
Abstract
The purpose of this study was to explore and describe older adults’ opinions regarding actions to prevent falls and to analyze differences in the opinions of highly versus less physically active older adults. An open-ended question was answered by 262 individuals aged 75 to 98 years living in the community. The answers were analyzed using qualitative content analysis, and differences in the categories were compared between highly and less physically active persons. Physical activity was measured according to a five-level scale. The content analysis resulted in eight categories: assistive devices, avoiding hazards, behavioral adaptive strategies, being physically active, healthy lifestyle, indoor modifications, outdoor modifications, and seeking assistance. Behavioral adaptive strategies were mentioned to a greater extent by highly active people, and indoor modifications were more often mentioned by less active older adults. Support for active self-directed behavioral strategies might be important for fall prevention among less physically active older adults.
Introduction
Falls among older people are common and often devastating, and the personal suffering (Rubenstein, 2006) and societal costs due to falls are extensive (Child et al., 2012; Heinrich, Rapp, Rissmann, Becker, & König, 2010).The incidence of falls and fall-related injuries varies among populations and settings (Peel, 2011). An epidemiological review confirmed that in the majority of studies on community-dwelling people aged 65 years and older, 20% to 33% fell each year, and in the oldest group, up to 60% fell within a 12-month period (Peel, 2011). Falls can result in fractures, fear of falling, and nursing home admission (Robertson & Gillespie, 2013). The latest available evidence on the prevention of falls and fractures among community-dwelling older adults supports exercise programs for individuals or groups, including muscle strength and balance training (Gillespie et al., 2012). Vitamin D supplementation for people with low levels of vitamin D, home safety interventions, and individually targeted multi-factorial interventions are associated with fewer falls among community-dwelling older people who have risk factors for falling (Gillespie et al., 2012). Furthermore, slow withdrawal of psychotropic drugs and an anti-slip shoe device worn in icy conditions decrease falls (Gillespie et al., 2012). Likewise, individually tailored multi-factorial interventions reduce falls and the risk of falls (Stubbs, Brefka, & Denkinger, 2015).
Physical activity is currently defined as any bodily movement produced by the skeletal muscles that results in energy expenditure (Haskell et al., 2007). Physical activity in daily life can be categorized into occupational, conditioning, sports, household, or other activities (Caspersen, Powell, & Christenson, 1985). A primary role of physical activity in the prevention of falls is to avert the onset of disease, which may result in disability. The secondary and tertiary roles are to slow the progression of disease and system impairment and promote the rehabilitation of disabilities to reach a level of greater autonomy in daily activities (Rose, 2008). Physical inactivity is a behavior-related risk factor for falls (Boelens, Hekman, & Verkerke, 2013) that doubles the risk of developing a disability that will affect mobility (Rose, 2008). The current consensus recommendations for physical activity in older adults are 150 min/week of moderate intensity (Chodzko-Zajko et al., 2009).
In a study by Hill et al. (2011), 333 older persons were asked to suggest strategies for reducing their risk of falls in the first 6 months after discharge from the hospital. Only 2.9% of participants suggested strategies that were associated with exercise, and the study highlighted the gap between what older people know about fall prevention and the research evidence. Several studies have shown that older people value personal control, empowerment, participation, and self-management in fall-prevention actions (McInnes, 2011; Pohl et al., 2015; Robinson, Newton, Jones, & Dawson, 2014; Yardley, Donnovan-Hall, Francis, & Todd, 2006). Older peoples’ attitudes and beliefs affect their adherence to fall-prevention programs (Calhoun et al., 2011) and acceptance of fall-prevention options such as hip protector use (Sims-Gould, McKay, Feldman, Scott, & Robinovitch, 2014). The older population is heterogeneous with respect to health, and the opinions on fall prevention might likewise differ among older people. It is important to further explore, describe, and utilize older peoples’ opinions on fall prevention and then use that knowledge to develop appropriate support.
Although purposeful physical activity is important in preventing falls (Gillespie et al., 2012), no previous study has investigated older peoples’ opinions on preventing falls in relation to the level of physical activity.
