
Abstract
The extent to which a museum object-handling intervention enhanced older adult well-being across three health care settings was examined. The program aimed to determine whether therapeutic benefits could be measured objectively using clinical scales. Facilitator-led, 30 to 40 min sessions handling and discussing museum objects were conducted in acute and elderly care (11 one-to-ones), residential (4 one-to-ones and 1 group of five), and psychiatric (4 groups of five) settings. Pre–post measures of psychological well-being (Positive Affect and Negative Affect Schedule) and subjective wellness and happiness (Visual Analogue Scales) were compared. Positive affect and wellness increased significantly in acute and elderly and residential care though not psychiatric care whereas negative affect decreased and happiness increased in all settings. Examination of audio recordings revealed enhanced confidence, social interaction, and learning. The program allowed adults access to a museum activity who by virtue of age and ill health would not otherwise have engaged with museum objects.
Introduction
The Health and Social Care Act (Department of Health, 2012) introduced major reforms to U.K. health and social care delivery advocating preventive, multiagency approaches. Reforms were prompted by pressures on health care services from an aging population showing increases in age- and lifestyle-related diseases (e.g., dementia and diabetes) with poorer socioeconomic communities experiencing higher mortality and morbidity rates (Marmot, Ryff, Bumpass, Shipley, & Marks, 1998). Museums (including galleries) as community resources are well-positioned to promote cognitive and physical activity in nontraditional audiences (Camic & Chatterjee, 2013). Although museums have sufficient means to embrace individual and societal well-being, their contribution should be supported by appropriate research to quantify the therapeutic impact of museum-focused interventions (Chatterjee & Noble, 2013).
A review and trial of clinical scales of well-being, quality of life (QoL), and health status (Thomson, Ander, Menon, Lanceley, & Chatterjee, 2011) found that optimum measures for museum-focused health care interventions were the Positive Affect and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988) and Visual Analogue Scale (VAS; EuroQol Group, 1990). A comparison of handling and discussing museum objects versus discussing photographs found pre–post PANAS and VAS improvements for the tactile intervention (Thomson, Ander, Menon, Lanceley, & Chatterjee, 2012). Research with female participants receiving cancer care demonstrated enhanced well-being for tactile over visual interventions using the same measures (Thomson, Ander, Lanceley, Menon, & Chatterjee, 2012).
Reviews of arts-in-health interventions (Staricoff, 2004, 2006) indicate positive therapeutic and medical outcomes, including reduced stress, anxiety, depression, and blood pressure. Similarly, museum interventions aim to improve patients’ well-being and QoL, widening access to arts and culture (Chatterjee & Noble, 2009; Chatterjee, Vreeland, & Noble, 2009). A museum intervention for people with mild-to-moderate dementia (Camic, Tischler, & Pearman, 2014) comprising art-viewing-art-making sessions used three pre–post measures: Dementia QoL (Smith et al., 2005), Zarit Burden Interview (Zarit, Reever, & Bach-Peterson, 1980), and Bristol Activities of Daily Living Scale (Bucks, Ashworth, Wilcock, & Siegfred, 1996). Results showed nonsignificant pre–post differences probably due to small samples (n = 13 participant–caregiver pairs) though thematic analysis found self-reported cognitive capacity and social inclusion increases. A gallery intervention for people with mild-to-moderate dementia (Eeckelaar, Camic, & Springham, 2012) exploring art-viewing-art-making on pre–post cognitive measures showed enhanced episodic memory but inconclusive findings for verbal fluency. Thematic analysis of audio recordings from museum object-handling sessions determining features contributing to well-being (Ander et al., 2013; Paddon, Thomson, Menon, Lanceley, & Chatterjee, 2013) implicated novel thinking and meaning-making, increased vitality, sense of identity, and enhanced social skills.
Unlike health-related QoL measures linked to medical outcomes, well-being focuses on positive aspects of mood and cognition (Hird, 2003), is typically self-reported, and connects to positive psychology (Seligman, 2002). The Health Education Authority (1997, p. 49) defines well-being as “emotional and spiritual resilience,” and Keyes (2002, p. 210) describes high levels of well-being, positive emotion, and psychological functioning as “flourishing.” A contentious issue in well-being measurement is the interdependency of constructs such as wellness, happiness, and QoL. Hird (2003) differentiates objective well-being related to material and social circumstances from subjective well-being based on individual self-assessment and further split into hedonic and eudemonic well-being. Hedonic, associated with happiness, implies interdependency of life satisfaction and positive mood whereas eudemonic, related to realization of potential, advocates independency of happiness and well-being.
