
Abstract
In the UK context of financial austerity and the promotion of the social responsibility through the concept of the “Big Society,” volunteers are becoming a more important part of the labor workforce. This is particularly so in the long-term care (LTC) sector, where both shortages of staff and demands for support are particularly high. This article investigate the levels and profile of contribution of volunteers in the LTC sector using a large national data set, National Minimum Data Set for Social Care, linked to local area levels of rurality and socio-economic status. The analysis shows that volunteer activity in formal care services varies between sectors and service types, with no strong relationship between local area deprivation, unemployment levels, and levels of volunteering. However, some significant association was found with level of rurality. The contribution of volunteers is most evident in provision of counseling, support, advocacy, and advice.
Introduction
The first national adult social care workforce strategy in England identified volunteers as part of the adult social care workforce (Department of Health, 2009). Volunteer labor in social care and community support has long been prominent in the care of older people (Brenton, 1985; Netting & Thibault, 1986) and within the community care sector volunteer input has been thought important in developing a mixed economy of welfare (Knapp, Koutsogeorgopoulou, & Smith, 1996). There is new policy emphasis in England on maximizing volunteers’ potential contribution. In part, this is driven by theories about the benefits of enhancing social capital and civic engagement (Putnam, 2000), although some research shows that such links are not always guaranteed, especially when volunteering is not associated with freedom of choice to participate (Theiss-Morse & Hibbing, 2005). A further spur is the expanding demand for support associated with the growth of older people in situations of frailty and disability. For the United Kingdom Coalition Government, volunteering in formal and informal roles is one part of its aspirations to mobilize social responsibility through the “Big Society” (Alcock, 2010).
Social or civic engagement can take a number of forms, ranging from monetary donations to more active involvement through volunteering time and expertise. This donation of time is characterized as enhancing social linkages through the reciprocity and trust deemed so important to social capital (Putnam, 2000). In an environment of recession and public sector resource cuts, UK government policy points to the greater “scope” and opportunity for volunteering to sustain but also to develop support and care (Cabinet Office, 2010).
In the United Kingdom, early religious and philanthropic efforts led to a flourishing voluntary sector providing social care services among other expressions of mutual aid and social solidarity (Beveridge, 1948). The changing nature of some voluntary organizations within the care and welfare sector (Broadbridge & Parsons, 2003) has resulted in a highly differentiated sector, spanning “grass-roots” local activism to professional staff working at national and local levels, delivering complex services within not-for-profit organizations.
Given the current climate of financial austerity in the United Kingdom affecting public welfare services, it may not be surprising that volunteers in the care sector are seen as a resource that could be further developed. However, research about volunteering in the United Kingdom is limited, partly because studies of volunteering do not come under one discipline but cut across a number. In relation to volunteers in the social care sector, generally, as in most economically developed countries, the majority of volunteers offer their services to nonprofit or voluntary organizations, mostly undertaking human services work (Wilson et al., 2005; Butler & Eckart, 2007). International comparisons, however, are not always easy to make because the term “human services” may be broadly and variously defined.
The definition of the role of the volunteer is not fixed and includes notions that a volunteer in health and care services is principally a helper at the side of the trained professional, to “fill gaps” within services (Butler & Eckart, 2007), stretching to the belief that (if well trained) volunteers enhance professional services, may provide unique support (Cornes, 2007) and can also improve service quality (Manthorpe, 2007). Capitalizing on the unique contributions of volunteers may enable organizations to expand outreach activities (Hiatt & Jones, 2000) or offer personal one to one support (Wilson et al., 2005), whilst having a significant positive effect on volunteers’ own well-being (Greenfield & Marks, 2004).
The UK government’s Home Office (2001) Citizenship Survey data showed a high level of participation in civic affairs among the population, defined as engaging in at least one of a range of nine representative activities. Eighty-three percent of respondents had participated in civic affairs within the year preceding the survey. However, this “civic activities” list was wide, including items such as signing a petition or contacting one’s local council in addition to volunteering (Prime, Zimmeck, & Zurawan, 2002). People aged 35–49 years, White people, and men were most likely to participate in civic activities. Based on the Citizen Audit 1 (2000–2001) it is estimated that four million people in Great Britain volunteer their time and labor to formal organizations (Pattie, Seyd, & Whiteley, 2003). The same Audit showed that people volunteer most often in residential, sports, religious, and cultural organizations, suggesting considerable potential for the social care sector. Volunteering within a formal organization is usually defined as “highly active” civic engagement, in comparison to “modest participation” such as contacting a local politician or belonging to a social club (Crick, 2000; Attwood, Gurchand, & Prime, 2003). It is this “highly active” area of volunteering that this paper considers.
