
Abstract
As part of its Medicaid program restructuring, New York State funded 11 Workforce Investment Organizations (WIO) to support training initiatives for the long-term care workforce. Focusing on one WIO, this formative evaluation examined quality improvement training programs delivered to 11,163 Home Health Aides employed by home care agencies serving clients of Managed Long-Term Care plans. Results are presented from a thematic analysis of qualitative interviews with organizational and program stakeholders examining contextual factors influencing program objectives, implementation, barriers and facilitators, and perceived outcomes. Findings suggested that WIO training programs were implemented during a period of shifting organizational strategies alongside value-based payment reforms and challenges to aide recruitment and retention. Stakeholders appraised WIO training programs positively and valued program flexibility and facilitation of communication and collaboration between agencies and plans. However, delivery and implementation challenges existed, and industry-wide structural fragmentation led stakeholders to question the WIO’s larger impact.
Introduction
Since 2016, the New York State Medicaid program has undergone a major transformation in its payment structure away from a high-cost “fee-for-service” model toward a more financially sustainable “value-based payment” model that rewards comprehensive, high-quality, and integrated care management (New York State Department of Health, 2016). The transition toward a value-based payment model was supported through a 1115 Medicaid waiver. An agreement between New York State and the Centers for Medicare and Medicaid Services under Section 1115 of the Social Security Act allowed the State to direct monies toward investments in comprehensive Medicaid delivery and payment reform (About Section 1115 Demonstrations, 2021; New York State Department of Health Office of Health Insurance Programs, 2019). A focus of these investments was workforce training, viewed by the State as instrumental in helping healthcare organizations navigate the value-based payment environment and building local employment capacity by enhancing skills and supporting career advancements for healthcare workers. $245 million was made available through the 1115 Medicaid waiver for New York State’s Workforce Investment Program, which allocated funds for training initiatives between April 2018 and March 2020 to enhance the recruitment, retraining, and retention of healthcare workers in the long-term care sector (Espinoza, 2019; New York State Department of Health, 2018). The primary goal of this investment was to prepare a competent workforce to serve the growing number of clients receiving Medicaid long-term care in home, community, and facility settings.
Direct care workers including home health aides, personal care aides, and nursing assistants were specifically targeted through the Workforce Investment Program for their central role within the long-term care system (Cook, 2019). An estimated 1.3 million jobs are expected to be added to this workforce nationally by 2028 (Campbell et al., 2021). The New York State Department of Health designated 11 Workforce Investment Organizations (WIO) to serve as training centers tasked with identifying the long-term care workforce training and career development needs within their local areas, investing in programs that address those needs, soliciting broad participation, engaging stakeholders, and supporting the expansion of home-based long-term care (Espinoza, 2019; New York State Department of Health, 2018). While these investments represented a massive undertaking, little is known about their implementation or impact. We conducted qualitative interviews with stakeholders of one WIO to examine contextual factors surrounding implementation, barriers and facilitators, and perceived outcomes of training and skill-building programs for Home Health Aides employed by Licensed Home Care Services Agencies serving clients of Medicaid Managed Long-Term Care plans.
Background and Significance
New York State Long-Term Care Policy and Role of Workforce Training Initiatives
New York State operates a Managed Long-Term Care (MLTC) system in which privately operated health plans manage and coordinate health and care services to individuals with chronic health problems or disability to support these individuals to stay in their homes and communities and reduce excessive medical expenditures associated with avoidable inpatient care (New York State Department of Health, 2016). Managed Long-Term Care health plans contract with a network of provider organizations to deliver services, including Licensed Home Care Services Agencies (agencies) that provide home health services (New York State Department of Health, 2021). Agencies employ Home Health Aides, Personal Care Attendants, and Home Attendants (for the purposes of this article we refer to them as “aides”), to provide the majority of hands-on care, including assistance with self-care and activities of daily living (Institute of Medicine (US) Committee on the Future Health Care Workforce for Older Americans, 2008; New York State Department of Health, 2018). Under New York State’s value-based payment model, MLTC health plans are required to enter into financial risk-sharing arrangements with agencies serving sizable amounts of their plan members to jointly receive bonus payments or monetary penalties based on plan members’ performance on State-defined value-based payment measures (Cook, 2019). Examples of value-based payment measures for long-term care include falls resulting in injury, influenza vaccination, emergency room visits, and avoidable hospitalizations (New York State Department of Health, 2020). Workforce Investment Organizations training centers were established to support agencies in educating their direct care workforce on the new payment structure, metrics, and other topics around care quality improvement (Cook, 2019). The risk-sharing agreements and WIO funding motivated collaboration between MLTC plans and their contracted agencies to define shared quality goals, identify workforce training needs, and create targeted training programs.