The current research aimed to evaluate museum interventions for older adults in differing health care settings using subjective well-being measures (PANAS and VAS). The study advanced research by making comparisons of acute and elderly and residential care with psychiatric care, a setting not previously measured in museum interventions. It was hypothesized that pre–post comparisons would demonstrate enhanced well-being (increase in positive emotion, wellness and happiness; decrease in negative emotion) across settings.
Method
Design
A mixed, pre–post design with repeated-measures factors of score (pre- and postsession) and between participant factors of setting (acute and elderly, psychiatric or residential) was employed. Self-report measures comprised PANAS (10 positive and 10 negative emotions rated from 1 “not at all” to 5 “extremely”) and VAS (vertical scales rated from 0 “unwell”/“unhappy” to 100 “well”/“happy”). Incomplete data sets were omitted. Mauchley’s sphericity test showed data violated ANOVA assumptions so one-tailed, mixed test by setting (2 × 3) MANOVA with Wilks’s λ F value adjustment was used. Simple effects were examined using planned, one-tailed t tests. Proportion of variance was estimated by
Participants
Participants (n = 40) were older adults (65-85 years) in three health care settings: Central London hospital acute and elderly care with chronic conditions (n = 11; 2 males, 9 females); two regional hospital psychiatric wards with clinical anxiety and depression (n = 20; 5 males, 15 females); and north London residential nursing home (n = 9; 4 males, 5 females). Participants gave their own consent and none had a diagnosis of dementia. Though more females than males participated, the gender imbalance was similar to health care setting ratios.
Materials/Apparatus
