
Abstract
Balance training decreases fall risk among older adults, but few participate in such training. We examined the association of exposure to social marketing to promote balance classes, personal characteristics and other factors, with older adults’ balance class participation. Adults aged ⩾60 years were eligible for this case-control study if they attended any church enrolled in a trial testing the effect of social marketing on balance class participation. Cases attended balance classes during the study period; controls were randomly sampled congregants who did not join a class. Cases were more likely to attend churches that received the social marketing program, and were older, more often female, and more frequently experienced “near falls” than controls. Participation was also associated with increasing age of the church’s leader and rural church attendance. Programs to promote balance classes may need to be tailored to target some risk groups, including men and urban and suburban congregants.
Introduction
Unintentional falls are a leading cause of injury-related morbidity and mortality among adults aged 65 years and older worldwide (World Health Organization, 2007). Approximately 29% of adults aged ⩾65 years in the United States fall annually (Bergen, Stevens, & Burns, 2016). Falls among older adults result in significant pain, suffering, diminished quality of life, and financial burden to themselves and to society (Harthold et al., 2011; Stevens, Corso, Finkelstein, & Miller, 2006).
Balance and strength training exercise classes are effective in reducing risk of falls among older adults (El-Khoury, Cassou, Charles, & Dargent-Molina, 2013; Gillespie et al., 2012; Sherrington, Tiedemann, Fairhall, Close, & Lord, 2011). However, there are barriers to fall-prevention exercise class participation among older adults, including fatalism, denial of risk, lack of previous exercise history, lack of resources, history of falls, and fear of falling (Stevens, Noonan, & Rubenstein, 2010; World Health Organization, 2007; Zijlstra et al., 2007).
Messaging strategies that emphasize enhanced quality of life, social interaction, and independence are potentially beneficial for encouraging older adults to participate in exercise classes (Robins et al., 2016; Stevens et al., 2010). Social marketing could be an ideal strategy to communicate these messages, as it promotes voluntary behavior change by increasing its perceived advantages and reducing barriers (Kotler & Roberto, 1989). Several studies have suggested beneficial effects of social marketing strategies on participation in fall-prevention classes by older adults (Clark, Thoreson, Goss, Zimmer, & DiGuiseppi, 2013; DiGuiseppi et al., 2014; Li, Harmer, Glasgow, et al., 2008; Li, Harmer, Mack, et al., 2008; York, Shumway-Cook, Silver, & Morrison, 2011). Such studies have used target audience assessments to identify perceived advantages and potential barriers to class participation, such as desire to stay independent and build social relationships versus the possible difficulty of the exercises and concerns about the cost, frequency, timing, or location of class sessions. Social marketing strategies used in response to these perceived facilitators and barriers have included, for example, holding classes at convenient locations such as senior centers, reducing the number of class sessions per week, and promoting positive benefits of participation (e.g., maintaining independence and opportunities for social interaction).
The current study aimed to assess the independent contributions of characteristics of individual congregants, their churches, and their churches’ leaders, and of exposure to a social marketing program implemented at one’s church, to participation by older adults in community fall-prevention exercise classes.
Method
Study Design, Setting, and Participants
A case-control study design was used to investigate the influence of personal and church-related characteristics on N’BalanceTM class participation. N’BalanceTM, an adaptation of FallProof!TM (Rose, 2010), is a community-based class, delivered twice weekly for 8 weeks by trained instructors, which addresses balance, gait, flexibility, and strength. N’BalanceTM significantly reduces fear of falling and improves balance (Headley, Payne, & Keller, 2013).
