, subjective norm, and perceived behavioral control were modeled with centered product terms. Finally, Pearson’s correlations of intention with age, ABC-C (balance-maintaining confidence) scores, attitude, subjective norm, and perceived behavioral control were calculated.
For each behavioral belief, separate linear regression analyses were conducted to explore how attitude relate to each individual belief item. For each behavioral belief, attitude was regressed on the behavioral belief (BB), its outcome evaluation (OE), and the interaction (BB × OE). The same procedure applies to subjective norm and perceived behavioral control. Subjective norm was regressed on normative belief, motivation to comply, and the interaction term of a particular belief. Perceived behavioral control was regressed on control belief, perceived power, and the interaction term of a particular belief. An example of the regression equation in which attitude was regressed on the first behavioral belief/outcome evaluation (BB/OE) combination could be written:

A second regression of the same form would occur for the second BB/OE combination, then another regression for the third set and so on, until each BB/OE combination predicting the attitude had been examined. Thus, there were eight regression equations for attitude since there were eight behavioral beliefs.
To assess the independent prediction of attitude from each BB/OE pair, the predicted value of attitude based on each BB/OE pair was calculated for all participants, and then attitude was regressed on the eight predicted values. Assessment of the independent prediction of subjective norm and perceived behavioral control from each corresponding belief pair followed the same procedure. A p value of .05 or lower was considered significant for all statistical tests conducted in the study.
Results
Falling History, Balance-Maintaining Confidence, and SBT/Tai-Chi Program Attendance
Most participants (65.6%) reported no falls during the past year, and 18.6% and 11.3% of participants had fallen once and twice, respectively. On a scale of 0% to 100%, participants scored an average of 73.3% for ABC-C scores (balance-maintaining confidence; SE = 1.36). By way of comparison, Mak et al. (2007) found the mean balance-maintaining confidence score to be 71.6% among community-dwelling older adults in Hong Kong. Finally, a large proportion of participants had never engaged in SBT exercises (81.4%) or Tai-Chi exercises (81.9%).
Differences Between Study Sample and Those Lost Because of Missing Data
We examined demographic differences between the female participants dropped because of missing data (n = 57) and those remaining in the sample (n = 221). There were no statistically significant differences regarding education level, marital status, falling history, SBT program attendance (yes/no), Tai-Chi exercise attendance (yes/no), general health status, and the past month family income. Age and religious practice, however, were different between the two groups. Compared to the individuals analyzed, those who were eliminated because of missing data were older (M = 76.5 years vs. 72.2, p < .0005) and more likely not to practice any religion (11.4% vs. 2.8%, p < .05). Individuals who are older might have more physical and mental limitations. These limitations might lead to difficulties in completing the questionnaire and, thus, make a person more likely to be eliminated. We also examined whether the amount of missing data in the final data set was related to participant’s cognitive ability among those who passed the cognitive screening. The result of an independent sample t test showed that the number of missing data was not significantly different between those who had no cognitive impairment (AD8 score = 0, n = 47) and those who had one cognitive impairment (AD8 score = 1, n = 174). Thus, participants’ cognitive ability did not have significant influence on the number of questions being answered.
Intention
Participants’ intentions to attend SBT programs were quite strong, 6.4 on a scale of 8. As shown in Figure 1, each of the three theory of planned behavior constructs significantly and positively correlated with participants’ intentions to attend SBT programs. The strongest of the associations was perceived behavioral control with intention. Figure 1 also summarizes the regression of intention on attitude, subjective norm, and perceived behavioral control. Together these explained 45% of variance in participants’ intention to attend SBT programs. Each of the three associations remains significant when the standardized regression coefficients (β) were examined. Additionally, it was found that the ABC-C (balance-maintaining confidence) score was positively correlated with intention to attend SBT programs (r = .28, p < .001). When intention was regressed on ABC-C scores and theory of planned behavior variables, the association between intention and the theory of planned behavior variables remained significant; however, the association between ABC-C scores and intention disappeared.
