
Abstract
This article describes the development of a new mutual support group intervention for long-term care homes (LTCH); evaluates the processes, structure, and content of the intervention; and addresses replication and sustainability. Tom Kitwood’s model of personhood is used as the basis for developing a weekly discussion group using themes chosen by participants and theme-associated music, readings, and photographs. A mixed-methods qualitative process evaluation design encompasses focus groups, systematic observation of six resident groups, individual resident interviews (N = 65), and staff interviews (N = 7) in three LTCH in British Columbia, Canada. Resident reports and observations indicate positive benefits including a decrease in loneliness, the development of friendships, and increased coping skills, understanding, and support. Participating staff reported numerous benefits and described how the unique group structure fosters active participation of residents with moderate-severe cognitive impairment. This preliminary study suggests that mutual support groups have potential to offset loneliness, helplessness, and depression within LTCH.
Despite advances in policy and programs to improve the psychosocial well-being of those living in long-term care homes (LTCH), residents continue to report feelings of loneliness and helplessness, as well as frustration with their lack of influence on decision-making (Bondevik & Skogstad, 1996; Fessman & Lester, 2000; Timonen & O’Dwyer, 2009). Research suggests that loneliness and depression among the elderly have a reciprocal influence on one another (Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006) and a study by the Canadian Institute for Health Information (CIHI) found almost half (44%) of those living in care homes have a diagnosis and/or symptoms of depression (CIHI, 2010). The study revealed that only a small proportion of those identified with symptoms and a diagnosis of depression actually received an evaluation by a licensed mental health professional (8.4%) or psychological therapy (2.6%). This is a critical social issue that has yet to be resolved and it highlights the need to develop and implement innovative approaches that support the mental health of those living in LTCH.
Residents diagnosed with depression describe loneliness, loss of autonomy, and lack of meaningful activities as major themes related to their condition (Choi, Ransom, & Wyllie, 2008). Treatment within LTCH continues to focus on pharmacotherapy to address depression, but research suggests that the use of non-pharmacologic interventions in conjunction with pharmacotherapy is a more effective approach in treating mental health problems (Hyer & Intrieri, 2006). However, Cody, Beck, and Svarstad (2002) have identified a number of challenges that preclude the use of this approach, including regulatory and economic barriers, as well as the lack of available programs and staff training.
In a discussion of the challenges that institutionalized residents face, Berman-Rossi (2005) describes the need for mutual aid or mutual support groups. He argues that institutions bear the responsibility of providing means to support residents in dealing with institutional stressors as well as ways to empower them to engage in decision-making processes. The mutual support structure gives residents a means to foster resiliency in a supportive environment of their peers (Berman-Rossi, 2005). There is an emerging body of research that documents the effectiveness of mutual support groups in alleviating loneliness and depression in the community (Bright, Baker, & Neimeyer, 1999; LeBarge & Trtanj, 1995; Logsdon et al., 2010; Roberts & Silverio, 2009; Snyder, Jenkins, & Joosten, 2007) but limited evidence of this type of intervention within care homes.
Conceptual Foundations
The concept of personhood as put forth by Tom Kitwood (1997) is used extensively in the literature and provides the theoretical foundation for this study. Kitwood defined personhood as “a position or social relationship that is bestowed on one human being by ‘others’, in the context of relationship and social being” (p. 8). He describes a malignant social psychology in our society—one that places higher values on intellectual functioning than on noncognitive attributes and argues that, in many instances, the social positioning that occurs around those with losses in functioning and capacity results in loss of personhood. Within LTCH, this is demonstrated by staff who often inadvertently place persons with dementia in a position of “other”—someone with less ability and status. This positioning can occur in a myriad of subtle ways, both between the staff and residents and among the residents themselves, even when the intention is caring and positive (Dewing, 2008).
Social relationships that residents develop within residential care are believed to have a greater effect on loneliness and depressive symptoms than the relationships with those outside, such as family and friends (Carpenter, 2002; Fessman & Lester, 2000; Park, 2009). Having mutual empathy for one another builds bonds that can create new relationships from which psychological and physical benefits are derived. Through giving and receiving support individuals develop a stake in the welfare of others, consistent with the connection between empathy and altruism (de Waal, 2008). The present study expanded Kitwood’s key concepts beyond dementia care to include the care of residents living in LTCH with a wide range of disabilities. In addition, it expanded the concept of care given by the staff to the residents to care given by the residents to one another in the development of their interpersonal relations.
As illustrated in Figure 1, the conceptual model developed for this study was based on personhood (Kitwood, 1997), aspects of reciprocal altruism (Trivers, 1971), and the helper-therapy principle (Riessman, 1997). Residents share challenges living with disabilities as well as numerous losses related to moving into an institution. Loss of control over everyday decision-making is an example of a loss that has a significant impact on well-being. Empathy for others who are in similar challenging situations can act as an emotional cue and foster feelings of closeness. Aspects of personhood—validation, holding, and facilitation—leads to reciprocal altruism, balanced giving and taking, which ultimately lead to trust (Trivers, 1971). When reciprocity is expressed in groups (within the helper-therapy principle framework), helping benefits both the individual and the group through the synergy created (Riessman, 1965). The helper-therapy principle is similar to the concept of social support from peers but includes group members giving as well as receiving help from one another; the group as a whole benefits from this bidirectional supportive structure. This assertion is empirically supported by numerous studies with different populations (Kyrouz, Humphreys, & Loomis, 2002).

Conceptual Map.
The concept of empowerment is central to Riessman’s helper-therapy principle and provided a guide to the development of this intervention. Empowerment is a process in which people gain mastery over their affairs and increase their sense of effectiveness within their community (Rappaport, 1987). However, Paterson (2001) describes a myth of empowerment that is perpetuated in health care. It is at times mistakenly assumed that residents, when offered the opportunity, will become active agents in their own lives. Findings indicate that if people do not feel prepared and are not given sufficient time, they will likely rely on someone else to make decisions for them (Paterson, 2001). This is particularly important for those with cognitive impairment.
The main purpose of this article is to present a rationale for and describe a new intervention involving mutual support groups in LTCH; to evaluate its process, structure, and content; and to provide evidence that supports refinement and replication. Specifically the article consists of three parts: (a) a description of development of the intervention and program elements, (b) a description of the piloting of the intervention combined with a process evaluation, and (c) replication considerations and sustainability.
Design and Methods
A mixed-methods qualitative process evaluation was utilized in order to conduct a multimodal evaluation of the processes involved, including systematic observation of the groups, resident and staff interviews, and resident focus groups carried out by the principal investigator. The process evaluation consisted of an assessment of the structure, content, and components designed to keep the program on track. Due to the small number of participants involved, it is not the intent to look at statistical differences but rather to describe and assess the delivery of the intervention and compare what was intended with what actually happened. It is important to note here that the purpose of a process evaluation is to establish whether the intervention was implemented as intended before investing in the resources needed to conduct an outcome evaluation (Saunders, Evans, & Joshi, 2005). Thus, although this article describes the study participant reports, these are not outcomes as such but rather an assessment of the program design and implementation.