The purpose of this study was to explore and describe older adults’ opinions regarding important actions to prevent fall incidents and to analyze the differences in opinions regarding preventive actions among physically active versus physically less active older persons.
Method
The study design was cross-sectional, descriptive, and comparative with a combined qualitative and quantitative design.
Participants and Measurements
Participants were randomly selected from a population-based national register for two Swedish county councils. The inclusion criteria were community-dwelling people aged ≥75 years. Within the two county councils, there were 47,855 inhabitants aged 75 years or older at the time of data collection. Of a random sample of 600 persons obtained from the Swedish Central Bureau of Statistics, 525 persons met the inclusion criteria, and an information letter, consent form, and questionnaire were sent to these older adults. Seventy-five of the 600 persons appeared to live in elder care facilities. These persons were identified by author K.H. and author A.C.J., who examined all the addresses, and persons with addresses of sheltered living establishments were excluded. The individuals who agreed to participate completed and returned the questionnaires together with their signed consent forms. After two reminders, 378 individuals (72%; M age = 81.7 years, range = 75-101) from mixed geographic locations responded to the postal questionnaire. Data collection was accomplished between May 2010 and July 2010. The study was approved by the Regional Ethics Review Board of Uppsala, Sweden (Dnr 2010/136).
The study-specific questionnaire contained questions about the level of assistance in daily activities, use of walking aids, level of education, occurrence of falls in the last 6 months, fall-related self-efficacy, health-related quality of life, living arrangements, and level of physical activity (Hellström et al., 2013). The open-ended question, formulated by the research team, “What do you consider to be important actions to prevent falls?” was answered with short, handwritten narrative responses by 262 persons with a mean age of 81.3 years and a range of 75 to 98 years (69.3% of the submitted questionnaires; n = 378). Of all of the people meeting the inclusion criteria (n = 525), the response rate for the open-ended question was 49.9%. No significant differences were found between those who answered the open-ended question and those who did not with respect to age, gender, social status, fall frequency, use of a walking aid, or fear of falling. However, the education level was significantly higher among those who answered the question.
The sample was divided into highly physically active individuals (n = 135) and less physically active individuals (n = 124) based on each participants’ response to the question “How much time do you spend, in a typical week, performing moderately strenuous activities that make you warm? For example, walking at a brisk pace, gardening, heavier housework, bicycling or swimming. It can vary during the year, but try to give an average” according to a five-level scale (Folkhälsomyndigheten Public Health Agency of Sweden, 2014). The five-level scale is frequently used by the Public Health Agency of Sweden. It has been further developed into a compatible seven-level scale, which has recently been validated with a correlation coefficient of .7 with activity monitors (Olsson et al., 2016)
Answers that corresponded to the three lowest activity levels were considered low physical activity (1 = never; 2 = less than1 hr/week; and 3 = 1-3 hr/week), and the two highest score levels were classified as high physical activity (4 = more than 3 but less than 5 hr/week; 5 = ≥5 hr/week). The participant characteristics are shown in Table 1. The less physically active people were more likely to require assistance with the activities of daily living, use walking devices, and live in apartment blocks than the highly physically active people. The degree of fall-related self-efficacy and the scores on the EuroQol 5 Dimensions Visual Analogue Scale (EQ-5D VAS) were significantly lower among the less physically active persons. Falls in the last 6 months were less common in the highly physically active group. No significant differences were observed between the two groups regarding age, gender, accommodation with others, or education level.
Characteristics of the Study Participants (N = 262; High Activity n = 135, Low Activity n = 124; p Values for the Difference Between Groups).
