
Abstract
Types of compromised resident behaviors licensed nursing facility social workers encounter, the behavioral health role they enact, and effective practices they apply have not been the subject of systematic investigation. Analyses of 20 in-depth interviews with Bachelor of Social Work (BSW)/Master of Social Work (MSW) social workers averaging 8.8 years of experience identified frequently occurring resident behaviors: physical and verbal aggression/disruption, passive disruption, socially and sexually inappropriateness. Six functions of the behavioral health role were care management, educating, investigating, preventing, mediating, and advocating. Skills most frequently applied were attention/affirmation/active listening, assessment, behavior management, building relationship, teamwork, and redirection. Narratives revealed role rewards as well as knowledge deficits, organizational barriers, personal maltreatment, and frustrations. Respondents offered perspectives and prescriptions for behavioral health practice in this setting. The findings expand understanding of the behavioral health role and provide an empirical basis for more research in this area. Recommendations, including educational competencies, are offered.
Keywords
Social workers in residential long-term care settings address psychosocial needs of residents as part of the facility’s responsibility to assure resident mental health and well-being (Bern-Klug, 2011; Bern-Klug & Kramer, 2013; Grabowski, Aschbrenner, Rome, & Bartels, 2010; Omnibus Reconciliation Act, 1987; Simons, Bern-Klug, & An, 2012; Simons, Connolly, et al., 2012). Professional guidelines and regulations (Centers for Medicare & Medicaid Services, 2011; National Association of Social Workers [NASW], 2003, 2008; U.S. Department of Veterans Affairs, Office of Social Work Service, 2001) specify ways social workers ethically engage the psychosocial needs of residents. For example, the NASW (2003) Standards for Social Work Services in Long-Term Care Facilities state that the social work program should “assist with attaining or maintaining the highest practical mental and psychosocial well-being, while helping residents who display mental or psychosocial difficulty receive appropriate treatment and services” and “[act] as a resource to staff participating in behavioral interventions” (p. 14).
These standards are particularly relevant when behavioral health is compromised by a lack of attention to resident needs within the nursing care facility. This discontinuity between what the resident is seeking and the responsiveness of the care environment creates resident behavioral responses that may challenge the capacity of care providers to respond. Behavioral responses may be expressed as resident physical aggression toward other residents, leading to resident-to-resident elder mistreatment and sexual aggression (Beaulieu, 2012; Doron & Koren, 2004; T. Rosen, Lachs, & Pillemer, 2010). From the staff perspective, these behavioral responses may be viewed as harmful physically, emotionally, and/or relationally and include physical, verbal, and sexual aggression. The inability of staff to adequately address the underlying factors that motivate resident aggressive behavior toward them may affect their morale, turnover, and job satisfaction (Lachs et al., 2012).
As individuals living in nursing facilities progressively require mental health and behavioral management resources (Grabowski, Aschbrenner, Feng, & Mor, 2009), nursing home social workers are increasingly called on to fulfill the role of in-house behavioral health managers. Most nursing facilities and the social workers they employ are unprepared for this emerging responsibility (Bonifas, 2011; Simons, Bern-Klug, & An, 2012; Tirrito, 1996). Their accumulated practice wisdom, with the assistance of behavioral health consultants and colleagues, inform social workers’ responses to these resident behaviors. Recent attention has been directed to identifying the types of aggressive resident behaviors nursing facility staff encounter (Lachs et al., 2016; T. Rosen et al., 2010) and the practices they apply (Grabowski et al., 2010; T. Rosen et al., 2016). This literature focuses on the reports of nursing staff and primarily addresses aggressive acts (physical, verbal, and sexual) directed either to other residents or to staff. Bonifas (2015), for the first time, extended research on staff responses to resident behaviors by including social service department directors in an investigation of their responses to resident-to-resident aggression and their collaboration with nursing staff. Building on Bonifas’s work, we report the experiences of 20 BSW or MSW prepared, licensed nursing facility (LNF) social workers across a wide array of resident behaviors and offer an expanded understanding of their behavioral health role in nursing facilities.
Purpose and Rationale
The researchers recognized that the behavioral health role had not yet been systematically examined from the perspective of LNF social workers who deal with challenging resident behaviors on a day-to-day basis. Our research goal is to add to the perspective and narratives of the nursing facility social worker in addressing resident behaviors to a larger and maturing literature that primarily draws on samples of nursing care staff. In this first phase of our more extensive research agenda examining the experiences and practices of these social workers, we systematically identify the types of behavioral responses they encounter, the functions of the behavioral health role they enact, and the approaches they employ to understand and address these behaviors. Our sample of experienced social workers responded to the following questions: What challenging resident behaviors do you encounter? When you encounter these problematic behaviors, what do you do?
These social workers were uniquely qualified to specify the types and prevalence of resident behaviors that they encountered and identify the range of responses they employed. Through in-depth analysis of their rich narratives, what has been known anecdotally and in practice wisdom about the behavioral health role is being verified, and the new knowledge made available to affirm, strengthen, and inform those committed to resident behavioral health as well as inform educational, regulatory, and industry organizations who prepare, regulate, and employ them. We conclude the study by recommending educational initiatives intended to develop the capacity of social workers to competently identify and address the unmet needs and unresponsive care environments that limit resident behavioral health.
