
Abstract
Introduction
Today, one in three Americans is obese (defined as a body mass index [BMI] ≥ 30) leading to very high annual obesity-related medical spending (Finkelstein, Fiebelkorn, & Wang, 2003; Finkelstein, Ruhm, & Kosa, 2005; Flegal, Carroll, Ogden, & Curtin, 2010; National Heart Lung Blood Institute, 1998). Obesity takes a significant toll on individuals and the health care delivery system. Obese patients are hospitalized longer (El-Solh, Sikka, Bozkanat, Jaafar, & Davies, 2001; Hauck & Hollingsworth, 2010; Schafer & Ferraro, 2007) and experience more medical complications than non-obese patients (Craft, May, Dorigo, Hoy, & Plant, 1996; Williamson, Webb, Szekely, Gillies, & Dreosti, 1993). Obese patients also placed greater demands on staff (Rose, Baker, Drake, Engelke, & McAuliffe, 2007). Recent evidence is also indicating that morbid obesity of patients is making it difficult for hospital staff to locate skilled nursing facility placements for these patients after leaving the hospital (Miles et al., 2012).
The care challenges experienced by morbidly obese patients in the hospital settings most likely persists in other settings, such as nursing homes (NHs) and/or private homes (Miles et al., 2012). Emerging research indicates that newly admitted NH residents who are obese require significantly more personal assistance than their non-obese peers (Felix, 2008). They also require a substantial amount of staff time and specialized equipment for routine care (e.g., showering; Felix et al., 2009; Felix et al., 2010; Powell et al., 2010). Unfortunately, many NHs lack appropriate bariatric equipment and supplies, specialty-trained staff, and adequate number of staff (Lapane & Resnik, 2006) which can lead to negative resident outcomes such as rapid onset of pressure ulcers (U.S. General Accounting Office, 2003). Because of the challenges faced by NHs in providing care for obese individuals, it is possible that some facilities may not be willing to admit obese patients, potentially leaving them “stranded in hospitals” (Miles et al., 2012) and vulnerable to adverse medical events and increased health care costs. Anecdotal reports by hospital staff suggest this to be the case; yet few studies have examined NH admission decisions for post-acute care needs of morbidly obese patients (Davis, Devoe, Kansagara, Nicolaidis, & Englander, 2012; Miles et al., 2012; Popejoy, Galambos, Moylan, & Madsen, 2012). We are aware of only one study (Miles et al., 2012) that has specifically addressed hospital to NH care transition of morbidly obese patients. Documenting the experience and perceptions of NHs in making admission decisions for morbidly obese patients leaving the hospital is important to assess access to post-acute care settings as well as inform potential interventions to address NH admission challenges to ease challenges in the hospital to the NH transition process. Toward this end, the purpose of our study was to determine NHs’ willingness to admit patients weighing 325 pounds and above and identify barriers to admission.
Design and Method
This cross-sectional study used data obtained from postal mail surveys and existing sources to examine issues NHs considered when making admission decision for morbidly obese patients discharging from hospitals. We conceptualize the NH admission decision process as being influenced by facility-level characteristics related to the availability of resources. We categorized the characteristics as capacity (number of beds and occupancy rate), facility type (profit status and chain affiliation), internal resources (staffing levels and equipment concerns), and rurality. We hypothesize that NHs with fewer resources (fewer beds, higher occupancy rate, non-profit status, not a part of a chain, inadequate staff, equipment concerns, and rural location) will be more likely to view morbid obesity as an admission barrier.
The study was approved by the institutional review boards (IRBs) at the University of Arkansas for Medical Sciences and the University of Pennsylvania.
Sample
The study targeted nursing directors at all federally certified NHs in Arkansas (AR) and Pennsylvania (PA). NHs were identified using the publicly available online database, Nursing Home Compare (www.medicare.gov/nursinghomecompare). To be eligible for the study, participants had to be (a) a director or their designee of a federally certified NH in Arkansas or Pennsylvania, (b) able to understand and communicate in English to complete the survey instrument(s), and (c) over 18 years in age.