The Development of the Intervention
A mutual support group pilot named the Java Music Club was implemented by the principal investigator, an accredited music therapist with over 15 years of clinical experience facilitating therapeutic groups. All residents within one area/unit within the care home were invited and approximately 12 to 15 residents attended on an ongoing basis. Through a process of experimentation with discussion topics generated by staff and residents, a group structure developed over a 6-year period. Group participants helped to mould the group structure in many ways. Some would choose topics or themes that were of interest to them, as well as related music, photographs, and readings. Others would offer different coping options to the challenges that were shared by the group members. Those options that the group liked were accepted as a part of the weekly program. For example, one of the ways the group chose to address self-esteem challenges that some were facing was through the adoption of a positive group affirmation read at the end of each session. To assist with special needs of the residents, a staff member co-led the groups along with rotating resident group members.
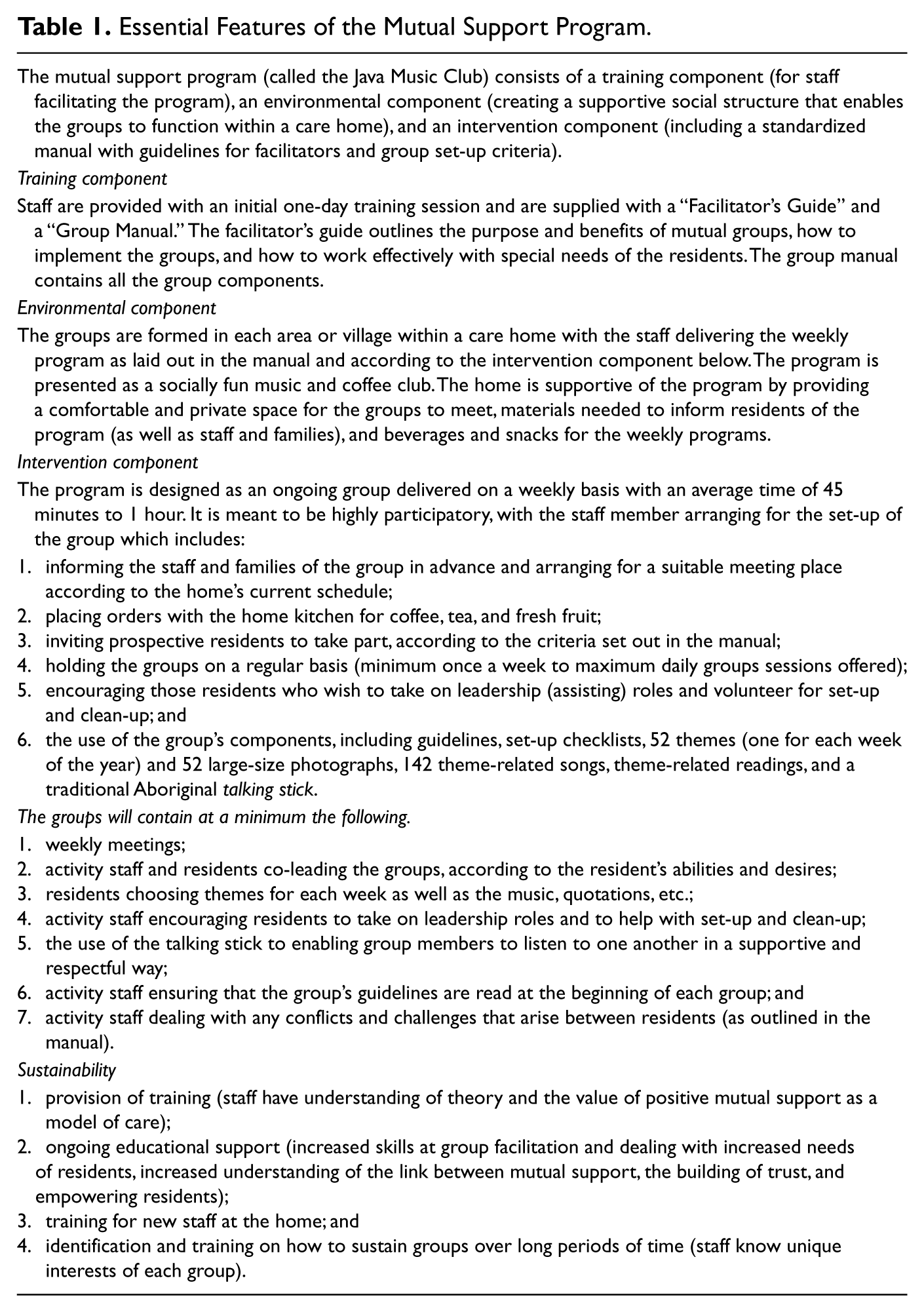
From this pilot, the principal investigator developed a group manual and a facilitator’s guide. The essential features of the group structure are described in Table 1. All residents living within a unit or neighborhood are invited to attend, but a typical group session averages 8 to 12 residents. Before the group begins, coffee and treats are served and quiet background music is played and the staff facilitator invites one of the residents to assist or co-lead. The resident co-leader chooses a theme for the discussion from a list provided or a theme of their choice. After the opening song is sung the resident co-leader reads the group guidelines from the manual provided. Group members are then invited one by one to share how their week has been and any thoughts they have on the chosen theme. Those sharing hold a traditional Aboriginal Talking Stick provided as a visual cue and a reminder to respect others’ opinions. After a few of the participants share, the resident co-leader either chooses a theme-related song, which is played on a CD player, or asks another group member to read a theme-related quote or reading. Both are provided with the manual. This gives the group a break from talking and also provides mental and/or emotional stimulus for the discussion. When appropriate, the staff facilitator also shows a theme-related photograph that often stimulates memories or storytelling. A topic example is “Day-to-Day Challenges.” Associated songs include “Pick Yourself Up,” “Side by Side,” and “Don’t Worry, Be Happy.” A relevant quote reads, “It’s not whether you get knocked down, it’s whether you get up again,” and a related photograph shows a person struggling with a physical challenge. The discussion continues until all the group members have shared or until about 45 minutes have passed. Participants sing a closing song and are then invited to help with clean-up and to aid fellow group members requiring assistance back to their rooms.
Essential Features of the Mutual Support Program.
The specific objectives for this intervention are listed below and were generated from Riessman’s principles and related to different group members based on their individual characteristics, personal goals, and preferences:
to increase self-determination by taking on leadership and making choices;
to increase giving and receiving help;
to increase the focus on inner strengths, beliefs, and abilities;
to strengthen supportive relationships with one another; and
to increase expression of challenges faced in a way that allows for new interpretations.
Table 2 briefly describes these principles and illustrates the essential differences in characteristics between a mutual support group and a typical social group activity in LTCH.