Occurrence and Management of Compromised Resident Behavioral Responses
The preponderance of the evidence related to compromised resident behaviors and effective interventions in nursing facilities focuses on maladaptive responses that affect other residents and staff. Orengo et al. (2008) estimated that between 6% and 20% of residents display physically aggressive behavior and 11% significantly resist care (“MDS Active Resident Information Report,” 2010). Jones (2002) noted that the incidence of emotional and mental health challenges within the nursing facility is greater than the incidence of physical conditions. Prevalence is more pronounced among patients with dementia, reported at above 50% (Buchanan, Wang, Ju, & Graber, 2004; Kolanowski, Litaker, Buettner, Moeller, & Costa, 2011; T. Rosen et al., 2016). Although much research is available concerning the relationship between dementia and behavior management issues in nursing homes, patients without a dementia diagnosis may also exhibit compromised behaviors in residential long-term care settings. McCarthy, Blow, and Kales (2004) also reported that patients with severe mental illness (SMI) display more disruptive behaviors than patients with no cognitive impairment. The same study also states that SMI patients were more verbally disruptive than dementia patients, but the two groups “did not differ in physically aggressive or socially inappropriate behaviors displayed” (p. 2031). A survey of health care practitioners in nursing homes revealed the most common compromised behavioral responses that nursing home employees experience from residents are resisting care, vocal or verbal disturbance, physical aggression toward staff, and inappropriate sexuality-related behavior (Cohen-Mansfield, Jensen, Resnick, & Norris, 2012). Furthermore, the incidences of resident-to-resident elder mistreatment are reported at 20%, with the verbal aggression occurring most frequently (46%) and hitting (11%) the most frequent form of physical aggression (Lachs et al., 2016). Studies of resident–staff aggression reveal an incidence rate of 15%, with verbal aggression (screaming) at 12% and physical aggression (hitting) at 7.6% (Lachs et al., 2012).
Many difficult behavior issues are situational and not necessarily linked to impaired capacity of cognition. The wide range in compromised behavioral responses also stems from an array of potential causes, originating from the interaction of personal and social characteristics of the person (e.g., neurocognitive pathology, personality, cognitive and health status, social capital) with the facets of the care environment, for example, familiarity, responsiveness, caregiver skill and commitment, and organizational climate (Isaksson, Åström, Sandman, & Karlsson, 2009). Illustrations of how the care context affects resident responses are available in a well-designed study by Lachs et al. (2012), addressing the prevalence of resident-to-staff aggression. The researchers found clear associations between the occurrence of these behaviors in the resident’s room (77%), in the morning (84%), during the provision of routine activities of daily living (ADLs).
The prevalence of behavior challenges in nursing facilities leads to the question of how the behaviors might best be managed. An increasing body of research documents an array of nonpharmacological, evidence-based interventions for management of nursing home patient behavior. However, none of this research examines social worker management of behavioral health in nursing facilities. Most of the work around nonpharmacological strategies focuses on physical and verbal aggression related to dementia, resulting in several reports of effective interventions (Kolanowski et al., 2011; McGee & Bratkovich, 2011; Teri, Logsdon, & McCurry, 2002). These difficult behaviors in long-term care facilities are more frequent among dementia patients with depression, which is widely underdiagnosed (Menon et al., 2001). These interventions are also intended to address the need states of residents that include loneliness, depression, decreasing cognitive function, and a multitude of other elements.
Social and situational variables may contribute to the development of behavioral responses to unaddressed needs. Social isolation and separation from family may increase depression. Tsai, Tsai, Wang, Chang, and Chu (2010) found that a once weekly 5-min videoconference with family helps improve social support and decrease loneliness and depression. Other studies, such as Meeks and Looney’s (2011), suggest that depressed nursing home residents respond well to regular, positive staff interaction, unrelated to ADLs, which increases observed enjoyment and pleasure of participation in planned activities.
Ingersolldayton, Schroepfer, and Pryce (1999) noted that, along with social isolation, other social factors affect behaviors, as well. Residents who were moved, assigned new direct care staff members, or frequent medication adjustments were more prone to distressed behavioral expressions. The use of integrated interventions with patients needing additional attention because of behavior challenges was examined by Collet, Marjolein, de Vugt, Frans, Verhey, and Jos (2010), who found that a combination of medical, nursing, and psychiatric interventions are beneficial in behavior management of this type of population.
Other nonpharmaceutical approaches have been demonstrably successful as alternatives to medication. Connell, Sanford, and Lewis (2007) instituted an outdoor activity program for long-term care patients with dementia and found the program to have therapeutic effects on the residents in terms of disruptions, both in behavior and sleep. In a 2007 study by Dowling, Graf, Hubbard, and Luxenberg, the effect of morning or afternoon bright light exposure for dementia patients with problematic neuropsychiatric behaviors was assessed. The conclusion reached is that light therapy significantly decreased agitation and aggression along with other disruptive behaviors. Solution-focused therapy has also been found to be an effective alternative for modifying problem behaviors among nursing home residents (Ingersolldayton et al., 1999).
Opie, Doyle, and O’Connor (2002) initiated multiple intervention techniques among nursing home residents who were rated as behaviorally difficult by staff members, and concluded that intervention, in and of itself, provokes change in the long-term care setting. All the intervention groups showed significant improvement, as far as decreasing problematic behaviors. Another study found that strength of faith was associated with significantly lower rates of socially inappropriate behaviors (Branco & Braam, 2006). Other interventions observed to have a positive effect on problematic behaviors include pain management, individually tailored music regimens, and therapeutic massage (Zwijsen et al., 2011). A focus group consisting of 35 staff members from six nursing homes discussed the barriers to the implementation of nonpharmaceutical interventions to control behavior problems among nursing home residents. Although several barriers were discussed, including the lack of sufficient staff education, the key theme that emerged was that of time constraints (Kolanowski, Fick, Frazer, & Penrod, 2010).
A thorough examination of current literature revolving around the issue of nursing home resident behavior challenges highlights staff training as an essential element in improving intervention outcomes. A common observation emerges that interventions of many types improve resident behavior issues simply through increased interactions with staff members and the positive effects of exposure to supplementary attention.
Conceptual Framework
Algase et al. (1996) proposed the need-driven compromised behavior (NDB) model, an example of a helpful framework for understanding, assessing, and intervening with compromised (aggressive and passive) behaviors in persons living with dementia (PLWD). Although the model is specific to dementia-related interventions, the basic premise that compromised resident behaviors are an indication of unmet human needs is relevant for other resident behavioral health challenges. In this model, compromised behaviors are the outcome of discontinuity between predisposing risk factors such as physical and cognitive condition and personality on one hand, and predisposing contextual characteristics of the environment and the need state of the resident on the other (Kolanowski et al., 2011), thereby eliciting the range of compromised behavioral responses well documented in current research. As observed by Long (2005), Typically, a behavior problem—that is, something that is harmful physically or emotionally—happens because of internal and external factors. In fact, it often is hard to say whether a problem behavior is either completely internal or external. Every behavior problem is likely to have triggers or reinforcers of both types. (p. 1)
The NDB and other frameworks that highlight the importance of attention to need states as well as relational and contextual factors aim to create optimal congruence between person and care context, so that the resident can attain the highest level of functioning (Kuk, Rixt Zijlstra, Bours, Hamers, & Kempen, 2016). Implementing the NDB perspective turns the attention of care professionals from excessive focus on compromised behavioral expression to more effective interventions that match the capacities, interests, and personality of the resident with the facets of the care environment and the current needs of the resident.