Addition of Age to Model
Perceived behavioral control was the only theory of planned behavior variable that had significant association with age (r = −.14, p = .034). As the women’s age increased, their perceived behavioral control tended to decline. We also regressed intention on age, attitude, subjective norm, perceived behavioral control, and the interactions of age with the three theory of planned behavior variables (Table 1). Attitude, subjective norm, and perceived behavioral control retained their positive correlation with intention even with the addition of the age variable, but age did not show any significant independent association with intention. Age interacted with subjective norm, which is illustrated in Figure 2. Subjective norm was not associated with intention for the older women, but greater subjective norm was correlated with stronger intention among younger women.
Intention as a Function of Age, Attitude, Subjective Norm, Perceived Behavioral Control, and Interactive Effects Between Age and Theory of Planned Behavior Variables
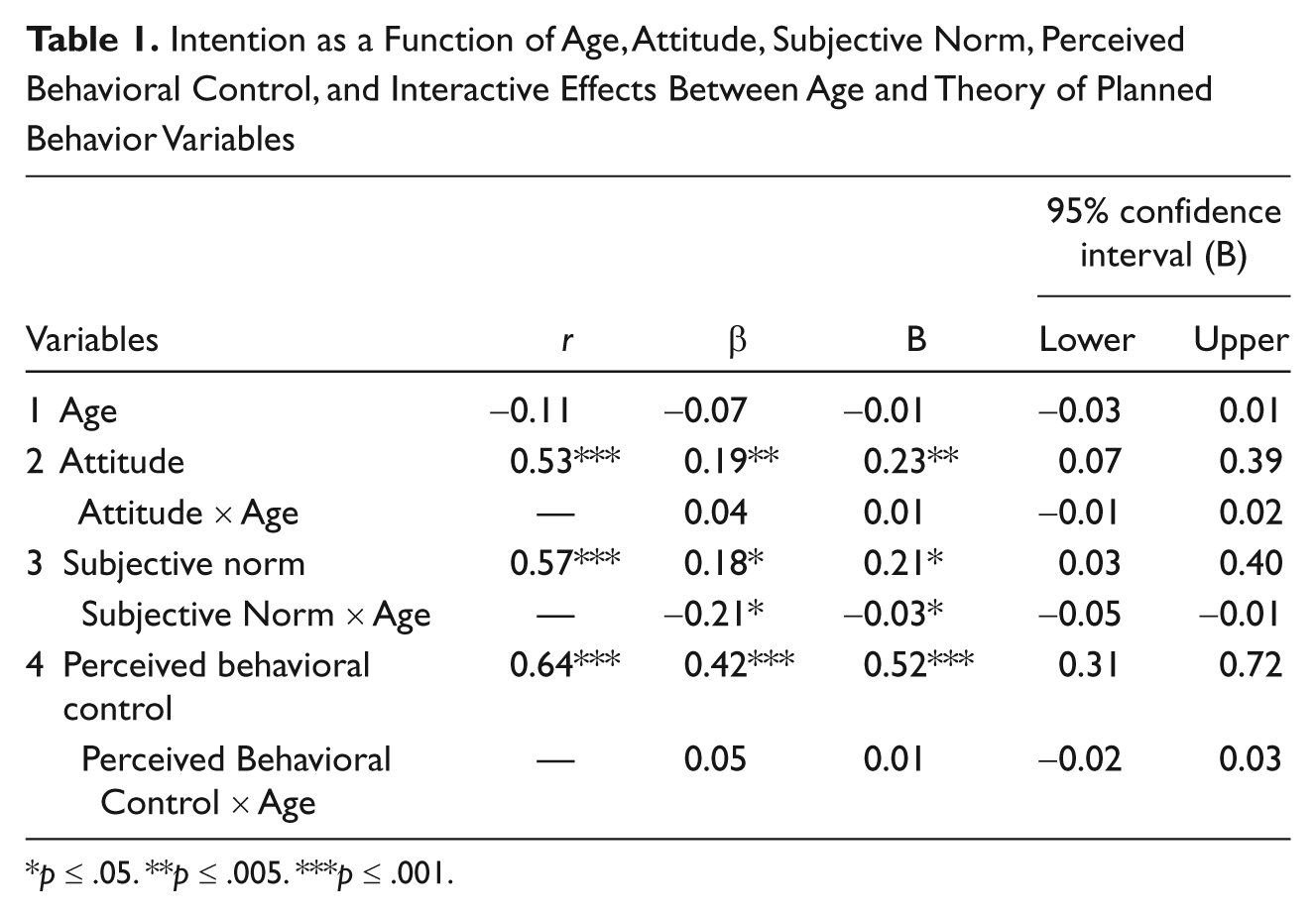
p ≤ .05. **p ≤ .005. ***p ≤ .001.