The two study counties comprised several small- to medium-size cities (urban) and remaining rural towns and unincorporated areas (rural). The population of the two study counties was 92.3% White non-Hispanic (U.S. Census Bureau, 2009). Any Christian church (whether denominational [e.g., Catholic, mainline Protestant, the Church of Jesus Christ of Latter-Day Saints] or nondenominational) was potentially eligible. We excluded non-Christian places of worship because there were too few of each within the study counties (specifically, only one synagogue and one mosque) to randomize effectively between groups. For practical and logistical reasons, we also excluded churches located in several geographically remote parts of the two counties as well as those with fewer than 15 members aged 60 years and older. Religious or other leaders of potentially eligible churches were contacted by mail and telephone from May 2009 to July 2010 to screen for eligibility and obtain consent for participation. Enrolled churches were randomized to receive the intervention (social marketing program) or no intervention. Details of the trial have been published (DiGuiseppi et al., 2014). The Colorado Multiple Institutional Review Board approved the study (Protocol #06-0636).
Social Marketing Program
The social marketing program, implemented in churches randomized to the intervention condition, addressed key social marketing elements, that is, product, price, place, and promotion (Maibach, Rothschild, & Novelli, 2002), to motivate older adults’ participation in balance classes. Course fees were subsidized, reducing the cost to US$20. To increase accessibility, courses were delivered at multiple, convenient locations. Marketing messages were delivered in each study church in 4-week “waves” immediately prior to each balance class being offered in the church’s locale. Messages emphasized promoting independence and building social relationships in a safe and comfortable environment, and were communicated through posters, brochures, flyers, coupons, bulletins, newsletters, pulpit announcements, and person-to-person marketing. In about half of enrolled churches, we successfully recruited church leaders, staff, or members to serve as “messengers” to market the class directly to older adults within their congregations. State health department staff and trained church messengers implemented the marketing program between January 2010 and September 2011. More detailed descriptions of the formative research that guided marketing program development (Clark et al., 2013) and the program itself (DiGuiseppi et al., 2014) have been published previously.
Case Selection and Data Collection
All adults aged ⩾60 participating in any N’BalanceTM exercise class offered in either study county during the marketing program implementation period were identified as potential cases. During the first session of each 8-week class (or the second session for a few class participants who missed the first session), potential cases capable of giving informed consent were invited to take part in the study. Consenting individuals completed a health and demographic survey at the start of the session, and a second brief survey about church attendance immediately after the session, and received a US$5 gift card. Cases were defined as first-time class participants aged ⩾60 who attended any study church (either intervention or nonintervention) and completed both research surveys. Cases completed an average of 12.5 (78%) of the 16 class sessions.
Control Selection and Data Collection
Research surveys that combined the health and demographic survey and the church attendance survey were mailed to a random sample of congregants aged ⩾60 who attended any enrolled study church, using church membership lists. The survey protocol included prenotification postcards, followed by questionnaires with US$2 incentives and, 2 to 3 weeks later, second questionnaires, to maximize participation (Edwards et al., 2009). This process was fully implemented by 58% of churches and partially implemented (e.g., omitting postcards) by the rest. In the latter group of churches, the number of surveys distributed was adjusted upward to account for lower anticipated response rates. Controls were defined as all respondents aged ⩾60 who attended any study church, completed a research survey, and reported that they had not participated in any N’BalanceTM or other exercise class designed to reduce falls during the study period. Return of completed surveys implied consent.
Measures
The research surveys completed by cases and controls included questions about demographic characteristics, church attendance, fear of falling (seven-item Fall Efficacy Scale–International [Short FES-I], which assesses level of concern about falling in different situations [e.g., taking a bath or shower, going up or down the stairs], with “high concern” defined as a score ⩾11; Delbaere et al., 2010; Kempen et al., 2008), fall history (self-report portion of the Elderly Fall Screening Test; Cwikel, Fried, Biderman, & Galinsky, 1998), and health status, depression, and past-month physical activity (Link, 2008). The survey also asked whether they had previously participated in N’BalanceTM or any other balance training classes (to determine eligibility).
Church-level data were collected at the time of church enrollment in the trial. Each church leader was surveyed about church characteristics and his or her demographic characteristics and perceptions of the importance of older adult falls, fall preventability, and potential benefits from balance classes, using a 5-point Likert-type scale. Information on church denomination and location were also collected.