This paper reports on a literature review and statistical data analysis investigating evidence of volunteering within the formal adult care sector in England (defined as legally registered care providers) using the largest national data set available in England, the National Minimum Data Set for Social Care, the NMDS-SC. The NMDS-SC, introduced in 2005, was the first attempt to gather standardized information on the social care workforce in England (excluding health care). By the end of December 2010, the NMDS-SC had been completed by over 24,000 employers who provided detailed information on nearly 800,000 employees. Over 50% of all social care providers registered with the Care Quality Commission (CQC) had completed the NMDS-SC; in addition, the data set includes information gathered from non-CQC registered providers including small organizations and some people employing their own care workers (such as private home care aides). Although this data set largely covers the paid workforce, mainly care home workers (care aides) and home care workers, employers are requested to supply information on any volunteers as part of their workforce. Skills for Care, the sector skills body that operates the NMDS-SC, defines a volunteer within the workforce as a someone who performs: “Any activity which involves spending time, unpaid, doing something which aims to benefit others (individuals or groups) other than or in addition to close relatives, or to benefit the environment.”
The definition further states that a “voluntary worker” may “receive a small financial contribution towards the time spent.”
Design and Methods
This analysis utilizes recent data from the NMDS-SC, up to the end of December 2010. Using both the “provision” (the care providing organization) data on aggregate numbers of different types of workers and “individual workers” files, which contain data on individual workers’ characteristics, such as age, gender, and ethnicity, 2 we focused our analysis on organizations providing social care to adults including older people, thus excluding records related to children’s services. We expected the NMDS-SC to provide information on some, but not all, volunteers offering their time to the care sector. What is provided may be considered to be an “elected sample” of 7,534 volunteers, representing only those recognized and considered by providers of social care to fulfill Skills for Care’s definition of a “volunteer” or a “voluntary worker.”
Completion of the NDMS-SC by care providers is not compulsory but there are some financial and training incentives. Because of the nature of volunteering and voluntary work, providers may not consider some such workers to be part of their workforce and thus may not report them as such. This may be the case particularly if volunteer activity is not regular or consistent, both arising from the nature of some volunteering (e.g., assistance with celebrations) as well as the level and duration of participation of individual volunteers (e.g., students volunteering over a short vacation). Bearing this in mind, we explored the profile, characteristics, and possible associations between volunteering and different micro-, meso- and macrolevel factors. We first used aggregated information to explore where and how volunteers contribute to social care services. The “provision data set” provided information on the type of services provided by each registered care provider, the user or client group, the sector of “employment” and other organizational characteristics. We then used the “individual workers” data set to investigate the profile of a sample of volunteers within the sector.
Given existing evidence linking civic engagement and local deprivation and unemployment levels (e.g., Baines & Hardill, 2008), we further linked an additional data set to the NMDS-SC to investigate any such associations. We used the English Indices of Multiple Deprivation 2007 (IMD, 2007), the government’s official measure of multiple deprivations at small area level. The IMD brings together 37 different indicators, covering specific aspects or dimensions of deprivation: income, employment, health and disability, education, skills and training, barriers to housing and services, living environment, and crime. These are weighted and combined to create the overall IMD 2007. The majority of the data underpinning the IMD 2007 are from the year 2005, although some data cover a number of years; for example, an average of 2003–2005. 3 Using unique local area identifiers, we linked these data to the NMDS-SC provision data set. The data were analyzed to examine any relationship between prevalence of volunteering and the level of deprivation in the local area. In addition to the overall IMD, we examined the association between volunteering in the care sector and both the income and employment subscales separately.
Another important factor related to both the opportunities for volunteering and the availability of volunteers is whether an area is predominantly rural or urban (European Commission, 2008). This affects population density and availability of transport. Geography can dictate the demand, availability, and accessibility of volunteering activities (Sherwood & Lewis, 2000; Blackburn, Skerratt, Warren, & Errington, 2003). To investigate the possible association between the geographical characteristics of an area and the prevalence of volunteers in social care services, we used rural–urban classification down to Council with Social Services Responsibility (CSSR) level. 4 These data were linked to the NMDS-SC provision data set and analyzed to explore possible associations between whether an area is rural or urban and the level of volunteering in the local care sector.
Finally, to investigate the personal profile of volunteers we analyzed the NMDS-SC “individual workers” file (December 2010). Employers completing the NMDS-SC provide detailed information on all or some of their workers. Using the detailed records from the “individual workers” data set, we identified 704 workers identified by employers as volunteers. This is a small sample of the total volunteers identified within the aggregate NMDS-SC data file (9.3% of 7,534 volunteers); we used this sample of volunteers to investigate their personal profile and to compare their characteristics to the overall social care workforce characteristics.
Results
Volunteering Activity in Registered Social Care Services
The aggregate information on 7,534 volunteers provides an average volunteer prevalence 5 of just 1% of the total workforce within this large sample of the NMDS-SC. A large group of care providers reported having no volunteers at all (n = 21,527 organizations representing 89% of all providers). Among them were 14,086 employers who provided information about the total numbers of permanent staff only; of these 84% were micro or small care providers, including people employing their own care worker(s). There is no clear evidence to assume a systematic error in the data entry process in relation to the total number of volunteers; however, there is still the possibility of inaccuracy of data reporting. Further detailed inquiry would be needed to see if those completing this data return reported all volunteers to estimate the likelihood that our figures are an underestimate of volunteer activity.
