
Abstract
Residential care/assisted living (RC/AL) communities are home to more than 835,000 residents nationwide (Caffrey, Harris-Kojetin, & Sengupta, 2015) providing care for older adults and younger adults with disabilities who cannot live independently but do not require the level of care provided in nursing homes (Rome & Harris-Kojetin, 2016). Interest in the RC/AL industry can be attributed to consumer preference for noninstitutional yet supportive housing as well as shifts in federal and state policy that are beginning to incentivize community-based long-term care services and supports over nursing home care. Regrettably, the median length of stay in RC/AL settings is a short 22 months, and 60% of residents eventually move to a nursing home (National Center for Assisted Living, 2010).
In compliance with state regulations, RC/AL communities may set policies for admission, retention, and discharge, but in some cases may not be permitted to provide increasing levels of care as residents’ functional status declines (Kissam, Gifford, Mor, & Patry, 2003). Already frail and medically complex, the onset of an acute medical problem prompts hospitalization for 32% to 39% RC/AL residents annually (Hogan et al., 2014; Sloane et al., 2011). Compared with services offered in nursing homes, the lack of registered nurse staffing, limited availability of diagnostic and therapeutic procedures, and difficulties prescribing and receiving medications impede medical care provision in RC/AL (Sloane et al., 2011). As a case in point, findings from the seminal Collaborative Studies of Long-Term Care, a multistate study of 2,078 residents in 193 RC/AL communities, showed that residents with greater physical and cognitive impairment, higher depressive symptoms, and lower social activity had a higher annual risk of discharge to a nursing home or death, with an annual mortality rate of 14.4% and nursing home transfer rate of 21.3% (Giuliani et al., 2008; Zimmerman et al., 2005). Similar annual rates and risk factors for transition from RC/AL to nursing homes and death have been reported in other studies (Maxwell et al., 2013; Phillips et al., 2003). In addition, the presence of a psychiatric disorder combined with functional and/or cognitive impairment presents greater risk of nursing home relocation, due in part to an inadequacy of psychiatric care that might ameliorate the combined effect of psychiatric conditions, cognitive impairment, and physical dependency (Dobbs, Hayes, Chapin, & Oslund, 2006; Watson et al., 2006).
Fortunately, the rate at which functional limitations and disability progress with advancing age can be altered by regular physical activity (Hatch & Lusardi, 2010; Keysor, 2003; McAuley et al., 2007). As a major theoretical framework guiding our understanding of function and disability, the disablement process model suggests that pathology (i.e., disease, injury, or congenital conditions) may lead to impairments—dysfunctions and abnormalities in bodily systems—that affect functioning and may produce discernable symptoms (Verbrugge & Jette, 1994). Functional limitations develop when impairments restrict an individuals’ performance of activities essential to daily life and ultimately lead to disability if these limitations threaten one’s ability to perform expected or specific societal tasks. Potentially influencing this pathway trajectory are intraindividual and extraindividual factors that can speed up or slow down disablement. Intraindividual factors, including behaviors such as physical activity and attitudes such as self-efficacy, impact the extent to which functional limitations develop and progress (McAuley et al., 2007). The social and built environment, medical care, and therapeutic regimens represent extraindividual factors in the model. Finally, the disablement process can result in adverse outcomes, such as hospitalization, institutionalization, and death.
Cross-sectional research indicates that higher levels of physical activity are associated with fewer functional limitations and less disability in RC/AL residents (Phillips et al., 2016, 2016; Hall & McAuley, 2011). Several experimental studies with 12-month follow-up reported beneficial effects of residents’ physical activity on functional outcomes. A physical therapy-guided wellness intervention in a small sample of AL residents revealed that those who exercised at least twice weekly for 9 months had fewer falls and less functional decline than residents who exercised less often or not at all, but this difference was not statistically significant (Hatch & Lusardi, 2010). Resnick and Galik (2015; Resnick and colleages, 2011) found significantly less decline in physical function at 12 months for AL residents receiving their Function-Focused Care intervention compared with the control residents, and although physical activity remained higher in the intervention group, the difference was not statistically significant. Last, the subjective health status of 68 RC residents who had engaged in a once-weekly low-threshold physical activity intervention showed sustained improvement at 1 year compared with baseline, but follow-up of physical performance and physical activity were not reported (Quehenberger, Cichocki, & Krajic, 2014).
A better understanding of the factors affecting change in physical function and the development of adverse outcomes in the RC/AL population is needed to identify targets for intervention. Therefore, the purpose of the present study was to identify predictors of physical function at 6 months, as well as relocation to a higher care setting or death at 12 months (hereinafter called relocation), from among variables collected at baseline in a sample of RC/AL residents. Our research questions were as follows:
Method
Design and Participants
This study used a correlational, repeated-measures design to estimate 6- and 12-month outcomes from baseline data collected from 272 RC/AL residents aged 65 years and older enrolled in the Physical Activity and Disability in Residential Care/Assisted Living Residents study. Institutional Review Board approval from the University of Missouri was obtained in advance of study activities. Written consent was obtained from all participants who successfully completed the Evaluation to Sign an Informed Consent Document for Research (University of Iowa, n.d.). Responsible parties provided consent on behalf of four participants. Details of recruitment procedures are described elsewhere (Phillips et al., 2016). In brief, using mailed recruitment letters and telephone calls, we contacted administrators of 72 licensed RC/AL communities, and of those, 34 agreed to participate.
