
Abstract
Keywords
Introduction
Chronic pain represents a significant public health challenge in the United States, with an estimated 100 million Americans suffering from common chronic pain conditions (Gaskin & Richard, 2012; Institute of Medicine, 2011; U.S. Department of Health and Human Services, 2016). In fact, pain has been cited as one of the most common and costly medical problems currently facing the United States (Gaskin & Richard, 2012). This high prevalence of chronic pain is projected to grow in part because of the demographic shifts in the United States (Institute of Medicine, 2011; U.S. Department of Health and Human Services, 2016). Projections show a continued rapid growth of older adults, where between 2012 and 2050, the population aged 65 and over is projected to almost double to 83.7 million (Ortman, Velkoff, & Hogan, 2014). While anyone may be at risk for pain, older adults are at particular risk of suffering from chronic pain. Estimates show that nearly 60% to 75% of adults over age 65 years report at least some persistent pain level (Molton & Terrill, 2014; Tsang et al., 2008). The prevalence of pain is even higher when examining older adults in assisted living or nursing homes (Molton & Terrill, 2014; Tsang et al., 2008). The association between age and pain is in part due to greater prevalence of chronic medical comorbidities in later life, and a growing number of Americans are expected to experience diseases associated with pain, such as arthritis (Institute of Medicine, 2011).
Chronic pain can have serious quality of life consequences and has been shown to significantly contribute to morbidity, disability, and premature mortality (Institute of Medicine, 2011). Older adults in persistent pain are likely to limit their physical activity, which may lead to a cycle of restriction, decreased participation, and greater disability (Jensen, Moore, Bockow, Ehde, & Engel, 2011; Molton & Terrill, 2014). Recent literature has established linkages of some socioemotional health variables, such as loneliness, as predictors of pain. Defined as the discrepancy between desired and perceived social relationships (Peblau & Perlman, 1982), loneliness has been associated with worse pain outcomes in chronic pain patients (Jaremka et al., 2013; Oishi, Schiller, & Gross, 2013; Wolf & Davis, 2014; Wolf, Davis, Yeung, & Tennen, 2015). In one study, loneliness predicted chronic back pain 7 years later (Jacobs, Hammerman-Rozenberg, Cohen, & Stessman, 2006). In another cross-sectional study of elderly Chinese patients in nursing homes, loneliness was more prevalent among chronic pain than nonchronic pain patients (Tse, Leung, & Ho, 2012). Although these studies suggest a link between loneliness and pain, to date no literature exists on the relationship in the other direction. Older adults may limit their social interactions due to physical pain. As such, pain might be associated with the onset of loneliness. We posit that the linkage between pain and loneliness can be bidirectional, where pain may also have an effect on loneliness. Older adults may limit their social interactions due to physical pain. This suggests that even those older adults who may not be traditionally considered at risk for loneliness (e.g., those married and/or living with others) could still be at risk for loneliness if they are experiencing pain. Thus, the aim of the current study is to examine whether pain is associated with the onset of loneliness in a sample of community-dwelling older adults. This is important because such a link suggests that appropriate pain interventions could prevent future loneliness, which in turn could prevent functional decline, disability, and premature mortality.
Method
Data
We used data from the 2008 and 2012 Health and Retirement Study (HRS). The HRS is a national area probability study of elderly households in the United States (HRS, 2016). Since 1990, the HRS collects data through in-person interviews biannually. In 2004, the HRS added self-administered questionnaires that were left with respondents upon the completion of the in-person interviews. These “Leave Behind (LB) questionnaires” included participants’ evaluations of their life circumstances and subjective well-being, including loneliness. We therefore used data from the HRS LB questionnaires for our analyses.
Sample
Although the core HRS is conducted biannually, the LB questionnaire was only administered every other wave. Therefore, we linked data from the 2008 HRS wave to 2012. We limited the sample to community-dwelling persons aged 60 years and over who were not lonely in 2008 in order to predict the risk of onset of loneliness (incidence) in 2012. All analyses used the 2008 HRS-provided sample respondent weights. After removing respondents with a zero respondent sample weight, we had a final analytic sample of 1,563 community-dwelling older adults.
Measures
To examine loneliness, we used the three-item loneliness scale (Hughes, Waite, Hawkley, & Cacioppo, 2004). Respondents rated on a scale of 1 (often) to 3 (hardly ever/never) how often they felt (a) they lacked companionship, (b) left out, and (b) isolated from others. Cronbach’s alpha for the scale was .76, which is a satisfactory value for comparing groups (Bland & Altman, 1997). Following extant research (Gerst-Emerson & Jayawardhana, 2015; Perissinotto, Stijacic Cenzer, & Covinsky, 2012), we dichotomized this scale by coding elders who responded “some of the time” or “often” to any of these three items as lonely.