Just over 700 employers/care providers stated volunteers were part of their workforce, with nearly half (43.5%) having only one volunteer; 17.5% having two volunteers; whereas 17% of this group had 10 or more volunteers. Organizations with at least one volunteer were almost equally divided between the voluntary (not for profit) and the private (commercial) sectors (49% and 45%, respectively) with only 5% of local authority (Council owned) care organizations reporting volunteer involvement. Voluntary sector organizations were more likely to have larger numbers of volunteers. On average, the mean number of volunteers within organizations with any volunteers was significantly higher in the voluntary sector, at 15.2 volunteers per organization (median = 5), followed by 8.5 volunteers per organization within the statutory (local authority) sector, and 2.1 volunteers per organization within the private or commercial sector (median = 2 for both sectors). These differences were statistically significant (F = 17.85, p < 0.001).
The vast majority of care services to older people in England are provided by small (10–49 workers) to medium (50–99 workers) size organizations. In our data, 60% of the 700 organizations reporting any volunteers were small organizations. However, the mean number of volunteers was largest within medium size organizations (50–99 workers), at 13.6 volunteers per organization. The data show that the majority of establishments reporting the presence of volunteers were providing residential care (long-term care facilities including nursing homes) (n = 382), followed by adult day care (n = 111). However, settings with the largest mean and median number of volunteers included adult community care and healthcare (mean = 23; SD = 28.2, and median = 17), albeit that the latter group included only 11 organizations. Although adult residential care constitutes a large proportion of organizations with any volunteers, it had the lowest mean number of volunteers per organization, at 3.17 volunteers (median = 1). In contrast, adult community care settings reported having the largest number of volunteers per organization, but among those with any volunteers, this setting had the highest standard deviation of 44.9; indicating a high variation in the number of volunteers within each individual organization.
We investigated the subsample of organizations, which reported having volunteers. The analysis indicated that both the private and the voluntary sectors recognize and report the presence of volunteers in their workforce; however, when volunteers are present they are more likely to be found in larger groups within voluntary sector (not for profit) providers. Similarly, more organizations providing residential services reported having volunteers; yet the mean number of volunteers per care home was quite low, at 3.2 volunteers per organization (median = 1), compared to a considerable 24.4 volunteers in each of the adult community care services with any volunteers (median = 6).
These findings are intercorrelated and reflect the way in which providers differ by sector and setting, with older people’s residential care (assisted living, congregate care, and nursing homes) being concentrated within the private, for profit, sector in England. However, community care services are likely to be run directly by local authorities and not for profit agencies; and their activities may rely more on the contribution of volunteers (e.g., help with transport, group activities, or befriending). Another finding relates to the relationship between volunteering, the voluntary (not for profit) sector, and the size of organization. Overall, the data indicate that volunteers are more likely to be active within micro to small organizations. Even within the voluntary sector, over 75% of organizations with at least one volunteer are micro to small size.
Nearly half of the identified volunteers offered their services in community care settings (day care and social support groups), followed by nearly 20% in both residential and day care settings, and 11% within domiciliary care settings. However, when examining the contribution of volunteers within each of these different settings, it is highest in day care settings, where volunteers constitute 6% of total workers. This is followed by community care, where volunteers form 4.5% of all personnel. Overall, volunteers in both residential care and domiciliary care services constitute only 0.3% of the total workforce.
Local Area Characteristics and Volunteering
We linked the NMDS-SC provision data file to a three-way classification of “Predominantly Rural” (R50 and R80), “Significant Rural” (SR) and “Predominantly Urban” (OU, MU, and LU) obtained for each Council with Social Service Responsibilities (CSSR). For each CSSR, we calculated the prevalence of volunteers out of the whole formal long-term care workforce as identified by the NMDS-SC. We then calculated the median and confidence intervals for this prevalence within the three categories of predominantly rural, significantly rural, and predominantly urban. Findings related to level of rurality presented in Table 1 indicate that the highest median of volunteers’ prevalence (at CSSR level) is in predominantly rural areas followed by predominantly urban areas. However, predominantly rural areas varied widely and included some CSSRs reporting up to 10% of their workforce being volunteers. However, the narrowest distribution of volunteers’ prevalence were in significantly rural areas indicating that the majority of individual CSSRs in this group have a comparatively low level of volunteering (this is not to say that neighborliness or other social support is less in these areas).
Median of Volunteers’ Prevalence at CSSR Level by Level of Rurality, NMDS-SC December 2010.