Onsite information sessions were held to recruit residents of participating communities. RC/AL residents who scored ≥17 on the Mini Mental State Examination-2 (MMSE) Standard Version (Folstein, Folstein, White, & Messer, 2010), were aged 65 years or older, could understand and speak English, and were able to give consent or assent were invited to participate. Exclusion criteria were as follows: (a) unstable medical or psychiatric illness (e.g., heart failure exacerbation, suicidal ideation), (b) terminal illness, (c) severe hearing and vision impairment, and (d) short-stay admission in the RC/AL (e.g., rehabilitation, respite, or terminal care). Our sample of 272 residents reflects a 62% recruitment rate.
The research team collected resident data by chart review, face-to-face interviews for self-report measures, and direct observation for performance-based measures. Staff and/or administrators independently completed questionnaires pertaining to the RC/AL community.
Measures
Variables in these analyses represent the Disablement Process Model’s risk factors, pathology, impairments, functional limitations, intraindividual and extraindividual factors, and adverse outcomes (Verbrugge & Jette, 1994). Figure 1 displays study measures corresponding to disablement constructs included in the present study.
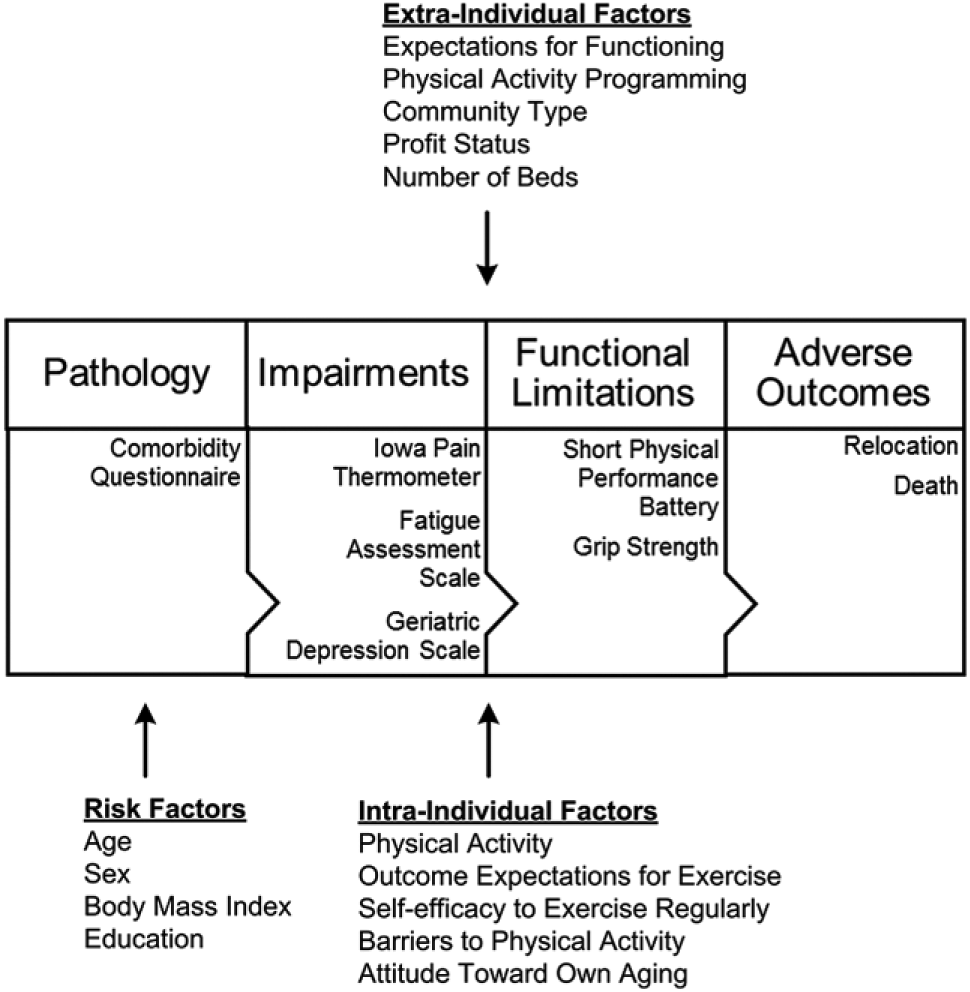
Study measures representing Disablement Process Model constructs.
Demographic characteristics and pathology
Representing risk factors in the disablement process model, demographic characteristics, height, and weight were abstracted from charts. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Pathology was captured with the Comorbidity Questionnaire, modeled after the Charlson Index and with demonstrated test-retest and concurrent validity (Charlson, Pompei, Ales, & MacKenzie, 1987; Katz, Chang, Sangha, Fossel, & Bates, 1996). The Comorbidity Questionnaire includes the same 19 conditions as the Charlson Index and allows participant report of data missing in the medical record. Scores on the Comorbidity Questionnaire range from 0 to 32, with higher scores representing greater comorbidity.
Impairments
Validated measures of pain, fatigue, and depressive symptoms represented impairments, mediating the relationship between pathology and functional limitations in the disablement pathway (Bennett, Stewart, Kayser-Jones, & Glaser, 2002; Penninx, Deeg, van Eijk, Beekman, & Guralnik, 2000). The Iowa Pain thermometer is a single-item pain scale that contains seven descriptors of current pain intensity from no pain to the most intense pain imaginable, plus numeric response options between words (Herr, Spratt, Garand, & Li, 2007). Pain scores may range from 0 to 12, with higher scores indicating more pain. The Fatigue Assessment Scale measures 10 fatigue symptoms on a 5-point Likert-type scale; scores range from 10 to 50, with higher scores reflecting greater fatigue (Michielsen, De Vries, & Van Heck, 2003). Cronbach’s alpha of the Fatigue Assessment items was 0.82 in the present study. The Geriatric Depression Scale-15 (Sheikh & Yesavage, 1986) is a self-report scale that solicits yes/no responses to simple questions about one’s feelings during the past week. Scores range from 0 to 15, with higher scores indicating greater symptoms. Internal consistency reliability in the present study (α = 0.76) was acceptable.