The Home Health Aide Workforce and Workforce Development Initiatives
There is a critical need to improve the quality, supply, and retention of aides amid increasing demand (Bureau of Labor Statistics, 2021; Marquand & Chapman, 2014; Nisbet & Morgan, 2019; Spetz et al., 2019). Experts have called for competency-based education requirements and support for training programs that recognize the value and contribution that aides bring to team-based home care (Stone & Bryant, 2019).
Despite the need for better training, limited evidence exists to inform the development and adoption of training programs within value-based payment models. Previous research evaluating training programs for aides and other direct care workers suggests that workforce development initiatives can help improve job performance, engagement, and retention (Danilovich et al., 2020; Feldman et al., 2019; Guerrero et al., 2020). Training for in-home supportive services dementia caregivers was found to increase their self-reported ability to provide care (Guerrero et al., 2020). Aides participating in a health interviewing program expressed that the training gave additional meaning to their work and facilitated conversations with clients (Danilovich et al., 2020). An initiative to improve skills, job satisfaction, and retention among aides found that an expanded training curriculum designed around adult-learners and peer-mentoring increased retention (Feldman et al., 2019). Workforce development initiatives implemented among direct care workers in nursing homes suggest mixed results. Training programs for certified nursing assistants that went beyond licensing and credentialing requirements were associated with greater job satisfaction (Han et al., 2014). Another large randomized study of a quality improvement program orienting nursing home staff to tools and strategies for identifying, assessing, communicating, and documenting resident status changes found no effects on hospitalization and emergent care utilization (Kane et al., 2017). The results of this study may be attributable to barriers surrounding program implementation, including the complexity of culture change, leadership instability, competing demands, scarce resources, and technical problems (Tappen et al., 2017). These findings highlight the importance of understanding how large-scale initiatives like the WIO are implemented in practice, particularly when those initiatives are intended to support systemwide transformation through value-based payment models.
Present Study and Guiding Research Questions
The success of complex interventions like WIO depend largely on their structural or system-level contexts (DeCorby-Watson et al., 2018; LaFond et al., 2002; McCreight et al., 2019; Smith et al., 2006). This study is part of a larger evaluation effort that attempts to understand the process, policy context, development, implementation, outcomes, and lessons learned from WIO. Qualitative interviews were conducted with healthcare organizations and program stakeholders to address the following research questions: (RQ1) What was the social and political context surrounding WIO implementation, and what problems were WIO training programs designed to address? (RQ2) How do stakeholders describe their experiences with WIO implementation, including their concerns, barriers, and facilitators? (RQ3) What were the outcomes, intended or otherwise, of WIO programs for collaboration and quality improvement efforts among MLTC plans and agencies?