Mutual Support Groups Versus Typical Groups in Long-Term Care Homes.
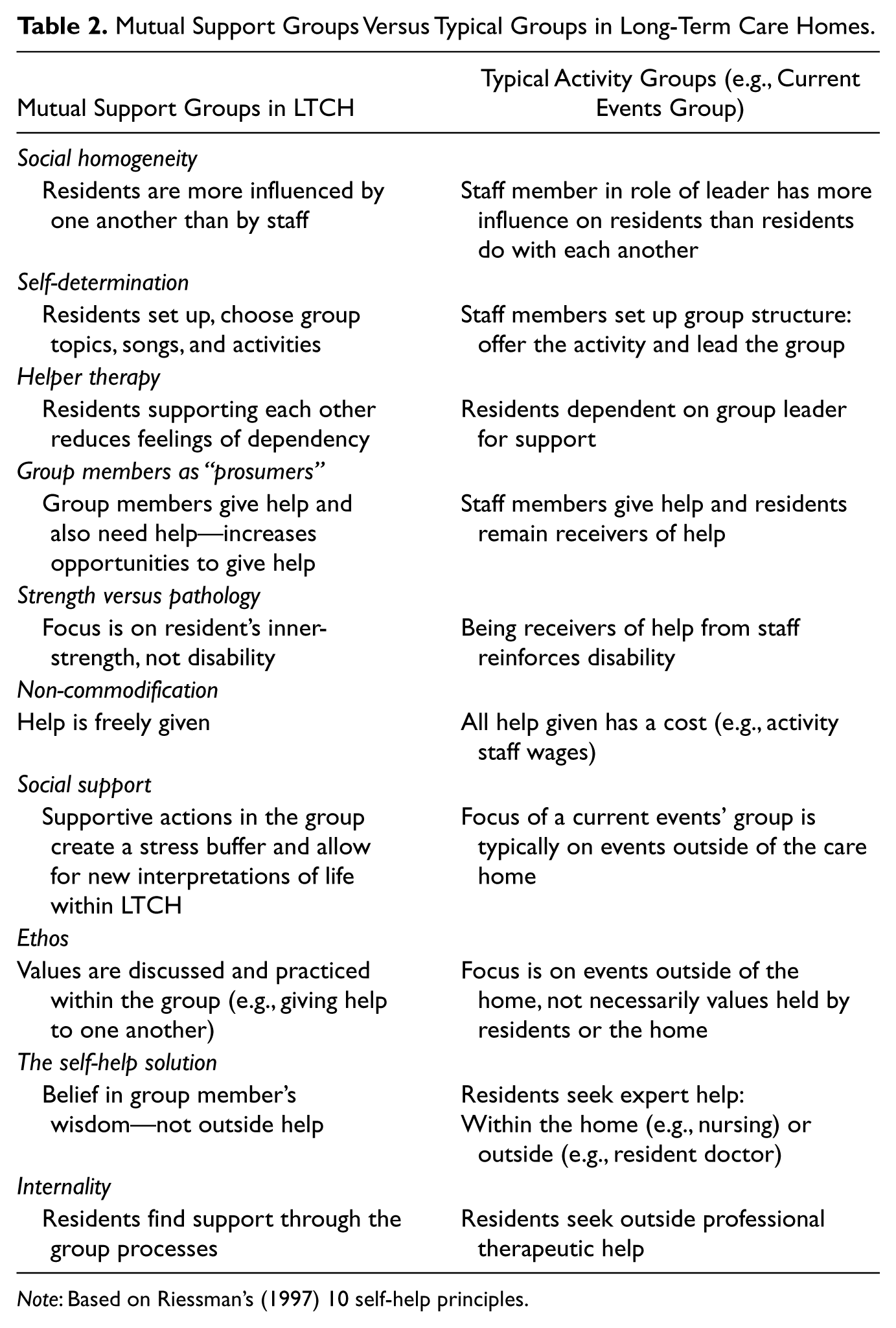
Note: Based on Riessman’s (1997) 10 self-help principles.
The Setting and Participants
Three residential care homes were selected in British Columbia, Canada. Two of the care homes are privately owned and one is a publicly funded not-for-profit. All three homes are in a single geographical region and classified as complex care (defined as a 24-hour professional residential care). In order to evaluate the potential use of the program across the different cognitive functioning levels, six groups were implemented: two in special care (secured units), three in complex care (unsecured units), and one in an adult day program within a care home. As the groups involved discussion, staff used purposive sampling and invited residents who were able to communicate verbally within a group discussion format to some extent (i.e., at least be able to answer yes and no to questions and track other group members’ sharing). Residents on temporary respite stay were excluded. For practical reasons, those residents whose needs could not be met by a single activity worker were also excluded (e.g., those with behavioral needs requiring frequent attention).
Cognitive status data were collected using the Mini-Mental State Examination (MMSE). Although these scores alone without age and educational adjustment are not a definitive indicator of cognitive status (Kim & Caine, 2002), the scores were meant for descriptive purposes only and to serve as indicators. In 2001, Folstein, Folstein, McHugh, and Fanjiang recommended the following MMSE scoring, which was used for the purposes of this study: ≥ 27 = normal; 21 to 26 = mild; 11 to 20 = moderate; ≤ 10 = severe. Ethical approval for the study was obtained as well as consent from next of kin for residents with significant cognitive loss (MMSE ≤ 21).
The Group Design and Procedure
Staff that regularly conducted activity programs were invited to facilitate the groups in the study. The selection consisted of two activity aides, two therapeutic recreational directors, two rehabilitation assistants, and one music therapist, all of whom received a single training session to become familiar with the program components. Training provided by the principal investigator included learning how to implement a mutual support group and facilitate the specific components of the group structure, as well as observing the pilot group in session. Training also included information on the theoretical foundation of mutual support groups and their impact on resident loneliness and depression, ways to enhance group facilitator skills and communication between group members, and how to facilitate mutual support groups in special/secured units. In addition, ongoing support was provided throughout the study along with a mid-point adherence check-in to make sure procedures were consistent across the six groups. The groups met on a weekly basis for a minimum of 12 sessions and each group session lasted for approximately 45 to 90 minutes.