Analysis
We compared cases and controls on characteristics of the individual, the church attended, and its leader using χ2, Wilcoxon rank-sum, or independent sample t tests, as appropriate. Multivariable logistic regression was used to examine the independent contributions to balance class participation of exposure to the social marketing program, church and church leader characteristics, and the individual’s own characteristics; the final model retained variables significant at p < .05. Interactions were assessed and interaction terms retained if p < .05.
Results
Of 243 eligible exercise class participants, 215 (88%) consented and completed the surveys. Of these, 173 met the case definition. A total of 280 congregants aged ⩾60 returned surveys (response rate ~62%), of whom 270 met the control definition.
Table 1 shows characteristics of cases (exercise class participants) and controls (nonparticipants), the churches they attended, and their church leaders. Consistent with results at the group (church) level (DiGuiseppi et al., 2014), cases were significantly more likely to attend a church where the social marketing program was implemented. There were also significant differences in the characteristics of congregants who participated in N’BalanceTM: Compared with controls, cases were older, in poorer health, less likely to have participated in any physical activities in the previous month, and more likely to be female, experience “near falls” more often (i.e., loss of balance in which recovery occurred to prevent a fall), and have a high fear of falling (Table 1).
Comparison of Characteristics of Balance Class Participants (“Cases”) and Nonparticipants (“Controls”).
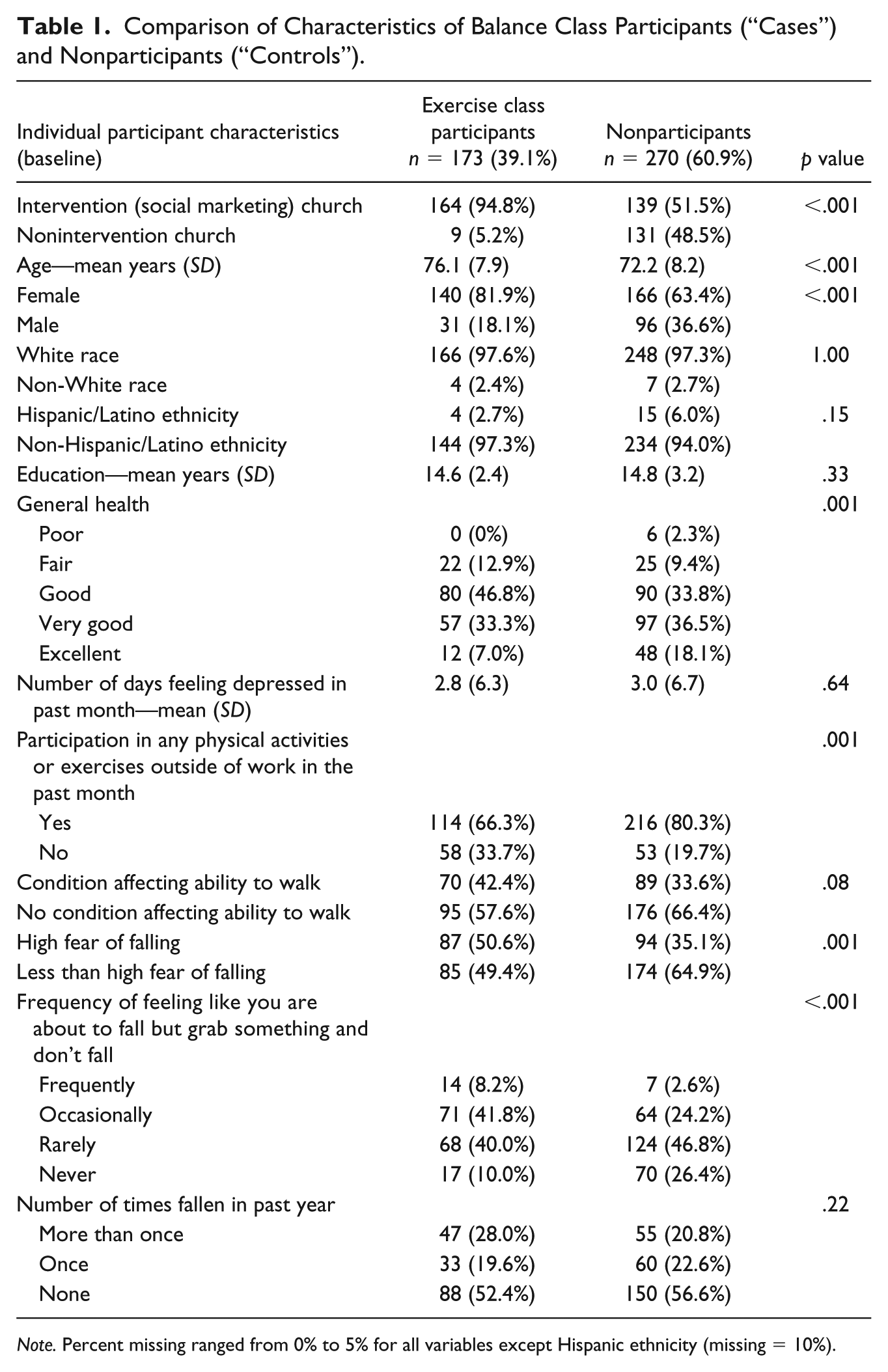
Note. Percent missing ranged from 0% to 5% for all variables except Hispanic ethnicity (missing = 10%).
Table 2 shows characteristics of the churches attended by cases and controls, and of the church leaders. Compared with churches attended by controls, those attended by cases were smaller, more often mainline Protestant and rural, and had fewer communication resources. The leaders of churches attended by cases were significantly older and less likely to believe that older adult falls were preventable (Table 2).
Comparison of Church and Church Leader Characteristics of Balance Class Participants (“Cases”) and Nonparticipants (“Controls”).

Note. IQR = interquartile range. Percent missing ranged from 0% to 5% for all variables.
Other leader types include board president, church administrator, director of senior adult ministries, minister’s wife/office administrator, and moderator/elder.
Scale of 0 = not at all to 4 = extremely.