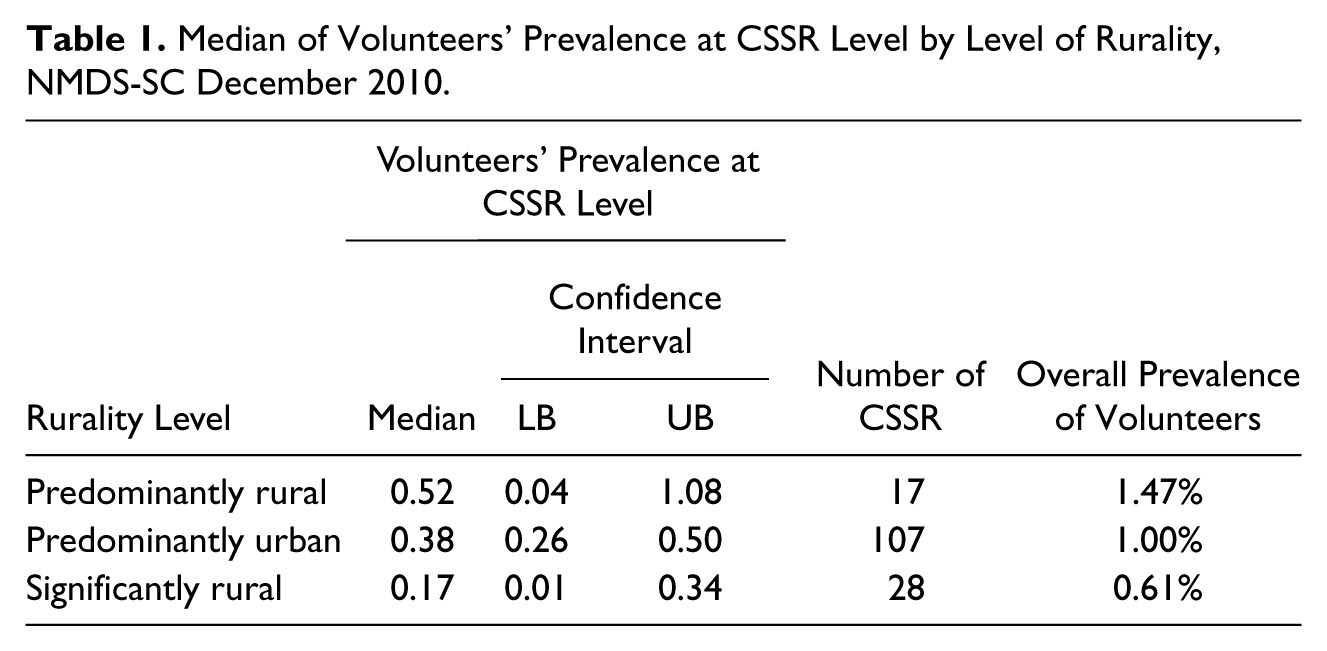
These findings are intriguing, posing the question of whether the relatively higher level of volunteering observed in predominantly rural and predominantly urban areas is associated with different sets of factors, including the make-up of local populations. For rural areas, volunteering may be considered an essential part in delivering health and social care services, and the local population may have different motivations to volunteer in long-term care provision, which are possibly related to the geography and structure of their local areas. It may be the case that volunteering comprises an important source of social interaction in remote areas; and levels of volunteering may be further influenced by the availability of jobs, level of deprivation, and how well-established are the local communities and social networks.
We hypothesized that the characteristics of a local community may affect volunteer activity in registered social care settings through a number of interacting factors. As indicated earlier, we linked the NMDS-SC provision data file to the English Indices of Multiple Deprivation (IMD 2007) on a small spatial scale called the Lower Super Output Areas (LSOAs). The income deprivation domain of the IMD captures the proportions of the population experiencing income deprivation in an area by using proxy indicators based on public welfare benefit receipt (e.g., income support, income-based job seekers’ allowance, etc.). “Employment deprivation domain” measures employment deprivation, defined as involuntary exclusion of the working-age population from the world of work. This scale is calculated in relation to a number of labor force measures, such as receipt of public welfare benefits related to unemployment and others (for full details, see Noble, McLeenan, Wilkinson, Whitworth, & Barnes, 2008). The analysis showed no clear relationship between volunteering and IMD scores, however, even in some areas where deprivation levels are relatively high, the prevalence of volunteers in care providing facilities reached over 5% of the paid workforce reflecting the complex relationships between income, choice, and volunteering.
It is clear from the data that a considerable number of employers in LSOAs (poorer areas) reported having no volunteers and this is related to the huge number of employers which reported no volunteers at all. Focusing on the relationships with both income and employment subscales, Figure 1 shows no clear correlation between prevalence of volunteering and income or employment scales on a local level; and yet points to a high prevalence of volunteering (up to 10% or more of the formal social care sector, when excluding outliers) in areas with better income and employment levels.