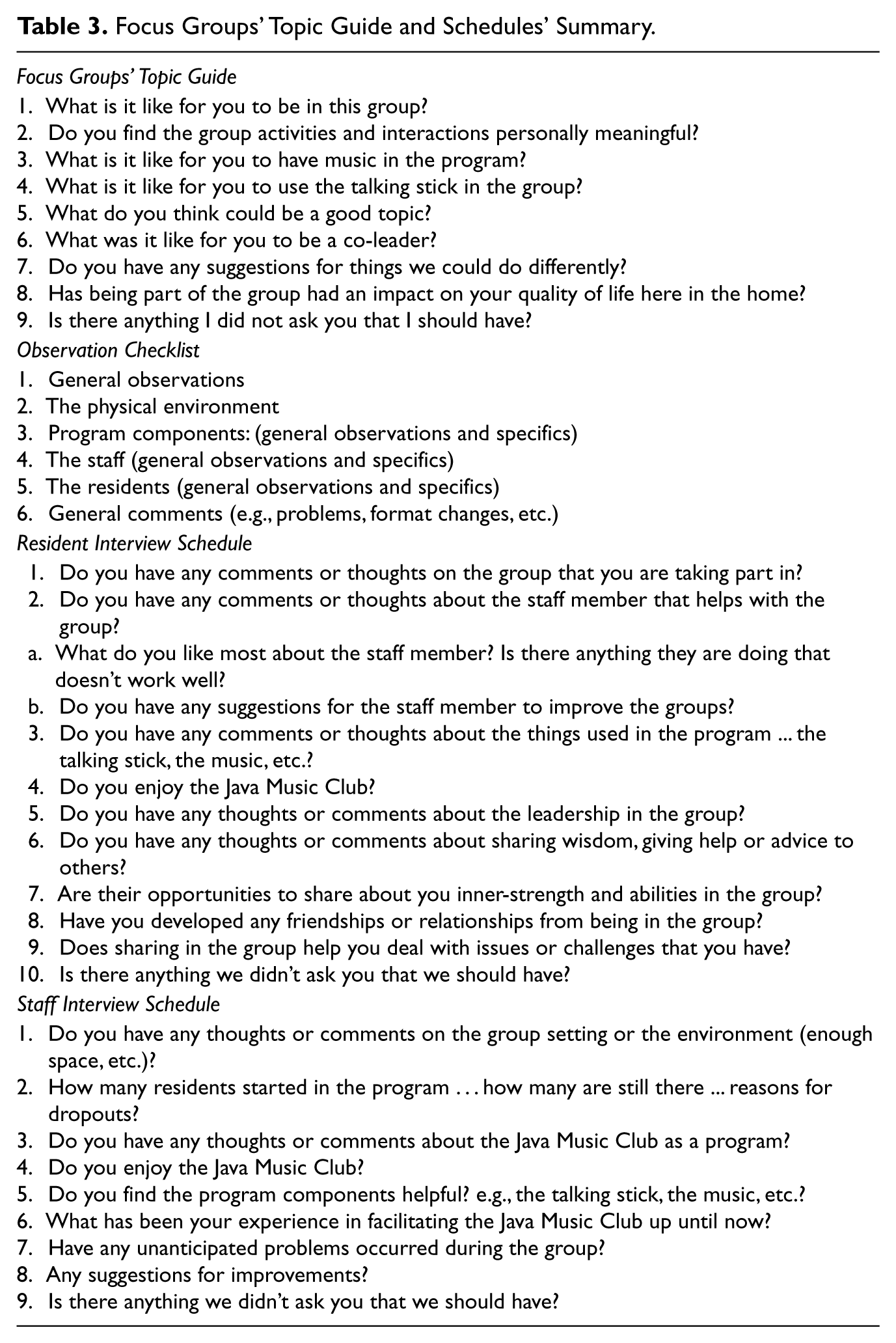
The observation checklist and the resident and staff interviews (see Table 3) were broadly based on a previously developed program evaluation called “Fit and Strong!”, an exercise and behavior-change program, adapted with permission for this study (Hughes et al., 2006). The adaptation included the use of a similar overall layout and outline, the use of section titles (such as “Environment”), and similar introductory wording to the sections. The observations took place during the first month. Data gathered from the group observations were used to inform the focus group topic guide. Resident and staff interviews were administered individually at end of the second month, and information from these interviews was also used to inform the focus group questions. The focus groups occurred near the end of third and last month. This approach to methodological triangulation (interviews, observations, and focus groups) provided replication of results and maximized trustworthiness and credibility.
Focus Groups’ Topic Guide and Schedules’ Summary.
Process Evaluation Plan
The process and program evaluation plan was based on a model developed by Saunders et al. (2005) and included five primary elements: recruitment, reach, fidelity, dose, and context. Their process evaluation was created for public health interventions and research in the medical field. In an effort to move away from a disease-based model of care within a medical system to a resident-empowered model of care in this study, the word dose was replaced with the word program (including components delivered and received). These five elements therefore included recruitment (which procedures were followed to recruit activity workers and residents), reach (degree to which the residents participated in the intervention), fidelity (extent to which the program was accurately delivered), program delivered (what was actually delivered to the residents), program received (what was actually received by the residents), and context (environmental aspects influencing the implementation of the intervention). The steps in the model consisted of (a) a description of the program, (b) a description of the complete and acceptable delivery of the program, (c) a list of potential process-evaluation questions, (d) determination of methods for the process evaluation, (e) consideration of the program resources and program characteristics and context, and (f) finalization of the process evaluation plan.
Due to the limited resources available, interviews and group observations were carried out by the principal investigator. Both the resident and staff interviews averaged 30 minutes to 1 hour. A combination of structured and unstructured observations was used in an attempt to capture both the physical and verbal behavior of participants and the whole picture or context of the mutual support groups. The focus groups were recorded and led by the principal investigator, who trained three music therapy interns who volunteered as research assistants. The students received training on key skills of an effective note-taker for focus groups, observational training, and were given checklists to follow. To improve reliability, a discussion was held in advance about the available choices, and notes were reviewed immediately after the focus groups and peer debriefings held to review and identify issues. In order to establish rigor and minimize the potential bias introduced by the researcher, an audit trail of evidence was kept, including all raw data from the observations and interviews, data reconstruction notes, summaries of the condensed notes, synthesis of the themes, and reflexive notes including predictions and intentions.
The researcher was also responsible for addressing considerations of validation in order to provide trustworthiness (Patton, 2002). The approach taken in this study was to include ethical and substantive validation for the focus group data collection and analysis. According to Patton (2002), this includes how solid and consistent the evidence is, to what extent the findings increased understanding, to what extent the findings are consistent with existing literature, and to what extent the findings are practical and useful. Aspects of ethical validation that were addressed in the study included ensuring that no one participant’s voice was excluded or demeaned, that the research generated new possibilities beyond the present understanding of the topic of mutual support in LTCH, and lastly that it opened possibilities for effective change in how group activities are approached in LTCH.
As reported in Angen (2000), substantive validation involves providing a chain of interpretations so that the reader can judge the trustworthiness of the conclusions drawn from the data. Similarly, as reported by Rabiee (2004), in order to establish rigor and minimize the potential bias introduced by the researcher and subjective selection and interpretation, an audit trail of evidence needs to be provided. The data analysis consisted of a number of stages. These stages included examining, categorizing, and tabulating the evidence in order to meet the original intentions of the study (Denzin & Lincoln, 2005).
