
Abstract
This article presents a critical review of the influence of interracial and ethnic variation on pain prevalence, intensity, interference/function/disability, and treatment in older adults. A search of scientific databases published from 1900 to 2011, using key words associated with pain, geriatrics, and race/ethnicity, identified 180 articles, of which 27 empirical studies met the inclusion criteria. Of the retained articles, 17 reported that race/ethnicity was a statistically significant factor at p < .05. Minority older adults reported a higher prevalence of pain and higher pain intensity, and variable responses regarding function/disability compared with responses by non-Hispanic White older adults. Minority older adults were less likely to receive prescription pharmacologic treatments and surgery, and they were more likely to use complementary and alternative medicine treatments. There are interracial/ethnic differences in pain assessment and treatment interventions among older adults.
Introduction
Pain is one of the most prevalent problems for older adults (American Geriatrics Society [AGS], 2002) and can lead to adverse physical and psychological outcomes that affect quality of life (AGS, 2009; Shavers, Bakos, & Sheppard, 2010). The prevalence of chronic pain increases steadily with age; 58% to 70% of community-dwelling older adults have long-term pain-related problems (AGS, 2009). Interracial and ethnic differences have been documented in several dimensions of pain (Burgess, Ryn, Crowley-Matoka, & Malat, 2006; Heins et al., 2006). This article reviews the literature with regard to racial/ethnic differences in pain, focusing on the older population.
Racial and ethnic minorities, defined as persons who are not categorized as non-Hispanic White, include those categorized as African American or Black, Hispanic/Latino, American Indian or Alaska Native, Asian, and Native Hawaiian or other Pacific Islander (Shavers et al., 2010; U.S. Census Bureau, 2000, 2010). Racial/ethnic minority older adults (65 years or older) represent one of the fastest growing population segments in the United States (Helme & Gibson, 2001); minority elders will increase from 14.1% of all U.S. residents in 2020 to 18.3% by 2050 (U.S. Census Bureau, 2000) and will constitute 25% of all older adults (Administration on Aging [AOA], 1994-1995). The growing population of minority older adults underscores the significance of research on current and projected racial/ethnic disparities in health care (Schneider, Zaslavsky, & Epstein, 2002).
Racial/ethnic minorities are less likely to have a primary care physician, have less access to a pain clinic (Burgess et al., 2006; Heins et al., 2006), and use emergency services more than non-Hispanic Whites. It follows that they are less likely to receive adequate pain treatment (Heins et al., 2006). Minority elders may not receive adequate health services due to lack of insurance. However, even controlling for socioeconomic status, they are less likely to be exposed to specialty medical care such as pain management and are more likely to suffer higher rates of chronic diseases in conjunction with pain (Green, Baker, Smith, & Sato, 2003). Therefore, they are at risk for inadequate pain assessment and treatment associated with health problems (Green et al., 2003; Reyes-Gibby, Aday, Todd, Cleeland, & Anderson, 2007).
Although pain is one of the most prevalent problems for older adults (AGS, 2002), most research on interracial/ethnic variations in pain prevalence, pain intensity, pain interference (or pain-related disability or functional deficits) and pain treatment has notspecifically focused on older adults, which has implications for health status, quality of life, resource allocation, and disparities in medical care (Green et al., 2003; Reyes-Gibby et al., 2007). While there is an emerging literature documenting disparities in pain among racial and ethnic minorities, a synthesis of the existing literature is needed to address differences in interracial/ethnic pain domains specific to the minority older population and to improve pain treatment efficacy. The purpose of this critical review is to delineate interracial/ethnic differences in older adults in the areas of (a) pain prevalence; (b) pain intensity; (c) function, disability, or pain interference; and (d) pain treatment, including pharmacologic and nonpharmacologic strategies, such as surgery, and complementary and alternative medicine (CAM).
Method
Inclusion/Exclusion Criteria
Criteria for inclusion of literature in the systematic review were that (a) the article reported empirical research in English in a peer-reviewed journal; (b) the article included racial/ethnic groups, as defined by the U.S. Census Bureau: non-Hispanic White, African American or Black, Hispanic/Latino, American Indian or Alaska Native, Asian, and Native Hawaiian or other Pacific Islander (Shavers et al., 2010; U.S. Census Bureau, 2000), and articles that reported on only a single minority (non-White) racial group were also included in this review; (c) race or ethnicity was examined as a predictor of one of the targeted pain outcomes; (d) the mean age of participants in the study was 60 years or older; and (e) pain prevalence, intensity, treatment, and pain as it relates to function, disability, or interference were primary outcomes measured in the study. The reasons for selecting a mean age of 60 years or older were to be more inclusive of aging populations. Case studies and review articles were excluded, but all types of pain were included.
Searches for Data Extraction
Comprehensive literature searches were conducted using standard scientific search engines, starting with the earliest date available for each of the search engines: Medline (1965-2011), Cumulative Index to Nursing and Allied Health Literature (CINAHL; 1937-2011), Science Citation Index (1900-2011), The Cochrane Library (1998-2011), and Psych Info (1967-2011) for peer-reviewed journal articles published through July 2011. Search key words were (ethnic groups or ethnicity or race or racial groups) and (older adults or elderly or seniors or geriatric or aged) and (pain or pain prevalence) or (pain severity or pain intensity) or (pain assessment or pain measurement) or (pain treatment) or (arthritis). To ensure the most inclusive capture of relevant studies, multiple terms were utilized in the search methodology because of the inconsistent use of various terminologies referring to ethnicity, race, aging, and pain (Anderson, Green, & Payne, 2009).
