
Abstract
The Seniors Centre Without Walls (SCWOW) program provides free social and educational programming for older adults via telephone. The target population for SCWOW is socially isolated older adults, a hard to reach population. The aim of this process evaluation was to examine whether SCWOW was reaching its target population and to gather participant feedback about program implementation and the perceived satisfaction and impact of the program. Telephone interviews were conducted with 26 participants (92% females; aged 57-85 years). Forty-two percent of the sample was socially isolated and more than half reported being lonely. Participants reported having no difficulty using the telephone system. On average, participants were very satisfied with the program and reported that SCWOW had several positive effects (e.g., connecting to the larger community, affecting mental well-being). Importantly, no barriers to participation were identified. The study suggests that telephone-based programs can successfully reach socially isolated older adults.
A large body of research has documented the negative effects that being socially isolated or lonely can have on older people’s health and general well-being (e.g., Cacioppo et al., 2002; House, Landis, & Umberson, 1988). There is also evidence that being lonely is associated with a greater likelihood of entering a nursing home (Russell, Cutrona, de la Mora, & Wallace, 1997). Research out of Manitoba, Canada, has shown that approximately 30% of Manitobans (aged 72+ years) identify themselves as being moderately to extremely lonely (Newall et al., 2009) and that being lonely or socially isolated has implications for older Manitoban’s health, physical activity, and even longevity (Havens & Hall, 1999; Newall, Chipperfield, Bailis, & Stewart, 2012).
Given the negative impact that social isolation and loneliness can have on older adults, it is not surprising that social participation and inclusion were identified as important indicators of age-friendly cities by the World Health Organization (WHO, 2007). According to WHO (2007), an age-friendly city is one where “policies, services and structures related to the physical and social environment are designed to support and enable older people to age actively” (p. 5). From this perspective, addressing the social problems of social isolation and loneliness can and should be done at the community level.
Offering programs and services targeting the socially isolated is important for improving the health outcomes of older adults and for potentially making communities more age-friendly. However, some of the characteristics that may predispose older people to become socially isolated or lonely (e.g., widowhood, low income, poor health, living alone, caregiving; e.g., Cloutier-Fisher & Kobayashi, 2009; Havens & Hall, 1999; Pinquart & Sorensen, 2001) may also make it difficult for individuals to partake in traditional social activities held in their community. A major question arises: How can services and programs reach the socially isolated? The present study evaluated a social and educational program offered in Manitoba, Canada, called Senior Centre Without Walls (SCWOW), specifically designed for socially isolated older adults.
Definition and Prevalence of Social Isolation and Loneliness
For the purpose of the present study, social isolation was defined as a lack or absence of meaningful social contact and opportunities (e.g., Scharf & de Jong Gierveld, 2008; Wenger & Burholt, 2004). However, of note, there is little consensus or consistency on how social isolation is measured or defined, making it problematic for researchers and practitioners to compare studies or identify/target the socially isolated (Sabir et al., 2009). Moreover, it is difficult to differentiate between the socially isolated who may benefit from outreach and those who prefer to be alone. Accordingly, assessing loneliness, a subjective feeling that the quantity/quality of one’s social relationships is insufficient (de Jong Gierveld, 1987), can provide important complementary information on people’s social relationships.
Notwithstanding the measurement issues, research suggests that a significant proportion of older adults are lonely and/or isolated. Approximately 20% to 40% of older adults report moderate to severe loneliness (e.g., Newall et al., 2009; Pinquart & Sorensen, 2001; Weeks, 1994; Wenger & Burholt, 2004), and it appears that prevalence rates for social isolation could be as high as 20% of older community-dwelling adults. Cloutier-Fisher and Kobayashi (2009) found that 17.5% of older Canadians (65+ years) were socially isolated. A recent study out of British Columbia, Canada, classified 17% of older adults (65+ years) as socially isolated based on a scale measuring relationships with relatives and friends (Kobayashi, Cloutier-Fisher, & Roth, 2009). Using this same scale on European samples, Lubben et al. (2006) found that 11% to 20% of older adults (65+ years) were socially isolated. This means that one out of five older people may be isolated from crucial social resources and support, making it particularly important to identify and provide appropriate programs or interventions for these individuals.