Design and Method
Setting and Program Description
This study focused on the development and implementation of care quality training and skill-building programs for aides whose employer agencies participated in one WIO collaboratively formed by the 1199 Service Employees International Union Training & Employment Funds, Continuing Care Leadership Coalition, and Visiting Nurse Service of New York (Ladders to Value Workforce Investment Organization, 2020). Under risk-sharing agreements, the training programs we studied were prioritized by respective agencies implementing the training among their workforce. The programs oriented aides to improve client performance on value-based payment measures with strategies for recognizing and reporting changes in their client’s health status, and working within an interdisciplinary care team (Appendix A). These training programs were distinct from those offered by other WIOs as the implementation involved substantial intra- and inter-organizational coordination. The selected programs were delivered through classroom lectures, with incorporated field internships in one program involving advanced training (i.e., Health Coaching). Agencies instituted mandatory completion requirements for aides serving clients of MLTC health plans affiliated with the WIO. Figure 1 displays a Logic Model detailing program processes and intended outcomes (Centers for Disease Control and Prevention, 2018). Briefly, this model proposes that investments into long-term care workforce development programs facilitated the delivery of training programs for aides. Training programs are intended to (1) enhance knowledge, skills, and team-based engagement among aides (short-term outcome); (2) strengthen communication and collaboration among MLTC plans and contracted agencies (intermediate outcome); and (3) improve retention, recruitment, and recognition of aides (long-term outcome). Contextual factors surrounding the programs include the transformation to value-based payment, challenges and barriers to the recruitment and retention of aides, and calls for increased support for training programs that recognize the value and contribution of aides. Between April 2018 and February 2020, a total of 11,163 aides across the four participating agencies completed one or more of these training programs. The WIO reimbursed agencies for the time that aides devoted to training programs in lieu of client services. Training recipients were mostly female (96.7%) with a mean age of 52 years (standard deviation = 11.9 years). These characteristics are comparable to U.S. home care workers (PHI., 2019). Logic model of home health aide training/career-building programs implemented by a workforce investment organization.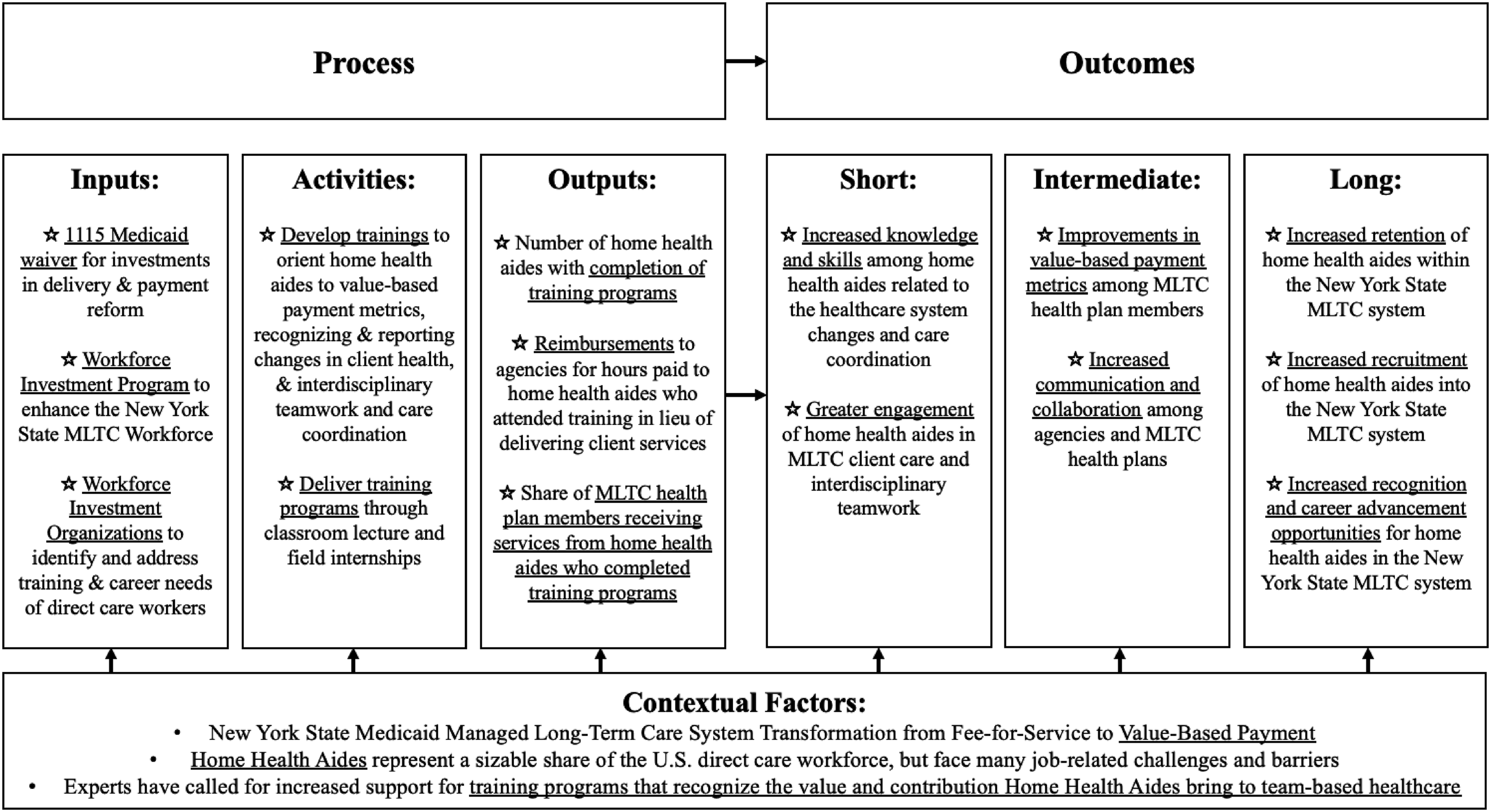
Data Collection
Stakeholder Group Participation and Format of Qualitative Interviews.