With the above information in mind, the data analysis in this study followed the series of steps outlined below:
The focus group process
The focus group processes included the following four components:
recorded and transcribed spoken language in the focus groups;
observations capturing the nonverbal communication of group members recorded by note-takers (volunteer research assistants);
a reflective diary kept by the moderator of the focus groups; and
reflection on the focus groups written immediately after each group by the moderator and the note-takers (Rabiee, 2004).
The data analysis
A framework analysis described by Krueger (1994), with key stages outlined by Ritchie and Spencer (1994), was used for the purposes of this analysis. The framework includes five key stages of focus group data analysis:
Stage 1: Familiarization: listening to recordings, reading the transcripts, and observational notes;
Stage 2: Identifying a thematic framework: writing memos from ideas and concepts arising from the text—beginning development of coding and categories;
Stage 3: Indexing: sifting data, making comparisons within and between cases;
Stage 4: Charting: lifting quotes from original context and rearranging them under themes; and
Stage 5: Mapping and Interpretation: making sense of the data as a whole using the following established criteria: words, context, internal consistency, frequency, and extensiveness of comments; specificity of comments; intensity of comments, and big ideas (Krueger, 1994; Ritchie & Spencer, 1994).
The analysis also explored any potential variations of themes across the two facilities and between the groups within each facility.
The evaluation analysis plan included a summary of the observations, the individual resident and staff interviews, and the focus groups. Data analysis consisted of a number of stages, including examining, categorizing, and tabulating the evidence in order to meet the original intentions of the study. Scores were calculated based on the number of intended activities and processes included in the programs. Substantive themes were generated and synthesized from the focus group data. A self-reflexive process was used to identify any biases that the principal investigator held during the course of the study and its interpretations. In addition, validity checks of the data interpretations were conducted by the investigative team as well as frequent debriefing sessions (Shenton, 2004).
Results
The evaluation focused on the process of implementing the program and how staff and residents felt about specific components of the program. Results were compared across groups and across homes, and it was predicted that there would be differences. Analysis of the individual resident interviews and focus group themes was done separately, but there was a substantial overlap and a decision was made to present the combined results. In addition, the salient themes were identified and a comparative analysis completed of the cognitively higher functioning residents (MMSE scores ≥ 21) and the cognitively lower functioning residents (MMSE scores ≤ 20). This was done to see if there were comparative differences in the experiences of these two groups of residents.
Recruitment
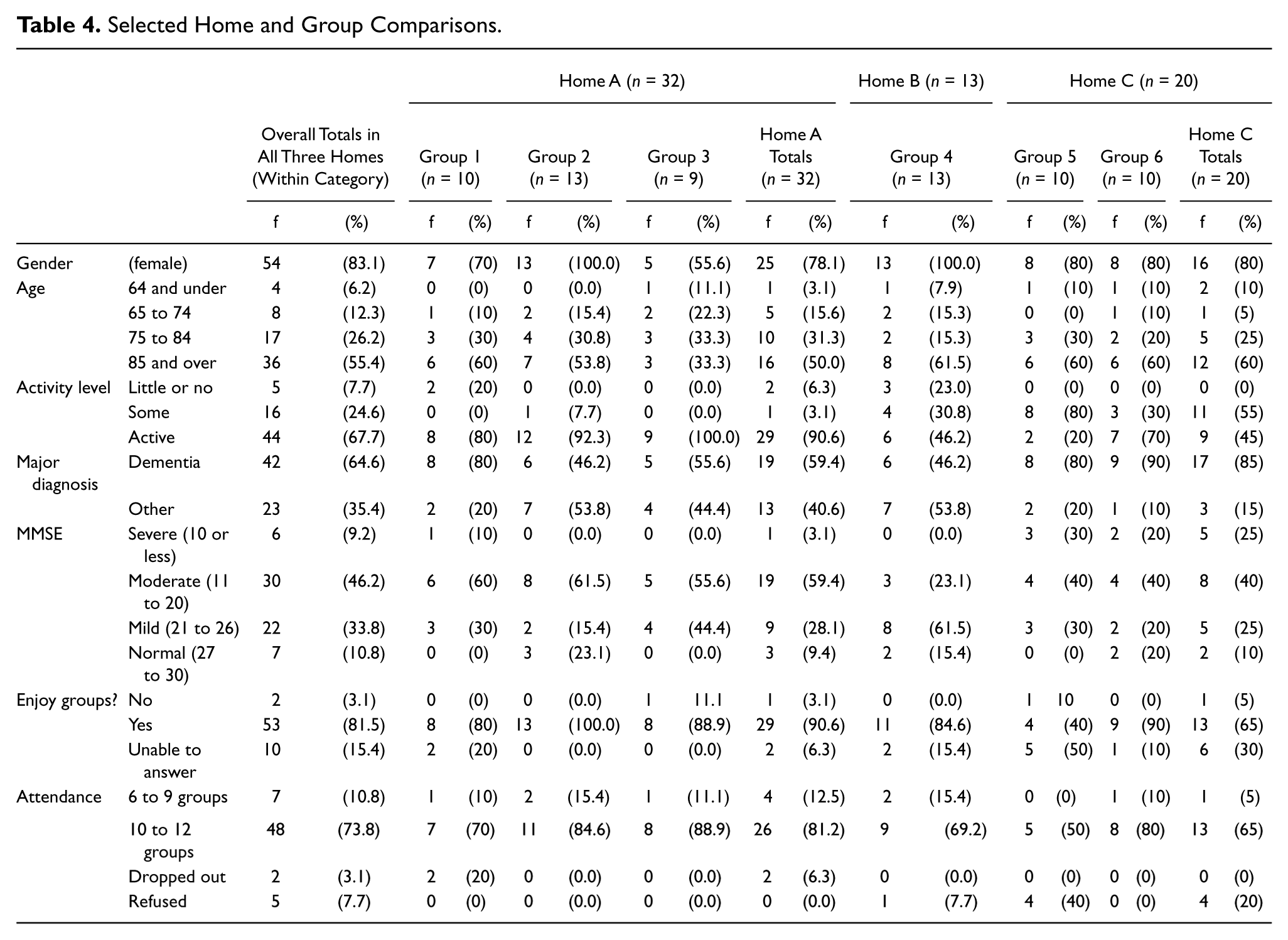
Data collection took place over a period of 6 months. Of the total number of participants (N = 65), the majority were female (83.1%), with two of the groups having no male participants (see Table 4). Over half of the participants were 85 years of age and older (55.4%), with a small minority (6.2%) who were 64 years of age and younger. A total of 64.6% of the participants had some form of dementia, and 35.4% had other disorders such as heart disease, psychiatric disorders, or musculoskeletal disease. The levels of involvement of the study participants in regular activity programs offered within the homes ranged from 67.7% who attended, observed, and/or engaged in 13 or more activities per month; 24.6% with 4 to 11 activities per month; and 7.7% with 0 to 3 activities per month.
Selected Home and Group Comparisons.