Addressing Social Isolation and Loneliness
A variety of approaches have been taken to address social isolation or loneliness in later life, including group or one-on-one interventions (for reviews, see Cattan, White, Bond, & Learmouth, 2005; Findlay, 2003; Hogan, Linden, & Najarian, 2002; Masi, Chen, Hawkley, & Cacioppo, 2011) and even interventions using the Internet (e.g., White et al., 1999). However, few studies have examined the use of the telephone as a way of reaching the socially isolated (Cattan, Kime, & Bagnall, 2011). It is possible that using the telephone to reach the socially isolated may be particularly effective, as the reasons older adults are isolated may create barriers to participating in face-to-face groups or social activities. Cattan et al. (2011) found that a telephone befriending service presented a low-cost way for older adults to increase their confidence and to be more socially active in general. For the present study, we had a unique opportunity to examine an ongoing social and educational telephone program that older people could access free of charge from their own homes.
Senior Centre Without Walls Program in Winnipeg, Manitoba
The SCWOW program was introduced in Winnipeg, Manitoba, in 2009 by the nonprofit organization, Age & Opportunity: Support Services for Older Adults. The social program was inspired by the SCWOW program developed out of San Francisco, California. Indeed, several such programs now exist worldwide, with Winnipeg’s being the first in Canada. SCWOW capitalizes on the idea that programming could be brought to people through something most people possess in their very own living rooms: a telephone. This low-technological concept is an alternative to having older people participate in programming at Senior Centres or other organizations. In this way, SCWOW is particularly suited for individuals who are socially isolated due to, for example, physical, financial, or geographical reasons.
The SCWOW program is open to anyone aged 55+ years living in Manitoba, a large prairie province in the center of Canada in which approximately 30% of seniors (65+ years) live in rural locations (Statistics Canada, 2006) and 70% live in urban centers, the largest being the province’s capital city Winnipeg (population approximately 650,000). Typically four times a year, Age & Opportunity releases a SCWOW program calendar offering 30+ social and educational sessions. The program offers a variety of daytime and evening sessions including one-time sessions (e.g., “Australian Tour,” “Nutrition and Healthy Aging,” “National Aboriginal Day”) and longer-term sessions (e.g., “Meditation Series,” “Brain Teasers,” “Education and Support Groups” for people with chronic lung disease and their caregivers, “Book Clubs,” “Coffee Talks”). Sessions are offered at specific times and are facilitated by invited guests, health professionals, or Age & Opportunity staff and volunteers. That is, individuals are linked on the telephone, calling in for particular sessions at a set time, with a session leader. Participants can register at any time of year for SCWOW via a toll-free telephone number, mail, or fax. At the time of registration, participants can choose to be called for their sessions, or they can call in using a toll-free number. This same number is used for all sessions. Packages are mailed to participants for many sessions to provide more tactile materials, such as scent samples for “Aromatherapy.”
The Present Study
The aim of the present project was to perform a process evaluation of SCWOW that would address questions surrounding the implementation of the program. This study was completed as part of a larger program of research on age friendliness in Manitoba, Canada (e.g., see Menec, Hutton, Newall, Nowicki, Spina, & Veselyuk, 2013. Menec, Means, Keating, Parkhurst, & Eales, 2011; Novek & Menec, 2013).
The specific objectives of the present study were as follows:
To examine who is participating and whether the SCWOW program is reaching its target population of isolated older adults.
To gather information from participants about the implementation of, satisfaction with, and perceived impact of the program.
Method
Procedure
This project was completed in collaboration with Age & Opportunity, Winnipeg. Ethical approval for the project was received from the University of Manitoba Bannatyne Campus Research Ethics Board (H2011:201). At the time of registration for SCWOW, people indicated whether they would be willing to have their name and telephone number given to a researcher from the University of Manitoba who would then contact them for their feedback. An interview schedule containing both closed- and open-ended questions was used to collect information from participants via telephone.
Participants
All individuals taking part in SCWOW for the May to September 2011 and October to December 2011 sessions were eligible (N = 62). Telephone interviews were conducted with participants near the end of each 4-month term. Twenty-nine people were willing to be contacted by a researcher, and 26 interviews were completed (two later refused; one was unavailable).
Measures
Sociodemographic variables
Sociodemographic information was gathered on age (in years), gender, marital status, housing, living arrangements (living alone or with others), location of residence (urban, rural), education level, and perceived income adequacy.
Health and limitations
Participants’ perceived general health was assessed (excellent to poor), and they were asked whether they had a serious health problem (yes/no). Participants were asked whether they were limited in what they would like to do by their health, income, or residence location (yes/no).