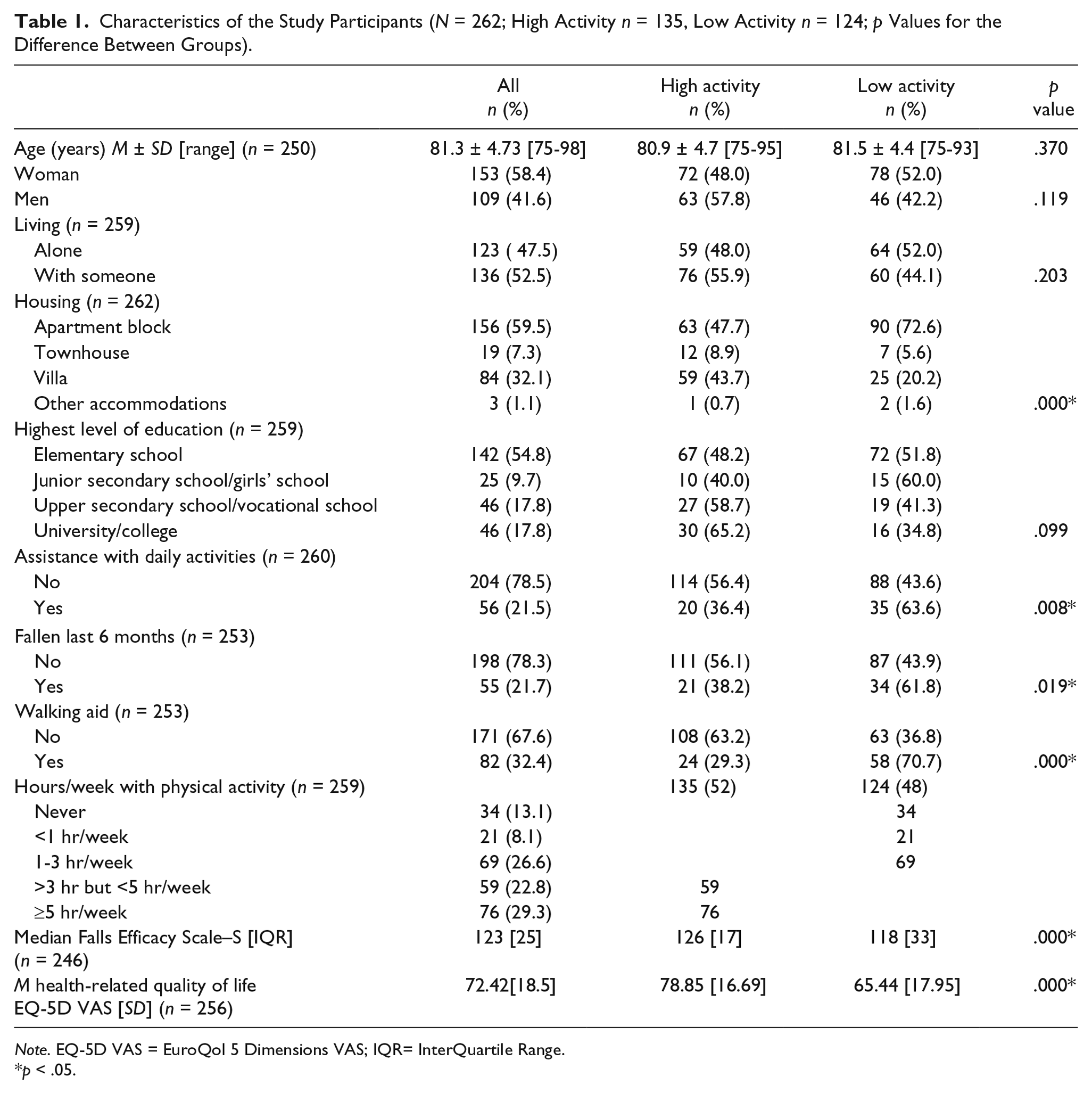
Note. EQ-5D VAS = EuroQol 5 Dimensions VAS; IQR= InterQuartile Range.
p < .05.
Data Analysis
Conventional qualitative content analysis was used to analyze the answers to the open-ended question (Hsieh & Shannon, 2005). To increase trustworthiness of the analysis results, three authors were involved (researcher triangulation), including S.T.J., who has clinical background within the field of elderly heath care, K.H., who has several years of field and research experience, and C.M., who has extensive qualitative research experience. All answers to the open-ended question were independently read several times by S.T.J. and K.H. to obtain an overall impression of the data, and statements were coded and classified into possible categories. The initial categories were agreed upon by S.T.J. and K.H. The selected category for each statement was then compared between these two authors, and adjustments were made. A third author (C.M.) was then involved in the analysis, resulting in a small redistribution of the categories and merging of some categories. As a parallel process, subcategories were suggested, and the three authors revised the analysis until consensus was achieved for the categories and subcategories. The content analysis was performed and completed in Swedish, and the participant responses were then translated into English. The content analysis was conducted without software program assistance.