Reach
The targeted groups of residents for this intervention were those who were able to communicate verbally to some extent within a group discussion format. Their degree of involvement was noted by attendance and participation in the group processes, for example, sharing with the talking stick, singing along with the music, and/or assisting. In the observations it was clear that, although the verbal responses of those with lower cognitive functioning was often jumbled, their facial expressions and body language demonstrated focused social and emotional involvement. It was hoped that some of the residents who tended to be more isolated would attend the program regularly, and to some extent this occurred (7.7% of those with little or no attendance in home programs and 24.6% of those with some attendance).
Fidelity
To assess the extent to which program implementation was consistent with the steps outlined in the manual, scheduled observations were conducted in the first and last month. Staff observed that the manuals provided adequate guidance and that the supportive materials worked effectively for the residents. They described how the photographs, music, and readings all served to increase the participants’ interest and ability to focus and that these components deepened the levels of sharing. They also talked about the importance of the talking stick, calling it a “fantastic tool” that enabled quieter residents to speak up—some for the very first time.
A number of recommendations for program refinement were identified by staff and these include revising the recordings to lower keys, use of a decorated talking stick to help residents with higher cognitive impairment identify its purpose, increased usage of the photographs, optimal groups sizes (8 to 10 residents), use of the word assistant rather than leader, and the use of a volunteer to help with set-up and clean-up.
Program components delivered and received
Of the 23 environmental and intervention components, 17 were achieved (see Table 5). Of the total sample, 84.6% of the residents attended at least the minimum number of groups (6 out of 12 sessions) and 73.8% attended most of the groups (10 to12 sessions). Although the staff experienced some time challenges in assisting the residents to the program each week, the attrition rate was low (15.4%; see Figure 2). Only five of the participants refused invitations to attend, and it was noted that, of those five, four attended no other programs and one attended sporadically. The refusals for these participants centered on not being physically well and/or not wanting to leave their rooms. Of the participants who did attend, only two were not able to continue—one due to increased confusion related to the progression of their dementia and one due to illness. Three residents moved to another home (were discharged) before the individual interviews could take place. The intent was to interview those who dropped out of the program, but the two remaining at the home were not able to remember that they were invited to participate in the study or what the program was about.
Completed Environmental and Intervention Components.
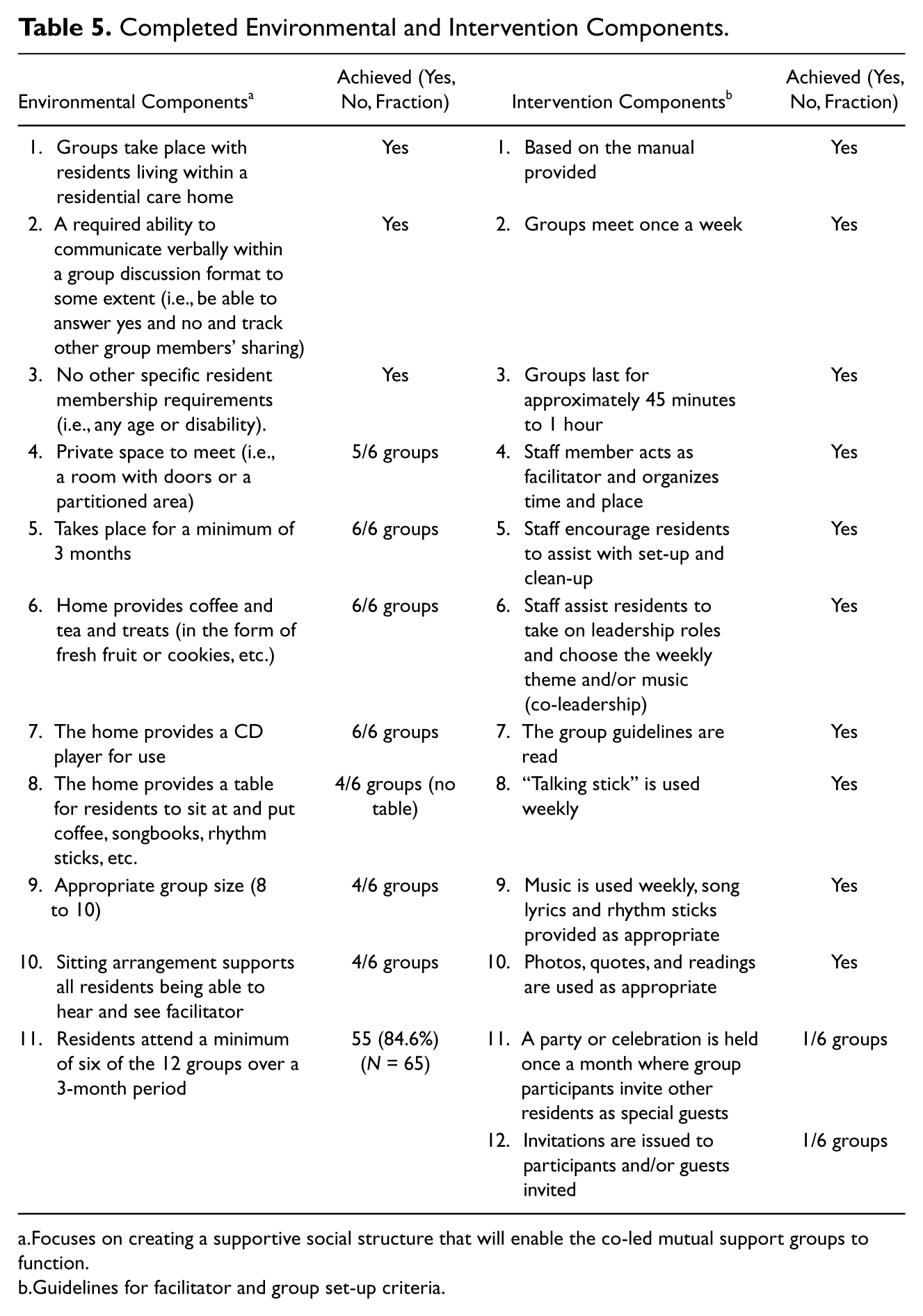
Focuses on creating a supportive social structure that will enable the co-led mutual support groups to function.
Guidelines for facilitator and group set-up criteria.

Initial Sample and Attrition Chart.
It was apparent from the observations and from the individual interviews that almost all attending residents actively participated and enjoyed the program. The majority appeared to enjoy the music and singing; toe-tapping and movement to the rhythm of the music was often noted. Most of the time residents listened attentively to one another’s sharing, leaning in closer to hear, making compassionate responses such as “ . . . me too,” laughing or responding with suggestions, and so forth. Only a few residents were not always engaged: two residents were extremely hard of hearing, a third spent some of the time talking to herself and looking through the songbooks, and on occasion, some of the participants fell asleep.