Loneliness
Participants were asked, “if we divide people into four categories where ‘1’ is the not lonely, ‘2’ is the moderately lonely, ‘3’ is the severely lonely, and ‘4’ is the extremely lonely, what do you consider yourself to be?”
Social isolation and meaningful social contact
Participants were asked an open-ended question: “Sometimes people can feel isolated because they do not have as many opportunities to socialize or to do fun activities as they would like. Do you feel isolated at all? If yes, how come?” Participants were also asked about their meaningful social contact (source, frequency, satisfaction).
Program feedback: Quantitative questions
Participants were asked about their overall satisfaction with the program (1 = not at all satisfied to 5 = extremely satisfied) and whether they agreed or disagreed with statements about SCWOW (e.g., I found pleasure and enjoyment in participating in the groups; I would recommend this program to others). Note that these questions were modified from the San Francisco (California) SCWOW evaluation form.
Program feedback: Qualitative questions
Table 1 shows the questions asked of participants that were designed to tap into (a) access/barriers, (b) satisfaction with the program, and (c) impact of the program.
Listing of Open-Ended Questions.

Analysis of Qualitative Data
The interviews were completed by the first author, who wrote down participant responses verbatim. Responses were analyzed for common themes by the first author. For the questions requiring more straightforward answers such as “how did you hear about the program” or “how come participant missed a session,” responses were simply grouped based on similarity (e.g., missed a session due to a conflicting appointment) and then tallied to determine the most common responses. For the more open-ended questions, for example, the two questions tapping into the impact of the program, the first author reviewed the responses for each question and identified keywords (e.g., “making friends,” “connecting with others”). Next, the different keywords were grouped based on common underlying themes and a label was created (e.g., “feeling more connected”).
Results
Participant Characteristics
On average, participants had been taking part in SCWOW for two terms. The average age of the participants was 71 years (range 57-85 years). Twenty-four (92.3%) participants were women. Marital status varied with 31% widowed, 27% divorced, 23% married, and 19% single. About 73% of the participants lived in Winnipeg, and 27% lived in rural Manitoba. Most participants (73.1%) lived alone. About 38% of the participants had some high school education or had completed high school, whereas the remaining 61.5% had some university or a university degree. On average, participants reported that their income met their needs “with difficulty.” Last, although people generally reported having “good” health, most people (69%) had at least one health problem that they considered serious (e.g., hip problems, eyesight loss).
Identifying the Socially Isolated
To identify the socially isolated, participants were asked directly whether they felt isolated and, if applicable, the reason that they were isolated. If people gave either a firm “yes” or “no” response, they were categorized accordingly as isolated (n = 8) or not (n = 9), respectively. For the nine participants who gave less clear responses (“not really,” “depends,” etc.), those who indicated having daily meaningful social contact (n = 6), were categorized as not isolated. The remaining three people who did not have daily social contact were categorized as isolated. Based on these criteria, 42.3% (11/26) were socially isolated.
Limitations due to Health, Income, or Residence Location
People may be socially isolated for a variety of reasons. We examined limitations in health, income, and residence location. The majority of the participants reported being limited (and some even housebound) because of their health (81% of participants). They were also limited by their income (64% of the participants), followed by where they lived (46%). In examining these limitations further, we found that compared with the not isolated, the isolated participants were much more limited in what they could do (Table 2). For example, all the isolated individuals were limited by their health and 81% by their income. Compared with 33% of not isolated, 63% of the socially isolated participants were limited by where they lived. In sum, the socially isolated participants were more limited by their health, income, and residence location.
Characteristics of Isolated Versus Not Isolated Participants.