Museum objects comprising archaeological artifacts (amulets, flint tools, pottery), artwork (engraving plates, prints), geology samples (fossils, rocks, minerals), and zoology specimens (horns, shells, teeth) were selected from university collections on the basis of visual, tactile, and kinaesthetic properties. Objects were compiled into six boxes of six in conservation materials with fact sheets. Project information leaflets consent forms and measures were printed on A4 (210 mm × 297 mm) paper. Digital audio recorders were used when consent was given for recording.
Procedure
Sessions were conducted one-to-one for acute and elderly care, in small groups for psychiatric care, and using both methods in residential care depending on individual preference and staff availability. Both female facilitators (postdoctoral psychologist and postgraduate museum professional) received health and safety training (infection control from London hospital and object handling from university museum) and obtained Disclosure and Barring Service (DBS) clearance. Participants read information leaflets, signed consent forms, washed hands (soap or alcohol gel), and completed presession measures. Sessions lasting 30 to 40 min comprised semistructured interviews (see the appendix) featuring sensory and emotional aspects of objects (e.g., “What does it feel like?”; “How does it make you feel?”). Participants completed postsession measures and rewashed hands.
Results
PANAS and VAS pre–post mean differences for pooled settings (Table 1) showed increases in positive PANAS (13%), wellness VAS (9%), and happiness VAS (14%) and a decrease in negative PANAS (16%). MANOVAs (Table 2) showed highly significant main effects of test for all measures and an interaction of test by setting for positive PANAS.
Pre–Post Means, Standard Deviations (SD), and Mean Differences for Pooled Settings.
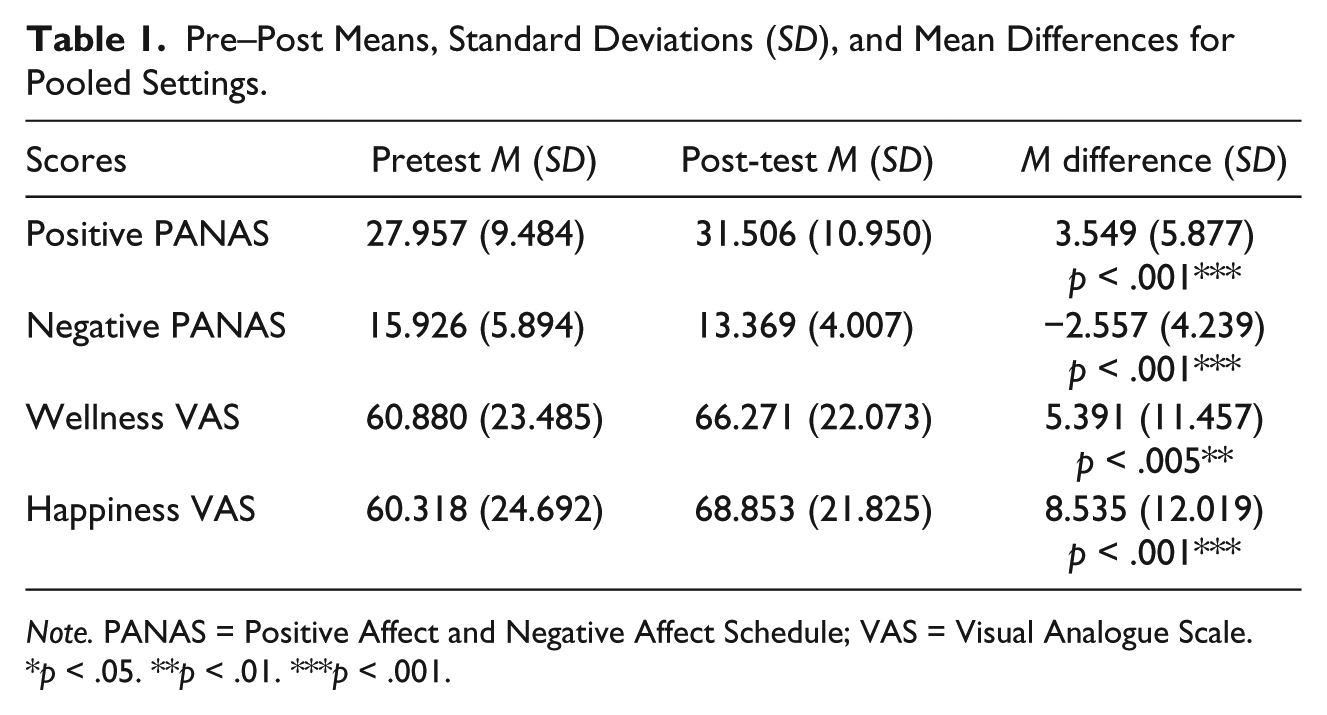
Note. PANAS = Positive Affect and Negative Affect Schedule; VAS = Visual Analogue Scale.
p < .05. **p < .01. ***p < .001.
F Value, Probability, and MS Error for Main Effects and Interactions.
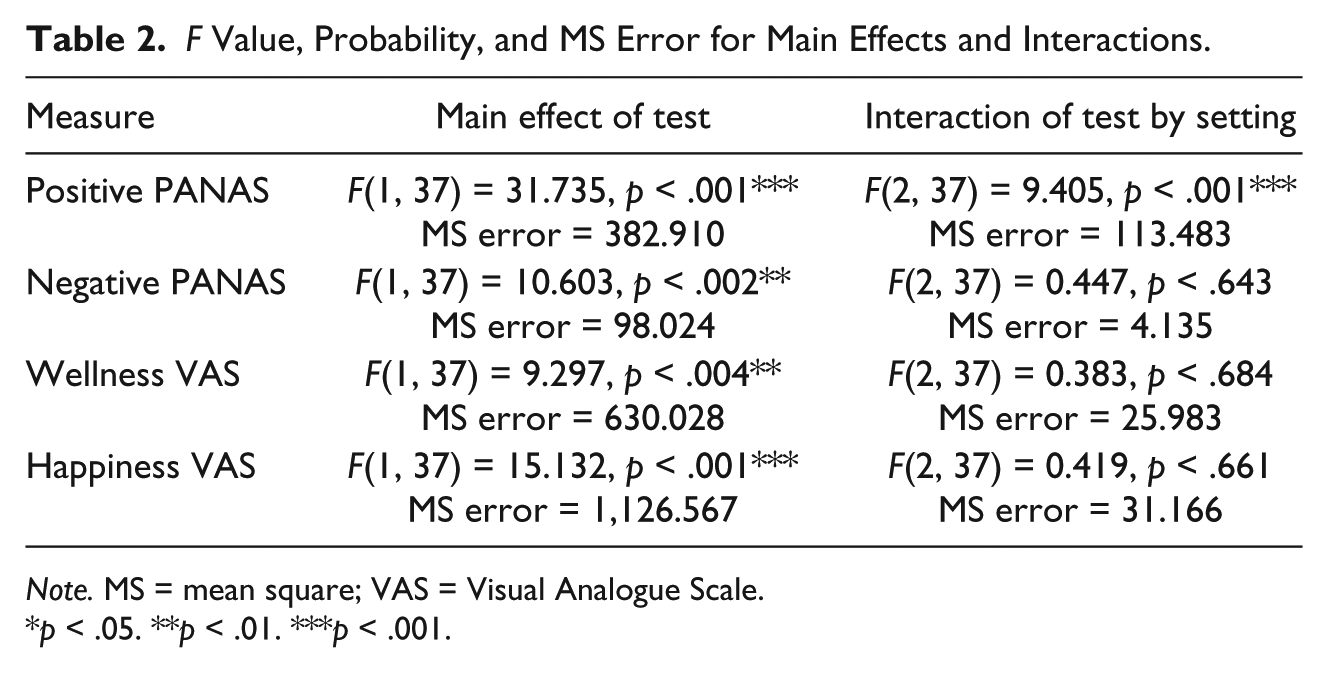
Note. MS = mean square; VAS = Visual Analogue Scale.
p < .05. **p < .01. ***p < .001.