The NDB model’s focus on the need that energizes the behavioral response of the PLWD is consistent with foundational values, knowledge, and skills of professional social workers. Just as the NDB framework guides interventions that address need states, competent social workers look beyond presenting behavioral issues and reach for deeper understanding of the meaning of human behavior. This orientation to fuller understanding of the person is consistent with core professional values of respect for persons and client self-determination. One of the intentions of NDB is to effectively match personality style of interest and functional ability with facility activity opportunities. Consistent with the model’s intentionality around fit between the PLWD and the facility environment, social workers are encouraged to view presenting issues from an ecological perspective (Germain & Gitterman, 1996), explaining maladaptive responses as an indication of a lack of fit between the needs of persons and the resources of their environment. To improve transactions between, in this case, residents and the care environment of the nursing facility, social workers enact the skills of tuning into the resident’s story and practicing the skill of engagement to respond effectively to the presenting need (Shulman, 2016). As observed by Kolanowski et al. (2011), “failure to understand the need communicated by the behavior may lead to inappropriate and ineffective treatment” (p. 1032).
As previously mentioned, Bonifas (2015) provided the first study focusing on the involvement of social services personnel in managing resident-to-resident aggression in nursing facilities. The study included individual interviews with 10 social service directors and 10 directors of nursing in 10 nursing homes. The researcher documented the ways that social workers moved beyond resident’s aggressive behavior to apply the care orientation that aligns with the perspective of the NDB model and foundational social work principles. For example, the interviewees stressed the importance of deep knowledge of the resident in understanding the causes of resident-to-resident aggression. The findings revealed interdisciplinary assessment strategies of gathering information about incidents, ruling out potential causal factors, and determining their psychosocial impact. The intervention process was also highly collaborative with nursing staff, based on a strengths-based and person-centered perspective. Prevention was emphasized, with significant attention to maintaining autonomy and a respectful approach. Careful roommate matches were essential from a prevention perspective. When appropriate, behavioral contracts were negotiated, supportive counseling was offered, referrals for additional support were made, and attention was paid to personal loss as a trigger for aggression. The findings of the interviews with social service staff yielded significant insight into professional practices around this, presenting behavioral challenge. In our study, we expand the contribution of Bonifas’s (2015) work by enlisting a sample of licensed and experienced nursing facility social workers who reflect on their experiences and responses with residents who deserve responsive care environments to their behavioral health needs.
Method
After receiving approval from the university’s institutional review board (project title: [207919-1] Social Workers and Administrators in Residential Long-Term Care Settings: Role Performance, Challenges, and Possibilities), the researchers conducted face-to-face interviews with a purposive sample of 20 social workers (Licensed Bachelor of Social Work [LBSW], Licensed Master’s of Social Work [LMSW], or Licensed Clinical Social Work [LCSW]) working within 20 nursing facilities who met these inclusion criteria: full-time employment as a licensed BSW or MSW social worker in one of the 20 facilities included in the study, a minimum of 1 year of employment in a licensed nursing care facility as a provider of social services, and a baccalaureate or master’s degree in social work.
The facilities in the sample represented more than half of the 36 LNFs in the catchment area of a southwestern state eligible to be included in the sample. The sampling frame and the distribution by facility type were private, nonprofit (n = 5); private, for-profit individually owned/limited partnerships (n = 6); private, for-profit corporately owned (n = 4); limited liability company (n = 3); private, for-profit medical center–affiliated (n = 1); and public (n = 1). The researchers sent an email to the administrators of the nursing facilities that met the facility sampling criteria that explained the purpose of the study and requested permission to contact the facility’s licensed social workers to invite them to participate in the study. Affirmative responses to participate were accepted until the benchmark of 20 licensed social workers in 20 facilities was met and there was at least one facility within each ownership category that agreed to allow the researchers to contact the facility’s social worker(s).
After receiving permission from the nursing facility administrator, the researchers sent via email an invitation to participate in the study to the most experienced, full-time social worker on their staff and followed up with a telephone contact. The invitation included the purpose of the study, the terms for participation, and an informed consent statement, emphasizing the social worker’s right to not participate or withdraw from the study at any time without consequences to his or her employment. All the invited social workers agreed to participate. At the initial interview, the informed consent statement was reviewed and signed by the social worker. No financial compensation for participation was offered.
Using a cross-sectional, semistructured interview design, face-to-face, in-depth, 60- to 90-min interviews were conducted in 2012, guided by a pilot-tested interview protocol (the appendix). They addressed questions about the compromised behavioral responses they encountered and the ways they responded. Interviewees’ responses and locations were deidentified to assure confidentiality. All the interviews were transcribed. Quantifiable data on years of experience, educational attainment, types of difficult behaviors, and practices in responding to resident behavioral responses were analyzed by calculating frequencies of responses by category.
Narrative data were examined through a thematic analysis approach supported by Atlas.ti (version 6.0) qualitative software. The qualitative data analysis began with extensive reviews of transcripts to gain familiarity with the data. We applied a modified constant comparison analysis approach (CCA; Glaser & Strauss, 1967) to iteratively and inductively reduce the social worker narratives. Following Fram (2013), we applied the CCA processes outside the intention to create grounded theory. We observed the similarities and differences among the social workers’ responses to our open-ended inquiries about their experience. When segments of the narratives addressed a common idea, we used initial codes with definitions to ascribe meaning to the segment. Every segment within the database was compared with one another and with the codes to ascertain whether it was illustrative of an established code or offered new understanding of the respondent’s experience, thus requiring a new code. After initial codes were set, code subcategories as well as higher order axial codes were proposed. The process of revisiting segments and codes continued until conceptual saturation was attained and all segments were analyzed (Elliott & Jordan, 2010). The entire set of data was then reviewed to ensure congruence between codes and segments.