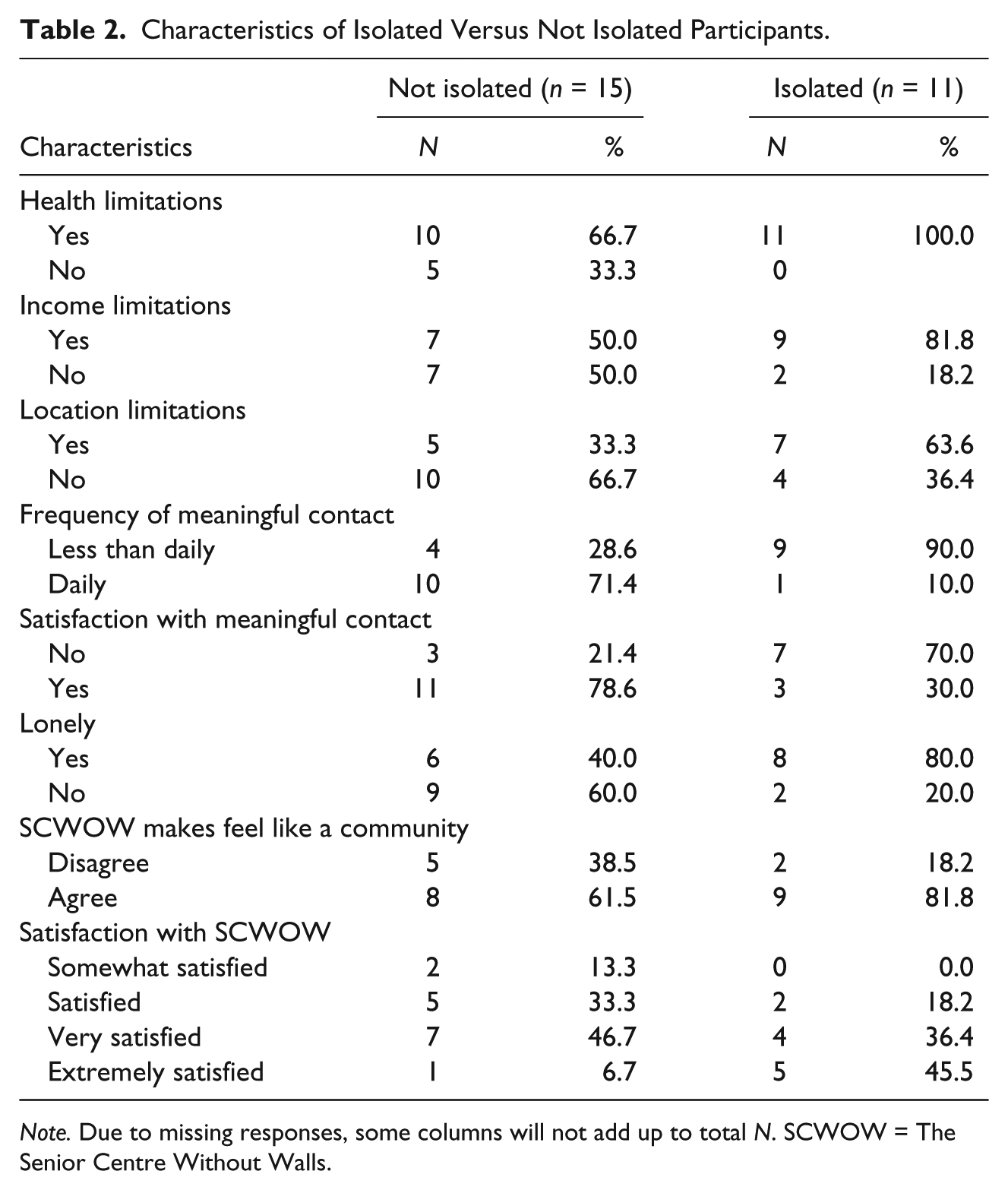
Note. Due to missing responses, some columns will not add up to total N. SCWOW = The Senior Centre Without Walls.
Social Contact and Loneliness
When participants were asked where they get the most meaningful social contact with people in their daily life, about half mentioned their spouses, families, and friends (12/26; 46%), and others mentioned sources such as church, coffee shop, and Seniors Centre. SCWOW was also mentioned as a main source of meaningful social contact by some. Comparing the isolated and not isolated (Table 2), 29% of the not isolated had less than daily meaningful social contact, whereas 90% of the isolated did. Similarly, 79% of the not isolated were satisfied with their amount of social contact, whereas, 30% of the isolated were satisfied.
In terms of loneliness, we found that for the full sample, 56% of the participants were lonely. Moreover, we found that 80% of the isolated participants were lonely, compared with 40% of the not isolated who were lonely (Table 2). In sum, not surprisingly, the socially isolated participants reported having less meaningful social contacts and being more lonely.
Program Feedback: Quantitative Data
All participants agreed that they would recommend this program to others, and most enjoyed the groups and activities and planned to continue with the program in the future (Table 3). Thus, people were overall “very satisfied” with the program (M = 3.8). Participants were less in unison on whether they thought that SCWOW helped them to feel as if they were part of a community, with about 70% agreeing with this statement.