Context
In their interviews, staff talked about numerous personal benefits associated with facilitating the mutual support groups, including becoming more engaged and connected with residents. They also, however, described the daily stress experienced from trying to meet the needs of too many residents and ongoing challenges in recruiting and inviting residents with not enough scheduled time. When comparing the three homes, there were two characteristics that stood out. Home C had the highest prevalence of indicators of dementia (85% compared to 46.2% [Home B] and 59.4% [Home A]), and Home A had comparatively high levels of active participation in activities (90.6% as compared to 46.2% [Home B] and 45% [Home C]).
Evaluation of the Program
Participating in the mutual support groups was a positive experience for the majority of the residents. To assess the resident satisfaction with the program, interviews were conducted beginning with the standard open-ended question, “Do you have any comments or thoughts on the program you are taking part in?” followed with specific questions that included, “Do you enjoy the Java Music Club? ...Why or why not? ... Please elaborate.” Of those able to be interviewed (n = 55), 96.4% said they enjoyed the groups (Table 4). Salient themes were identified and a comparative analysis completed of the cognitively higher functioning residents (MMSE scores ≥ 21) and the cognitively lower functioning residents (MMSE scores ≤ 20). There were some divergences and these centered on challenges that some residents encountered. Those with higher cognitive functioning had concerns about their abilities to help, not being able to sing, and being too old. Those with lower cognitive functioning expressed confusion around the talking stick and some anxiety about taking on a leadership role. Where they were similar was in the benefits they experienced around helping others.
The investigative team identified a thematic framework using the five program objectives as an analysis guide and four themes emerged: helping one another, having a say, building relationships, and finding new ways to cope (Table 6). These themes were then linked back to the program’s objectives. The first objective revolved around increasing self-determination, and this objective was met through the active participation of the group participants in helping to facilitate the group, choosing themes, making choices regarding music, taking ownership by helping with set-up/clean-up, and inviting guests. The second objective to increase giving and receiving help was evidenced by the frequency with which mutual support was observed to be both offered and received (the theme of helping one another). The third objective focused on building inner-strengths, beliefs, and abilities, and the talking stick was instrumental in providing a vehicle with which quieter participants were able to speak up (the theme of having a say). The fourth objective was to strengthen supportive relationships, and both the residents and staff reported developing friendships (building relationships). The fifth and final objective was to increase expression of challenges that residents faced in a way that allowed for new interpretations, and this was met in varying degrees as group members offered advice to one another and shared their successes and failures (finding new ways to cope).
Qualitative Comments on the Mutual Support Groups From Residents and Staff.
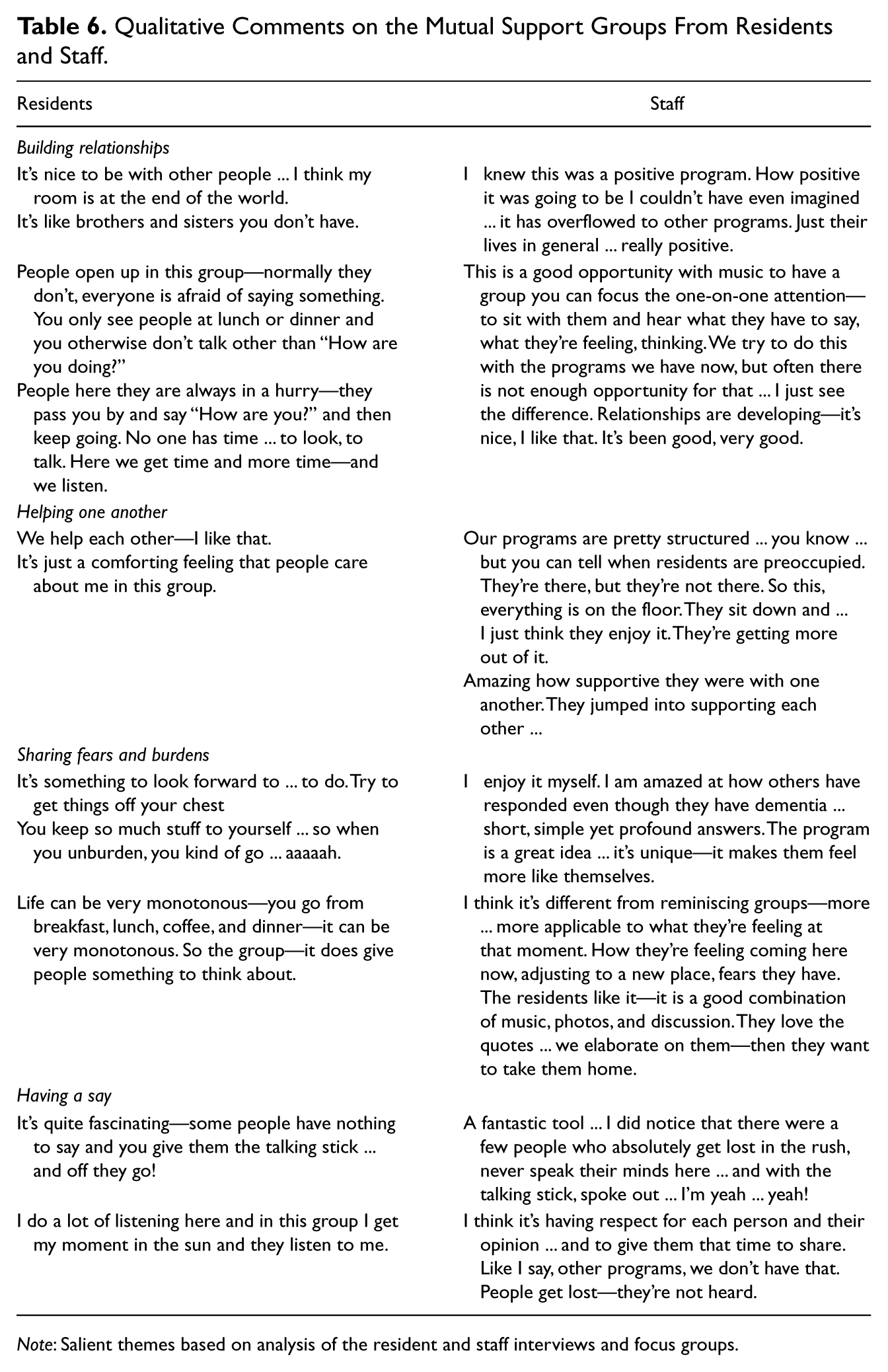
Note: Salient themes based on analysis of the resident and staff interviews and focus groups.
Staff Interviews
Staff also enjoyed the program and felt that the unique combination of program components helped to keep the pace moving along and the program interesting from week to week. Music provided context to the themes and helped keep the discussions focused. Six of the seven staff members had no musical skills but stated that the recorded music worked well. They also shared some of the challenges they faced in facilitating the groups. One group was held in a partitioned but open area, and therefore, distractions were a problem, and two of the groups were too large, with 13 members in each.