Transcript analyses occurred in regularly scheduled research team meetings to increase trustworthiness and accuracy of findings, process insights from research memos, and triangulate independent analysis of codes into emerging axial categories (Cresswell & Plano Clark, 2011). Differences in code-to-segment relationships, code and subcode names and definitions, and data interpretations were debated until consensus was formed regarding the findings. To further increase the accuracy of the findings, study interviewees were also invited to review the findings and recommend edits.
The research team, which included three social workers with research and practice experience in long-term care and a highly experienced behavioral specialist in resident behavioral management, had 20 conversations to process insights, map codes and emerging concepts, and challenge each other’s analysis. Insights from individual analysis and team conversations yielded 11 axial or “parent” codes to organize the 211 codes for the data. Transcripts and data analysis documentation are available from the first author. Primary data files related to this research are available upon request to
Findings
This section begins with a report on the characteristics of our sample, documenting the qualifications of our interviewees to provide an informed perspective on the role of social work in addressing resident behavioral health. Sample characteristics are followed by three major sections: resident-compromised behavioral responses (Table 1), functions of the social work behavioral health role and responsibilities (Table 2), and social work skills (Table 3). Each section has two parts—a summary of the findings using categories and frequencies based on our coding protocol as well as summary observations and quotes that clarify and illustrate their experience and reflections.
Resident-Compromised Behavioral Responses Encountered by Category.
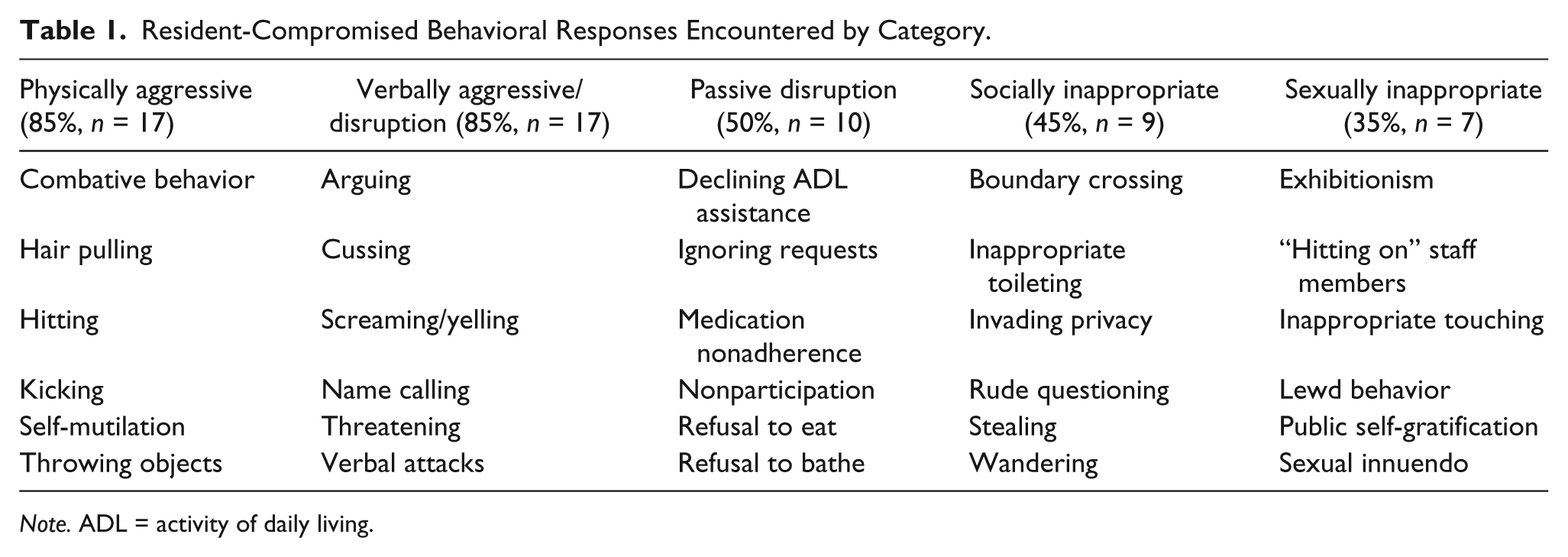
Note. ADL = activity of daily living.