Primary Data Collection
All identified NHs were mailed a survey packet containing a paper survey (see the “Instrument” section below); a postage-paid return envelope; and a cover letter that described the purpose of the study, the potential risks and benefits of participation, and the study procedures. Return of the survey signified consent to participate. To achieve a high response rate, potential participants that did not return a completed survey received up to three reminders (e.g., additional survey mailings, postcard reminders) to encourage completion of the surveys (Dillman, 2000).
Instrument
Data were collected through the use of an IRB-approved survey instrument (available from the authors) that was a modified version of the instrument developed by researchers at the East Carolina University based on their review of the available literature, their experiences as researchers, and their pilot testing of the instrument with clinical experts (Miles et al., 2012). For our study, participants were instructed to respond to survey items as if considering admission of a morbidly obese patient weighing 325 pounds or more.
Survey items focused on the issues NHs considered when making decisions about admitting morbidly obese patients discharging from a hospital. Survey questions had defined response options, but most questions provided space for comments.
Secondary Data Collection
Two online, publicly available sources, Nursing Home Compare and the University of Washington’s Rural Urban Commuting Area (RUCA) Codes database (Morrill, Cromartie, & Hart, 2005), were used to obtain existing NH facility-level characteristics. These characteristics enabled the profiling of NHs by capacity (number of beds and occupancy rate), facility type (profit status and chain affiliation), and rurality (RUCA code). They were selected, in part, based on previous literature indicating that these NH characteristics can affect admissions for special populations (e.g., racial minorities) and quality of care (Carter & Porell, 2003; Harrington, Woolhandler, Mullan, Carrillo, & Himmelstein, 2001; Harrington, Zimmerman, Karon, Robinson, & Beutel, 2000; Hillmer, Wodchis, Gill, Anderson, & Rochon, 2005).
Data Analysis
All collected survey data were coded and entered into a database for analyses that also included facility-level characteristics obtained from existing sources for all responding and non-responding NHs. Characteristics of non-responding NHs were compared with responding NHs, and descriptive statistics were reported to examine potential selection bias. For NHs that responded to the survey, descriptive statistics were used to summarize and compare responses of responding NHs overall and by state.
Using logistic regression, the effects of facility-level characteristics on NH admission decisions for morbidly obese patients discharging from the hospital were examined. The dependent variable was the dichotomous response to whether morbid obesity was considered an admission barrier. Independent variables considered in the analysis represented facility-level characteristics and were obtained from the survey (staffing levels and equipment concerns) as well as existing sources (number of beds, occupancy rate, profit status, chain affiliation, and rurality). These variables were initially tested individually against the outcome, and then together in a single model.
As a sensitivity analysis, the alternate but similar dependent variable was selected from the survey responses and tested with the previously listed independent variables (each individually and then all together). The alternate dependent variable was the dichotomized unwillingness to admit morbidly obese patients (calculated by combining the “often” and “always” refuse admission survey responses as “yes, unwilling to admit” and combining “never” and “rarely” refuse admission survey responses as “no, willing to admit”).
Results
Survey Population and Respondent Profile
Of the total 15,659 federally certified NHs in the United States (Nursing Home Compare; www.medicare.gov/nursinghomecompare), 944 were located in Arkansas or Pennsylvania and comprised our survey population.
In total, of the 944 surveys sent to NHs in Arkansas and Pennsylvania, 360 surveys were returned, producing an overall response rate of 38.1%. The response rate was 39.3% for Arkansas (92 responded out of 234) and 37.8% for Pennsylvania (268 responded out of 710). Table 1 shows facility characteristics of responding and non-responding NHs, overall and by state. Of the responding NHs, the average number of certified beds per NH was 121.8, with an overall mean occupancy rate of approximately 87.0%.
Characteristics of Responding Nursing Homes, Overall and by State.

Note. Statistically significant results at alpha of .05.
AR = Arkansas; PA = Pennsylvania; NH = nursing home.