Responses to Feedback Question Statements.

Note. SCWOW = The Senior Centre Without Walls.
We examined these last two questions on satisfaction and community more thoroughly by comparing the responses of the isolated with the not isolated (Table 2). As shown in the table, 82% of the socially isolated agreed that SCWOW helped them feel as if they were part of a community, compared with 62% of the not isolated. The isolated were more satisfied with the SCWOW program, as 82% were either very or extremely satisfied with the program, compared with 53% of the not isolated.
Program Feedback: Qualitative Data
The following section provides details about participant responses to open-ended questions that were designed to tap into (a) access/barriers, (b) satisfaction/dissatisfaction, and (c) perceived impact of SCWOW.
Access and barriers
Part of accessing programs is hearing about them in the first place. Participants most commonly heard about the SCWOW program via Age & Opportunity (brochure, poster, representative visiting a community group), followed by newspapers, newsletters, and Seniors Centres. Four people heard about the program through a health professional (e.g., social worker, mental health), which would seem to be a promising entry point into social programs for the socially isolated.
Participants reported little to no barriers in terms of accessing SCWOW. For example, people reported that the telephone system was easy to use and that they appreciated how the call-in number was the same for all the programs. Indeed, the majority of participants indicated that there was nothing at all that made participating in SCWOW difficult. If people registered and missed a session, it was due primarily to scheduling conflicts. In this vein, some people wished that there were more evening sessions when they had no appointments.
Of note, the most common reason for participating in SCWOW was because participants could access the programming from their home. Therefore, being able to access programming from home, using an easy-to-use technology, might break down many of the more common barriers to participation such transportation, cost of programs, or health problems.
Although accessing SCWOW appeared to pose no difficulty, several people did report barriers in being an active participant on the telephone. Participants noted problems with people monopolizing the conversation, not knowing whether you have been heard on the telephone, and difficulties keeping people focused on the topic. These problems are illustrated by the following comments:
Sometimes we get out of focus. People just talk about themselves. There needs to be some housekeeping rules. (Female, aged 58 years) The lapses in phone conversations was hard. There were delays. Sometimes you did not know if [the facilitator] heard you. I didn’t want to interrupt. [The facilitator] did a good job considering the number of people on the phone though, overall. (Female, aged 63 years)
Satisfaction with program
As highlighted by the following comments, overall, people were satisfied with the program content, with some noting that they especially appreciated the staff and facilitators:
Facilitators are fantastic. They are always in a good mood (which is not easy). (Female, aged 60 years) I enjoy the content. I especially like the travel ones, though I have missed a few. I was able to get a code for listening later in the evening though. (Female, aged 77 years)
Not everyone was satisfied with the program, however. Participants who were less satisfied with the content seemed to find that the program did not suit their needs or interests, as illustrated by the following comments:
I think the program was great. Not all of it was my cup of tea though. (Female, aged 63 years) I am needing to be active and so being on the telephone just doesn’t do it for me. (Female, age 69)
Perceived impact
There were several subthemes that emerged surrounding the perceived impact of the program as follows: feeling more connected, impact on mental well-being, something to look forward to, and increases knowledge.