Our main predictor variable of interest was pain. The HRS asked respondents “Are you often troubled with pain?” and those that responded “yes” were counted as being in pain. The potential confounding variables in the model were based on the literature (Emerson & Jayawardhana, 2016) and included sociodemographic variables of age (continuous), race/ethnicity (non-Hispanic Black, Hispanic, Non-Hispanic Other, Non-Hispanic White = reference), education (high school or more vs. less than high school), gender (male = reference), and marital status (not married = reference).
Pain is intricately linked to both physical as well as mental health conditions, and the model controlled for a variety of variables in both physical and mental health. Physical health included self-rated health, recoded into a dichotomous variable comparing “good/very good/excellent health” with “fair/poor health” (reference category). We also created a count of self-reported health conditions: high blood pressure, diabetes, cancer, lung disease, heart disease, stroke, or arthritis (range: 0-7). To capture physical disability, we used the Katz Activities of Daily Living (ADL) Scale (Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963). The ADL items measured self-reported difficulty with bathing, eating, toileting, dressing, transferring to/from bed, and walking. The items were added together to create a count of ADL limitation variable (range: 0-6). We measured psychological distress with the HRS short version (eight items) of the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977), which had a Cronbach’s alpha of .716 in our sample. Following previous literature, we dichotomized this scale into CES-D score ≥ 3 as high depressive symptoms (Andresen, Malmgren, Carter, & Patrick, 1994; Schane, Woodruff, Dinno, Covinsky, & Walter, 2008). We used a subjective measure to control for financial situation, using the survey question that asks respondents how satisfied they were with their current financial situation: satisfied (completely/very/somewhat) or not satisfied (not very/not at all).
Statistical Analysis
Because we examined change in loneliness status (onset of loneliness), we included each characteristic as a change across time. Therefore, each time varying variable was coded as improving, worsening, or staying the same (reference group) from 2008 to 2012. For example, if there was an increase in the number of chronic conditions reported across time, the variable in the model would be “worsening number of conditions,” as referenced to no change. All non–time varying variables remained constant in the model. We conducted a logistic regression analysis to examine the relationship between pain and the onset of loneliness controlling for potential confounding factors. All analyses were performed using Stata Version 14.1 (StataCorp LP, College Station, TX).
Results
Table 1 provides descriptives of the analytic sample, for baseline (2008) and follow-up (2012). Approximately 31.6% of participants reported loneliness at follow-up. At baseline, 27.3% of the sample reported pain, which increased to 30.2% at follow-up. A majority of the sample was female (56.9%), had a high school degree or more (84.9%), and was non-Hispanic White (84.4%). The average age at baseline was 71.1 (range: 60-94). A majority of the sample was married, though the proportion married declined from baseline (74.85%) to follow-up (68.8%). Those with high depressive symptoms increased between time periods, with 5.25% at baseline and 9.3% at follow-up, though there may be some overlap in prevalence. Physical health declined over the 4 years in both objective measures (ADL limitation, number of chronic conditions) and subjective measures (self-reported health).
Sample Descriptives at Baseline (2008) and Follow-Up (2012).

Note. All numbers in percent unless otherwise noted. Sample size = 1,563 unweighted; ADL = activities of daily living.
Table 2 presents results from the logistic regression examining the association of pain with the onset of loneliness from not lonely at baseline to lonely at follow-up. Results are presented in odds ratios to help the interpretation of the associations. Our main variable of interest, pain at both years, was significantly associated with incidence of loneliness. The odds of loneliness onset was 1.58 higher for those with pain at both time points compared with those who had pain at neither year. This relationship held even after controlling for physical and mental health conditions. The increase in number of chronic conditions and increase in ADL limitations were not significantly associated with loneliness. However, worsening of subjective health (self-rated health variable) was positively associated with loneliness, where those with worsening self-rated health had 1.70 higher odds of experiencing the onset of loneliness. In addition, respondents with worsening depressive symptoms (going from low to high depressive symptoms) had over double the odds of loneliness onset (OR = 2.08). We ran interaction models (results available upon request) interacting the significant symptoms with pain, and no interaction effects were significant. This suggests that there is not a synergistic relationship between pain and subjective health or depressive symptoms. A number of other control variables were significantly associated with loneliness, including losing a partner (positive association), married at both years (negative association), Hispanic (negative association), and higher education (negative association).
Logistic Regression Results on the Association of Pain and the Onset of Loneliness, Combining Data From 2008 and 2012.