Compared with Pennsylvania, responding NHs in Arkansas had smaller facilities (107.1 certified beds vs. 126.9) and a lower occupancy rate (76.7% vs. 90.4%). There were substantial differences in proportion of responders from for-profit facilities by state, with 77.2% of Arkansas responders being for-profit compared with 47.1% of Pennsylvania responders. Very few of the responding facilities were hospital-based, but just over half of the responders in each state (57.6% in AR and 54.1% in PA) were chain-based facilities.
The responding and non-responding NHs were found to significantly differ on certain NH characteristics. Overall, those responding had a significantly higher occupancy rate (86.9% vs. 84.9%; p = .04) and were significantly less likely to be for-profit (54.7% vs. 61.5%; p = .04) or affiliated with chains (55.0% vs. 62.7%; p = .02) compared with non-responding NHs. See Table 1.
When looking at responding and non-responding NHs within each state, significant differences were found only for Arkansas. Arkansas responders were found to have a higher mean occupancy rate (76.7% vs. 71.8%; p = .03) and were less likely to be chain-based facilities (57.6% vs. 74.7%; p = .01) than Arkansas non-responders. No significant differences were found between responders and non-responders in Pennsylvania (Table 1).
Survey Responses
Table 2 shows the responses to survey questions, overall and by state. Respondents were asked the frequency with which they received referrals to admit morbidly obese patients. Overall, about one third (29.2%) indicated they received monthly referrals whereas nearly 35.0% of responding facilities reported such referrals to occur more frequently than monthly (e.g., daily, weekly, bi-weekly). However, there was significant variability (p < .0001) in the frequency of referrals between the two states, with more facilities (about 41.1%) reporting referrals occurring more frequently than monthly in Pennsylvania compared with in Arkansas, where only 16.3% of NHs reported referrals more frequently than monthly. No facilities in Arkansas reported never receiving such referrals whereas five facilities in Pennsylvania indicated they had never received a request to admit a morbidly obese patient.
Responses to Survey Questions, Overall and by State.
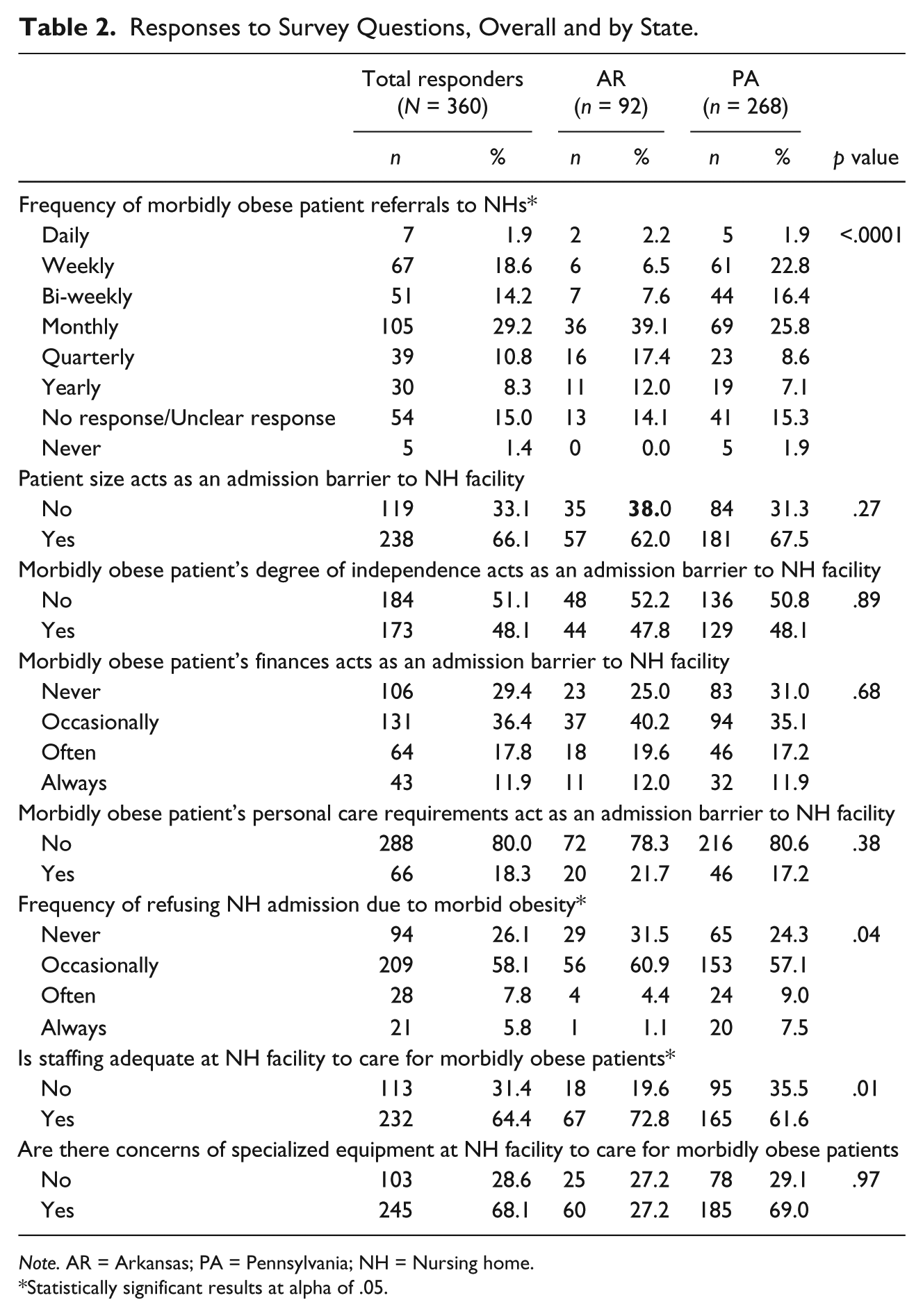
Note. AR = Arkansas; PA = Pennsylvania; NH = Nursing home.
Statistically significant results at alpha of .05.