Four critical areas were considered in reviewing each study: (a) pain prevalence; (b) pain intensity; (c) function, disability, or pain interference; and (d) pain treatment, including both pharmacologic and nonpharmacologic approaches, in racial/ethnic minority older adults. Some studies used the term pain severity instead of pain intensity; these studies were grouped with the pain intensity studies in this review. The relationship between pain and pain interference has important implications for older adults in terms of level of independence. Pain treatment studies retained for this review used instruments that measured function, disability, and pain interference. Consequently, all three of these domains were included in this review. While health status and quality of life measures are also relevant to pain, we focused on more specific essential Activities of Daily Living (ADL), including function, disability, and pain interference. For the purpose of this review the terms function and disability refer to physical, as opposed to psychological or cognitive, function and disability. Finally, studies did not use consistent terminology to refer to racial and ethnic groups, such as Blacks, African Americans, or non-Hispanic Blacks. Consequently, we used different terminology when referring to specific studies in order to remain consistent with the terminology used by each study.
Initial searches using the key words yielded 5,588 articles. Upon review of titles and/or abstracts of the items, 5,408 articles that did not meet the inclusion criteria were excluded due to the following reasons: duplicated studies (n = 567), mean age of participants <60 (n = 2,557), or article did not include race or ethnicity as a significant demographic characteristic (n = 2,284). Of the remaining 180 articles, 154 were excluded because none of the four critical areas was included as a major outcome variable. The authors agreed that the 27 empirical studies met the inclusion criteria for this review. Although the electronic database was reviewed from 1900 to the present, the oldest relevant article in this English language literature search was published in 1998.
Despite use of search key words relevant to geriatrics, the majority of published articles provided evidence of interracial/ethnic differences regarding pain in younger age groups (<60 years); many articles that included older adults and minority/ethnic groups in the descriptive demographics did not specifically evaluate pain in these groups, and few studies addressed interventions specific to racially/ethnically diverse older adults. Some studies (e.g., Ang, Ibrahim, Burant, & Kwoh, 2003; Baker & Whitfield, 2006) utilized instruments to measure function or disability that also include pain intensity (e.g., Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC]), but if pain intensity scores were not specifically reported, those studies were not included in the pain intensity section of this review.
Figure 1 illustrates the search process. Each of the studies identified as meeting criteria was thoroughly reviewed and details were recorded and analyzed. However, the reviewers were not blinded to the selected journals, institutions, and authors of the selected studies. All of the retained studies were descriptive and retrospective evaluations. Retained studies were assessed for relevance regarding the four pertinent areas of pain in older racial/ethnic groups, and whether race/ethnicity differences were statistically significant. Studies that addressed pain treatment were further evaluated to determine whether they included pharmacologic, surgical, and/or CAM treatment (Table 1).

Flowchart of study selection process for identifying systematic reviews.
Categories Addressed in the 27 Reviewed Articles.
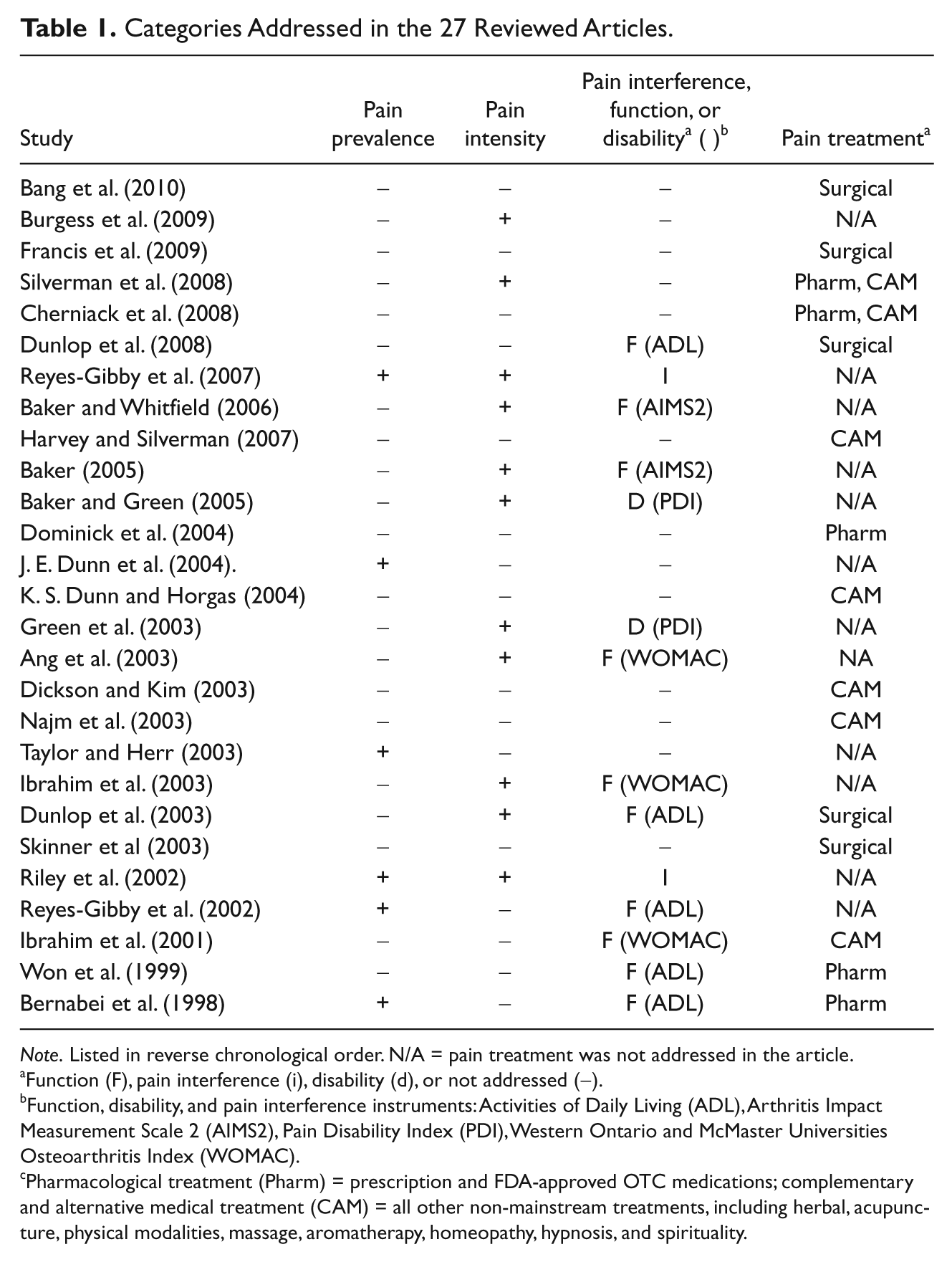
Note. Listed in reverse chronological order. N/A = pain treatment was not addressed in the article.