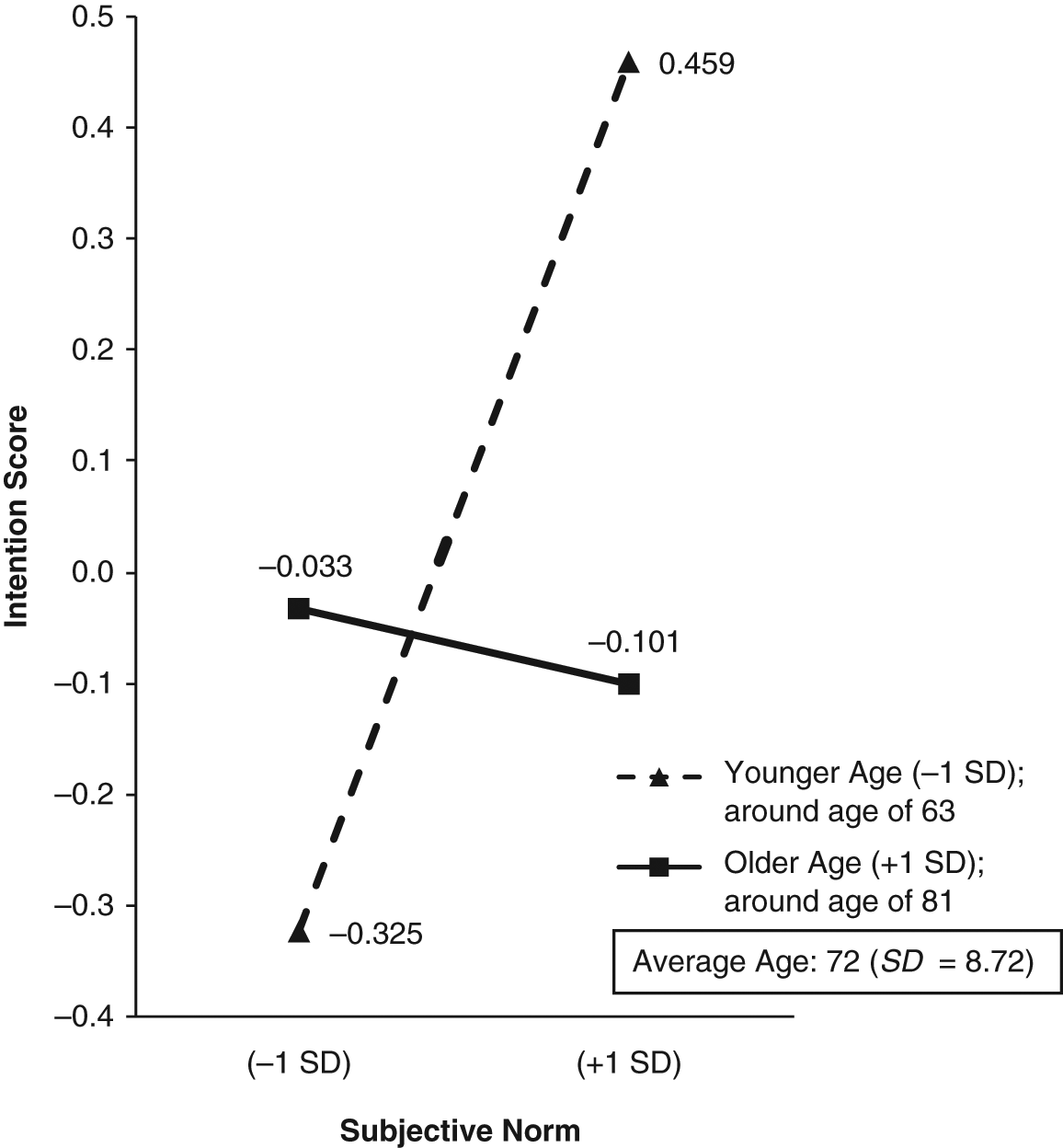
The interactive effect between age and subjective norm in prediction of participants’ intention to attend SBT programs
Behavioral Belief and Outcome Evaluation
Figure 1 also shows the regression of attitude on the eight outcome beliefs. These outcomes collectively explained 44% of variance in participants’ attitude toward SBT programs. All outcome beliefs were significantly and positively correlated with attitude. Becoming more independent in their daily life, however, was the only outcome that predicted participants’ attitude when all predicted beliefs were entered in a regression equation simultaneously.