Two thirds (66.1%) of responding facilities reported that patient size (e.g., morbidly obese) acted as an admission barrier, but only 5.8% (n = 21) reported that morbidly obese patients were always refused admission. There was no significant difference between states on patient size acting as an admission barrier. However, there was a significant difference (p = .04) between Arkansas and Pennsylvania NHs in terms of their reported frequency for refusing admission due to morbid obesity, with 7.5% of Pennsylvania NHs reporting they always refuse admission to morbidly obese persons compared with only 1.1% among Arkansas NHs. The independence level of morbidly obese patients was reported as an admission barrier by just under half of the facilities (overall and by state); whereas only about one in five respondents indicated that the personal care needs of morbidly obese patients would serve as an admission barrier.
Facilities were asked whether financial considerations (e.g., the cost of care for obese patients) affect admissions. Overall, 43 NHs (11.9%) reported that financial considerations would always act as an admission barrier for a morbidly obese patient. Similar response rates were observed among Pennsylvania (11.9%) and Arkansas (12.0%) responders.
Facilities were asked to indicate whether they had concerns about staffing levels or availability of specialized equipment to care for patients who are morbidly obese. There were significant differences between states on staffing concerns but no difference on equipment concerns. Nearly one third (31.4%) of NHs in both states reported having inadequate staff to care for morbidly obese residents; however, there was significant variation by state on staffing concerns. In Arkansas, only 19.6% of responding NHs (n = 18) reported having inadequate staffing levels whereas 35.5% of responding NHs in Pennsylvania (n = 95) reported the same (p = .01). More than two thirds of responding NHs in both states indicated that there were concerns about having adequate specialized equipment.
Facility Characteristics Associated With Admission Decisions
Table 3 shows the unadjusted and adjusted results obtained through the logistic regression models that were run to examine the association between NH characteristics and morbidly obese patient admission decisions. In the unadjusted analysis where separate models were run using only one NH characteristic as the independent variable, all six individually tested characteristics (number of certified beds, occupancy rate, for-profit status, chain status, staffing levels, and concerns about specialized equipment) were significantly associated with NHs indicating that morbid obesity would act as an admission barrier. Specifically, higher number of beds, higher occupancy rate, and concerns over available equipment were significantly and positively associated with NHs indicating that obesity would act as an admission barrier. NHs that were for-profit, chain-affiliated, and had adequate staffing had significantly lower odds (p < .01) of reporting morbid obesity as an admission barrier.