In multivariable analysis, individual characteristics independently associated with balance class participation included female sex, older age, and more frequent “near falls.” Balance class participation was also associated with attendance at a church located in a rural area and with increasing age of their church’s leader. The strong association of balance class participation with attending a church where a fall-prevention social marketing program took place persisted in the adjusted analysis (Table 3). No interaction terms were retained.
Adjusted ORs for Factors Associated With Balance Class Participation.

Note. OR = odds ratio; CI = confidence interval.
Scale of 0 = never to 3 = frequently.
Discussion
Exposure to a social marketing program to promote balance classes through churches continued to demonstrate a strongly positive association with balance class participation even after accounting for differences between participants and nonparticipants in their own characteristics and those of the church they attended and the church’s leader. This study expands on our past research to identify individual and church characteristics associated with balance class participation independent of exposure to a social marketing program.
Older age, female gender, and more frequent “near falls” increased the likelihood of balance class participation. Among older adults, increasing age and female sex increase the risk of unintentional falls and related morbidity (Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, 2016; Stevens, 2005; Stevens & Sogolow, 2005). Furthermore, self-reported near falls or missteps have been independently associated with self-reported falls (Srygley, Herman, Giladi, & Hausdorff, 2009). Our findings suggest that individuals who (correctly) perceive themselves as having a higher risk of falls are more likely to respond to messaging about balance classes for fall prevention and to participate in such classes.
The association between increasing age and greater exercise class participation is somewhat inconsistent with previous literature; for example, studies have found age to be negatively associated with behavior control and with coping appraisal (representing perceived benefits of participating in strength and balance training and appropriateness for people like them), both of which are correlated with intention to participate in strength and balance training (Lin, Lee, Modeste, & Johnson, 2010; Yardley, Donovan-Hall, Francis, & Toded, 2007). It is possible that our results differed because the social marketing strategy used in our study allowed older adults to overcome perceived barriers to balance class participation, such as those related to the coping appraisal or behavior control constructs previously described, or because we measured actual attendance rather than intention. It may also be that younger congregants (those aged closer to 60 years) did not feel that the balance class was appropriate for them based on their perception of low fall risk, the content of the class, or the messages we disseminated about the classes.