Note. PANAS = Positive Affect and Negative Affect Schedule; VAS = Visual Analogue Scale.
Pre–Post Mean Differences.
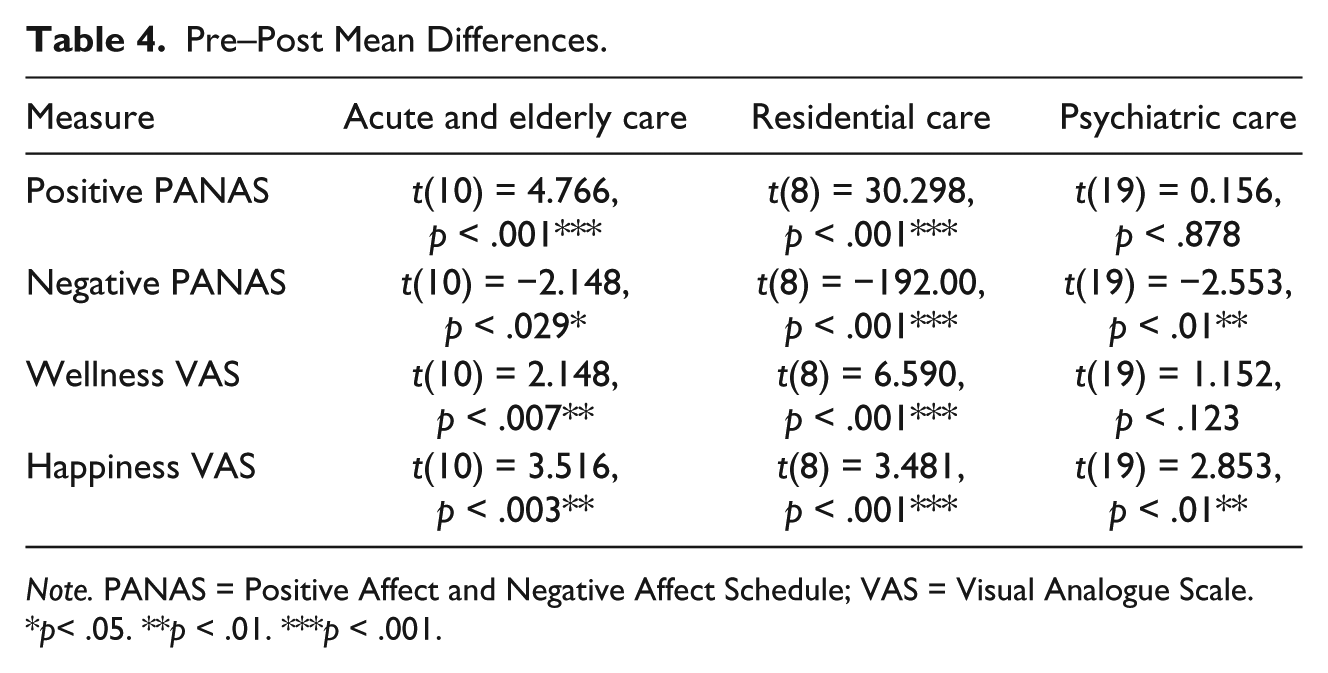
Note. PANAS = Positive Affect and Negative Affect Schedule; VAS = Visual Analogue Scale.
p< .05. **p < .01. ***p < .001.

Pre–post means (error bars ±1 SD) for health care settings.
Discussion
Object-handling sessions were successful in measuring well-being using clinical scales. Inferential tests showed that positive PANAS, wellness VAS, and happiness VAS increased, and negative PANAS decreased in acute and elderly and residential care but found no differences in positive PANAS and wellness VAS in psychiatric care. For acute and elderly and residential care, increases in positive PANAS were larger than decreases in negative PANAS. Psychiatric participants showed the largest reduction in negative PANAS, moderate gains in VAS wellness, and greater gains in VAS happiness. A qualitative study of psychiatric care (Ander et al., 2013) reported museum sessions gave depressive or anxious participants an additional focus to wondering about their discharge date, a finding that could account for increase in happiness but not lack of improvement in positive well-being so alternatively, duration of stay was explored.