Unadjusted and Adjusted Analysis of the Association Between Nursing Home Characteristics and Morbid Obesity Acting as an Admission Barrier.
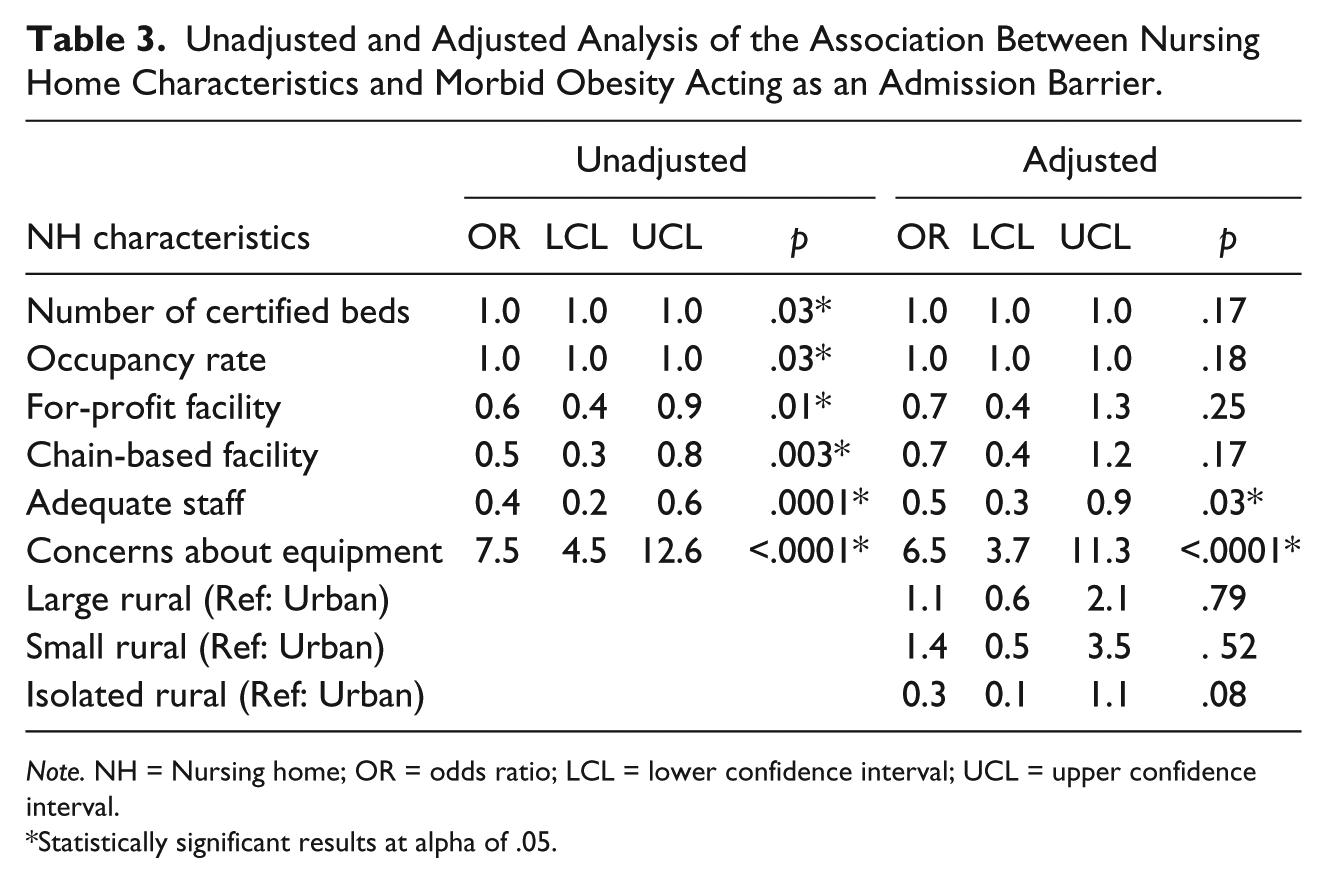
Note. NH = Nursing home; OR = odds ratio; LCL = lower confidence interval; UCL = upper confidence interval.