Normative Beliefs and Motivation to Comply
Subjective norm was regressed on five referent groups examined in the study (Figure 1). These referents collectively explained 56% of variance in participants’ subjective norm. While all referent groups had significant positive associations with subjective norm, only family and doctors had independent prediction of participants’ subjective norm.
Control Belief and Perceived Power
Perceived behavioral control was regressed on the eight control beliefs assessed in the study (Figure 1). All control beliefs together accounted for 59% of variance in participants’ perceived behavioral control. While all control beliefs were significantly and positively correlated with perceived behavioral control, only three control beliefs had independent prediction of perceived behavioral control. Performing SBT exercises in a familiar place predicted perceived behavioral control most strongly, followed by participants’ being able to control the amount of exercise desired and participants having enough willpower to complete the program.
Discussion
Participants in this study had fairly strong intentions (average intention is 6.4 on an 8-point scale) to attend an SBT program. This was consistent with what Yardley et al. (2007) found. Participants in their study had a median intention score of 6 on a 7-point scale to attend the SBT program. The behavioral intention shows an individual’s readiness to engage in a specific behavior. In the theory of planned behavior, intention is considered as the most immediate antecedent of behavior (Ajzen, 1991). Rhodes et al. (1999) indicated in their review article that exercise intention is a consistent predictor of exercise behavior, and they estimated that exercise intention explained 30% of variance in exercise behavior. Thus, we could expect that a high level of exercise intention will translate into at least some increased rate of participations in SBT programs among the study participants if the SBT program is available and recognized by them. Although there are free and available SBT programs throughout most of the counties in Taiwan, all of the focus group participants indicated that they have never heard about the program. This indicates that marketing of the SBT program plays an important role of program participation.
In addition, we also found that attitude, subjective norm, and perceived behavioral control collectively explained 45% of variance in participants’ intentions to attend SBT program—similar to what Armitage and Conner (2001) found in their meta-analytic review. They reported that attitude, subjective norm, and perceived behavioral control accounted for 39% of variance in intention. More specifically, Rhodes and Blanchard (2006) indicated that attitude and perceived behavioral control together explained 40% of variance in intention to perform exercise.
Attitude, subjective norm, and perceived behavioral control all provided significant influences on participants’ intentions to attend SBT programs. Intention was most strongly predicted by perceived behavioral control, followed by subjective norm and attitude. Unlike previous research, attitude assessed in this study did not produce a very strong association with older adults’ intention to attend an SBT exercise program. Gravelle, Paré, and Laurencelle (1997) found that attitude explained 73.3% of exercise intention among active older adults. The higher predictive power of perceived behavior control found in this study, however, was consistent with Rhodes et al. (1999) who indicated that research using the theory of planned behavior to assess exercise adherence generally found that perceived behavioral control added slightly more explained variance to intention than either attitude or subjective norm.
Additionally, participants’ ABC-C scores (balance-maintaining confidence) was positively associated with their intention to attend SBT programs. Possibly individuals who have high balance-maintaining confidence (indicative of low perceived susceptibility for falling) tend to worry less about falling when considering SBT program and ultimately have a stronger intention to attend the programs. This also implies that increasing older adult’s awareness of his or her susceptibility for falling may not necessarily increase his or her intention to attend the programs. Health care professionals need to be cautious when using increased susceptibility of falling as a justification to convince older adults to participate in SBT programs.