Acute and elderly participants experienced the shortest stay (3-5 days) though some remained on the ward for 6 weeks waiting for residential assessment. Although psychiatric participants experienced a longer stay (12 weeks) that might explain low presession well-being, residential participants would most likely remain in care until the end of their lives, though possibly regarded the care home as their own home as they had their possessions about them. As duration could not account conclusively for poor psychiatric well-being, audio was analyzed. Thematic analysis revealed potential reasons why acute and elderly care settings showed well-being improvements; participants asked questions, engaged in meaningful conversation, held amulets they wanted to “keep,” and spontaneously commented on the value of object handling. One participant said she was feeling anxious in hospital, unable to concentrate on television or books but felt better looking at interesting objects. Another with a poor prognosis said the session took her mind off the bad news, helping her not to get immersed in it.
Responses to object handling from psychiatric participants elicited curiosity; most found objects fascinating but expressed dissatisfaction with the system. Participants with improving health commented on how seeing things so old helped them come out of themselves and interact with the world again. Although postsession positive PANAS measures remained similar, negative PANAS decreased more than in other settings. It was plausible that as negative emotions were plentiful given the mental health diagnosis, there was greater scope for reduction, though this explanation proved inconclusive as presession measures showed only marginally greater negative emotion for psychiatric than acute and elderly care. It was likely that several severely depressed participants, who the therapist thought would benefit from joining in, experienced a larger drop in negative emotion reducing the group average.
Residential participants showed improvements in well-being and happiness but were apathetic about objects; if persuaded to hold them they handed them back after a few seconds and comments were initiated by staff. Lack of interest was attributed to the fact that many had never visited a museum or had done so once on a school trip. Participants preferred to read fact sheets and look at pictures demonstrating curiosity but limiting conversation. Group sessions were held to encourage sociability but after realizing they required support by as many staff as participants, one-to-ones were conducted instead. Although these engendered conversation, focus was an issue; residents deviated to reminiscence (e.g., being a Land Girl, meeting the Queen) or daily routine (e.g., teatime, visitors). Staff advised that residents preferred soft colorful textiles and a passive role in activities (e.g., listening to a story). Textiles were not used for sessions because of risks to infection control. Furthermore, the protocol was developed to promote shared exploration not story-tell.
Limitations
Findings of the study should be regarded with caution due to the small sample size, short intervention exposure, lack of control group, and mix of one-to-one and group sessions. Regarding the lack of control group, permission for research was given on the basis that participants would experience a museum session; therefore, there was no “life-as-usual” condition making it unclear whether differences were due to the intervention or other factors such as increased social interaction or attention. Control groups would add considerable rigor to a quasiexperimental study of this sort, and it is recommended that future studies conduct randomized controlled trials where participants experience a museum-related intervention or life-as-usual so that comparisons can be made. Further recommendations include the consistent use of one-to-one or group methods and carrying out a series of sessions over a longer time span.
Conclusion
The research objective was to conduct museum object handling with older adults in differing health care settings and measure therapeutic benefits using valid and reliable clinical scales. Previous quantitative research into museum interventions found well-being improvements in acute and elderly (Thomson, Ander, Lanceley, et al., 2012) and residential care (Thomson, Ander, Menon, et al., 2012), but participants from psychiatric care were not included in the studies. The current study compared older adults receiving psychiatric care with those in acute and elderly and residential settings. Findings showed increased positive emotion and wellness for acute and elderly and residential though not psychiatric care and increased happiness and decreased negative emotion for all settings. Participants were not diagnosed with dementia as in the Camic et al. (2014) and Eeckelaar et al. (2012) studies but analysis of audio recordings implied similar cognitive gains of enhanced confidence, social interaction, and learning. The study allowed people who would not otherwise have engaged with museums to benefit from access to museum objects albeit the intervention only measured short-term gain. It is recommended that a longitudinal study taking measures over several weeks is conducted within a randomized controlled trial to endorse the current findings.
Footnotes
Appendix
Acknowledgements
The research was conducted with the support and advice of the hospital arts curator and hospital and health care staff.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The AHRC is a non-departmental public body sponsored by the Department for Business, Innovation and Skills, along with the other U.K. Research Councils. The AHRC is governed by its Council, which is responsible for its overall strategic direction, and is incorporated by Royal Charter. Dr. Helen Chatterjee was the principal investigator and Dr. Linda Thomson was lead research associate on the AHRC-funded “Heritage in Hospitals” research project. Both authors are full-time employees of University College London.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Arts and Humanities Research Council (Award No: AH/G000506/1; Heritage in Hospitals).