Statistically significant results at alpha of .05.
In the adjusted analysis, after controlling for capacity (number of beds and occupancy rate), facility type (for-profit and chain affiliation), internal resources (staffing and equipment) and NHs rurality status, only two factors were significantly associated with NHs reporting morbid obesity as a NH admission barrier. NHs reporting adequate staffing were significantly less likely than those understaffed (odds ratio [OR] = 0.5; 95% confidence interval [CI] = [0.3, 0.9]) to report that morbid obesity would act as an admission barrier to the NH (p = .03), after controlling for other characteristics in the model. NHs reporting concerns about the availability of specialized equipment required to care for the morbidly obese patients were significantly more likely to report morbid obesity as an admission barrier (p < .0001), after controlling for other characteristics in the model.
Sensitivity Analysis
Table 4 shows the results of the sensitivity analysis where the outcome measure models whether NHs would often or always refuse admission to patients due to morbid obesity. Both unadjusted and adjusted results show that equipment concerns and staffing levels affected admission decisions in the same manner as the original model: lower equipment concerns and higher staffing levels positively affected admission decisions. However, in the alternate model, higher occupancy rates were shown to negatively affect admission decisions.
Unadjusted and Adjusted Analysis of the Association Between Nursing Home Characteristics and Often or Always Refusing Admission due to Morbid Obesity.

Note. NH = Nursing home; OR = odds ratio; LCL = lower confidence interval; UCL = upper confidence interval.
Statistically significant results at alpha of .05.
Discussion
In this study, 360 directors of federally certified NHs (or their designees) reported on the issues considered when making decisions about admitting morbidly obese individuals. Study findings add to the limited existing literature and provide new insights regarding access to post-acute care for the morbidly obese.
Almost one third of our respondents noted that they received monthly referrals from an acute hospital setting, and another third reported at least weekly or bi-weekly referrals. In a recent study by Miles and colleagues (2012), 78% of skilled nursing facility directors reported monthly referrals. Therefore, it seems that NHs in our study, particularly those located in Pennsylvania, receive more frequent weekly or bi-weekly referrals than previously reported in the literature. This may be attributed to differences in the population of NH residents in these states, potential differences in the location of facilities included in our study (rural, urban, and suburban) versus those in the Miles et al. study which were primarily rural, and/or the increasing numbers of obese individuals seeking either short- or long-term care in the NH settings (Bradway, DiResta, Fleshner, & Polomano, 2008; Lapane & Resnik, 2005).
Not surprisingly, concerns about availability of bariatric equipment in NHs appear to negatively affect the admission decisions. Our findings strongly suggest that NHs without appropriate bariatric equipment are significantly more likely to view morbid obesity as a barrier to admission than those facilities not concerned about equipment issues. This is similar to findings from the North Carolina NHs study (Miles et al., 2012), which revealed 81% of the respondents from the considered equipment as a “major barrier” to successful NH placement. In addition to being a challenge to admission decisions, equipment concerns are also a recurring theme throughout the literature regarding the general care needs of obese NH residents. NHs accepting obese individuals need to plan for increased costs and staff in-service instruction associated with the purchase and use of specialized equipment such as larger beds, scales and lifts, shower and other chairs, and alterations to the physical environment including wider doorways and larger bathrooms (Felix, 2008; Lapane & Resnik, 2005; Lapane & Resnik, 2006). Obese individuals are also keenly aware that equipment plays an essential role in their day-to-day experiences in a long-term care setting. For example, one assisted living resident (who has since moved to a NH setting due to increased care needs) notes that he has “a beautiful outdoor patio—but my wheelchair is too wide to negotiate the doors, so I can’t wheel myself out onto it” (Bayne, 2012; Vitez, 2013). In another study, NH residents and nursing staff identified “fitting in the environment” (including numerous examples of how equipment and supplies, and/or the lack thereof, affected care (Bradway, Miller, Heivly, & Fleshner, 2010) as a primary theme associated with continence care and obesity.