Feeling more connected
Several participants noted not being able to take part in many activities outside of their homes because of health problems or living in a remote location. Therefore, an important aspect of the program was that it made them feel more connected to other people and the outside world. The formation of friendships was a common theme, as people appreciated making friends over the phone, and discovering that they had things in common with others. On the flip side, participants appreciated getting to know others in different circumstances, as some reported that they had learned more about what it is like to have different problems or to be homebound, and felt relief knowing that SCWOW existed if/when they were to become less mobile themselves. The following comments highlight some of these feelings of connection:
It makes me more connected with the outside world. We have a wonderful lunch in the apartment but I can’t go downstairs anymore. I can’t sit for any length of time. The [SCWOW] program is an added boon to be able to converse with more than one person. I can’t get dressed sometimes, but I can sit and be comfortable for the programming. (Female, aged 76 years) Main thing is you feel more connected. And I find I have things in common with people. There are some people who are not mobile who really get a lot out of it. It is good to know that if I ended up in the same position [not mobile] that there is something there. (Female, aged 66 years) I am happy I joined. When I became widowed I realized I was sheltered. Makes you feel good to have a friendly voice all the time on the line! It makes you realize that we’re all in the same boat. It is nice to be able to talk. And you become friends. (Female, aged 70 years)
Impact on mental well-being
Participants specifically brought up the impact of SCWOW on their mental well-being, mentioning that SCWOW helped them feel less lonely, feel happier, and deal better with their depression. It appears that having the option to participate in a session when they want to and need to, and having something to look forward to, helped with people’s mental well-being. These ideas are illustrated by the following comments:
I like the conversations, the interactions, with thoughts. I don’t quite feel so lonely because I can pick up the phone and have friends in my living room! (Female, aged 76 years) I suffer from depression, and the program made it easier to deal with. If I have a bad day, I will have an interesting day to look forward to. It has helped a lot! (Female, aged 60 years)
Something to look forward to
Participants valued SCWOW for giving them something to look forward to and to help provide structure or purpose to their day. One person noted that they received few visits and, therefore, especially appreciated looking forward to a call from SCWOW:
When you [have my health condition], a lot of people don’t want to come the way they used to. When you know you’re getting a call, that’s something to look forward to. (Female, aged 85 years) It gives you something to look forward to. It is better for a person to have a schedule, you know, a shape and a form to your day. (Female, aged 76 years)
Increases knowledge
Participants simply appreciated the knowledge gained through SCWOW, for example, on a new language, or on different cultures and events. Learning about health issues such as arthritis was also appreciated. Several participants felt that SCWOW helped open their minds or develop new interests, as illustrated here:
It’s given me more broader things to think about. I really liked the [Folk Festival] pavilions. You read over the materials and then I had questions in my mind already. I had lots of questions and they [facilitators] were good at answering the questions. It opens up your mind. (Female, aged 63 years)
Discussion
In the present study, we gathered sociodemographic and health information on participants of the SCWOW program and obtained feedback on the programming in terms of satisfaction, barriers to participating, and personal impact of the program. The study is important as it provided an opportunity for older participants themselves to voice their feedback on a rather unique program offering social and educational opportunities over telephone. The study also allowed an examination of whether the program was reaching its target population of socially isolated adults, and whether the program was being delivered in a way appropriate to the needs of this group, with little barriers.
Reaching the Socially Isolated
A main research question was whether SCWOW was reaching the socially isolated. Studies indicate that approximately 17% to 20% of older adults aged 65+ years are socially isolated (Cloutier-Fisher & Kobayashi, 2009; Kobayashi et al., 2009; Lubben et al., 2006). In comparison, we found that 42% of the SCWOW sample was isolated. Thus, it appears that Age & Opportunity’s SCWOW program is successfully reaching socially isolated older adults. Moreover, we found that the socially isolated were particularly limited by their health, income, and residence location and that most were lonely and had unsatisfactory social contact. Taken together, these are important findings as they suggest that it is not simply the more “socially engaged” older person who is also engaging in SCWOW but rather people who may not be able to access other programs due to health, income, or geographic limitations.
Removing Barriers and Providing Opportunities for Choice
Another aim of this study was to examine barriers to participating in SCWOW. First, people reported having no major difficulty using the telephone system. Second, it was revealing that no major barriers were mentioned by the participants. Perhaps this is because there were no cost barriers and transportation was not an issue because it is offered out of people’s own homes. Indeed, the participants reported that an important aspect of why they joined SCWOW was because it was accessible from their homes. Having the programming offered from home, with a variety of content, and times of day also provides participants with an incredible amount of choice and personal control over their own participation in SCWOW. This aspect of enhancing opportunities for control or self-efficacy over their participation and social contact could do much to improve the well-being of socially isolated participants (e.g., Baltes & Baltes, 1990; Schulz & Heckhausen, 1996) and may transfer to other parts of people’s lives (e.g., Cattan et al., 2011). Interestingly, simply knowing that SCWOW was available appeared to provide some of the “not isolated” respondents a sense of relief because SCWOW would be there if they were to become isolated or less mobile. This suggests that SCWOW could serve as a tool to prevent social isolation or loneliness, a form of primary prevention (Uchino, 2009). In sum, the fact that it is flexible, free, offered from home, and via telephone are all important and unique aspects of the SCWOW program. SCWOW appears to be filling a gap by providing people with a way to be connected and take advantage of social and educational programs when and if they want to, and regardless of where they live, how poor their health is, and whether they have a high or low level of income.