Intraindividual factors
Physical activity, defined as “any bodily movement produced by skeletal muscles that results in energy expenditure,” was operationalized as daily walking and recorded with the Fitbit® Tracker (Fitbit Inc., San Francisco, CA; hereafter called Fitbit) that participants wore at the lateral waist for three consecutive days from morning to night (Caspersen, Powell, & Christenson, 1985). The Fitbit is a triaxial accelerometer that uses three-dimensional motion sensing technology similar to the Nintendo Wii technology (Montgomery-Downs, Insana, & Bond, 2012). Activity, recorded in 60 s epochs, is displayed on a web-based server as steps taken in 5-min intervals. Prior to distribution, research staff verified that steps recorded on the Fitbit matched a count of test steps. Based on high between-day reliability for accelerometer steps (intraclass correlation coefficient = 0.87) over as few as 2 days of monitoring in older adult samples (Rowe, Kemble, Robinson, & Mahar, 2007), we adopted a 3-day wear schedule to minimize both respondent burden and missing data. Participants and RC/AL staff received written and verbal wear instructions. Research staff put the Fitbit on participants and placed reminder calls to RC/AL staff to reinforce the 3-day wear schedule. Fitbits were not distributed to 10 participants whom staff believed would not consistently wear the device or would lose it, and to another 14 participants who ambulated with wheelchairs.
As an intraindividual factor, physical activity may be influenced by psychosocial attributes that are themselves intraindividual factors. Psychometrically sound measures of outcome expectations, exercise self-efficacy, perceived barriers, and attitude toward aging were used to assess intraindividual factors. The Outcome Expectations for Exercise Scale (Resnick, Zimmerman, Orwig, Furstenberg, & Magaziner, 2000) assesses perceived physical and mental health outcomes of exercise. Respondents rate the extent to which they agree or disagree with nine statements on a 1 to 5 scale with higher mean scores reflecting more positive outcome expectations. Internal consistency reliability (α = 0.93) in the present study was excellent. The Self-Efficacy to Exercise Regularly Scale is a 3-item scale to rate one’s confidence for gentle exercise, aerobic exercise, and exercise without making symptoms worse (Lorig et al., 1996). Items are scored from 1 (not at all confident) to 10 (totally confident) and averaged. Cronbach’s alpha was 0.67 in the present study, whereas Lorig et al. (1996) reported internal consistency coefficients ranging from 0.77 to 0.92. The Barriers to Physical Activity Subscale of the San Diego Health and Exercise Questionnaire–2-year follow-up version (Sallis, 2010) asks respondents to rate 16 items on a 0 to 4 scale describing various problems that keep them from exercising. Higher summed scores indicate greater perceived barriers. Internal consistency reliability (α = 0.85) was good in the present study. The Attitude Toward Own Aging subscale of the Philadelphia Geriatric Center Morale Scale (Lawton, 2003) contains five items about perceptions of aging. Using yes/no or better/worse formats, questions address potential changes in one’s life as a result of aging; higher scores reflect more positive perceptions. Cronbach’s alpha was 0.64 in the present study, slightly lower than the previously reported alpha of 0.75 (Kleinspehn-Ammerlahn, Kotter-Gruhn, & Smith, 2008).
Functional limitations
The research team administered the Short Physical Performance Battery (SPPB) to evaluate physical function (Guralnik et al., 1994). Tests of standing balance, gait speed over a distance of 4 meters (m), and repeated chair rise are each scored on a 0 to 4 scale and summed to yield a total performance score from 0 to 12. Cronbach’s alpha was 0.62 in the present study. Participants who relied on wheelchairs for ambulation could accept or decline SPPB testing; nine of 14 wheelchair ambulators performed at least one of the component SPPB tests.
Immediately following SPPB testing, we assessed grip strength, an indicator of upper extremity strength, with the Jamar Hydraulic Hand Dynamometer three times in each hand, in accordance with the American Society of Hand Therapists procedures (Shechtman, Mann, Justiss, & Tomita, 2004). The greater value of the right or left mean hand strength in kilograms was used for data analysis.
Extraindividual factors
Administrators completed the Expectations for Functioning subscale of the Multiphasic Environmental Assessment Procedure Policy and Program Information Form, a measure of the community’s intolerance for residents who are unable to, for example, dress themselves or make their own beds (Moos & Lemke, 1996). Raw scores were converted to percentages, with higher percentages indicating higher expectations for functioning. Internal consistency reliability in the present study was 0.80. Activity staff completed a questionnaire developed for the present study to record the frequency of each type of physical activity program offered per week. Activity options included chair exercise, structured walking, strength training, stretching, balance, dance, and water exercise. Administrators also provided descriptive information about their community, RC or AL licensure, for-profit or not-for-profit status, and number of beds.
Relocation and death
At 6- and 12-month data collection, the research team asked staff for information on the whereabouts of participants who no longer resided at that community. Data indicated whether residents permanently relocated to a nursing home, intermediate care residence, or hospice, or had died. Because the number of events was low, these analyses combined relocation and/or death as “yes” versus “no” (no relocation or death). Residents who had relocated at 6 months to an equivalent level of care (e.g., with family or another RC/AL community) were excluded from the analysis as we could not confirm their disposition at 12 months.