Finding a NH bed for an obese individual is difficult. In the Popejoy et al. (2012) study, hospital health care professionals noted that morbid obesity caused difficulties in finding appropriate skilled nursing facility placement for patients ready for discharge, and in another study (Miles et al., 2012), 62% of the NH staff respondents noted size to be a barrier for admission. Similarly, more than two thirds of the respondents in our study noted that size acted as a barrier to NH admission; however, despite acknowledgment of this issue, a much smaller percentage noted that morbidly obese patients were “often” or “always” refused NH admission.
Next Steps
This is a complex issue with multiple organizational, environmental, and patient factors likely affecting the decision. Our findings indicate organizational resources are important factors. However, finding a bed for an obese individual may also be associated with the reimbursement mix/financial resources of the NH (e.g., whether payers will cover the cost of more expensive bariatric equipment; Felix et al., 2009; Powell et al., 2010; Zhang, Li, & Temkin-Greener, 2013), the physical environment of the NH (e.g., whether doorways are wide enough for bariatric equipment) and evacuation concerns, as noted by one of our respondents: The “fire marshal does not like bariatric beds, too hard to evacuate.” Finally, patient’s functional status and level of independence are important factors to consider. We therefore recommend further investigation to understand whether these additional factors affect the admission decisions for the morbidly obese. Similar calls for research into the effect of obesity on NH operations have been by other researchers who have examined the increase in diabetes among NH residents in Texas (Coxe, Lennertz, & McCullough, 2013).
Limitations
This study was conducted in Pennsylvania and Arkansas, and although our response rate of 38.1% was low, it is higher than in the recent study by Miles and colleagues (2012) and similar to what is typically obtained in survey research targeting organizations (35.7%) (Baruch & Holtom, 2008). Nevertheless, the low response rate and focus on two states limit the generalizability of our findings to other states, areas of the country, or globally; however, we can build on similar data collected in primarily rural North Carolina (Miles et al., 2012). This allows us to begin to develop a more complete understanding of the issues NHs confront with making admission decisions for the post-hospital care of morbidly obese individuals.
An additional limitation of note is the wide confidence intervals for our finding regarding equipment concerns from both our initial models and our sensitivity models. These wide confidence intervals create uncertainly around our estimate of the effect of equipment concerns on admission decisions. To improve the precision of the estimate, we recommend expansion of the survey population to increase the sample.
Implications
Results from this study have clinical as well as economic implications as health care providers and organizations attempt to deal with increasing numbers of morbidly obese patients. Additional research, including examination of current regulations and reimbursement policies, should be undertaken to understand NH equipment acquisition decisions. Such research will likely have important implications for research and optimal care of obese individuals during times of transition. Further research is also recommended to address other areas of the United States and worldwide, and to describe the ongoing needs of NHs as they provide day-to-day care for obese residents and test strategies for addressing these needs. We also believe it is essential to consider inter-professional perspectives including licensed and unlicensed nursing staff who oftentimes spend the most time with the obese NH resident, as well as the perspective of the resident and family members/significant others in the experience of transition between settings. Additional studies are also needed to build on this study, and the work of Miles and colleagues (2012) describing the transitional care challenges experienced by hospital discharge planners and home health care agencies associated with care of obese individuals. Finally, it is of utmost importance and urgency that research findings are widely disseminated and used to address necessary changes in reimbursement and health policy for the NH industry.
Footnotes
Acknowledgements
The authors wish to thank Suzanne Leimkuhler (University of Pennsylvania’s School of Nursing [UPenn SON]) for assistance with data collection, Mary Lou Wallace (University of Arkansas for Medical Sciences [UAMS]) for assistance with data collection and processing, Jinger Morgan (UAMS) for assistance with data processing, and Mary Ann Rose and colleagues at East Carolina State for assistance with the data collection instrument.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received support for this work from the Research Committee of the University of Pennsylvania’s School of Nursing (UPenn SON), the Center for the Study of Obesity of the University of Arkansas for Medical Sciences (UAMS) Fay W. Boozman College of Public Health, and the UAMS Translational Research Institute (UL1TR000039).