Discussion
The goal of this study was to develop and implement a new mutual support group intervention in LTCH and to evaluate its process, structure, and content. Almost all the participants in this study had some form of cognitive impairment, and close to half had moderate to severe cognitive impairment. Although it would appear that a verbal discussion program such as a mutual support group would not work well with this population, observations and interviews of participants revealed that not only did those with mild-moderate cognitive impairment actively participate and appear to benefit, but some of those with severe cognitive impairment did as well. The overall findings are in keeping with Kitwood’s (1997) theory of the psychotherapeutic interactions that promote positive relationships. The phenomena of caring and being cared about was the most frequent response by both the residents and the staff, attesting to the importance of attending to this need.
With respect to the delivery of the program, it was found that, despite a few problems encountered with the facilitation, most of the environmental and intervention components were used correctly and the objectives of the intervention were achieved. The active involvement of almost all of the participants and the low attrition rate enabled group members to fully experience the benefits of the support available. Although there was no direct measurement of outcomes, the interviews and structured observations revealed several validated themes: self-determination (taking on leadership), giving and receiving help to one another, discussions of their inner-strengths and beliefs, and expression of the challenges they were facing and how to better cope with them. The findings lend support to Kitwood’s concept of personhood in the context of relationships and specific group components that empower residents. The talking stick, for example, highlights the importance and value of each person in the group. This is particularly important since activity programs often focus on those residents who are more able, outspoken, and socially active. The mutual support group format allows the voice of typically withdrawn residents to be heard and validated. The talking stick played a significant role, and the use of it seemed to grant participants courage to share more than was usual in their social circles.
The supportive group structure also appeared to play a significant role in encouraging group participants to make new social contacts and develop connections with other residents. These ties were further developed by offering group members opportunities to give and receive help during and after the groups. Being of help to others is not commonly associated with residents in LTCH, however it is in keeping with studies of older Canadians in the community that suggests that engaging in helping behaviors increases a sense of belonging and feelings of connection to others (Theurer & Wister, 2010). Residents also reported that group members, who had a more difficult time expressing themselves, appeared to be empowered by observing others.
The inclusion of music served to meet a number of the objectives of this intervention: to increase self-determination (residents chose the songs), to strengthen supportive relationships (singing brought them closer together), and to increase expression of challenges (enhanced self-expression after the music). The participants reported enjoying the variety of the program components, including the music, the quotes, the talking stick, and the photographs.
Some of the recommendations identified by staff for program refinement are simple revisions easily done, such as increased usage of the photographs. Other recommendations are more difficult to implement. For example, keeping the group sizes from 8 to 10 residents will likely be more problematic since it is difficult for staff to turn away interested residents. Finding regular volunteers can also be a challenge. Another recommendation that may be difficult to achieve due to financial constraints is re-recording the songs in lower keys. This would, however, increase the group members’ active engagement with the music.
Based on the analyzed data from the four themes that developed, the objectives of the intervention were met. These objectives reflect Riessman’s self-help principles, and the findings attest to the benefits of the bidirectional support structure of this new intervention (Riessman, 1997). As more residents took on helping and supportive roles, the ability of each member to be of help was strengthened. Observations also revealed residents developing new friendships and becoming increasingly engaged in the group processes.
Replication Considerations and Sustainability
The presented findings document the potential of mutual support groups to act as an effective and practical intervention to help address barriers and constraints on resident autonomy. The staff of the two secured unit groups found that the program worked effectively with some adaptations. The adaptations included increasing the use of the photographs and music, simplifying the guidelines, keeping the questions short and concrete (rather than abstract), not using the song lyric sheets, using a decorated talking stick, and clearly repeating and/or paraphrasing the participants’ responses.
The use of existing staff and resources available within a home makes this program cost-effective; the standardized manuals and training make it sustainable. There was a remarkably low attrition rate over a 6-month period, and almost all the participating residents enjoyed the program and experienced benefits. In addition, the majority of the study participants attended most of the group sessions, the groups continued to meet after the study completed, and more groups were added. Staff found the standardized manuals easy to use and expressed enjoyment in facilitating the program, increasing the likelihood of the programs’ sustainability.
Several limitations need to be identified. This relatively small sample was based in three care homes within one geographical region and was predominantly female. The purposive sampling technique meant that there could also be a selection bias. Since it was not possible to interview the participants who dropped out, the results may be biased in favor of the program. In addition, the principal investigator was involved in both the design of the program and its evaluation, and the inter-rater reliability of the students was not assessed. However, the use of an audit trail, self-reflexivity processes during the study, and a committee to validate interpretations mitigated potential biases.
The strength of this evaluation lies in the choice of method triangulation including descriptive, qualitative, and focus group methods that provide corroborating evidence of the findings. The positive consensus of resident and staff reports in both the interviews and focus groups indicate that regular participation in the mutual support groups facilitated empowerment. Based on the analyzed data from the four themes that developed, the objectives of the intervention appear to be validated. Additional evaluations are required to provide evidence of the program’s effectiveness in alleviating loneliness and depression in LTCH.
Future research could include a pre- and post-test quasi-experimental design with an inert control condition to ascertain if the relative effects of the mutual support group intervention can be identified. True random assignment is not practical within the natural setting of a long-term care home, however once selected and available participants have expressed interest, they can be randomly assigned to a treatment and control group (delayed program inclusion) within each care home (i.e., both groups operation within each home).
Future research might also explore the use of the mutual support group format for enhancing the effectiveness of resident council meetings within LTCH. An exploration of institutionalized resident experiences and coping strategies based on recording resident council meetings and interviews highlighted a range of unmet needs (Timonen & O’Dwyer, 2009). In this clinician’s experience, frustration is often expressed by the residents over limited opportunities to participate in decision making concerning their lives. Due to the increasing complexity of health needs and levels of disability in homes, having resident council meetings that are both inclusive and representative is a challenge. A pilot is underway in one of the research sites using the mutual support group in each area as a foundation for a more effective council structure. Clearly delineating the psychosocial role of the mutual support group and the advisory role of Residents’ Council is improving the effectiveness of both. With a positive mutual support structure in place, more residents are prepared and confident to engage in decision making within the home, thus increasing the chance of taking on a more active role in Resident Council meetings.
To our knowledge, this study is one of the first to explore the mutual support group structure within LTCH. Introducing mutual support groups as a part of a system of care within LTCH has a number of potential benefits. The format creates a group dynamic that encourages individual participation. With a positive support structure in place, more residents will be empowered to engage in decision making. Given the disparity between the unmet needs of residents and the costs of individual care, offering opportunities for residents to engage regularly in mutual support groups could provide cost savings. Finally, although further research on outcomes is needed, mutual support groups represent tremendous therapeutic potential for decreasing the loneliness, helplessness, and depression currently prevalent in care homes.
Footnotes
Declaration of Conflicting Interests
Subsequent to this study, the principal investigator is presenting the Java Music Club mutual support group program at conferences and to health professionals and is receiving financial remuneration for program materials and workshops.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada [766-2007-0656]; and the Michael Smith Foundation for Health Research [ST-JGS-01379-(07-1)POP].