Data Analysis
Data were cleaned and checked for incorrect values. Basic summary statistics were calculated for all variables. Physical activity was summed in steps per hour, rather than steps per day, to account for variation in duration of wearing the Fitbit. Then, each participant’s three maximal non-zero hourly counts over the 3-day wear period was averaged to estimate their observed capacity for physical activity. The distribution of raw physical activity was skewed because a few participants had very large maximal hourly count values (e.g., 3,000–4,000 steps/hr); therefore, for statistical analysis purposes, the natural logarithm of activity was used but is referred to as “physical activity capacity” from here on.
All analyses were performed using SAS v9 (SAS Institute Inc., Cary, NC, USA). SAS’s GLIMMIX procedure was used to evaluate potential differences between RC and AL residents and Wilcoxon rank sum tests evaluated differences between RC and AL communities. Data analyses were optimized for a larger sample at the 6-month analysis to examine change in physical function and a longer follow-up at 12 months to predict adverse outcomes. The independent variables considered in the analyses for both research questions included baseline age, sex, years of education, BMI, comorbidity score, pain score, depressive symptoms score, fatigue score, physical activity capacity, exercise self-efficacy, outcome expectations for exercise, perceived barriers to exercise, attitude toward own aging, grip strength, physical function score, and RC/AL community-specific characteristics for the number of beds, profit type, number of physical activity programs, mean expectations for functioning, and RC or AL. Both analyses used a backward elimination approach from among the 20 original predictor variables, and only those variables with statistically significant coefficients at the p < .05 level were retained in the models. To predict 6-month physical function (i.e., SPPB score), multiple linear regression with the GLIMMIX procedure was used to allow use of the RC/AL community as a random effect to account for clustering of respondents within a community.
To predict the dichotomous outcome of relocation/death at 12 months, logistic regression using random RC/AL effects were used with the GLIMMIX procedure. We checked the linearity assumption for retained variables by dividing the values into deciles and examining the plot of the log-odds of outcomes within the deciles against the midpoint of the decile.
Results
Baseline descriptive statistics for 272 participants and 34 RC/AL communities are presented in Table 1. Participants were primarily White (99%), female (81%), and widowed (70%), with a mean age of 85 years. Eighteen communities were licensed as AL. The majority of communities were for-profit (77%) with an average of 49 beds. RC and AL residents had similar demographic characteristics and scores on study variables as shown in Table 1. Comparisons of community characteristics revealed that only the number of physical activity programs (8.0 vs. 4.3) differed significantly by RC or AL licensure (p < .01).
Baseline Descriptive Statistics for Participating Residents (N = 272) and Residential Care/Assisted Living Communities (N = 34).
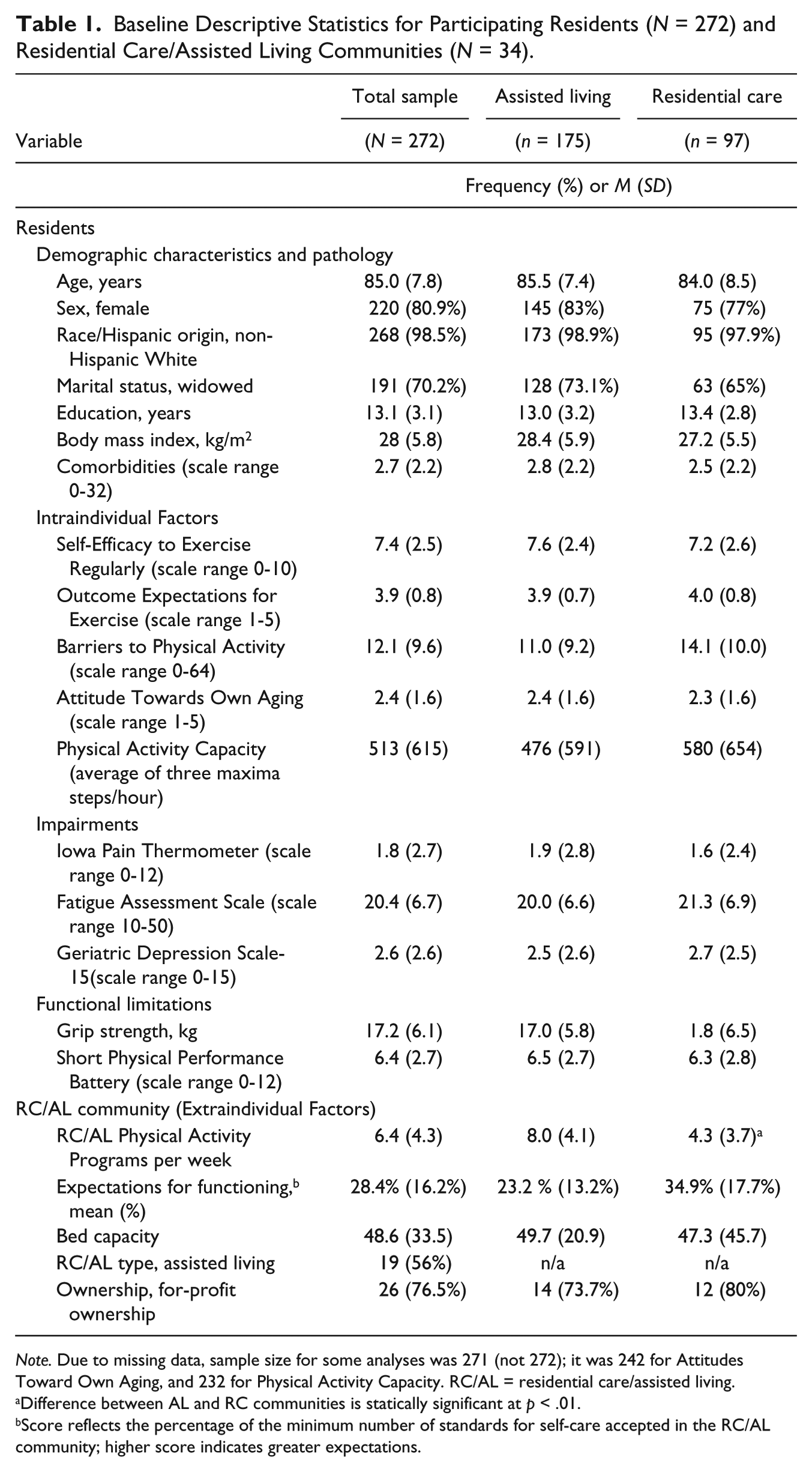
Note. Due to missing data, sample size for some analyses was 271 (not 272); it was 242 for Attitudes Toward Own Aging, and 232 for Physical Activity Capacity. RC/AL = residential care/assisted living.