Additional recruitment efforts are needed to attract those who have less confidence in maintaining balance as they might have even greater needs for SBT programs. Based on our findings, program recruitment materials should emphasize how safeguards have been implemented in the program to prevent potential falls during the exercise class as this will reduce fear of falling among potential participants and possibly increase their willingness to attend SBT programs. Despite the significant positive correlation with intention, balance-maintaining confidence (ABC-C scores) had no association with intention to attend once theory of planned behavior variables were taken into account. This would suggest that an emphasis on the variables influencing attitude, subjective norm, and perceived behavioral control might be more profitable in recruiting individuals to an SBT program. However, it is possible that once an individual gets into a program, balance-maintaining confidence would be important for keeping them in the program. More research is needed on this point.
The associations of age with intention, attitude, and subjective norm were negative but nonsignificant in this study. Previous studies found similar but statistically significant associations. Specifically, as individuals’ age increases, their positive attitudes toward exercise (Rhodes et al., 1999) and intention to attend SBT programs (Yardley et al., 2007) declined. It should be emphasized that the recruitment efforts of SBT program target specifically those with advanced age as this group of people are at high risks of falling and lack adequate intention to attend such programs. In our study, perceived behavioral control was the only variable that was significantly and negatively correlated with age. While declines in physical and mental functioning is part of the normal aging process, it is likely that compared to younger individuals, older individuals are more inclined to believe they do not possess adequate capability to perform SBT activities. To help older individuals gain confidence in performing SBT exercises, it is important for program planners to assign appropriate dose and form of exercise to participants across different age groups: young-old (60-69 years), old-old (70-79 years), and oldest old (80+ years), in addition to various levels of physical and mental health conditions. This may help older individuals to have a greater sense of perceived behavioral control. Additionally, age had a significant interaction with subjective norm; subjective norm had greater positive impact on younger women’s intention to attend SBT programs than on older women. Possibly as individuals become older, they are more likely to have declines in physical or mental functions. This may prevent a strong intention to attend SBT programs even when referent others encourage participation. Another possibility is that as individuals become older their social network may decrease in size as friends die and the individuals become less able to ambulate. The contracted social network would have less effect on intentions, and, thus, subjective norms would be less influential in older individuals. To strengthen potential participants’ social support to attend the SBT program, program planners could provide them with a list of myths about attending SBT program and encourage the potential participants to pass on the information to relatives, friends, or neighbors whose opinions they consider to be important. Based on our results, this strategy to promote attendance will possibly be more beneficial for the young-old group as they still retain an adequate social network. For the old-old and oldest-old groups, who lack an adequate social network, program planners should help them expand their social network by assigning counselors or social workers who can regularly contact them and encourage their engagement in SBT exercises.
Becoming more independent in daily life was the strongest predictor of participants’ attitude. It may be important for program planners to focus SBT program campaign messages on this potential benefit. Since family and doctors had significant independent predictions of participants’ subjective norm, program planners may want to work on increasing approval of individuals’ SBT program attendance by families and doctors in order to enhance participants’ intention to attend.
Having SBT programs in familiar locations, participants’ being able to control the amount of exercise that they do in the program, and having enough willpower to complete the program were the dominant control factors that predicted perceived behavioral control. While designing the program, program planners should consider conducting the program in places familiar to participants, as this may reduce environmental distractions and alleviate participants’ potential anxiety levels. The SBT program being held in a place familiar to the participant was the strongest predictor of the perceived behavioral control that, in turn, was a good predictor of intention to attend. To target the old-old and oldest-old groups who are less likely to ambulate around the community and have enough strength to perform exercise, program planners could consider designing and advertising home-based and age-appropriate exercise intervention for these groups of people, as this would create an exercise environment that is familiar to them and allow them to gain increased perceived behavioral control over the exercises that they will perform.
There should also be an option for participants to select the amount of exercises they wish to perform, as this may allow participants to feel that they will gain adequate control over their own SBT program. Recall that the participant believing they could control the amount of exercise was the second strongest predictor of perceived behavioral control. This control by the participant should be advertised in the recruitment materials to increase potential participants’ desires to attend SBT programs.
Having enough willpower to complete the SBT program was the third strongest predictor of perceived behavioral control. To increase older adults’ feelings of willpower, program planners may consider providing lessons that deal with the skills needed to strengthen participants’ perseverance to complete the SBT program (e.g., use of relaxation skills to resist temptation to quit exercising) prior to the inception of the program. This will ultimately increase older adults’ perceived behavioral control and prevent possible attrition of the program. Another way to increase participants’ commitment to complete the program is to have them sign a contract during the enrollment stage of the SBT program (Putnam, Finney, Barkely, & Bonner, 1994). From the recommendations discussed earlier, it is apparent that understanding the design and course content of the program may help potential participants to gain more perceived behavioral control to perform SBT exercises. Thus, program planners are advised to first develop the SBT programs and then create the recruitment materials tailored to the target population.