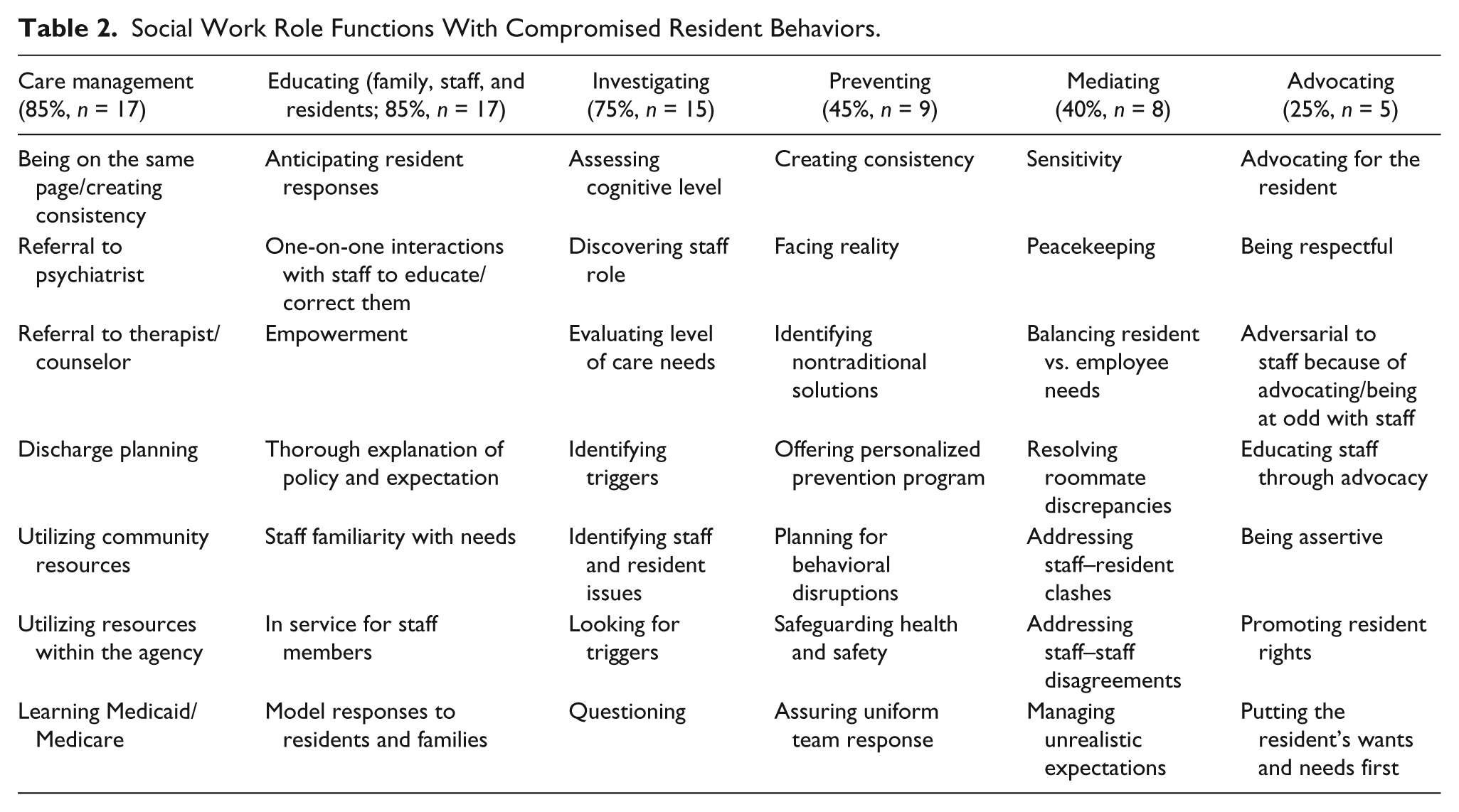
Social Work Role Functions With Compromised Resident Behaviors.
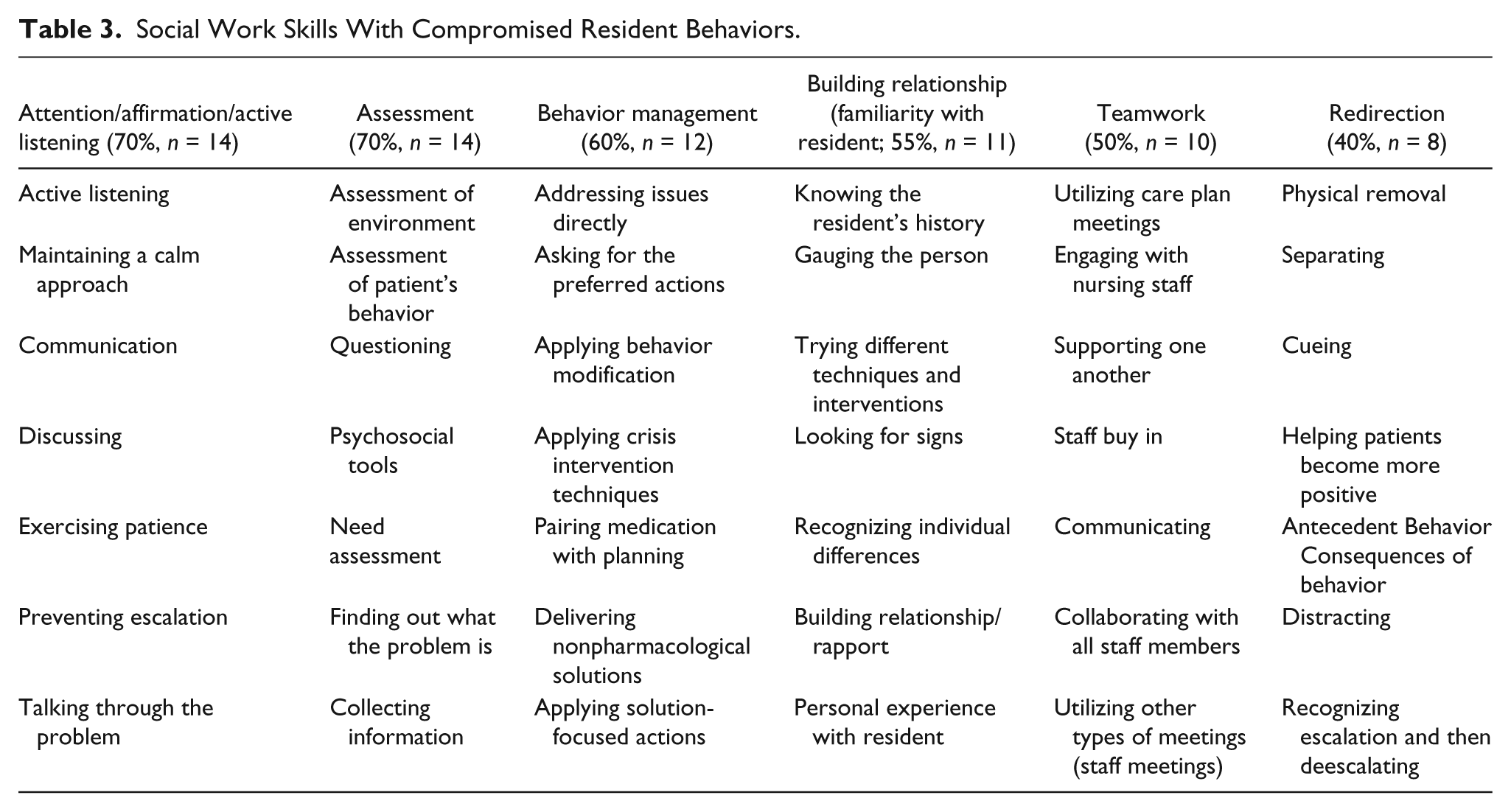
Social Work Skills With Compromised Resident Behaviors.