Function (F), pain interference (i), disability (d), or not addressed (−).
Function, disability, and pain interference instruments: Activities of Daily Living (ADL), Arthritis Impact Measurement Scale 2 (AIMS2), Pain Disability Index (PDI), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC).
Pharmacological treatment (Pharm) = prescription and FDA-approved OTC medications; complementary and alternative medical treatment (CAM) = all other non-mainstream treatments, including herbal, acupuncture, physical modalities, massage, aromatherapy, homeopathy, hypnosis, and spirituality.
Study Quality
The identified studies in the current review were assessed using 13 items selected from the Downs and Black quality rating checklist (Downs & Black, 1998), as modified by Meghani et al. in their review of the pain literature (Meghani et al., 2012; see Table 3). In the current review, item 6 (Are the main findings of the effect of race/ethnicity on the pain treatment outcome clearly described?) was modified to omit the word treatment to include all four pain components (prevalence, intensity, effects on daily activities, and treatment) in the current review. Each study was assessed with regard to the quality of the study design, study population, methodological rigor, and clarity of reporting.
The 13 items are scored as yes (1) or no or unable to determine (0). Scores are summed (maximum score 13), with higher scores indicating higher quality. Three categories for study quality were identified based on the percentage of criteria fulfilled (high when a study fulfilled 76% or more of the criteria, moderate when a study fulfilled 51% to 75% of the criteria, low when a study fulfilled 50% or less of the criteria; Meghani et al., 2012). The two authors independently extracted from the relevant articles the following: study design, sample size and characteristics, details of intervention and control group, type of musculoskeletal disorder, outcome measures, and main results. Disagreements were resolved by consensus.
Results
Twenty-seven articles describing racial/ethnic differences in pain in older adults were retained for this review. Table 2 summarizes the selected articles in terms of study design, mean age of participants, sample size, race/ethnicity of participants, pain or functional measures, and main results. Regarding type of design, 18 studies (67%) used cross-sectional design and 9 studies (33%) used longitudinal design. Telephone interviews were conducted in three studies (11%), 12 studies (44%) used self-administrated surveys, and 12 studies (44%) conducted secondary data analyses. Although English language articles published in the United States and international peer-reviewed journals were included in the literature search, all of the studies that met the inclusion criteria for this review were conducted in the United States.
Summary of the 27 Reviewed Articles (Arranged in Reverse Chronological Order).

*Race/ethnicity was a statistically significant factor at p < .05.
The reviewed studies showed significant differences in pain and health status based on race/ethnicity. Of the 27 studies, 17 (63%; Table 2 for more information) studies reported that race /ethnicity was a statistically significant factor at p < .05. Twenty-five studies (93%, excluding Dickson & Kim, 2003; Najm, Reinsch, Hoehler, & Tobis, 2003) included African Americans and 12 studies (44%) included Hispanics as study participants. Five studies (19%; Bernabei et al., 1998; Dickson & Kim, 2003; K. S. Dunn & Horgas, 2004; Francis, Scaife, Zahnd, Cook, & Schneeweiss, 2009; Najm et al., 2003) included Asian Americans or Pacific Islanders, and three studies (11%; K. S. Dunn & Horgas, 2004; Francis et al., 2009; Riley, Gilbert, & Heft, 2002) included American Indians. Five studies (19%) examined intraracial differences in only one racial/ethnic group. Four studies included African American elders (Taylor & Herr, 2003; Baker, 2005; Baker & Whitfield, 2006; Burgess et al., 2009), and one study included Korean older adults (Dickson & Kim, 2003).
Eight of the studies examined the effects of age. Four of these studies (Baker & Green, 2005; Bang et al., 2010; Dunlop et al., 2008; Reyes-Gibby et al., 2007) compared the older adults with a younger cohort, while the other four studies (Baker, 2005; Najm et al., 2003; Reyes-Gibby, Aday, & Cleeland, 2002; Won et al., 1999) examined various aspects of pain or pain treatment in older adult populations stratified by age. Four studies examined chronic pain in the veteran population (Ang et al., 2003; Burgess, et al., 2009; Ibrahim, Burant, Siminoff, Burant, & Kwoh, 2001; Ibrahim, Burant, Mercer, Siminoff, & Kwoh, 2003). All three of the studies that compared interracial/ethnic groups in the veteran population (Ang et al., 2003; Ibrahim et al., 2001, 2003) reported similar results for the pain domains studied in older adult minority groups and non-Hispanic Whites.
In terms of type of pain, one article (4%; Bernabei et al., 1998) focused on cancer pain, 11 articles (41%; Ang et al., 2003; Baker, 2005; Baker & Whitfield, 2006; Dickson & Kim, 2003; Dunlop, Song, Manheim, & Chang, 2003; Francis et al., 2009; Harvey & Silverman, 2007; Ibrahim et al., 2001, 2003; Silverman, Nutini, Musa, King, & Albert, 2008; Skinner, Weinstein, Sporer, & Wennberg, 2003) explored arthritis pain, one article (4%; Cherniack et al., 2008) described low back pain, and the rest (51%) examined chronic pain. None of the studies focused on acute pain.