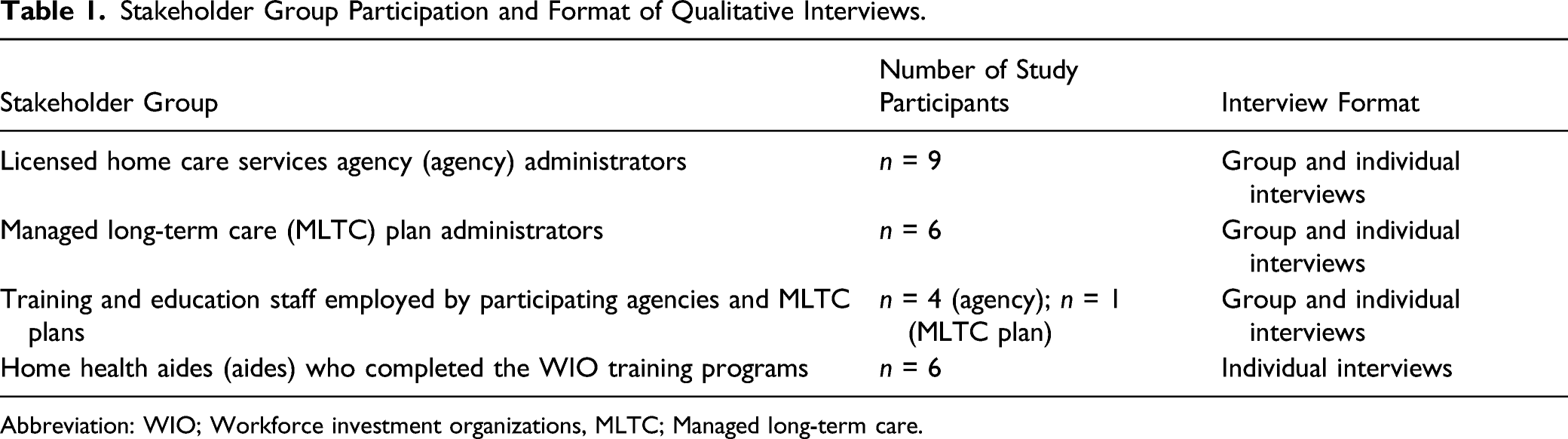
Abbreviation: WIO; Workforce investment organizations, MLTC; Managed long-term care.
Data Analysis
Thematic analysis was used to draw insights from and summarize key features of the qualitative data by examining the perspectives of different WIO program stakeholders and highlighting their similarities and differences (Nowell et al., 2017). Transcripts of the interviews were imported into NVivo software to aid with creating a codebook and data analysis. The lead author (DR) familiarized themself with the data by reading transcripts line-by-line and documenting initial thoughts about codes and themes. Next, the lead author developed a coding framework by reviewing five transcripts for a priori topic areas (e.g., implementation challenges, aide skills, interdisciplinary teamwork), and emerging concepts (e.g., value of aide services, collaboration between MLTC plans and agencies). This framework was revised and refined through discussions with the second author (MF), incorporating feedback on content and parsimony. The lead author then applied this final framework by coding all transcripts. Three authors (DR, MF, EF) independently reviewed coded excerpts related to each of the research questions. Then, over the course of several meetings, these authors met to discuss themes by identifying patterns, connections, and distinctions in the data. Stakeholder groups were analyzed separately and then compared and contrasted to highlight emergent themes and divergent perspectives. Findings and analytic decisions were discussed in regular team meetings. Detailed notes and memos documented personal assumptions to limit biases and strengthen objective interpretation. We returned to this audit trail throughout the analytic phase to confirm our interpretations and ensure that no relevant data was inadvertently or systematically excluded (Lincoln & Guba, 1986).