Sample Characteristics
All interviewees who responded held a social work degree from an accredited institution and a social work license at the baccalaureate or master’s level; however, one of the 20 interviewees did not have a degree from an accredited social work institution. The interviewees had been employed in their current nursing facility as a social worker for an average of 3.2 years, with a range of 2 months to 11.5 years, and a median of 2.5 years. Their overall experience in the nursing facility social work role averaged 8.8 years, with a range of 2 to 30 years of experience, and a median of 7 years. One interviewee did not provide the number of years of experience in their current nursing facility, or his or her total years of experience in the nursing facility social work role. Although all the social workers provided responses to compromised behavioral health issues, 14 (n = 70%) of the 20 included this role as part of their social worker job description.
Behavioral Responses Identified
Social workers in long-term care encounter a plethora of resident behavioral situations over the course of their careers, finding that there is always a new and different challenge to be met. A variety of behaviors were identified, which reportedly require social work assessment and intervention. To assist in the examination of these behaviors, a coding classification system was implemented during the data analysis phase. Table 1 displays six categories of resident-compromised behavioral responses that social workers in our sample encountered, including the frequency that these behaviors were mentioned in the interviews. This summation of the data is followed by respondent reflections and quotes. It is important to note that the authors are describing the behavioral responses as close as possible to the narrative given by the interviewee, recognizing that they represent an attempt by the resident to communicate an important need and/or an inadequate provision in the care environment.
Analysis of interview data was facilitated by categorizing the compromised behavioral responses identified by the interviewees. Of the compromised behaviors identified, those classified as physically and verbally aggressive were most frequently cited as a major concern, closely followed by socially and sexually inappropriate behaviors. Nonadherence to care plans was the behavior that interviewees most frequently referred to a medical professional licensed to prescribe medication. These behaviors frequently involved withdrawal or depression.
Physically aggressive and verbally aggressive behaviors
Concerns surrounding physical and verbal aggression were reported as an important focus of both intervention and prevention. At times, the compromised behaviors described were so excessive that law enforcement would be involved or residents may have to be transferred to a facility better able to handle problematic and complex behavioral conditions. Examples of aggressive threats include “If you don’t do something I’m going to kill the social worker!” or “The social worker discharged me from the nursing home and didn’t give me any Oxycodone. I’m gonna go down there and kill her!” One interviewee reported, “We’ve had patients threaten to physically harm staff members before and actually have a knife or some type of weapon and we have actually called the police and the police come out and, if necessary, arrest the patient.” The significance of threats such as these are frequently unexpected by those entering the field and call for a deeper understanding of the internal and external factors that create them.
Verbal disruptions
Verbal disruptions among residents in long-term care are frequently encountered. As was pointed out earlier in this article, the authors are describing the disruptive behaviors without attempting to identify their causes. One respondent said, “The most frequent is definitely the yelling out.” Compromised behaviors such as calling out, complaining, and calling 911 were problematic to staff members, other residents, and may affect family members, as well. Verbally disruptive statements mentioned by interviewees included, “I want to go home. I want to go home. I want my Mama. I want my Daddy” and “Help! Help! Help!”
Passive disruptions
Passive disruptions such as refusal of care were worrisome to interviewees. Unwillingness even though physically able, refusal to participate in activities, medication nonadherence, and declining ADLs were mentioned by social workers interviewed. Interviewees recognized that unmet needs help explain the behavior the staff view as problematic. Summed up by one respondent, “Refusing care or refusing to shower. Refusing to eat. Refusing ADL care. Those kinds of things are seen quite frequently because they want to have some sort of control over their lives.” Enriching social activities are also frequently declined. “They don’t want to play BINGO. They don’t want to come to the living room to watch TV because look at the other people that are in the living room watching TV.” Although nonparticipation is recognizably an option of choice, interviewees observed that isolation and nonparticipation could be symptomatic of depression, which will frequently be treated with medication in combination with counseling, if available.
Socially inappropriate behaviors
Compromised behaviors of a socially inappropriate nature frequently intrude on the rights of other individuals, including other residents, staff members, or those visiting the facility. Several participants expressed concern for protecting the rights of those affected by these behaviors. An interviewee commented, “One person’s rights end when it starts affecting somebody else’s rights, here in the facility. So that’s how we kind of try to explain it to them.” Residents exhibiting social inappropriateness were described by one interviewee as “those that stay up all night and sleep all day and those that are asleep all day and then they’re up all night, keeping everybody else up, roaming in and out of rooms.”
Sexually inappropriate behaviors
Compromised sexually inappropriate behavior frequently intrudes on the rights of other individuals, including other residents, staff members, or those visiting the facility. Several participants expressed concern for protecting the rights of those affected by these behaviors. Discussing the sexually inappropriate behaviors, one respondent said, “Everybody does have a right to not be offended or not to feel uncomfortable.” Another statement was, “One person’s rights end when it starts affecting somebody else’s rights, here in the facility. So that’s how we kind of try to explain it to them.” Concerning sexually inappropriate touching of staff, one social worker stated, “it’s real easy when you’re being lifted out of the wheelchair to just grab wherever you can.” Although residents touching staff in a sexually inappropriate manner does not imply much physical risk, there certainly are risks to resident quality of life and staff job satisfaction
Social Work Role and Responses
Social workers in the sample were asked how they responded to the compromised resident behaviors they identified in Table 1. The researchers organized the social workers’ responses by clustering them within six functions of the behavioral health role they enacted: care management—planning and coordinating the variety of services each resident needs; investigating—determining the factors that contributed to the behavior; mediating—facilitating transactions between the resident, family, and staff; educating—delivering knowledge and modeling helpful behavior; preventing—avoiding the occurrence or reoccurrence of compromised behavior; and advocating—speaking and acting in behalf of the resident engaged in these behaviors.
Table 2 displays the six role functions that social workers in our sample reported when responding to compromised resident behaviors and a range of specific actions associated with each function. It also contains the frequency with which the actions in each function were reported. Care managing and educating were the most prevalent functions of the behavioral health role.