Pain Prevalence
Of the 27 studies reviewed, prevalence of pain was reported in 5 studies (19%; Bernabei et al., 1998; J. E. Dunn, et al., 2004; Riley et al., 2002; Reyes-Gibby et al., 2002, 2007). Race/ethnicity influences the prevalence of reporting of pain. Based on year 2000 data from the Health and Retirement Study (Reyes-Gibby et al., 2007), community-dwelling Hispanic older adults reported higher pain prevalence than counterparts in other racial/ethnic groups compared with non-Hispanic Whites, non-Hispanic Blacks (odds ratio [OR] = 1.78; 99% confidence interval [CI; 1.33, 2.37]), and Hispanic Whites (OR = 1.80; 99% CI [1.26, 2.56]) were at greater risk for severe pain (p < .003; Table 2). In a survey of older nursing home residents with cancer pain, Bernabei et al. (1998) reported that older minority patients with cancer, including Asian Americans, American Indians, and Hispanics, were less likely than non-Hispanic Whites to report pain, even after controlling for language differences. In particular, African Americans had 63% greater probability of being untreated than non-Hispanic Whites (OR = 1.63; 95% CI [1.18, 2.26]; Table 2), which suggests that pain prevalence is underreported in this minority population. One study (J. E. Dunn et al., 2004) described a significantly higher prevalence of ankle pain in Puerto Rican Hispanics (44.7%) versus Non-Hispanic Whites (12.2%) and African Americans (17.5%), at p < .001. Another study (Riley et al., 2002) described a lower prevalence of facial pain in African American females (p < .05) than in White females (RR = 2.2, p < .01). One study (Reyes-Gibby et al., 2002) did not report any significance in pain prevalence among racial/ethnic groups (see Table 2 for details). Of the five studies that examined pain prevalence, three compared pain prevalence among older population stratified by age, but none of these articles made interracial/ethnic comparisons, and two (Reyes-Gibby et al., 2002, 2007) did not find significant difference in pain prevalence. One study (Won et al., 1999) noted that the OR for pain prevalence decreased when ages 75 to 84 years (OR = 0.81; 95% CI [0.77, 0.86]) and ≥85 years (OR = 0.64; 95% CI [ 0.61, 0.68]) were compared with the age group 65 to 74 years.
Pain Intensity
Eleven studies (41%) reported on pain intensity, and a majority of these studies revealed that racial/ethnic minorities rated their pain with higher intensity scores than did non-Hispanic Whites (see Table 2). African American or Hispanic older adults reported higher levels of pain intensity (Baker, 2005; Baker & Green, 2005; Baker & Whitfield, 2006; Burgess et al., 2006; Green et al., 2003; Reyes-Gibby et al., 2007; Riley et al., 2002; Silverman et al., 2008). In one study, one fourth of the non-Hispanic Blacks (OR = 1.78; 99% CI [1.33, 2.37]) and Hispanic Whites (OR = 1.80; 99% CI [1.26, 2.56]) reported high pain intensity, compared to 17% of non-Hispanic Whites (p < .0001; Reyes-Gibby et al., 2007). In another study, African Americans reported significantly more pain (M = 3.41, SD = 1.54 versus M = 2.63, SD = 1.37, p < .05) on the Multidimensional Pain Inventory, 7-point Likert-type scale, as well as more depression due to pain, and more disability than did non-Hispanic Whites (Green et al., 2003).
While most studies did not specifically evaluate reasons for differences in pain intensity, one study suggested that alleged racial discrimination may affect pain intensity (Burgess et al., 2006). In the study by Burgess et al. (2006), the perception of racial discrimination among African American male veterans was associated with higher levels of bodily pain compared to Whites (β = −0.25, p < .0001), even after controlling for socioeconomic (e.g., age, employment status, years of education, income) and health-related characteristics.
Higher pain intensity has been documented in younger and older minority groups, including African Americans and Hispanics (Baker & Green, 2005; Silverman et al., 2008). Two studies examined pain intensity by age in African Americans without interracial comparisons. Baker and Green (2005) noted that African Americans under age 50 years had significantly higher pain levels (McGill Pain Questionnaire [MPQ] scores, p < .01) than African Americans equal to or older than age 50 years, while Baker (2005) also found a negative correlation between pain intensity and age among older African Americans.
Function, Disability, or Pain Interference
The relationship between pain and its effects on daily activities is relevant, but different studies used different instruments to determine the effects of pain on daily activities, using measures of function, disability, or pain interference. Fourteen studies (52%) reported on function, disability, or pain interference. Of the 10 studies that reported on function, five used ADL scores (Bernabei et al., 1998; Dunlop et al., 2003, 2008; Reyes-Gibby et al., 2002; Won et al., 1999), two used the Arthritis Impact Measurement Scale 2 (AIMS2; Baker, 2005; Baker & Whitfield, 2006), and three used the WOMAC (Ang et al., 2003; Ibrahim et al., 2001, 2003) to measure physical function. Of the five studies that reported on ADLs, two (Bernabei et al., 1998; Reyes-Gibby et al., 2002) did not assess function relative to race, and Dunlop et al. (2003) reported greater functional limitations among minorities (Whites 34%, Blacks, 47%, Hispanics 50%) and noted higher ADL limitations (greater disability) for minority older adults versus older Whites (OR = 2.48; 95% CI [1.52, 4.04]; Table 2).