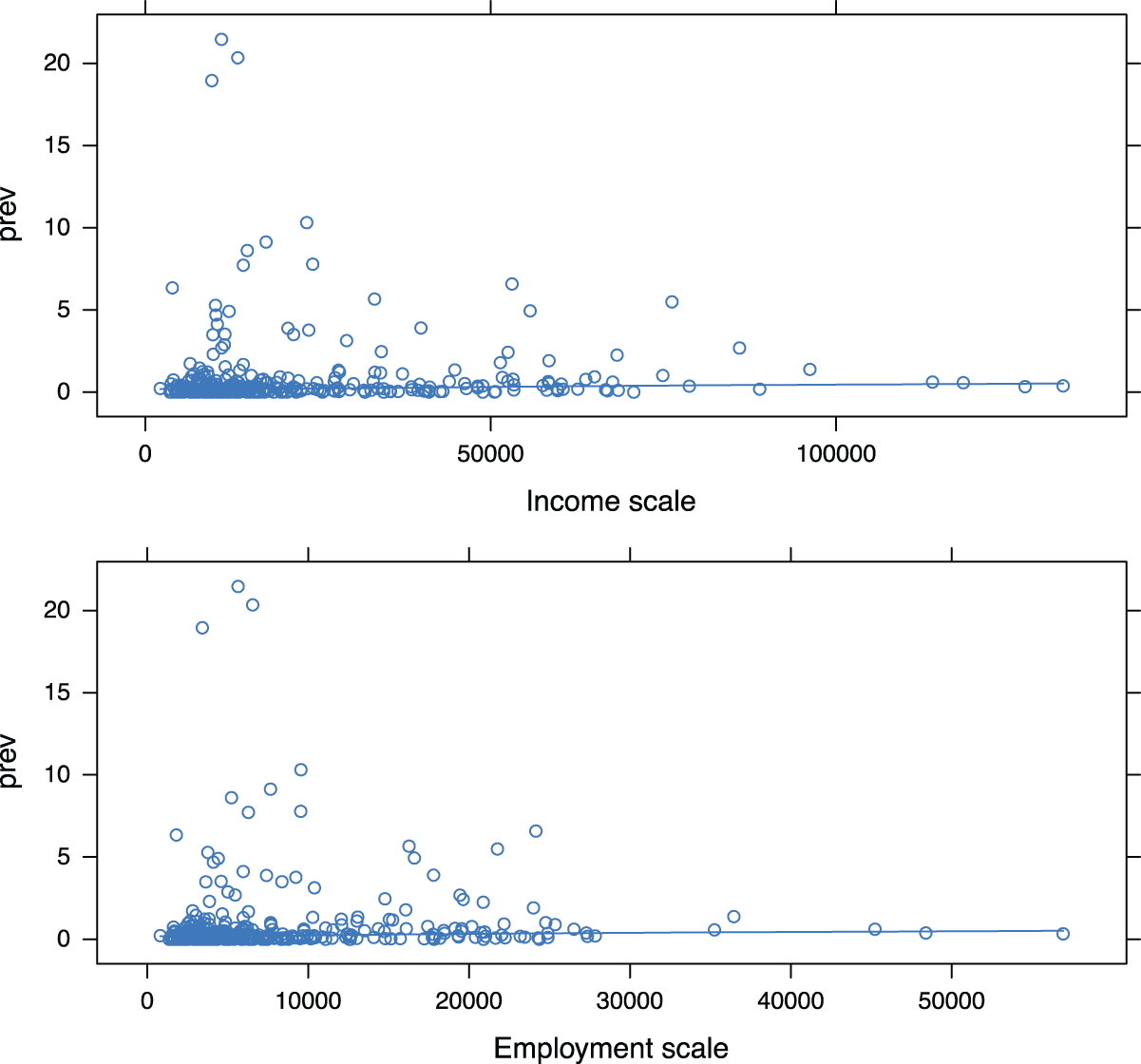
Scatter plot of prevalence of volunteering in LSOAs by income and employment scales. (†, The higher the value of the scale the more deprived the area in terms of income and employment.) NMDS-SC December 2010 and IMD (2007).
Roles of Volunteers in Care Services
The NMDS-SC data allowed us to explore the reported activities undertaken by volunteers in care provision. Table 2 outlines what volunteers do within care services, as well as the relative importance of their contribution to each of these tasks. The distribution of volunteers by main role may reflect the overall structure of the service, for example, 22% of volunteers act as “care workers” whereas 18% perform “other non-care-providing job roles,” such as advisors. A smaller proportion of volunteers, 17%, were reported as taking on the role of “community support” or “outreach,” which may include activities such as driving and accompanying disabled older people in the community.
Number, Distribution, and Prevalence of Volunteers Identified in Organizations Providing Long-Term Care Services by Main Role, NMDS-SC December 2010.