Difference between AL and RC communities is statically significant at p < .01.
Score reflects the percentage of the minimum number of standards for self-care accepted in the RC/AL community; higher score indicates greater expectations.
At 6 months, 207 participants were available for data collection. Table 2 details the reasons for attrition at both 6 and 12 months. Chi-square and Kruskal-Wallis tests revealed no statistically significant differences in demographic characteristics (age, sex, education, race, ethnicity, and marital status) or health characteristics (BMI, MMSE score, and Comorbidity Questionnaire score) between the baseline and 6-month samples. The mean physical function score at baseline for the participants who would remain at 6 months was 6.66 (standard error [SE] = .19) compared with 5.55 (SE = .29) for the 67 participants who left the study (t = 2.94, p = .004). The 6-month samples’ physical function score was 6.56 (SE = .20). Table 3 displays results of the linear regression analysis to predict 6-month physical function for the 205 participants with outcome data; baseline physical function, grip strength, gender, and community type were statistically significantly at the p < .05 level. Physical function score increased 0.67 points for every 10 kg increase in grip strength. Females’ 6-month physical function score was higher (6.59, SE = .19) than males’ (6.41, SE = .23). In addition, RC residents had higher 6-month physical function scores (6.96, SE = .20) than AL residents (6.32, SE = .20).
Reasons for Attrition at 6 and 12 Months.
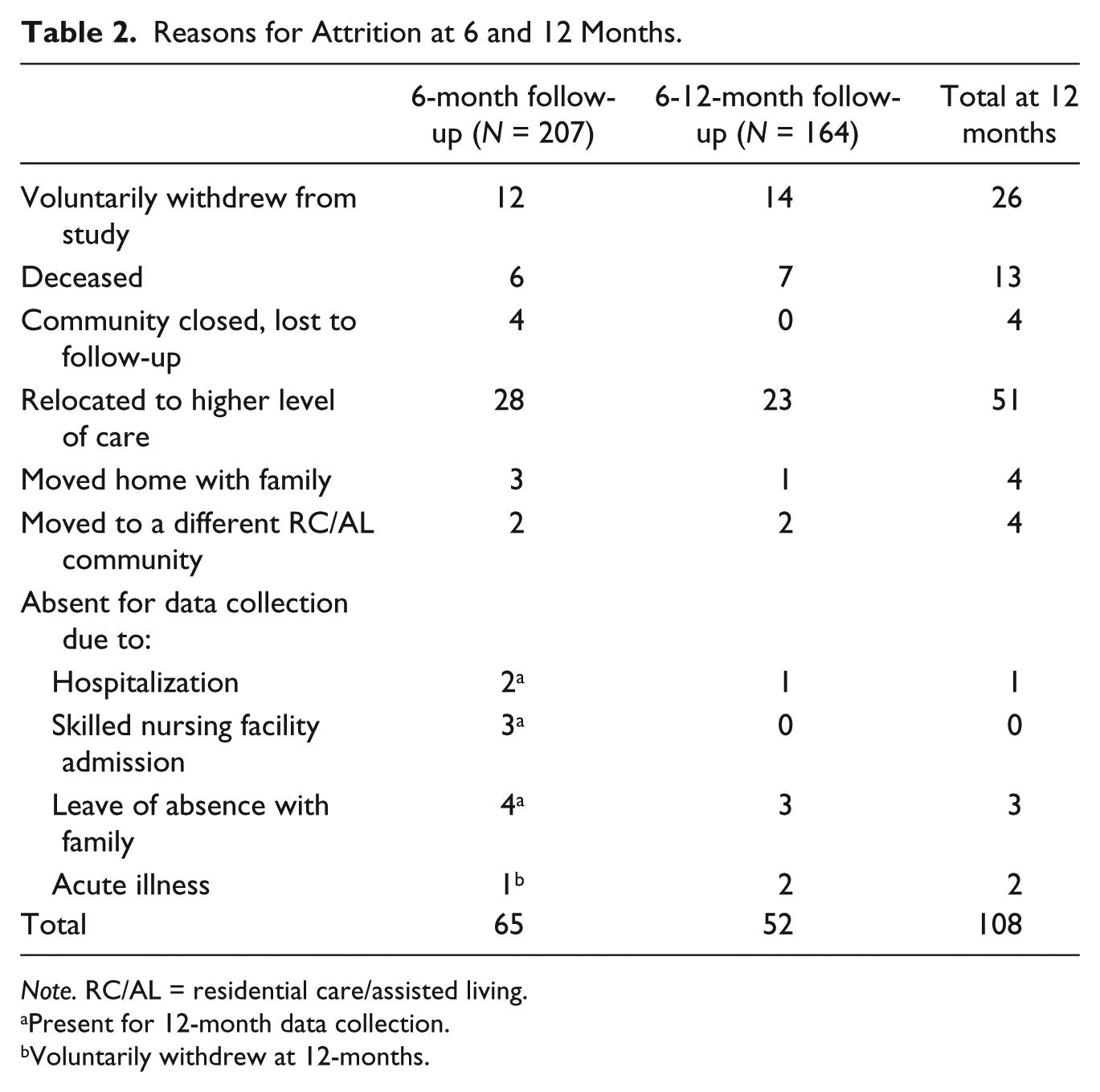
Note. RC/AL = residential care/assisted living.