Next Steps
The quantitative and qualitative results from this study point to some areas that could be focused on in the future. For example, “younger” older adults were not well represented in our study, as only 12% of the sample was below 60 years. Therefore, it is unclear whether these “younger” older adults would have different feedback. In addition, men were not well represented in our sample; however, this seems to reflect the fact that there are, by far, more women participating in the program than men (Age & Opportunity Program Manager, personal communication, July 27, 2012). Therefore, it seems that more specific targeting will need to be done to identify men who may be isolated and living in the community. This is a particularly important issue as males may be particularly at risk for loneliness, especially those living alone (e.g., Greenfield & Russell, 2011). It is possible that men would respond better to particular activities/programs or that the over-the-telephone nature of the program is not as suitable for men. This all remains speculation, however, as the results of this study do not provide sufficient insights, and, in general, the research literature on older men and participation in social programs is scarce (Reynolds, 2011).
Developing programming designed to facilitate friendship formations might also be of value, as more than half the sample was lonely. Some participants requested more (or longer) coffee talk social sessions offered at different days and times. Offering more social programming (such as coffee talk) might help foster a sense of community. On this note, it should be stated that telephone communication is not necessarily a substitute for face-to-face interaction. Cattan et al. (2011), for example, found that participants of a telephone befriending service wanted to meet their “befriender” to put a face to their name. In other words, SCWOW should not be seen as a replacement for important programming that includes transportation to and from Senior Centres, for example. Rather, there ideally should be a variety of social programming options that suit different needs.
Finally, it was sometimes difficult for people to be an active participant over phone because of, for example, individuals monopolizing the conversation. This can be a challenge to any group setting; however, given the lack of visual cues over the telephone, it may be even more challenging. Moreover, as the program becomes more popular, with greater numbers, this will no doubt be an issue that will need to be continually addressed.
Satisfaction With Program and Potential Impact
An important consideration of this study was whether people were satisfied with the program and what impact it had on the participants. In general, participants of SCWOW were satisfied with the program, and this was even more apparent when we examined only the socially isolated. In addition, compared with the “not isolated,” the socially isolated tended to report that SCWOW made them feel as if they were part of a community. As it is a difficult feat to create a sense of community, this seems a promising finding.
An important finding was that participants reported that SCWOW had a positive impact on their mental well-being in terms of helping with their loneliness and depression. In addition, SCWOW made people feel more connected to the outside world and to other people. By providing opportunities for older people to interact with others (whether they choose to take advantage of these opportunities or not), the SCWOW program is helping to create a more age-friendly community. Moreover, given that the nonprofit organization Age & Opportunity provides other services, SCWOW is linking people not only with other participants but also with the larger support system as well.
Limitations
Our study design precludes us from making causal conclusions about the impact of SCWOW. To move toward making these sorts of conclusions would have required that we restrict who participated in the program to create a control and intervention group and ideally assess participants’ social isolation pre- and post-participation. Given that SCWOW was designed to be as open and accessible to all, restricting participation was not a viable route to take for this study. To try to get a sense of the potential impact of the program, we simply asked participants their thoughts. Of course, a limitation of our study is that we do not have information on the non-responders in terms of their satisfaction with the program. It is not known whether those who are satisfied with the program were particularly apt to participate in this study. In addition, another limitation was the small sample size for the current study. Having a larger sample would have helped to increase confidence in the generalizability of research findings. Another limitation was the use of a self-reported measure of social isolation. It would have been more ideal to have responses from an objective social isolation scale so that results could be directly compared with other larger studies. Directly asking about social isolation and allowing participants to reveal reasons for social isolation did allow us, however, to perhaps capture some of the nuances of isolation. For example, in one case, follow-up questions revealed that although the respondent lived with others, she or he was basically alone and housebound during most of the day. As another example, someone who reported being isolated but also had daily contact was referring to daily visits by a home care worker.
To conclude, MacCourt (2007) discussed key features that should to be taken into account when designing programs for older adults, including the need to deliver services in ways that are appropriate to the needs of the target group. In this respect, a program such as SCWOW may be on the right track.
Footnotes
Acknowledgements
We would like to thank Michelle Ranville, Program Manager, Age & Opportunity, for her assistance on this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Canadian Institutes of Health Research (CIHR) Post-Doctoral Award in the area of Longitudinal Study on Aging to the first author; and a Social Sciences and Humanities Research Council of Canada (SSHRC) Community University Research Alliance grant (no. 833-2007-1013) to the second author. V. Menec holds a Canada Research Chair in Healthy Aging.