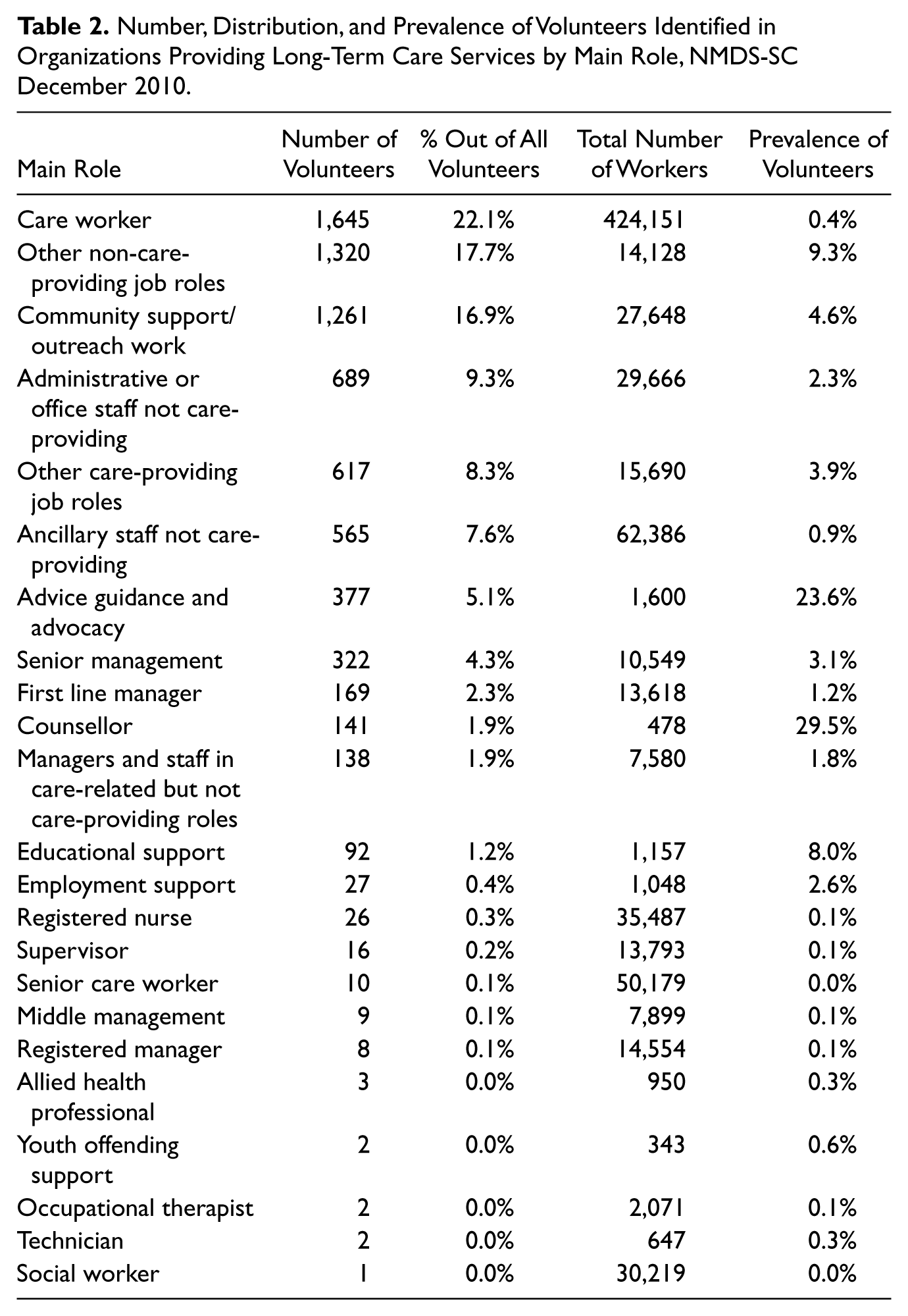
If we consider the relative contribution of volunteers to different job roles, volunteers undertake tasks such as “advice, guidance, and advocacy” and “counseling,” constituting considerable proportions of these labor forces (24% and 30%, respectively). Similarly, but to a lesser extent, volunteers comprise 8% of the workforce whose main role consists of “providing education support.” Such tasks do not include personal care (i.e., help with toileting, eating, washing, and dressing), which are key activities undertaken by the main workforce in care settings.
Profile of Volunteers in the Care Sector
Among the 704 volunteers about whom we had details of their personal characteristics, 87% identified themselves to be of White ethnicity. This is higher than the average of 82% for the whole adult social care workforce in England (Hussein, 2009), but similar to the general population. There were equal proportions of 5% of Black or Black British and Asian or Asian British workers among the volunteers. A larger proportion of volunteers was identified as having any form of disability compared to employed workers (13.2% vs. 2%). Some of the distinct characteristics of volunteers when compared with the overall long-term care workforce were related to both gender and age. In terms of gender, there were proportionally more male volunteers than paid employees. Over a third of the volunteer sample identified through the NMDS-SC was male (33.6%, n = 232), whereas women form the vast majority of the paid care workforce in England (Hussein, 2009).
The median age of volunteers was also significantly higher than the paid workforce at 48 years (mean age = 47 years), compared to 43 years (mean age = 42 years) among nonvolunteers. However, to a lesser extent, volunteers included proportionally younger people than nonvolunteers. For example, 7% of volunteers were aged 19 years old or younger, compared to 2% of the paid workforce; possibly reflecting some “required” volunteering activities as part of building a personal career oriented profile among younger people (see Figure 2). There was a smooth distribution of ages among volunteers with a slight peak among younger ages (<20 years) and a more evident peak at older ages (65+ years). Among the paid workforce, however, there was significant concentration around the middle age-groups (45–55). On average, male volunteers were 1 year younger than female volunteers (median age of men = 47.5 and median age of women = 48.5). Previous studies have indicated that specific volunteers’ roles are likely to be associated with their age (Black and Kovacs, 1999).