Results
Themes from Stakeholder Interviews and Illustrative Quotes.

Implementation Context: Value-Based Payment Re-Oriented Organizational Workforce and Service Delivery Priorities for Plans and Agencies
Managed Long-Term Care plan and agency stakeholders described the New York State long-term care system as a diffused industry with complex plan-agency affiliations, a transient home care workforce, and a lack of centralized management over organizations comprising the State’s long-term care system. The transition to value-based payment motivated MLTC plans and agencies to focus on “quality,” manifested concretely through standardized metrics intended at operationalizing abstract notions of “value” and “member choice.” Financial risk-sharing introduced through the value-based payment model placed pressures on plans and agencies to get the “monetary reward” and motivate their staff to be more “proactive” in working toward improving metric performance, including through training and education programs as well as collaborative quality improvement initiatives. As a response to the State’s value-based payment requirements, MLTC plan administrators described their efforts to “fine tune” their agency networks to enable development of risk-sharing contracts and closer collaboration with agencies serving larger shares of their members. Workforce Investment Organizations funding enabled agencies to develop and implement training programs for aides that focused on selected quality metrics incentivized by the payment system. Consequently, some training program curricula were directly aligned with risk-sharing value-based payment contracts between MLTC plans and agencies.
Implementation Context: Home Health Aide Recruitment and Retention is Undermined by their Undervalued, Precarious Role in Long-Term Care
The undervalued and precarious role of aides within the growing long-term care industry was seen by agency administrators as a central barrier to workforce recruitment and retention. While aides themselves expressed motivations for pursuing a job in home care, including flexible scheduling and a desire to serve in a caring profession, both agency administrators and aides pointed to issues of aides working across multiple employer agencies, receiving minimal compensation and recognition for physically and emotionally challenging labor, and lacking a team-based connection to other healthcare workers. Agency administrators also noted competition with other low-wage positions, minimal licensing and training requirements, a lack of credentialing programs to distinguish between aides with greater or lesser training and experience, and limited career advancement opportunities.
Implementation Experiences: WIO Flexibility and Resource Sharing were Valued by Stakeholders but Generated Uneasiness
Workforce Investment Organizations policies granted agencies considerable flexibility in the design and implementation of training programs. This flexibility was valued by both agency and MLTC administrators because it encouraged sharing of training materials between agencies and allowed training programs to focus on shared quality goals defined by performance on value-based payment measures. Workforce Investment Organizations’s flexibility also enabled smaller agencies with limited staffing resources to subcontract with larger agencies to deliver training programs to their aides. While MLTC administrators favored flexibility, agency administrators expressed hesitation about collaborating with competing agencies, fearing they may lose aides and patients to competing agencies with preferred training/service offerings.
Implementation Experiences: Training Program Instruction was Viewed Favorably, Yet Delivery and Implementation Challenges Existed
Agency administrators and aides rated the quality of instruction favorably. Managed Long-Term Care plan administrators felt they were not close enough to training programs to judge them. Instructors described taking a practical, hands-on approach in which they used multiple, interactive modalities to foster learning and engagement, while reducing repetition. Aides valued the time devoted to training programs, the clarity of instruction, and the applicability of course concepts to client care (e.g., understanding how health promotion efforts can be viewed through the transtheoretical model “stages” of health behavior change). Instructor experience, training, and versatility were viewed by agency administrators and instructional staff as beneficial to the program’s quality. Instructors also noted the complexity of their roles in working with such a diverse workforce, reporting that they served as counselors for aides navigating their healthcare careers and needed to balance their pedagogy between aides with different literacy levels. While the content and delivery of the programs were viewed positively by aides and instructional staff, agency administrators described challenges with scheduling aides for training programs, balancing training requests with client care schedules, overtime rules, family responsibilities, and aides’ work hours across multiple agencies.