In a subsequent study (Dunlop et al., 2008), compared to Whites, a significantly higher proportion of Blacks and Hispanics (Blacks 43.41%, Hispanics 43.73%, vs. Whites 28.98%; p < .001) had more physical limitations for >65 age group. Similarly, compared to Whites, a significantly higher proportion of Blacks and Hispanics (Blacks 16.04%, Hispanics 16.29%, vs. Whites 8.01%; p < .001) had higher ADL scores for >65 age group, where higher ADL scores are associated with greater disability. Similar findings of significantly higher physical limitation and ADL scores for Blacks and Hispanics compared to Whites were noted for the 51 to 64 age group (p < .001). In another study (Won et al., 1999), daily pain was associated with higher ADL scores in older adults (OR = 2.47; 95% CI [2.34, 2.60]), but there was no interracial/ethnic comparison. The two studies that used the AIMS2 were performed only in African American older adults, with no interracial comparisons. One study found that pain intensity was significantly related to physical impairment (Baker & Whitfield, 2006; β = 0.30, p < .01), and the other study noted that physical impairment was significantly related to pain intensity (r = 0.39, p < .01; Baker, 2005). None of the three studies (Ang et al., 2003; Ibrahim et al., 2001, 2003) that used the WOMAC instrument noted any significant differences between racial/ethnic groups.
The two studies that examined disability used the Pain Disability Index (PDI; Baker & Green, 2005; Green et al., 2003). Baker and Green (2005) noted higher disability in African Americans than in Whites but did not make direct comparisons to determine the significance of this finding; Green et al. (2003) found that Blacks had a significantly greater disability than Whites (M = 42.35, SD = 13.96 versus M = 38.03, SD = 14.76; p = .0032).
The remaining two studies (Reyes-Gibby et al., 2007; Riley et al., 2002) examined pain interference based on a single specific item posed by the researchers. Riley et al. (2002) evaluated pain interference due to orofacial pain based on the statement: “I limited my daily activities or just stayed at home.” Black males, compared to White males, had an increased OR of 4.19, and White females had an increased OR of 2.07 for limiting activity due to jaw pain when compared to Black females. Black males, compared to White males, had an OR of 1.84 for limiting activity due to toothache. Significance was not reported (Riley et al., 2002). Among those reporting pain (60%) in the Reyes-Gibby et al. (2007) study, a majority in all racial/ethnic categories described limitations associated with pain-related activity, but minority adults experienced more functional limitations/impairment as a result of pain (Reyes-Gibby et al., 2007).
Based on the question: “Does the pain make it difficult for you to do your usual activities such as household chores or work?” Non-Hispanic Blacksreported higher rates of pain interference compared to Hispanics and non-Hispanic Whites (non-Hispanic Blacks 51%, Hispanics 35%, non-Hispanic Whites 39%; p = .028) for mild levels of pain (Reyes-Gibby et al., 2007). However, there were no significant interracial differences noted for pain interference at moderate/severe levels of pain in this study.
Pain Treatment
Fifteen studies met the inclusion criteria in this area and were included for the current review (Table 1). In order to characterize the reviewed studies, articles were categorized based on whether they addressed (a) pharmacological, (b) surgical, and/or (c) CAM treatments. Pharmacological treatment refers to FDA-approved prescription or nonprescription medications and does not include herbal or dietary supplements (which are discussed in the CAM treatment section). The only retrieved studies that addressed interventional pain treatments or surgical treatments were arthroplasty studies. CAM refers to non-Western allopathic medical treatments, including traditional remedies used by different cultures, such as herbal extracts, dietary supplements, and acupuncture, as well as religious coping methods. All of the reviewed studies were observational; there were no prospective interventional treatments performed.
Pharmacologic pain treatment
Although a significant number of studies examined pharmacological pain therapy in older adults, 5 studies (19%; Bernabei et al., 1998; Cherniack et al., 2008; Dominick et al., 2004; Silverman et al., 2008; Won et al., 1999) met the inclusion criterion of reporting pharmacologic pain therapy in interracial/ethnic minority older adults. Bernabei et al. (1998) reported on cancer pain treatment among nursing home patients. Approximately 28% of Hispanic patients and 31% of African American patients received analgesics of insufficient strength to manage their pain. African American patients were 63% more likely than non-Hispanic White patients to receive no pain medication (OR = 1.63; 95% CI [1.18, 2.26]; Bernabei et al., 1998). Both Hispanic and Black older veterans were likely to receive fewer days supply of analgesics than were non-Hispanic White veterans. Dominick et al. (2004) revealed that Hispanics were less likely to receive a prescription nonsteroidal anti-inflammatory drug (OR = 0.47; p < .01) than Whites; and Blacks and Hispanics were likely to receive fewer days prescription of pain medications than Whites (38, 31, and 43 days respectively, p < .01; Dominick et al., 2004). Also, pain medications were less likely to be prescribed for Blacks (OR = 1.69; 95% CI [1.40, 2.05]) and Hispanics than Whites (OR = 1.56; 95% CI [0.70, 1.04]; Won et al., 1999). In another study of community-dwelling older adults (Silverman et al., 2008), African Americans were more likely than non-Hispanic Whites to use topical analgesic treatments (OR = 1.83; p < .05), including ointments, creams, hot/cold treatments, and self-massage. In a different study (Cherniack et al., 2008), Hispanics were the greatest users of over-the-counter (OTC) medications to treat low back pain (p < .001).
Surgical treatments
Five reviewed studies (19%) reported racial/ethnic disparities among older minority groups in the utilization of arthroplasty to treat hip and knee arthritis pain (Bang et al., 2010; Dunlop et al., 2003, 2008; Francis et al., 2009; Skinner et al., 2003). Although older African American and Hispanic minorities were more likely than non-Hispanic Whites to complain about arthritis and functional limitations, older minorities were significantly less likely than non-Hispanic White counterparts to undergo joint replacement, even after controlling for socioeconomic status and comorbid medical issues (Bang et al., 2010; Dunlop et al., 2003, 2008; Francis et al., 2009). A large national database study of hip and knee arthroplasties using annual data from 1996, 2000, and 2004 for individuals ≥65 years old revealed significant disparities between Hispanic and Black minority groups compared with Whites. The ORs for hip arthroplasties for each year respectively were: 0.35 (95% CI [0.31, 0.40]), 0.41 (95% CI [0.36, 0.47]), and 0.47 (95% CI [0.40, 0.53]) for Blacks compared to Whites (p < .0001), and 0.40 (95% CI [0.32, 0.50]), 0.39 (95% CI [0.28, 0.55]), and 0.37 (95% CI [0.31, 0.44]) for Hispanics compared to Whites (p < .0001). Similarly, ORs for knee arthroplasties for each year respectively were 0.46 (95% CI [0.41, 0.52]), 0.55 (95% CI [0.49, 0.61]), and 0.52 (95% CI [0.46, 0.59]) for Blacks compared to Whites (p < .0001), and 0.66 (95% CI [0.55, 0.79]), 0.71 (95% CI [0.61, 0.83]), and 0.75 (95% CI [0.61, 0.91] for Hispanics compared to Whites (p < .0001, except for 2004 when p = .004; Bang et al., 2010).