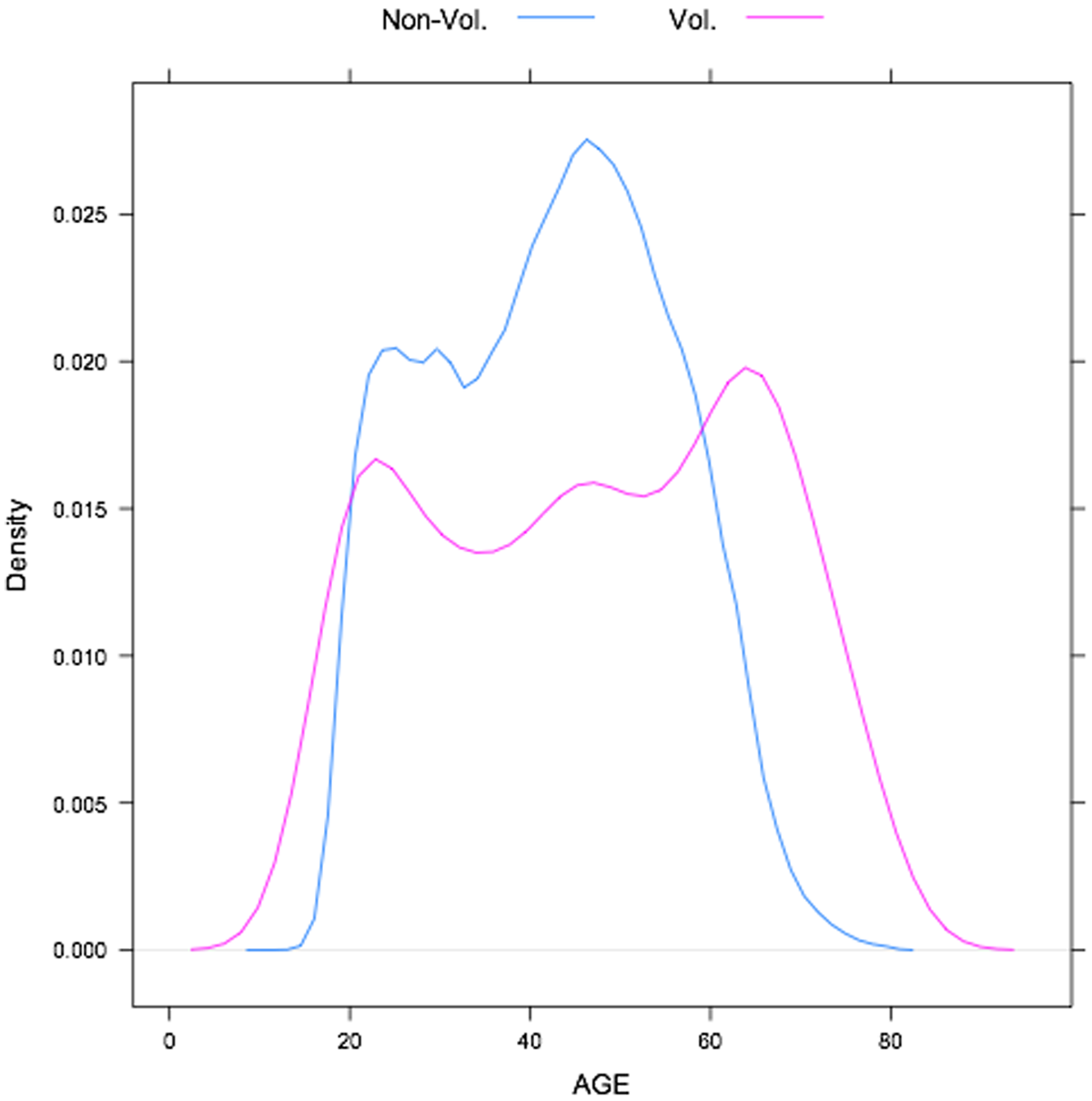
Density function plot of the distribution of volunteers’ and nonvolunteers’ age, NMDS-SC December 2010.
Overall, 18% of volunteers were reported as holding no qualifications and 56% of those possessed qualifications were not relevant to the care sector. Nearly three-quarters of volunteers (72%) had completed (or were in the process of completing) an induction or orientation course related to the setting where they were volunteering.
Discussion
This analyses and associated findings provide insight into the contribution of volunteers in the formal or registered social care sector in England. Bearing in mind that volunteering in formal settings or organizations could be construed as one of the highest levels of civic engagement, the data point to the considerable contribution of volunteers to the sector. Overall, the current data set indicates that volunteers constitute just 1% of the overall care workforce, however, it is likely that the actual contribution is much larger than this. Within organizations using volunteers, the contribution of volunteers was high: in many they constituted over a quarter of the workforce. Volunteers seem to be more common in small- to medium-sized organizations but scarce in large organizations, even in the voluntary sector itself. The NMDS-SC does not provide any data on volunteers’ motivations. There would appear to be scope to investigate sources and processes of recruitment further by collecting specific information through surveys and qualitative methods.