Program Outcomes: WIO Further Facilitated Inter-Organizational Communication and Provided a Structure for Collaboration
Managed Long-Term Care plan and agency administrators both viewed WIO as facilitating cross-organization communication and providing a “structure” for collaborations already underway with the shift to value-based payment. Managed Long-Term Care plans and agencies introduced new workflows, interventions, initiatives, and technologies alongside WIO training programs to monitor high-risk clients and improve communication within and across organizations. One example included clinical rounds to discuss client health and healthcare utilization, including recent falls and hospitalizations. Steps were taken to integrate aides into interdisciplinary healthcare teams by encouraging them to notify MLTC plans of medical problems observed in the home that might otherwise go unreported, such as medication reactions, wound deterioration, infections or falls. Aides described how training programs improved their observation and communication skills, by encouraging them to voice their concerns and interact with clinical staff, leading them to feel more empowered and engaged. However, agency and MLTC administrators noted several barriers to communication and collaboration, including multiple aides working for the same client, gaps in data and information sharing between plans and agencies that allow aides to share clinical events and alerts with care management teams, and the exclusive focus of WIO training on aides as opposed to other interdisciplinary team members.
Program Outcomes: Stakeholders viewed WIO Training Programs as Beneficial but Questioned Measurable Impacts
Agency and MLTC administrators praised WIO training programs for enabling a large number of aides to learn new concepts and skills, and promoting confidence, empowerment, and engagement within a value-based payment environment. However, in the absence of a formal outcome evaluation of WIO, MLTC administrators expressed uncertainty about the measurable accomplishments of WIO beyond simple training numbers, and difficulty in discerning which aspects of training programs worked and how. According to MLTC administrators, difficulties in discerning program accomplishments may be attributed to a lack of standardized data collection efforts, as well as performance incentives emphasizing client health outcomes rather than aides’ application of preventative strategies taught in training programs. Managed Long-Term Care administrators questioned whether the WIO could meet the dual goals of achieving value and facilitating retention of aides. Agencies hypothesized that training programs improved care quality and facilitated more trusting client-aide relationships, which could facilitate aide retention and improve client performance on value-based payment measures. However, agencies lacked data to support their hypothesis. Finally, WIO investments were time-limited and stakeholders questioned how, and in what form, to continue the programs. Aides and agency administrators also expressed frustration that skills acquired through training programs were not directly tied to career advancement opportunities.
Discussion
The New York State Workforce Investment Program represented a novel approach to strengthen the direct care workforce amid a transformation to value-based payment and growing demands for MLTC services. The present study explored stakeholder perspectives toward a WIO designated by New York State to implement training and skill-building programs for aides. These programs focused on orienting aides to state-defined value-based payment measures, signs of changing health status among their clientele, and preventive care strategies. Themes revealed several important findings. First, stakeholders described how WIO programs were implemented during a period of considerable focus among MLTC plans and agencies on meeting quality performance goals, as well as a time in which agencies faced substantial obstacles to recruit and retain aides. Agencies operate on tight margins and face significant competition for workers from other economic sectors (Scales, 2021). Agencies reported problems with losing their workforce to other employers over wages and stable schedules. Agencies expressed hopes that the implementation of value-based payment in New York State would bring greater attention and job quality investments to their aide workforce, including resources that lead to greater role recognition and respect, as well as the creation of career advancement opportunities that leverage interpersonal and problem-solving skills to drive improvements in targeted quality measures (Cook, 2019; Scales, 2021). Evidence that such investment leads to strengthening of the home care workforce is found in Taiwan’s experience, where implementation of a volume-based payment system was attributed to greater worker autonomy, a larger number of home care recipients, and higher incomes for home care workers (Wu et al., 2021). Workforce Investment Organizations training programs were intertwined with, and specifically developed to support, the State’s transition to a value-based payment model. Further research is needed to disentangle the unique impacts of large-scale workforce training programs like WIO from payment system transformations.