Care management
Care planning and making referrals was reported as an important role for the interviewees in many instances. For example, one social worker noted, “One [role] is to try to care plan the behavior so that staff have a better understanding of how to address the behavior with that patient. And so that we’re all on the same page and [provide] consistent care.” Interviewees reported making referrals to multiple resources, including those outside the agency, as well as inside.
Sometimes I make a referral to [psychologist] and sometimes we make a referral to [name], the psychiatrist, so they can look at the medication, or, we will get in touch with the primary care doctor to see what they want to do. Sometimes if it’s just out of boredom, they can go over to the [facility], the [name] program. And sometimes that helps. And then sometimes just getting them involved in activities here helps.
Investigating
Looking into what actually created a resident behavioral challenge falls to the social worker in many instances. The interviewees reported that they asked several questions as they investigated the factors that explain the maladaptive behavioral response: “What need is not being addressed?” “Does this patient have a urinary tract infection?” “What is their cognitive process? What are they thinking?” “What is preceding the behavior? What is the preceding interaction?” Learning triggers to problematic behaviors was one key to identifying how they might be prevented in the future.
Some interviewees expressed awareness that staff members may be the cause of negative reactions.
In my mind, when I hear someone has hit someone, a patient has hit a staff member, my first immediate thought is, “How did that staff member approach that patient?”. . . If you flipped on a light and came in there and started moving them around and you didn’t say, “Hello. Good morning.” You weren’t polite. You weren’t gentle. You weren’t kind. You were abrupt with them. Of course, they’re going to be abrupt back.
During the course of the investigative phase, clues may be identified, which will allow for formulation of a behavior plan, which will hopefully eliminate or minimize continued trigger behaviors for the resident. “Looking at the time of day it’s occurring . . . what’s the noise level? Do we have two radios going on? That’s very stimulating and upsetting.” Triggers of overstimulation may be easily remedied, but must be identified to be corrected. Whatever the factors associated with the behavior, the interviewees emphasized “focusing on what the problem is” and holding that focus must remain the top priority.
Mediating
Responses to roommate disagreements were at the top of the list of compromised behaviors that require social work intervention in the form of mediation. One respondent noted, “Not getting along. Not working out. Those are generally things that you can work with the two on trying to find ways to be more compatible or, if not, look for alternate placement within the facility.”
When an altercation is between a resident and a staff member, mediation requires skillful social work finesse. “This is something that we’ve had to deal with because as we’re sensitive to the patient and that patient’s needs, we also have to be sensitive to the employee’s needs from a human resources perspective. So, it gets very sticky.” Although mediation seems just a matter of smoothing out ruffled feelings, there may also be an element of advocacy involved on the part of the social worker when it comes to resident–staff issues. “A lot of times, you’re an adversary to staff because you’re advocating for a patient and staff don’t always want to hear it.” A representative view was, “it’s part of our mission here to help set a good example but then also help them see it from all other sides.” Or, as one interviewee stated, “We’re basically like peacekeepers.”
Educating
The interviewees highlighted the importance of the educating function in behavioral health. Although a primary educational responsibility would appear to be directed toward residents, most discussion about education centered on informing staff members in how to best deal with resident behaviors. When speaking about education of residents, one social worker stated, “That can be very, very difficult because normally there is some type of mental impairment that’s keeping them from understanding.” Another facet of education frequently mentioned concerned family members, to ensure that family members had realistic expectations concerning their loved one’s long-term care experience.
Across the board, the interviewees concluded that behavior management is shared by all staff members, necessitating that staff be well informed and adequately trained to handle situations as they arise. One example provided by several interviewees involved helping staff manage their relationship with residents: “We do a lot of educating on how to give care without getting so close to that person and we talk a lot about boundaries and how you speak to someone, how you physically handle someone.”
Preventing
Interviewees’ identification of antecedents to compromised behavioral responses assisted them in preventing the behavior from occurring in the first place. “The difficulty is figuring out how to keep those things from happening again,” said one social worker. Another expressed an interest in “coming up with a plan for future situations like that so that it doesn’t end up in that type of a situation again.” Identification of causation and proactive planning to avoid similar future instances falls to the social worker, according to multiple interviewees.
Advocating
The interviewees highlighted the necessity of the advocating function of the behavioral health role as well. “ . . . I’m a patient advocate. I want what the patient wants,” said one social worker. Another noted being at odds with staff members, due to their advocating function as a social worker—“They don’t always want to be told they’re wrong.” Advocating for residents in regard to other staff and family members was also important, according to several social workers.
Social Work Skills
Social worker interviewees in the sample were also asked about the skills they applied in managing various resident behaviors. The researchers organized the narratives related to skills by clustering their observations into six categories, which we name and define: attention/affirmation/active listening—core intentional awareness of the resident’s needs/concerns and capacity to engage these concerns, assessment—comprehending the diverse and complex factors and processes that contribute to the behavioral concern (the first step in the problem-solving process), behavior management—monitoring and modifying behaviors, building a relationship or familiarity with the resident—knowing the resident’s history and intervening with this knowledge, teamwork—appropriately working together with staff, and redirection—diverting residents from unhelpful or harmful behaviors.
Table 3 displays the six most prominent social work skill sets and specific skills that our interviewees used when addressing compromised behavioral responses. The table also includes the frequency that the social workers reported using these skills.
Attention/affirmation/active listening
These skills rely on maintaining a calm approach while practicing healthy communication and listening techniques. For the purposes of this study, attention relates to how well the social worker listened to, talked with, and provided meaningful connection with the resident. One social worker reported the importance of giving attention to residents to gain cooperation. The social worker stated, “Really knowing what’s going on and paying attention and learning what they’re gonna respond to.” Furthermore, affirmation of residents includes validation, encouragement, and support. A statement one respondent used that displayed affirmation was, “I can see how upset you are.” This same respondent also noted the significance of “ . . . really validating the feelings . . . ” Active listening is another vital social work skill that involves many components such as eye contact, physical gestures, summarizing, and paying attention. One social worker reported that, “Probably the best thing to intervene in a behavior, before it gets out of control, is to use active listening.” This highlights the importance of the skill.