There are pressing reasons for better information. The care sector itself may wish to attract and sustain volunteers. The private long-term care sector, for example, experiences considerable staff turnover (Hussein, 2010; Hussein & Manthorpe, 2011), and volunteers may provide continuity of relationships, particularly for those older people with no living or accessible family members.
A tentative finding is that areas with the highest levels of volunteering were the wealthiest in terms of income and employment scales. This may reflect an “inverse care law” where volunteering is facilitated in better-off areas. The need for volunteers in long-term care within rural communities is advocated (e.g., Wilson et al., 2005; Skinner, 2008). Some reasons for this relate to geography and spatial features, as well as socio-demographic factors, such as the outward movement of rural young people and associated reductions in social networks. Our analysis shows that the prevalence of volunteers is, on average, higher among predominantly rural and predominantly urban areas but not “significantly” rural areas, which may relate to the dispersed nature of residencies and possible transportation barriers within such communities.
A “volunteer” was traditionally visualized as a middle-aged woman, of middle to upper income, and possibly without a career (Davies Smith, 1993). This analysis contributes to the growing evidence that disputes this. Volunteers include all age groups, including the very old, and are from all socio-demographic and economic groups (Wardell, Lishman, & Whalley, 2000; Skinner, 2008; Hank & Erlinghagen, 2009). There are some assumptions that volunteers tend to be of the same age as their clients, so that peer relationships may develop (Snyder & Omoto, 2000). We found that volunteers were on average significantly older than the paid workforce, yet they contained relatively larger proportions of younger people (19 years or younger). Men were also overrepresented among volunteers compared to the paid workforce in the care sector and tended to be younger than women. This points to the potential for recruiting from outside traditional pools of volunteers. It appears to be already possible to attract volunteers from more diverse groups, in terms of gender, age, and social background, than are currently recruited to the paid workforce.
When volunteering takes place in organizational settings where professionals are present, the volunteer often augments professional activity, especially by providing companionship and information (see Neno & Neno 2007, for example). Research, especially from the United States, suggests that the role of volunteers within services for the older population is concentrated around providing information and transport, and other day-to-day assistance such as shopping (Baines & Hardill, 2008). In this way, volunteers often “fill gaps” within the system (Butler & Eckart, 2007) and they may also free professional time. The tasks that volunteers perform provide insight about where and with whom volunteers spend their time and may be linked to their motivations to volunteer their time and energy. One important finding here is the significant and distinct role volunteers play within formal care services. Their roles mainly related to providing support, advice, and advocacy. Consistent with the assumption of “filling gaps” at a time of austerity, these specific roles of paid advocacy and support are likely to be reduced. These opportunities might be communicated and social care providers may consider targeting volunteer recruitment more precisely if they have specific activities or vacancies in mind. With the recent abolition in the UK of the Place Survey (UK Statistics Authority, 2011a) and plans to cancel the regular Citizenship Survey (UK Statistics Authority, 2011b), the NMDS-SC is likely to become a more important resource about volunteering for public policy researchers and gerontologists.
It is likely that some of the information provided by employers may not accurately reflect the full contribution of volunteers. There is the chance that some employers may not report volunteers as part of their workforce, either because of a misinterpretation of questions in relation to what constitutes “workforce,” or of the nature of volunteers’ contribution to the care provider, and the regularity and pattern of that contribution. There is no easy way to further investigate these suggestions using existing datasets, but the observations in relation to the large number of organizations with no volunteers may need to be confirmed. It might be possible to undertake direct questioning of a sample of these employers to see if they were failing to report volunteer input for any reason.
Conclusion
Our study has provided new evidence of the diversity of volunteers compared to the paid care workforce in England, and has identified the importance of volunteers in small social care settings where they may have much to offer older people. Care providers who report having no volunteers may wish to learn more of how to recruit and sustain volunteers from others in the sector. General policy encouragement of volunteering should be informed by existing practice and not portray volunteering as simply a supplement to paid jobs. National data sets have the disadvantages of providing general data but they also provide valuable information. In the case of this study, the data provided a unique opportunity to compare volunteers with paid staff in care settings; and to consider if older and disabled people living in rural and poorer areas were disadvantaged in terms of access to the support of volunteers. We suggest that it is more likely that poorer areas lack volunteers and the implications of this further inequality may need to be considered by national volunteer initiatives and investment.
Footnotes
Acknowledgements
The authors are grateful to Skills for Care for providing us with the NMDS-SC data and also to those social care providers for completing the surveys. The authors are thankful to Analytical Research Ltd. for their quantitative support in linking and modeling the data sets.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was commissioned by the Department of Health under its Policy Research Programme support for the Social Care Workforce Research Unit. The views in this article are the authors and should not be necessarily interpreted as shared by the Department of Health or Skills for Care.