Statements in each category were then analyzed according to whether a highly physically active person or a less physically active person made the statement. According to the type of data, the chi-square test, the Mann–Whitney U test, or the independent-samples t test was used to examine differences in characteristics between the two groups. A chi-square test was used to analyze the differences in category distribution between these two groups. Three people did not answer the question regarding their physical activity level; therefore, their statements were not included in the comparative analysis. Statistical significance was set at p < .05, and statistical analyses were performed using the IBM SPSS statistics software, Version 22.0.
Results
Older Adults’ Statements Regarding Actions to Prevent Falls
Two comprehensive areas of responses were identified: internal strategies, that is, self-reinforcing (or avoiding) personal strategies, and external strategies, which involve external help or modification of the environment. Eight categories of actions to prevent falls emerged. The categories, in alphabetical order, are as follows: assistive devices, avoiding hazards, behavioral adaptive strategies, being physically active, healthy lifestyle, indoor modifications, outdoor modifications, and seeking assistance. Each category contained three to 10 subcategories, which are presented in order according to the number of statements in each subcategory (Table 2). Example responses for each subcategory are provided.
Categories and Subcategories Describing 262 Older Adults’ Opinions on Actions to Prevent Falls.
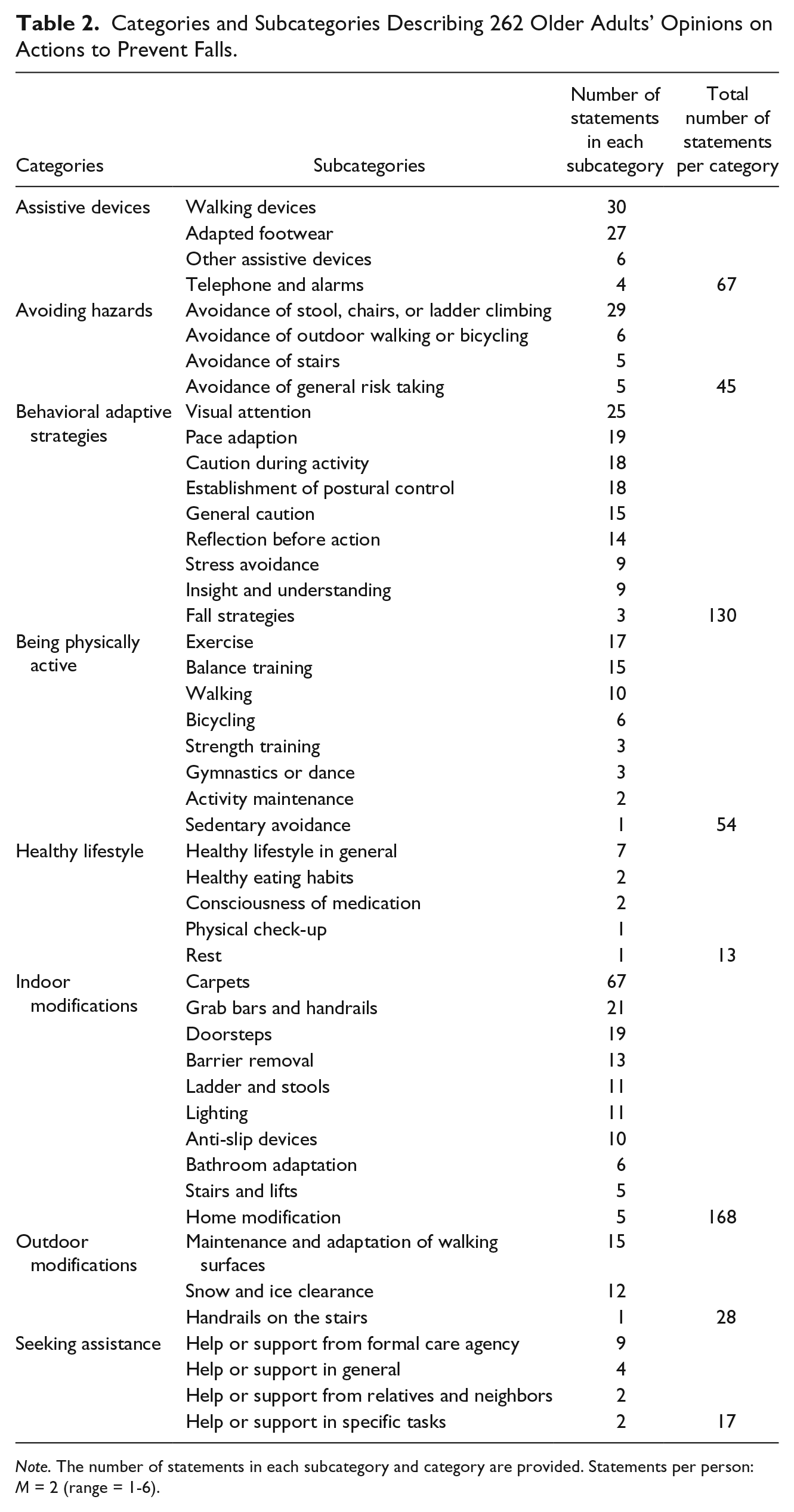
Note. The number of statements in each subcategory and category are provided. Statements per person: M = 2 (range = 1-6).
Assistive devices
This category contained statements referring to various types of supportive devices that were perceived as helpful in preventing falls or supporting the perception of safety. The four subcategories were as follows: walking devices, adapted footwear, other devices, and telephones and alarms.
“Every older person should have a walker or a stick,” “I’m unsteady and weak; without a walker it wouldn’t work,” “Use good shoes with tested insoles,” “Good glasses,” and “It feels safe having an alarm ’cause I live alone.”
Avoiding hazards