Additional research is also needed to better understand the impacts of payment system transformations and workforce investments on aide recruitment and retention. Training programs for aides, including the Health Coaching program that was implemented as part of this WIO’s quality improvement initiatives, can spark interest among aides in career advancement within healthcare and motivate them to develop new skills (Russell et al., 2017). This is critical because aides who perceive their agencies and supervisors as respectful and supportive of their careers tend to report greater job satisfaction, especially when perceived appreciation is paired with higher wages (Yoon et al., 2016; Yoon & Khan, 2020). While New York State authorized the Advanced Home Health Aide role in 2016 to allow aides with additional training to carry out tasks like medication administration (Advanced Home Health Aides: Chapter 471 of the Laws of 2016, 2021), the WIO programs we examined were not directly connected to specialized programs utilizing newly developed skills, expanded practice, or promotion to advanced positions. Our findings support long-standing advocacy efforts to improve recruitment and retention of the home care workforce through career advancement opportunities that connect experienced aides with specialty training, advanced roles, higher wages and greater benefits (PHI, 2018; Scales, 2018).
Second, while WIO training programs may facilitate cross-organization collaboration at the administrative and executive levels of MLTC plans and agencies, these partnerships may not lead to greater communication and teamwork among frontline care staff. Technologies such as apps to report findings could support aides in documenting and communicating their observations with other care staff (Sterling et al., 2020). However, these technologies should be paired with educational efforts and structural changes to promote greater recognition of aides within home-based long-term care. Research demonstrating links between aide care and client outcomes, such as the impact of continuity in the provider of aide services, could also serve to recognize the value of aides.
Our study has notable limitations, including a small sample size of stakeholders. However, our goal was obtaining insight into stakeholder experiences within a specific WIO, rather than generalizing to broader contexts (Hennink et al., 2017). Additionally, while stakeholders offered positive appraisals of WIO programs, we did not formally evaluate knowledge and skill development among aides, nor MLTC client outcomes. Assessments of capacity-building initiatives like the WIO should incorporate more sensitive measures into evaluation design, such as measures of relational care and institutional support of direct care workers (Franzosa et al., 2018). Existing value-based payment models fail to capture the range of supports that aides provide to clients, including socio-emotional support, monitoring health conditions, reporting health changes to care providers, and household management to reduce clutter and other safety hazards (Franzosa et al., 2018; Reckrey et al., 2019).
Our study found that WIO facilitated collaboration between MLTC plans and agencies. However, these collaborations generated uneasiness among agency stakeholders due to concerns about competition for aides and clients. Policy makers might consider incentives that encourage partnerships between agencies to collaborate on training schedules, access to online learning tools, and payment for aide release time during training (Wilson et al., 2002). Future large-scale workforce initiatives like the WIO could experiment by piloting cross-agency training series that encourage resource sharing, which may indirectly support aide retention and career advancement (Harris-Kojetin et al., 2004). Aides positively evaluated WIO programs, including program length and applicability to client care. However, future workforce investments should consult aides about their training needs and solicit their input into training design. Training programs with aide input have been linked with greater involvement of aides in client care, as well as reductions in client hospitalizations and emergency room visits (Gallup et al., 2018). Future training programs could include peer mentoring to foster relationships between experienced and junior aides to encourage knowledge transfer, mutual support, and continuous learning across experience levels (Kreiser et al., 2010). Peer mentoring may also assist experienced aides with becoming peer coaches or training instructors.
Conclusion
Home Health Aides are the “eyes and ears” of the long-term care system serving the health, medical, and daily functional needs of people with chronic illness or disability (Reckrey et al., 2019). Recruiting and retaining aides is an urgent concern given rising long-term care service demand and high workforce turnover (McCall, 2019). Workforce Investment Organizations represented a novel approach to strengthening the direct care workforce amidst value-based payment reforms. Value-based payment reforms re-oriented MLTC plans and agencies to develop shared quality goals and implement WIO training programs that involve aides in supporting those goals. Although implementation challenges existed, stakeholders favorably appraised the WIO for allowing flexibility in training design, equipping a larger number of aides with new skills, laying a foundation for career advancements, and supporting organizational collaborations. Structural barriers including industry-wide fragmentation, prolonged aide role devaluation, and lack of a data-sharing infrastructure to effectively leverage trained aides generated uncertainty about the larger impacts of WIO. Additional efforts are needed to transform public attitudes toward aides, encourage interdisciplinary teamwork, and develop best practices for advanced training programs that lead to career advancement opportunities and higher wages.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the New York State Department of Health in support of the Managed Long-Term Care Workforce Investment Program.