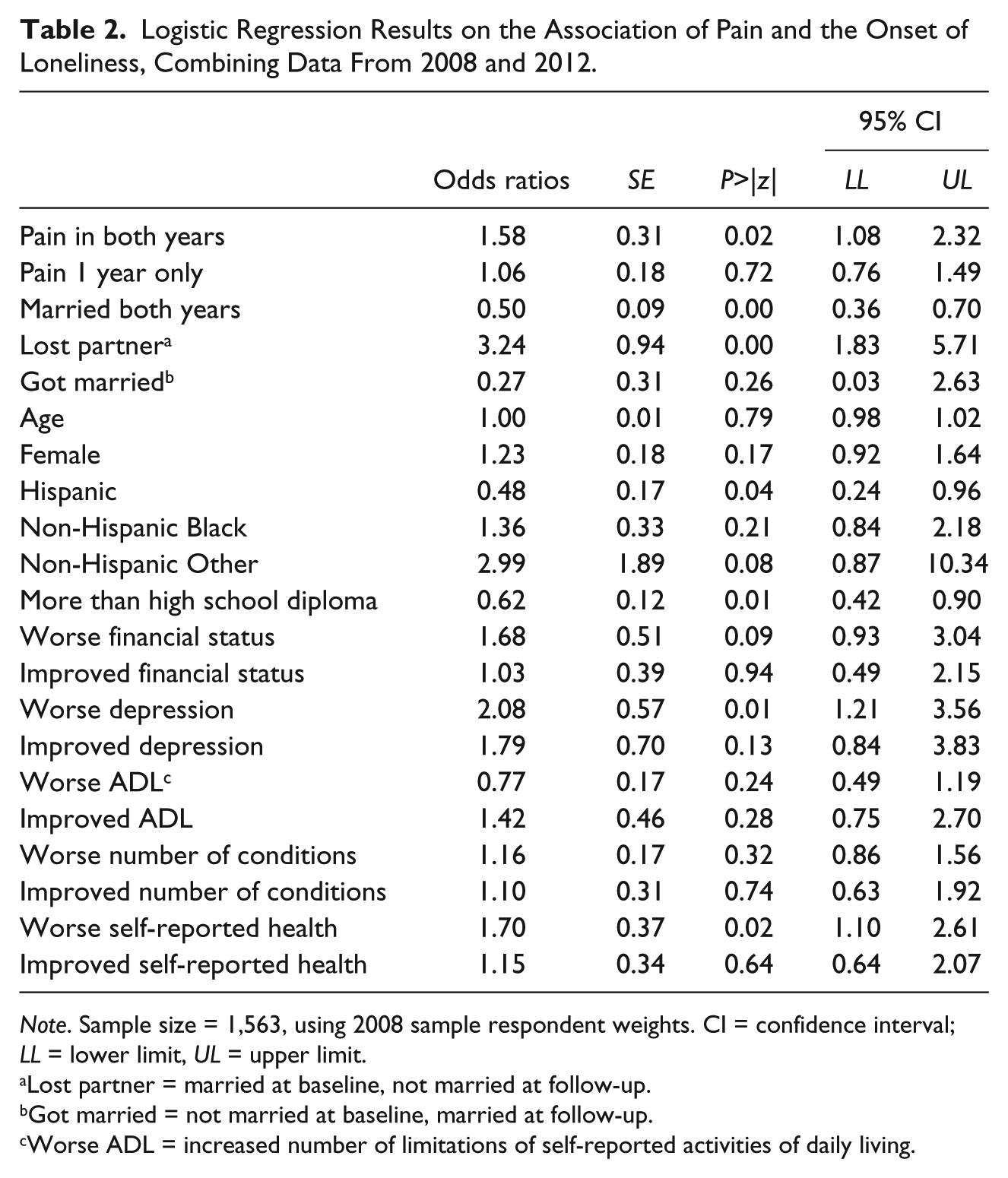
Note. Sample size = 1,563, using 2008 sample respondent weights. CI = confidence interval; LL = lower limit, UL = upper limit.
Lost partner = married at baseline, not married at follow-up.
Got married = not married at baseline, married at follow-up.
Worse ADL = increased number of limitations of self-reported activities of daily living.
Discussion
Pain is a significant problem for many older adults, but the social consequences of pain remain inadequately explored. This study shows that consistent pain (pain in both time periods) was significantly associated with the onset of loneliness in a sample of community-dwelling older adults, independent of potentially confounding variables. While previous research has established loneliness as a risk factor for pain, this study suggests that the linkage between the two may be in the other direction as well: Pain may increase the risk of loneliness. Pain in only one year was not significantly associated with loneliness at follow-up, suggesting that the association may not be significant for short term or temporary pain. Rather, pain that is consistent over longer periods of time appears to be a risk factor for loneliness.