Present for 12-month data collection.
Voluntarily withdrew at 12-months.
Predictors of Short Physical Performance Battery Score at 6 Months (N = 205).
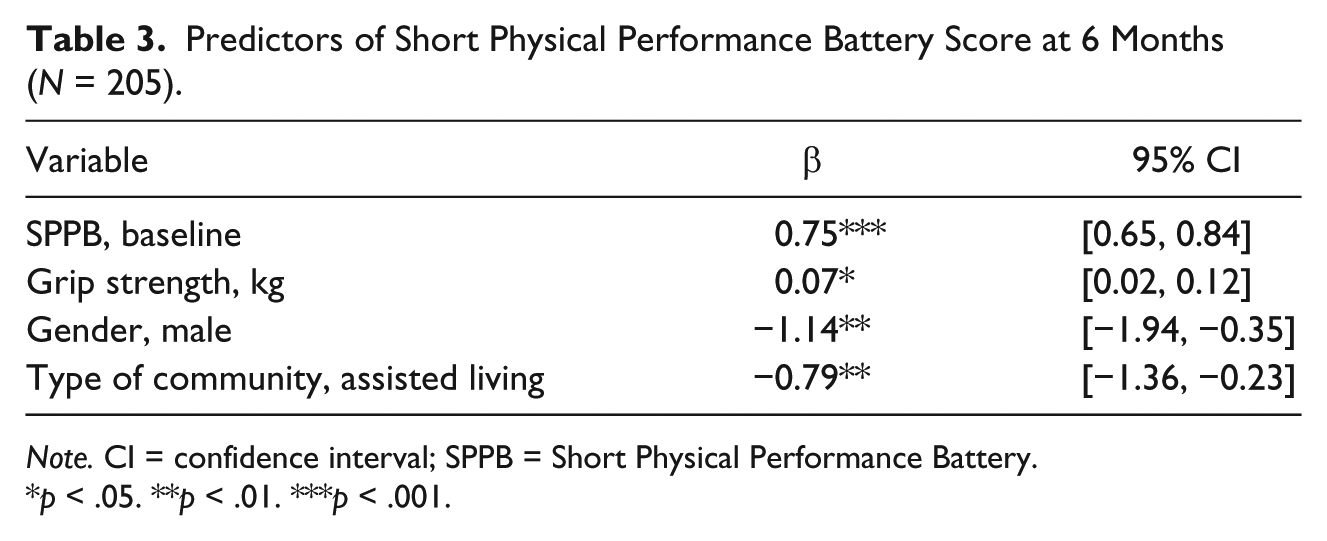
Note. CI = confidence interval; SPPB = Short Physical Performance Battery.
p < .05. **p < .01. ***p < .001.
By 12 months, 164 of the original 272 participants remained. As with the 6-month sample, no statistically significant differences in demographic or health characteristics were observed between baseline and 12-month samples. Outcome data (i.e., 12-month disposition) was missing on 22 of the original 272 participants. Of the 250 participants for whom 12-month disposition was known, 64 (25.6%) relocated to higher care or died. The final logistic regression model included the 249 participants with complete data on predictors significant at p < .05 (i.e., physical function and depressive symptoms). The odds ratio for relocation or death at 1 year for a one-point increase in physical function score was 0.84 (95% confidence interval [CI]: [0.74, 0.95]), and for one-point increase in depressive symptoms score was 1.16 (95% CI: [1.03, 1.31]). The estimated probability of a relocation or death, when the depressive symptoms score was fixed at its median value of 2, as a function of physical function score is shown graphically in Figure 2a; as physical function improves, the probability of relocation or death decreases. Similarly, if the physical function score is held constant at its median of 6, the probability of relocation or death increases as depressive symptoms worsen (Figure 2b).