The higher likelihood of balance class participation among females is consistent with previous fall-prevention trials (Close et al., 1999; Voukelatos, Cumming, Lord, & Rissel, 2007). There may be gender-related disparities in perceptions of fall risk and the need to prevent them, or in the acceptability of balance classes for fall prevention. Previous research has noted gender differences potentially relevant to fall-prevention strategies, for example, men’s concerns about embarrassment due to “competition that pits participants against each other,” perceptions that women are “high-priority recipients of . . . fall-prevention messages,” and differing likelihood of attending same- or mixed-sex classes (Clark et al., 2013).
As noted by Stevens (2005), interventions shown to be most effective (i.e., exercise, balance training) are not always the most acceptable to older adults. Future programs might conduct more extensive market research to more effectively target perceived benefits of and barriers to balance classes among men as well as the “young old,” who may not perceive themselves as at risk despite the observed increased morbidity and mortality from falls in both sexes (World Health Organization, 2007). More research also needs to be conducted to identify which types of exercise or other fall-prevention programs may be more appealing to men and to the younger set of older adults.
Members of rural churches were more likely to participate in balance classes than urban church members. Churches typically represent non-geographic social networks (Debertin, 2015). However, in rural communities, the social network created by belonging to the same church may be similar to social networks based simply on location. This overlap in geographic and congregational social networks within rural communities may contribute to increased readiness to participate in church-sponsored activities. Fewer options for other exercise or social activities in rural areas may also contribute to the increased uptake in our study. Furthermore, rural older adults of lower socioeconomic status have increased fear of falling and perceived fall risk compared with their urban counterparts, which may have increased motivation to participate in balance classes (Cho et al., 2013). Further research is needed to understand differences between rural and urban congregants and congregations that might help explain our findings and enable future marketing programs that address fall prevention to better target urban residents.
Our control selection strategy was designed to ensure that controls came from the same communities and churches as cases, to avoid selection bias. The relatively low (62%) mail survey response rate for controls may have increased the potential for selection bias, although this rate is similar to or higher than those of other mail surveys conducted in similar populations (e.g., Edelman, Yang, Guymon, & Olson, 2013; Medway & Fulton, 2012). The lack of congregations in large cities, of non-Christian faiths, or having substantial minority congregants in our study area may limit the generalizability of these results. In addition, there may be differences in beliefs related to balance class participation and receptiveness to social marketing across the religious denominations that were included in this study. Finally, some social marketing strategies may have differed in terms of quantity and quality within the different intervention churches, especially person-to-person marketing, which was offered by different health department staff members and church messengers depending on the interest level and available communication resources at each church. This may have affected the strength of the association between the social marketing intervention and balance class participation.
Conclusion
This study found that, along with exposure to a social marketing program to promote balance classes, female gender, increased age, and rural church location were all significantly associated with balance class uptake. Older men and “younger” older adults, who may not recognize their increased risk for falls, may be important targets for efforts to promote balance classes and other fall-prevention programs. Future research aimed at examining interventions targeting these groups as well as testing of social marketing programs in urban churches and in settings other than places of worship (e.g., senior centers) are needed to demonstrate the feasibility of this approach for diverse older adult populations. This study provides insight into groups that can be successfully targeted for older adult exercise classes through church-based social marketing programs and identifies target groups that may be harder to reach, who may require new messaging strategies and greater efforts to address barriers to participation.
Footnotes
Authors’ Note
Research assistants Faye Boss, Joyce Chynoweth, Sarah Morehouse, and Vedavani Tiruveedhula made substantive contributions to this study. Cynthia W. Goss is now affiliated with Centers for American Indian and Alaska Native Health, USA. Ms. Thoreson has since retired from the Colorado Department of Public Health and Environment, Denver, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant R49/CCR811509 to the Colorado Injury Control Research Center from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.