This category covered statements expressing the total or partial avoidance of hazardous activities or risk taking in general to prevent falls. The emerged subcategories were as follows: avoidance of stool, chairs, or ladder climbing; avoidance of outdoor walking or bicycling; avoidance of stairs; and avoidance of general risk taking.
“Avoid rickety stools,” “Show discipline, avoid climbing,” “Don’t stroll in the dark,” “Don’t walk outside when you are tired,” “Do not live on the third floor,” and “Don’t expose oneself to risks.”
Behavioral adaptive strategies
The category of behavioral adaptive strategies contained statements regarding the actions to adjust behavior in an ongoing or forthcoming situation or activity to reduce the risk of falling. The nine subcategories were as follows: visual attention, pace adaption, caution during activity, establishment of postural control, general caution, reflection before action, stress avoidance, insight and understanding, and fall strategies.
“Watch carefully where you’re going when you are outdoors, so you don’t stumble on uneven ground,” “Sit for a little while before you rise from your bed,” “Tread carefully on the stairs,” “If you have to rise rapidly, make sure there is something to hold on to,” “Consider a certain degree of wariness,” “Think before you act,” “Don’t rush,” “Don’t overestimate your capacity,” and “Prepare oneself for putting out a hand to break a fall.”
Being physically active
This category included statements regarding various types of physical activity and sedentary avoidance to prevent falls. The eight subcategories were as follows: exercise, balance training, walking, bicycling, strength training, gymnastics or dance, activity maintenance, and sedentary avoidance.
“Move yourself as much as possible,” “Exercise your balance through standing on one leg while brushing your teeth,” “Taking a walk every day,” “Do Nordic walking,” “I use my exercise bike every morning before I wash myself,” “Perform strength exercises to the best of your ability,” “Do gymnastics every day,” “Sustain your activity level,” and “It’s no good to keep still.”
Healthy lifestyle
The statements in this category referred to various aspects of maintaining health-promoting behaviors. The following subcategories emerged: healthy lifestyle in general, healthy eating habits, consciousness of medication, physical check-ups, and rest.
“Keep up your good shape,” “Keep a careful check on your food,” “Be aware of your medication,” “Health examination,” and “You should be reasonably rested.”