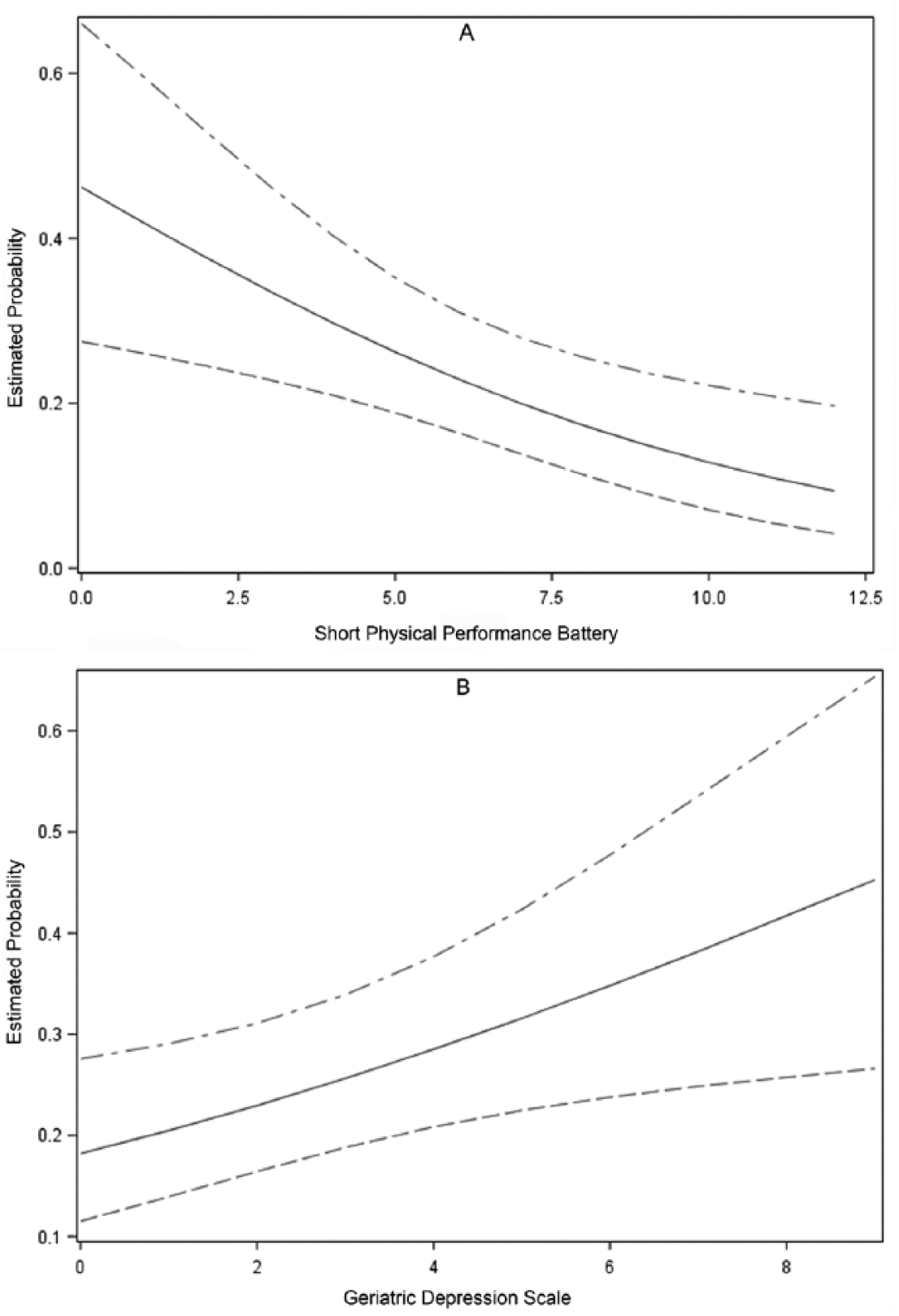
(a) Estimated probability of relocation or death as baseline SPPB score (range: 0-12) increases with baseline Geriatric Depression Score (range: 0-15) fixed at median level of 2; (b) estimated probability of relocation or death as baseline GDS score (range: 0-15) increases with baseline Short Physical Performance Battery score (range: 0-12) fixed at median level of 6.
Discussion
The present study examined individual and extraindividual factors related to 6-month physical function and 12-month relocation or death in RC/AL residents. Our sample compared similarly to RC/AL residents in the National Study of Long-Term Care Providers (Harris-Kojetin et al., 2016). Nationally, 93% of RC/AL residents were aged 65 years and older, 70% were female, 84% were non-Hispanic White, and 71% resided in communities with more than 50 beds (Harris-Kojetin et al., 2016).
In answer to our first research question, better baseline physical function (SPPB) and grip strength, female sex and RC community predicted better 6-month physical function, the latter of which remained relatively stable from baseline values, perhaps due to attrition of more frail participants. Of these statistically significant predictors, only physical function and grip strength are amenable to change. Our prior analysis showed greater disability for AL than RC residents, which is consistent with state regulations for RC communities that require persons admitted to RC be able to independently evacuate safely compared with AL where residents needing more than minimal assistance to evacuate may be admitted (National Center for Assisted Living, 2016). Baseline physical activity capacity (as measured by the FitBit) was not associated with 6-month physical function, standing in contrast to previous findings from this sample’s baseline data in which physical activity was significantly correlated with physical function (Phillips et al., 2016). Given that in at least some instances physical activity is correlated with physical function in this population, it seems important to continue improving means of measuring physical activity. The recent growth in the activity monitor market has yielded new designs and technologies with improved measurement accuracy and compatibility for older adult users (Floegel, Florez-Pregonero, Hekler, & Buman, 2017). The Fitbit One and the StepWatch are reported to have the least error across different ambulation abilities and offer either hip or ankle placement, respectively. Alternatively, self- or informant-reports of physical activity using the Physical Activity Scale for the Elderly or the Physical Activity Survey in Long-Term Care, respectively, capture multiple types of physical activity in which persons in wheelchairs may engage (Resnick & Galik, 2007; Washburn, Smith, Jette, & Janney, 1993). Generally considered a less valid method of measuring physical activity, questionnaires may be a useful adjunct to, or substitute for, accelerometer-measured activity in the RC/AL population.