In a study by Dunlop et al (2003), older minorities were significantly less likely to undergo arthroplasties than Whites (OR = 0.37; 95% CI [0.20, 0.71]; Dunlop et al., 2003). In a more recent study by Dunlop et al (2008), which controlled for health and income variables, it was noted that hazard ratios (HR) for hip and knee surgery comparing older Black versus Whites was 0.38; 95% CI [0.16, 0.55] (reported as statistically significant; no p values reported), while the HR for older Hispanics versus Whites was 0.60; 95% CI [0.32, 1.10], which was not statistically significant. Income levels were primarily responsible for the differences between the Hispanic and White groups. Furthermore, there was no significant difference in the rates of these surgeries between Blacks, Whites, and Hispanics under age 65 years. Finally, in the study by Fancis et al. (2009), it was noted that OR for minority versus White older adults for joint arthroplasties were between 0.60 and 0.69 for urban and rural residents, respectively (Francis et al., 2009).
Differences in intensity of symptoms did not explain observed interracial/ethnic differences in utilization of joint replacement. Regional differences in knee arthroplasty rates accounted for differences among Hispanics and Black females when compared with non-Hispanic Whites, but differences for Black males compared with non-Hispanic White males (1.84 per 1,000 versus 4.82 per 1,000; p < .05) persisted even after adjusting for regional variations in knee arthroplasties (Skinner et al., 2003).
Complementary and alternative medicine
Seven studies (27%; Cherniak et al., 2008; Dickson & Kim, 2003; K. S. Dunn & Horgas, 2004; Harvey & Silverman, 2007; Ibrahim et al., 2001; Najm et al., 2003; Silverman et al., 2008) address CAM therapies for pain in minority elders. Four of these studies (Dickson & Kim, 2003; K. S. Dunn & Horgas, 2004; Ibrahim et al., 2001; Silverman et al., 2008) focused on the use of CAM for pain, while the other three studies assessed CAM for pain as part of general medical conditions and chronic illness. It was noted that Asians preferred dietary supplements, oriental medicine, and acupuncture for pain treatment; Hispanics preferred dietary supplements for treatment of arthritis; and non-Hispanic Whites preferred chiropractic and massage for pain treatment (Najm et al., 2003). In the same study, there was no difference in CAM use among age-stratified groups (i.e., 65-69, 70-74, 75-79, 80-84, 85+) of older adults (Najm et al., 2003). African Americans were more likely than non-Hispanic Whites to use movement/exercise for arthritis pain (OR = 1.64, p ≤ .05) and less likely to rely on diet supplements or diet change (OR = 0.58; p ≤ .01; Silverman et al., 2008). Older African Americans were more likely than older Whites to rely on home care remedies and CAM (Ibrahim et al., 2001). In this study using ORs adjusted for age, disease severity, functional status, socioeconomic status, and depression, the authors report that treatments such as medicated creams (OR = 2.27; 95% CI [1.38, 3.73]), massage (OR = 2.54; 95% CI [1.48, 4.37]), herbal medicine (OR = 1.71; 95% CI [1.11, 2.63]), and copper bracelets (OR = 1.67; 95% CI [1.07, 2.60]) were efficacious (Ibrahim et al., 2001). In a qualitative study, seven Korean older women used folk remedies, such as herb teas, moxa, cautery, and copper bracelets, to treat osteoarthritis pain (Dickson & Kim, 2003).
Three studies (K. S. Dunn & Horgas, 2004; Harvey & Silverman, 2007; Ibrahim et al., 2001) addressed religious coping strategies in older African American population with chronic pain. African Americans tended to rely more on religious coping strategies (K. S. Dunn & Horgas, 2004; Harvey & Silverman, 2007) than on other CAM treatments. In one of the studies, religious coping strategies were significantly more common in African Americans than in Whites (t = 5.65, p ≤ .01; K. S. Dunn & Horgas, 2004). In another study (Harvey & Silverman, 2007), older African Americans were more likely than Whites to think of God in terms of healer or enabler. Ibrahim et al. (2001) also noted that African Americans are more likely than Whites to rely on prayer to deal with pain (OR = 1.93; 95% CI [1.19, 3.14]; Ibrahim et al., 2001).
Twelve of the studies had subject sizes of 2,000 or greater (Table 2) and four of these studies had databases of greater than 40,000 subjects (Bang et al., 2010; Francis et al., 2009; Won et al., 1999; Skinner et al., 2003). Most of the remaining studies involved several hundred subjects. One qualitative research study (Dickson & Kim, 2003) had only 7 subjects and two other studies involved fewer than 100 subjects (Harvey & Silverman, 2007; Taylor & Herr, 2003). Studies dealing with pharmacological and surgical treatments uniformly had large subject size, while some of the CAM studies had smaller study population, so the quality of the CAM evidence was not as strong due to the small population size (Dickson & Kim, 2003; Harvey & Silverman, 2007; Taylor & Herr, 2003).