Indoor modifications
This category was the most represented category, and it included statements about adaptation to and modification of the indoor environment. The 10 subcategories were as follows: carpets, grab bars and handrails, doorsteps, barrier removals, ladders and stools, lighting, anti-slip devices, bathroom adaptations, stairs and lifts, and home modifications.
“You shouldn’t have carpets in the kitchen (but I have them anyway),” “To have handrails on both sides of your basement stairs,” “Low or no thresholds in one’s home,” “Do not have things on the floor that you can stumble on,” “Step-ladder with a high handle!” “Proper lighting where you walk,” “Use carpet pads,” “Non-slip bath tub with a step-out handle,” “Use markings on stair-steps,” and “Adjusted apartment where everything should be easily accessible.”
Outdoor modifications
This category described adaptation to, and modification of, the outdoor environment. The subcategories were as follows: maintenance and adaptation of walking surfaces, snow and ice clearance, and stair handrails.
“Fix defects in the streets and pavements,” “Lighted walkways,” “Improved clearance of sidewalks as soon as possible after a snowfall,” and “Grab bars where there are level differences or stairs.”
Seeking assistance
This category described various types of human assistance requested for preventing falls or supporting the perception of safety. The four subcategories were as follows: help or support from formal care agency, help or support in general, help or support from relatives and neighbors, and support in specific tasks.
“Information or supervision from a physiotherapist on appropriate exercises,” “If you start falling, you will need an alarm, right? . . . or being taken care of,” “Ask for help if you need it,” “To have a neighbor who has a key and pays a visit quite often,” and “Get help with light bulb changes, curtain changes and such situations when stair climbing is necessary.”
Differences in Opinions Between Highly Physically Active and Less Physically Active Older People
All the statements were divided into two groups according to whether the statement was expressed by a physically highly active or less active older person. The distribution of opinions differed significantly between the two groups in the eight categories (p = .028; Table 3).
Number of Statements in Each Category of Actions to Prevent Falls in Older Adults With High and Low Levels of Physical Activity Based on 513 Statements From 259 People.

Note. Percentage of total statements per group shown in parentheses. Difference in the category distribution between groups: p value = .028. *p = 0.03. **p = 0.001.
“Behavioral adaptive strategies” accounted for 28.2% of all of the statements expressed by older people with a high physical activity level and 19.9% of the statements made by people with a lower physical activity level. “Indoor modifications” accounted for 26.4% of the statements of highly active people and 40.7% of those of less physically active persons. The category “being physically active” accounted for 12.3% and 8.1% of the statements of people with high and low physical activity levels, respectively. No differences were found between the two groups in terms of the categories “assistive devices,” “avoiding hazards,” “healthy lifestyle,” and “outdoors modifications.”
Discussion
In this study, one aim was to explore and describe older adults’ opinions regarding important actions for preventing falls. The responses from 262 community-dwelling older people revealed a broad range of opinions on actions to prevent falls. Eight categories and 47 subcategories emerged (three to 10 subcategories in each category). Two comprehensive areas of responses were identified: internal strategies, that is, self-reinforcing (or avoiding) personal strategies, and external strategies, which involve external help or modification of the environment. The second aim was to analyze the differences in fall-prevention opinions between highly physically active and less physically active older people. Highly physically active people more often mentioned internal behavioral strategies than did less active people, and less active people more commonly reported strategies for environmental modification than did highly active people.
The suggested actions and strategies in our study correspond to responses in a study by Hill et al. (2011) in which a similar, but not identical, population was included. In the Hill et al. study, 333 participants (M age = 79.2 years) responded to an open-ended question during a semi-structured interview prior to discharge from the hospital. The obvious population differences between the studies are the different countries (Australia vs. Sweden) and patients completing a hospital stay versus a random sample of older adults living in the community. Hospital stay in general was not evaluated in the present study. Only hospital stay and health care contact due to fall incidents were included. The seven categories that emerged in the study by Hill and co-workers were as follows: behavioral, support while mobilizing, approach to movement, physical environment, visual, medical, and activity and exercise. The answers obtained in that study largely matched the statements in our study. The focus of the Hill et al. study was to investigate the gap between older peoples’ knowledge of fall-prevention strategies and existing research knowledge. Although regular exercise can help prevent falls, only 2.9% of participants suggested activity and exercises as a fall-reduction strategy (Hill et al., 2011). However, in our study, 10.5% of the statements were related to physical activity and exercise. This difference between studies might be explained by a higher awareness of the positive effects of physical activity in the participants of the present study, differences in education level, and/or differences in the selection of participants.