In answering our second research question, and consistent with the disablement pathway, we found that residents with greater baseline depressive symptoms and poorer baseline physical function and had higher odds of relocation at 12 months than their counterparts with lower depressive symptoms and better physical function. It is surprising that extraindividual factors, especially AL licensure, did not predict 12-month relocation or death, because the 6-month analysis showed physical function scores were better for RC than AL residents. At 12 months, the combined rate of transfer to a higher care setting or death (25.6%) was lower than that observed in the Collaborative Studies of Long-Term Care (Zimmerman et al., 2005), a difference that may reflect the nonprobability sampling of both RC/AL residents and communities in the current study as well as the exclusion of individuals with dementia. Giuliani and colleagues (2008) found a significant association between physical performance measures and nursing home transfer, but not mortality; however, an important difference between that study and ours is that due to our smaller sample size and lower frequency of transfer and death, we combined both as an outcome. Finally, and unique to our study, was our examination of actual physical activity, which as measured with the Fitbit, had no relationship to relocation or death.
These study findings suggest that efforts to improve and maintain physical function could promote longer tenure in RC/AL. The Healthy People 2020 objective to reduce the proportion older adults with moderate to severe functional limitations (U.S. Department of Health and Human Services, 2017) has application to RC/AL settings. Prior research shows that regular exercise (defined as structured, repetitive, and purposeful physical activity done to improve or maintain fitness) helps older adults maintain or improve physical function that would otherwise decline (Caspersen et al., 1985; Hatch & Lusardi, 2010; Marshall & Berg, 2010; Sung, 2009), yet the availability of services to ameliorate functional decline—including occupational and/or physical therapy—varies widely depending on community size (Park-Lee et al., 2011). Attesting to the potential for additional services in RC/AL, a recent falls-related intervention study noted a lack of exercises other than those that were chair-based (Zimmerman et al., 2016), demonstrating how little exercise programming has changed in the past 20 years (Mihalko & Wickley, 2003; Wasner & Rimmer, 1997). Contrary to clear evidence that deconditioning resulting from sedentary behavior increases fall risk, literature indicates that RC/AL staff fear that residents will fall unless they remain seated for exercise, which poses a barrier to promoting more challenging activity (Galik, Resnick, Lerner, Hammersla, & Gruber-Baldini, 2015; Gruber-Baldini et al., 2011; Resnick, Galik, Vigne, & Carew, 2016). In a different vein, because mind-body exercise programs such as yoga and qigong improve physical function and also mood, well-being, and sleep, RC/AL providers may want to consider allocating resources to these types of holistic programs as well (Chen, Chen, et al., 2010; Chen, Fan, et al., 2010; Tsang, Fung, Chan, Lee, & Chan, 2006).
These findings also support increased attention to depression screening and treatment; not only did we find that greater depressive symptoms increased the odds of relocation and mortality, but other studies indicate that older adults with depression are more likely to experience a fall, which itself may result in hospitalization, nursing home transfer, and/or death (Ambrose, Paul, & Hausdorff, 2013). At all levels of lower extremity function (as seen in Figures 2 and 3), risk of relocation or death increased as depressive symptoms increased. Given that 23% of RC/AL residents have a diagnosis of depression, standardized depression screening in these settings, such as is mandated in nursing homes, could aid in identifying residents who may otherwise go untreated and experience adverse outcomes (Harris-Kojetin et al., 2016). The U.S. Preventive Service Task Force recommends depression screening of adults involved in programs that have adequate systems in place to safeguard correct diagnosis, effective treatment, and proper follow-up (Siu et al., 2016). As settings that provide, at a minimum, room, board, 24-hr oversight, and assistance with activities of daily living, RC/AL communities are well positioned to implement routine depression screening, as is done in nursing homes with the Mood Questionnaire (Azulai & Walsh, 2015). Unfortunately, depression screening is not standardized in the RC/AL setting, and only 52% provide mental health services (Azulai & Walsh, 2015; Harris-Kojetin et al., 2016). As recognition is the first step to accurate diagnosis and treatment of depression, the importance of screening cannot be overstated.
Some limitations of this study are worth noting. First, our sample was slightly less ethnically diverse than the general population of residential care users (Harris-Kojetin et al., 2016). Second, with nonprobability sampling, there may be some self-selection bias making the sample healthier and more active than would be other RC/AL residents. Third, because our 12-month analysis lacked the disablement pathway concept of disability, the extent to which disability may have been associated with adverse outcomes was not identified. In addition, the 12-month span of data collection may have been insufficient time to witness physical function decline, relocation, or mortality for some residents and mortality estimates may be slightly incorrect because we could not determine 12-month disposition for 22 residents who had relocated at 6 months. Finally, we encountered missing physical activity data because some participants did not receive (e.g., wheelchair ambulators) or consistently wear the Fitbit. Even with modifying the analysis of Fitbit data, 40 of 272 participants did not have usable physical activity data at baseline.
In conclusion, this study of RC/AL residents shows that issues affecting tenure in RC/AL communities persist two decades after earlier reports in the Collaborative Studies of Long-Term Care in 1997 (Zimmerman et al., 2005), indicating that there remains need for interventions to promote physical function. Strong evidence suggests that age-appropriate exercise programs can slow the age-related decline in physical function that prompts adverse outcomes for a large proportion of RC/AL residents, yet exercise programs are not commonplace in RC/AL settings. In addition, attention to depression screening and treatment, which remain unstandardized and lacking, may be fundamental to promote aging-in-place for RC/AL residents and maintain occupancy in RC/AL communities.
Footnotes
Acknowledgements
The authors would like to thank the residents, staff, and administrators of the participating communities that made this work possible. The authors appreciate Dr. Richard Madsen’s assistance with statistical analysis and Ms. Sandra Dearlove’s assistance with formatting graphics. Both Dr. Madsen and Ms. Dearlove are affiliated with the University of Missouri Sinclair School of Nursing, the latter of which provided their support.
Authors’ Note
The University of Missouri Health Sciences Institutional Review Board approved the study (Project number: 1185357).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (R15 NR012835-01).