There were a few limitations inherent in the current study. First, we eliminated 35% of participants due to missing data. The demographic characteristics of those who were analyzed may not represent the entire group of respondents, although the differences between those who were eliminated and analyzed were minimal. Second, as study participants were healthy and adequately educated (all participants were students from a late life education institution), it may be difficult to generalize study results to older adults in the Taiwanese general public. The use of a convenience sample rather than random selection from the target population also limited our study’s generalizability.
Third, we were unable to recruit sufficient number of male participants to make gender comparison feasible. The measure of intention to attend an SBT program collected from our sample may be artificially lower than the intention scores obtained from the general public, including both men and women, since women tend to be slightly less inclined to participate in SBT programs (Yardley et al., 2007). As we were unable to compare gender differences regarding intention to attend SBT programs, future studies should investigate the cause of disparity in intention and explain why it is inconsistent with the established fact that women tend to attend general health promotion programs more than men do. Fourth, it is conceivable that participants who volunteered for the study have more interest in SBT programs and, hence, have more positive attitude, beliefs, and intention to attend SBT programs.
Furthermore, as the principal investigator presented a lecture prior to the data collection, a bias could be introduced in participants’ responses though the bias was attenuated as the topic of the lecture (healthy eating) was not related to the central theme of the research. Finally, we were unable to follow participants to observe their actual attendance at SBT programs; thus, we could not assess the correlation between intention and actual SBT program attendance. Future research should follow participants’ program attendance.
While previous research regarding attitudes and beliefs toward SBT program has focused mainly on qualitative studies (Grossman & Stewart, 2003; McInnes & Askie, 2004; Simpson et al., 2003; Stead et al., 1997; Yardley et al., 2006), an advantage of this study is that it provides quantitative assessment to determine factors that significantly influence older adults’ intention to participate in SBT programs. Participants from aforementioned qualitative studies have reported several facilitators that would promote their motivation to attend SBT programs: (a) perceived benefits of SBT programs such as improved health, social interaction, and personal autonomy; (b) encouragement from families, friends, and physicians; (c) stronger self-efficacy toward SBT activities; and (d) programmatic enhancement, including low-to-moderate exercise, lower cost, and convenient transportation.
Our quantitative study was able to validate that some of these facilitators were indeed significantly associated with older adult women’s intention to attend SBT programs. This study can also guide health care professionals in developing tailored recruitment materials and incorporating exercise intervention elements that promote the engagement in SBT programs among older individuals. Further research should include randomized controlled trials with two groups: one emphasizing recommendations derived from this study, and another without these additions. Then, compare the intention and participation rate between two groups to confirm the validity of the observed facilitators. Once validated, a template/guide of SBT program recruitment material can be created and distributed to health care professionals who promote and design SBT programs. Should such research show the importance of the recommendations developed here policy makers might consider requiring programs to include such components.
Our study provide significant contribution to the literature regarding SBT programs by suggesting many specific behavioral, normative, and control beliefs that are most crucial for developing SBT program recruitment materials. We also suggest many ways to increase older adults’ perceived behavioral control, which was found to be most strongly associated with the intention to attend SBT programs. Our initial finding regarding the possible mediation effect of balance-maintaining confidence on the relationship between intention to attend SBT programs and theory of planned behavior variables is noteworthy as the relationship among these variables has not yet been explored in previous studies. Further investigations should utilize structural equation modeling to validate the mediation effect exerted by balance-maintaining confidence. In addition, since the study participants were exclusively comprised of older adult women, we were able to suggest important facilitators that would help health care professionals to better recruit older adult women who tend to lack the intention to attend SBT programs. Finally, we were also able to examine how age influences the beliefs associated with older adult women’s decision to attend SBT programs.
Footnotes
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
This study was partially supported by a small dissertation research grant from the Loma Linda University Center for Health Research.