In Sweden, older adults can increase their awareness and knowledge of fall-prevention strategies via sources such as media (e.g., television, radio, newspapers, and magazines), health care providers, social care providers, senior citizen groups, friends, and relatives. Some municipalities in Sweden have well-developed plans for fall-prevention programs, but often, the implementation processes are slow and complicated because evidence-based interventions require evidence-based implementation methods (Fixsen, Scott, Blase, Naoom, & Wagar, 2011), which are not always used. Furthermore, Sweden lacks national fall-prevention guidelines for older adults living in the community; national guidelines only exist for health care settings (bSwedish Association of Local Authorities and Regions [SALAR], 2011). The two county councils represented in this study did not have structured fall-prevention guidelines at the time of data collection. Many municipalities in Sweden support older citizens by providing information about fall prevention in general, and the benefits of removing loose carpets are often emphasized. Of the 513 statements in our study, 167 (32.6%) were in the category “indoor modifications,” which indicates that a well-established fall-prevention action is the modification of your immediate environment. In this category, statements about carpets were the most frequently mentioned. Some respondents stated that although carpets should be removed, they nevertheless did not want to remove them, which reflects ambivalence about changing the home environment. Other studies have shown that many individuals are uninterested in household modifications for improving safety (Kruse, 2010; Tanner, 2008). Kruse (2010) found that participants’ residences had vital personal and social meanings and that managing one’s own physical environment was essential for making “a house into a home” such that recommendations from others may be considered an intrusion on personal choice.
Only two individuals in the present study (0.7%) mentioned medication management as an important action for preventing falls. A similar finding was reported by Hill et al. (2011), with five of 333 participants mentioning medication management as a strategy, and in the study by Laing, Silver, York, and Phelan (2011), zero of 101 participants spontaneously endorsed the review and management of medication as a possible action for preventing falls. These concordant results indicate that knowledge of the impacts of medication on falls should be increased among older adults.
To the best of our knowledge, the relationship between older adults’ opinions on fall-prevention actions and older adults’ level of physical activity has not previously been explored. The two comprehensive areas of responses identified in this study were internal strategies (i.e., self-reinforcing [or avoiding] personal strategies) and external strategies (involving external help or modification of the environment), which were related to physical activity level. The highly physically active people proposed more internal strategies, reflecting a self-management approach. In contrast, external actions were more commonly suggested in the less physically active group. As this was a cross-sectional study, the direction of causality regarding these findings cannot be determined, although it has been confirmed in other studies that older people with limited mobility (e.g., in need of a walker) more commonly report poor health, pain, and physiological problems as barriers to physical activity (de Groot & Fagerstrom, 2011; Rasinaho, Hirvensalo, Leinonen, Lintunen, & Rantanen, 2007) than do older adults with high mobility. In a previous study (Hellström et al., 2013) that was also based on the sample of the present study, low fall-related self-efficacy appeared to explain changes in activity behavior, and therefore, a more passive attitude toward fall-prevention actions was shown. In a recent study (Skipper & Ellis, 2015), a significant correlation was found between balance confidence and physical activity.