Results of Study Quality
Tables 3 and 4 show results of the consensus review, based on the modified Downs and Black quality index. Table 3 reveals that 20 studies (74%) were retrospective and the remaining seven studies were prospective (Dunlop et al., 2003, 2008; Ibrahim et al., 2001, 2003; Riley et al., 2002; Silverman et al., 2008; Taylor & Herr, 2003). All of the studies clearly described their hypotheses/objectives (Item 2). In most of the studies, the main outcomes measured were clearly described (Item 3), the racial/ethnic breakdown of the study population was clearly described (Item 4), and the statistical tests used to assess the main outcomes were appropriate (Item 9). The use of race and ethnicity in the analysis (Item 10) was scored zero score if there was no control group for comparison.
The Modified Downs and Black Quality Rating Checklist.

Review Scores and Quality Ratings.
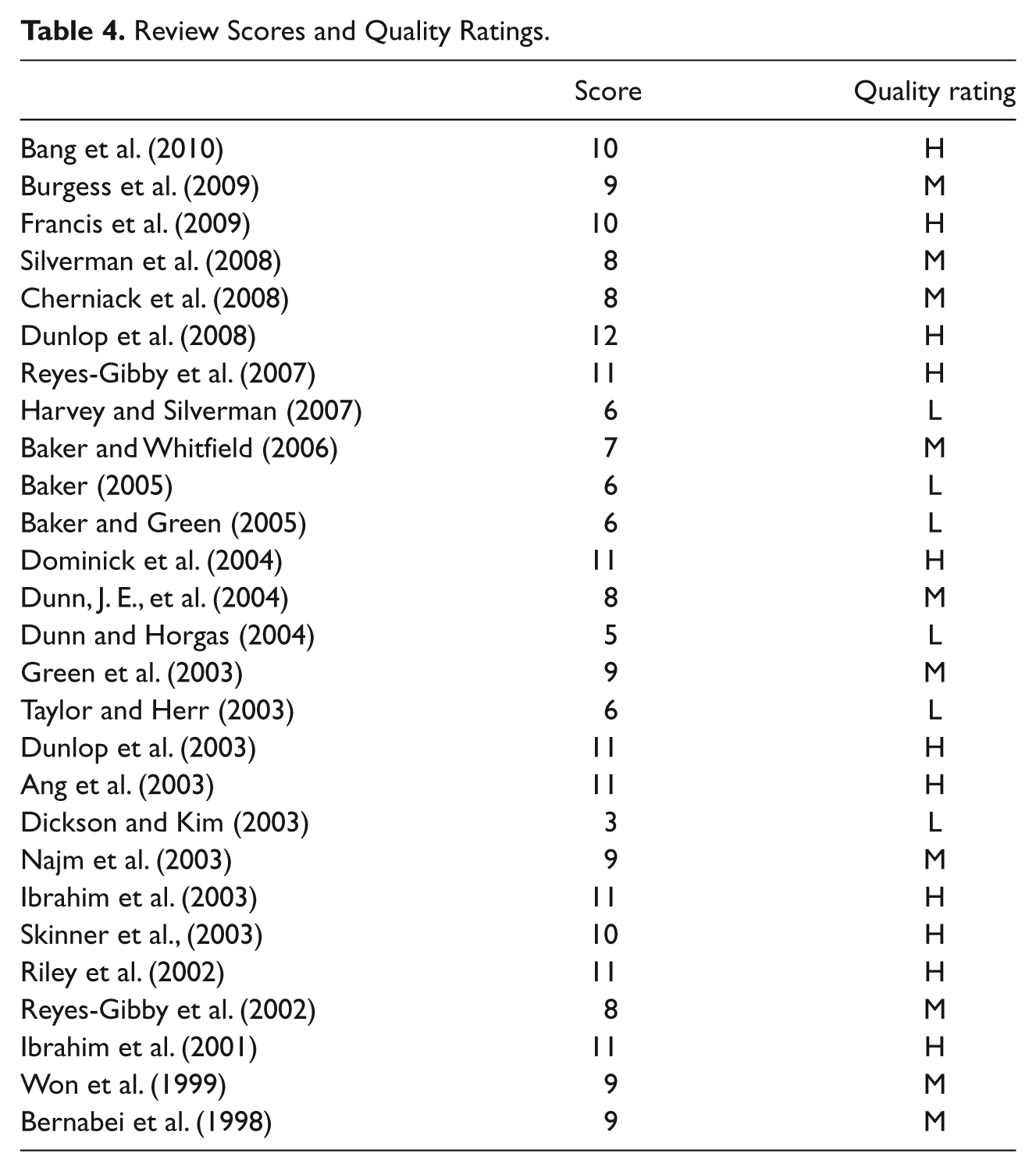
The quality scores for the retained studies ranged from 3 to 12 (maximum possible score = 13; Table 4). Only 11 of the 27 studies (41%) received high-quality scores (achieving at least 76% of the criteria); 10 studies (37%) received moderate-quality scores (51% to 75% of the criteria), and 6 studies (22%) received low-quality scores (50% or less of the criteria).
Discussion
There is lack of empirical evidence regarding interracial/ethnic-related variation in pain and pain treatments (Austrian, Kerns, & Carrington Reid, 2005), especially in minority older adults. In the current review, a majority of the studies focused on African Americans or Hispanics; few studies included Asian Americans, Pacific/Islanders, or American Indians, and, where included, these groups usually represented only a small percentage of the minority older adults sample in the study (K. S. Dunn & Horgas, 2004; Francis et al., 2009; Riley et al., 2002). Some of the studies used very broad racial and ethnic categories, such as “Asian,” whereas other studies examined a specific ethnic group (e.g., Korean Americans; Dickson & Kim, 2003). Different terminologies were used to characterize racial and ethnic groups, such as Blacks, African Americans, and non-Hispanic Blacks. More attention should be given to the selection of population and source of population, and studies should include control groups that are matched to the general structure of the treatment groups.