The relationship between consistent pain and onset of loneliness remained even after controlling for marital status, which is a potential source of social connectedness. Research has found that married adults have lower levels of loneliness compared with other groups (Emerson & Jayawardhana, 2016; Pinquart, 2003). Our data show a similar significant association (those married in both years were negatively associated with onset of loneliness). However, our model also shows that even after controlling for marital status changes, pain was still significantly associated with onset of loneliness. Therefore, even those that might be considered less at risk for loneliness had a higher risk of loneliness if they had pain at both years. This is an important finding given the detrimental health and psychological effects of loneliness.
There are a number of potential explanations for this association. It may be that older adults with pain limit their social engagement outside the home due to the physical pain, preferring to remain less active in their home. While a natural strategy for pain is a reduction in activity, research shows that persistent pain may lead to a cycle of restriction and decreased participation (Jensen et al., 2011; Molton & Terrill, 2014). Despite being physically able to get out of the house, the discomfort and pain may be a significant barrier to social engagement. Some research suggests that older adults may limit social and physical activities in lieu of seeking pain treatment (Molton & Terrill, 2014). Therefore, persistent pain can include a decrease in social engagement and meaningful activities (Molton & Terrill, 2014; Parkinson, Gibson, Robinson, & Byles, 2010).
It may also be that pain medication produces side effects that could inhibit social engagement, such as lethargy or nausea. Opioids are commonly indicated for the management of chronic pain among older adults (Chau, Walker, Pai, & Cho, 2008), but these are often associated with serious side effects, including nausea, constipation, sedation, and mild cognitive impairment (Chau et al., 2008). Such side effects are likely to inhibit social engagement both in and outside the home. Memory lapse and concentration difficulty side effects may be particularly worrisome for older adults, who may already be worried about developing dementia (Mol, van Boxtel, Willems, & Jolles, 2006; Molton & Terrill, 2014). It is possible therefore that physical and mental pain medication side effects may curb social engagement of older adults.
It should be noted that these explanations are not mutually exclusive, and the associations between pain and incidence of loneliness are multifactorial. Furthermore, some older adults may respond to pain in ways that protect them from future loneliness. Research shows that those who use active pain adaptive strategies (e.g., handling the pain or carrying on functioning despite the pain) have lower depression, less functional impairment, and higher general self-efficacy (Bussing, Ostermann, Neugebauger, & Heusser, 2010). Future work exploring adaptive behavior as moderators of the pain/loneliness relationship could shed light on adaptive strategies of maintaining social functioning in the face of pain.
Strengths and Limitations
This study has a number of strengths, including the large sample of community-dwelling older adults and panel data. However, there were several limitations, and the results should be interpreted with caution. First, because of the selected sample, the results are not generalizable to the larger population of older adults. In addition, the measurement of pain across time has several limitations. The measure of pain itself was limited as a simple yes/no variable, not allowing for a more nuanced analysis of pain. Also, because we only have data at baseline and at follow-up, we were not able to capture any changes in pain in between the 4 years and hence could not examine any trajectories of pain. For example, persons that had two separate isolated incidences of pain in 2008 and 2012 were in the same category as someone who had pain throughout the entire 4 years. Therefore, pain at both times cannot be assumed as chronic pain. In addition, while we have a number of health conditions in the model, pain can be caused by numerous additional diseases, which we were not able to account for in the model. Likewise, loneliness in older adults could arise from multiple causes. Some older adults may be chronically lonely whereas others may experience new onset of loneliness because of recent events. Finally, our results only show an association between pain at both times with the onset of loneliness and do not show any causal effects. Further longitudinal research across multiple time points and using in-depth pain information is needed to examine causal effects of these variables.
Conclusion
The findings have implications for clinical practice and public health interventions. There are a number of pharmacological and nonpharmacological pain management options available. Intervening and managing pain early among older adults would not only ease physical discomfort but could prevent loneliness years later. Because loneliness is known to longitudinally predict pain (e.g., Jaremka et al., 2013), preventing pain from causing loneliness might be an important step in circumventing a negative cycle of pain and poor social outcomes.
Furthermore, members of the care team (including social workers, physicians, psychologists, and nurses) who see older patients with pain should also consider their psychosocial health outcomes, not only their physical outcomes. If a patient’s pain or pain medication appears to restrict their social engagement, it may be important to refer them to social engagement from other sources, including telephone calls, or in-home friendly visitor programs. Because the link is consistent even for those that may not be considered vulnerable for loneliness (e.g., married persons), it is important for health care providers to address loneliness even for older adults who appear to have social networks in place.
In addition to easing a potential source of suffering, the identification and targeting of interventions for pain may prevent future loneliness, which in turn could prevent functional decline, disability, and premature mortality. Therefore, identifying and intervening in both pain and loneliness is important for individual quality of life as well as for overall public health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.