The results of our study can be explained within the framework of the health belief model (HBM; Janz & Becker, 1984), which is a commonly used conceptual framework for guiding health-behavior interventions. According to the HBM, individual beliefs (perceived susceptibility, threats, benefits, barriers, and self-efficacy) influence individual health behavior and thoughts about health behavior. For example, a person with perceived susceptibility to falls and barriers to physical activity might conclude that time spent on muscle training is not worth the effort due to an unconscious consideration of the physical strain in relation to the possible gains. Moreover, if his or her self-efficacy for exercising is low, it is likely that this person will focus on strategies other than exercise in attempting to prevent falls. The support of behavioral change in less physically active persons, which results in increased physical activity and behavioral adaptive strategies, requires knowledge and skills in behavioral change methods among the health professionals involved. It has not yet been determined which behavior change techniques are most effective for older adults (French, Olander, Chisholm, & Mc Sharry, 2014). However, behavior change interventions have been successful at enhancing self-efficacy and physical activity, although the effect sizes were small (French et al., 2014). In the present study, highly physically active older persons were more likely to suggest behavioral adaptive strategies and physical activity than were less active people, which might indicate perceived benefits (rather than barriers) in the suggested fall-prevention actions. These people might benefit from societal and community-based support, such as access to gyms that are adjusted for older adults, well-prepared pavements, and secure walking areas, to maintain or increase their level of physical activity. This suggestion is supported by a recent review (Franco et al., 2015) in which environmental and financial access to physical activity opportunities were identified as important factors influencing participation in physical activity. Consequently, health professionals supporting fall prevention in older adults must consider the heterogeneity and diversity in the individual needs of support and in the clinical or home rehabilitation settings; special attention should be paid to less physically active people. It is important to investigate the physical activity levels of older adults. A recent umbrella review of meta-analyses emphasized the importance of individual assessments, preferably made by physical therapists, in conducting individually tailored interventions for persons at high risk of falling with a range of limitations (Stubbs et al., 2015).
In the present study, an open-ended question was used to capture spontaneous statements regarding fall-prevention actions. A limitation of the study was that although the response rate for the questionnaire was high (72%), only 262 (of 378 respondents) answered the open-ended question regarding actions to prevent falls. In addition, the education level was significantly higher among those who had answered the open-ended question than among the non-respondents. A correlation between the response rate and level of education has been identified by other authors (Ekholm, Gundgaard, Rasmussen, & Hansen, 2010; Lindén-Boström & Persson, 2013). To collect responses from people with lower education levels, interviews might be more effective than open-ended questions. Individuals with higher levels of education are considered more disposed to be physically active (Gerrard, 2012; Shaw & Spokane, 2008). However, our study did not identify a significant difference in education level between the two groups, which possibly may be explained by the generally high level of education in the responding sample.
Living together with another person has been shown to have a positive impact on the time spent on physical activities (Satariano, Haight, & Tager, 2002; Seeman, 2000). However, this relationship was not observed in our study, as the living arrangements were similar between the high and low physical activity level groups.
The limit for high physical activity in this study was set at “More than 3 hr/week of activity that makes you warm,” which is 30 min more per week than the recommended 150 min/week (Chodzko-Zajko et al., 2009). The self-estimated level of performed physical activity is often overestimated (Dyrstad, Hansen, Holme, & Anderssen, 2014; Rzewnicki, Vanden Auweele, & De Bourdeaudhuij, 2003). Therefore, it is likely that estimations of Level 3 (1-3 hr of physical activity per week) often represented <150 min/week rather than the recommended >150 min/week, and therefore, Level 4 was set as the limit for high physical activity.
Clinical Implications
To the best of our knowledge, older adults’ opinions on fall-prevention actions, stratified according to their level of physical activity, have not previously been investigated. General fall-prevention programs often include physical activity as an important part of the intervention (Gillespie et al., 2012). These programs are valuable for many individuals, but a more individualized approach might be needed to enhance physical activity and other self-management strategies for fall prevention among frail older adults who require walking aids and assistance with daily activities, have low fall self-efficacy, and are less physically active. A distinct focus should be placed on dialogue with older adults regarding their individual current physical activity levels and thoughts regarding fall prevention. This practice would provide a basis for setting realistic goals regarding behavioral change to promote fall prevention, and the older adults should participate in the process.
As knowledge of the impacts of medication on fall risk seems incomplete, medication should be investigated in fall-prevention interventions and discussed with older adults to improve their awareness of the risks.
The findings of this study contribute to awareness of the different needs for support in fall-prevention actions among older community-dwelling people, in which less physically active persons might require more individual self-reinforcement and behavioral change support.
Footnotes
Authors’ Note
The study was approved by the Regional Ethics Review Board of Uppsala, Sweden (Dnr 2010/136).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the municipality of Uppsala and by The Regional Research Council in Uppsala and Örebro, Sweden.