Ethical Approval
All study protocols described in this article were approved by the Institutional Review Board of the Visiting Nurse Service of New York (Reference Number: I19-022)
Training Programs for Home Health Aides Implemented through the Workforce Investment Organization
The proportion of aides employed by the agency who completed the WIO training program and actively serving clients of risk-sharing MLTC plan Notes: With the exception of the Health Coaching Program (considered as “advanced training” available for a smaller number of eligible aides), all the other programs were mandatory in-service home health aide training within respective Agencies. Differences in implementation progress reflected differences in value-based payment contract dates between risk-sharing managed long-term care plan and the Agency, as well as the Agency’s capacity, resources, and readiness to execute training program(s) related to the contract, and the Agency’s operational ability to balance scheduling of aide training and client service delivery.
Program and implementation characteristics (program start date)
Program goals
Program description and key activities
Expected outcomes
Value-Based Payment Measures in Managed Long-Term Care, Reporting, and the Healthcare Team: Part I (June 2018) Agency 1 (n = 5397 aides completed program; 98% of workforce)a
Participants will learn about value-based payment measures, including measure definitions and importance, and methods for recognizing changes in client health and strategies for reporting them to the healthcare team
Four-hour classroom lectures and discussion on value-based payment measures for managed long-term care clients; supplemental post-training clinical experience with the interdisciplinary team, where trained aides report client health changes through real-time device usage
Improved client performance on value-based payment measures, as trained aides learn to observe and report on signs and changes in client health
Value-based payment measures in managed long-term care, reporting, and the healthcare team: Part II (April 2018)
Agency 1 (n = 5505 aides; 100% of workforce)Participants will learn about care management strategies and interdisciplinary teamwork with a focus on six types of potentially avoidable hospitalizations
Improved client performance on value-based payment measures, including potentially avoidable hospitalizations, as there is real-time communication to ensure timely intervention within the interdisciplinary team enabled by the technical device
Enhanced home health aide (July 2018)
Agency 2 (n = 3293 aides; 47% of workforce)Participants will learn about identifying signs indicating changes in client health and care strategies to support client health needs corresponding to client performance on value-based payment measures
Two-day in-class lectures, including an overview of value-based payment measures and care strategies to improve client performance on the measures
Improved client performance on value-based payment measures, as trained aides become aware of and act on signs of potential changes in the value-based payment measures
Health coaching (September 2018)
Agency 2 (n = 261 aides; 2% of workforce)Participants will gain a foundation in health coaching practice to assist client with self-care and obtain a potential career ladder in healthcare
Two-day in-class lectures introducing fundamentals of health coaching; One-week supervised field internship
Improved client performance on value-based payment measures, as trained aides coach patients to address their self-care needs, and identify and work toward their health goals
Home health aide skills development and healthcare teamwork (December 2018) Agency 3 (n = 516 aides; 37% of workforce)
Support long-term care workers professional development and improve the quality of care delivery through enhancing the skills and knowledge of the workforce and improving healthcare teamwork; reduce avoidable inpatient and emergency care utilization
Four-hour in-class lectures on population health & care coordination, communication skills, chronic care medical management, behavioral health care management, data collection
Improved client performance on value-based payment measures and care coordination, reductions in potentially avoidable hospitalizations and emergent care
Identifying and reporting changes in patient health (August 2019) Agency 4 (n = 149 aides; 21% of workforce)
Educate care staff to identify, report, and communicate about subtle yet observable signs indicating changes in patient health corresponding to performance on value-based payment measures
Four-hour in-class lectures and discussion around methods and tools for reporting client health changes, communicating with nurses in response respond to alerts generated through an electronic reporting platform
Improved client performance on value-based payment measures and improved quality of patient care, as trained aides become aware of signs of potential changes in patient conditions and effectively communicate about the signs with other staff and the clinical team