Methodologically, only seven of the studies were prospective, and most of the studies used a cross-sectional design. Thus, it is difficult to draw firm conclusions based on empirical evidence regarding pain and pain treatment in these population. Other methodological concerns were identified, including unclear selection criteria, inadequate use of pain assessments in cognitively impaired older minority population, and lack of randomization of pain treatments. Lack of control in sampling and design limits the generalizability of the results of each of the reviewed studies. The majority of these studies used reliable and validated measures across race/ethnicity; however, these measures were not validated specifically for psychometric properties in older minority population. Some of the instruments used to rate physical function and disability were not specific to pain-related deficits. Some of the studies that evaluated CAM treatments were not specific to CAM for pain, but evaluated CAM for general medical issues. There were relatively few robust arthritis studies on race/ethnicity differences in older adults where pain was an outcome variable, and these studies mainly dealt with hip and knee joint surgeries. With regard to pain treatments studies, there is a need for rigorous design, including prospective random controlled trials, which could increase internal validity.
Confounders associated with classification of race/ethnicity may influence pain-related outcomes among racially/ethnically diverse older adults (Anderson et al., 2009). In particular, language barriers, socioeconomic status (e.g., education level, income, insurance status, and access to transportation; Reyes-Gibby et al., 2007), and social support adversely affect access to health care. In addition, country of origin, religious beliefs, and level of acculturation are likely to be confounding variables that may influence pain perception, assessment, and choice of type of nonpharmacologic treatments in minority older patients (Anderson et al., 2009; Dente, Herman, Allen, & Hunt, 2006). For example, minority patients were more likely to report increased burden in paying for health care, even with Medicare and/or Medicaid (Edwards, Moric, Husfeldt, Buvanendran, & Ivankovich, 2005). It is also unclear whether veteran status is a confounder because none of the studies of older veterans noted significant differences between minorities and non-Hispanic Whites.
Regarding quality assessments of the 27 retained studies based on the modified Downs and Black quality rating checklist (Meghani et al., 2012), only 7 of the 15 studies included in the treatment section utilized prospective research design, which may require a more rigorous approach (e.g., randomized controlled design) to accurately measure pain-related outcomes related to race /ethnicity. Although confounding variables associated with pain-related outcomes were identified in the literature, only 15 studies adjusted for confounding variables in the analysis and 20 studies identified principal confounders in each ethnic group. The procedures used to estimate sample size and power analysis (Item 13) were described in only two studies (Skinner et al., 2003; Taylor & Herr, 2003). This question probably underestimated the quality of many of the studies because many of the studies dealt with large databases for secondary data analyses that had enough power to address the research questions.
This review underscores the interracial/ethnic variations in pain prevalence, intensity, function/disability/pain interference, and treatment. Minority older adults frequently receive a lower quality of care than non-Hispanic Whites. The challenge for addressing interracial/ethnic differences in pain and its treatment is to increase evidence-based data and convert this understanding to meaningful interventions to reduce and eventually eliminate disparities (Meghani et al., 2012).
Limitations
Notable limitations of the current review are identified. This literature search was limited to English language peer-reviewed journals. Also, the search strategy may not have retrieved all relevant articles that met the inclusion criteria, which could produce bias in the conclusions presented in the review. The absence of standardized terminology for race and ethnicity may have limited retrieval of all relevant articles, although a broad search strategy, including multiple terms, was utilized.
Implications for Health Care Providers and Policy Makers
The misperceptions of health care providers with regard to pain assessment and treatment may contribute to racial, ethnic, and cultural disparities in care (Shavers et al., 2010). Understanding racial and ethnic variations in perception and response to pain is essential for optimal pain management (Shavers et al., 2010). Greater awareness of minority differences among the older adults is the first step to address gaps in knowledge and competencies related to pain that may contribute to reducing disparities in pain care (Gerontological Society of America, 2012).
Policy makers should identify flexible strategies that take into account the various values and norms of diverse older racial/ethnic groups to optimize access to pain treatment and to ensure that medical care is sensitive to their needs and cultural diversity. Health care providers should be aware of interracial and ethnic variation in attitudes toward pain and pain management, and how this affects patient pain presentation and decision making. Understanding ethnic variations that affect patient perception and response to pain is essential to optimal pain management (Shavers et al., 2010). Health care providers may lack knowledge and training related to health care services for racial and ethnic minority patients. Deficiencies may include inadequate pain assessment and treatment, as well as mistaken beliefs and unrealistic expectations regarding the patients (Anderson et al., 2009). Understanding of these differences should also be included in continuing education training for health care providers.
Recommendations for researchers in this field include further study to determine how confounders, such as differences in pain beliefs, coping strategies, perceived locus of control, self-efficacy, and outcomes expectations, affect pain evaluations and outcomes in older racial/ethnic groups. Based on this review, there is a need for more prospective and interventional randomized controlled trials to test different strategies for assessing pain in older minority patients, improving communications between patients and providers regarding options for pain treatment, and determining the effectiveness of pain treatment modalities based on patient preferences. More research is needed to understand pain in older adults across race/ethnicity in order to measure the effectiveness of pain interventions in this population and to identify strategies that improve pain management in diverse racial/ethnic groups (Park & Hughes, 2012).
Conclusion
Although increasing empirical evidence shows interracial/ethnic differences related to pain, there are only limited findings focusing on pain and pain treatment in minority elders. Pain scores are generally high in minority older adult populations and there are differences in pain treatments among minority groups, such as reduced levels of opioid analgesic dosing, lower utilization of arthroplasty, and differences in acceptance of CAM pain treatment modalities. Until more conclusive evidence is available, health care providers are encouraged to exhibit sensitivity to differences related to racial/ethnic background in order to improve health care services for this population and to foster health policies that can remediate ethnic/racial disparities in pain care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.