Assessment
Assessment is one of the first steps social workers use in investigating the factors that contribute to the compromised behavior and that inform as their intervention. Assessment can include gathering, synthesizing, and analyzing information. Assessment can also utilize various scales or other tools. For the interviewees, part of assessment includes asking questions and gathering information. One social worker reported, “For one, you gotta know the reason why the behaviors will happen. It has to do with medications? Has to do with changes in the roommate conflicts? Or change of conditions in the body, you know?” Other interviewees reported using more formal tools. For example, one social worker reported, “I have mini-mental status questions or depression scale questions . . . ” Whatever the approach taken in assessment, our interviewees reported that assessment is an integral aspect of supporting resident behavioral health.
Behavior management
The interviewees also highlighted the skill of behavior management. Behavior management includes directly addressing issues, applying both crisis intervention and solution-focused techniques, applying behavior modification strategies, and delivering other nonpharmacological approaches. One social worker reported, “You have to look at why it’s [the behavior] happening, and behavior management in long term care is more looking at passive behavior management than active behavior management.” Another reported, And I like crisis intervention because . . . I know if I get them in the beginning when they are in trouble and that is my window for them to change. If I don’t get them then, if they set back into what they’re used to doing, then I’m not going to get them.
It is evident that the skill of behavior management can encompass many other skills and techniques as well.
Building relationship (familiarity) with resident
Building relationships and familiarity with residents was another essential skill in engaging this population and within this setting, according to interviewees. One social worker stated that, “So gauging the person makes a big difference in the experience of being here for so long. It’s a whole lot easier to address a behavior of somebody I know than a new admission that came in on Friday.” Another stated, “You have to get to know your residents to know how to take care of them. I can’t imagine not knowing all their social history information.” Aside from knowing personal histories, one social worker stated, “That’s where building those relationships becomes so important where you know exactly what each individual resident needs.” These statements highlight the significance of building relationships and familiarity with patients.
Teamwork
Several social workers reported teamwork or reliance on different staff members such as nursing, administrative, supervisory, and activities staff. One respondent expressed that, Just since I am the only social worker and don’t have social workers to communicate with on a daily basis, I really try to engage with the nursing staff that’s in management so we can brainstorm about different ways to help the residents. That’s been so helpful.
Another reported the significance of team meetings and communication. Specifically, the respondent noted, “We have a quality assurance meeting almost weekly and we’re supposed to look at behaviors . . . And that helps a lot if it’s being done routinely and all the disciplines are involved.” These examples display the emphasis on working as a team to meet the needs of patients and manage difficult behaviors.
Redirection
Redirection of residents was another notable skill used by interviewees. In fact, one social worker favored redirection over medication: “Less med, more redirection, more cueing, remove from situation. I think that would be the best way to go.” Another social worker reported, “You still have very basic skills . . . you listen to what they say, you validate, but you just have to redirect or provide the facts of how you can help.” The use of redirection in avoiding similar instances was a helpful technique, according to several interviewees.
Summary of Findings
Nursing facility social workers in our sample enacted a complex array of functions and practice skills related to the behavior management role when responding to a wide range of compromised resident behaviors. An analysis of our interviewees’ narratives offers a preliminary view of the substantial variability and complexity of the experience and practices of social workers who address resident behavioral challenges in the nursing facility setting. The six role functions (Table 2) and six skill sets (Table 3) map the range of responses that our social workers enacted to address the behaviors (Table 1) they reported. Our findings document that social workers do intervene to improve the behavioral health of residents while also practicing at the mezzo (family) and macro (advocating for resident’s rights and staff education) levels. Their involvement in resident behavioral health is enacted through balancing attention to the resident’s presenting behavioral concern and to the familial, social, and organizational context in which the behavior is occurring.
Discussion
The interviewees’ narratives map the path social workers in nursing care faculties follow in navigating the ambiguity of their initial encounter with a resident’s compromised behavioral response to how they individualize their role performance and intervention to restore or at least strengthen resident behavioral health. Immersion in their stories yields several observations about the micro and macro aspects of the behavioral health role of social workers in this setting.
Micro Aspects of the Behavioral Health Role
Not surprisingly, the compromised behaviors they reported are consistent with many other studies of these behaviors based almost exclusively on the reports of nursing care staff (Kolanowski et al., 2011; T. Rosen et al., 2016). This consistency verifies the reporting of our interviewees. What has not been previously reported for licensed BSW or MSW social workers are the ways they transparently experienced resident’s behaviors, including the satisfactions, personal maltreatment, and frustrations of doing this kind of work. In spite of the challenges they documented, none of the interviewees expressed responses that marginalized the residents or focused on blaming them. They seemed to adhere to standard practices around dealing with aggression in PLWD (Whall et al., 2008), stressing the importance of paying close attention to the resident as a unique individual. True to the values of the profession and their person-in-environment focus and the principles of the NBD model (Algase et al., 1996), their narratives revealed an immediate activation of the investigating function, seeking resident need and care environment explanations for the compromised behavior for the sole purpose of framing an informed, behavioral health-promoting response. Although the interviewees identified specific evidence-based modalities for dealing with compromised behaviors of residents, it was very evident that basic, generalist practice micro skills served them well in their responses. Active listening and redirection (reframing) stand out as having particular salience.
Macro Aspects of the Behavioral Health Role
Their observations on enacting the macro aspects of the behavioral health role also included reflections on organizational barriers and their aim to improve the responsiveness of the care environment. Although there was variability in the extent to which these components were enacted by individual social workers, their narratives documented the facilities’ overarching reliance on their assistance and intervention in addressing compromised behaviors. The most common negative response when interviewees were asked about the nursing facility stemmed from not feeling supported or appreciated by the facility’s direct care staff and administration. “It would be nice to feel appreciated for making certain things happen and when I don’t feel supported in that way, I really have a hard time wanting to come the next day,” said one social worker. The element of time is an additional factor of concern. “With more and more paperwork being demanded, it’s just hard because we have less and less time doing what we came into the field to do,” said a respondent. “That’s why we burn out so fast is because we don’t get the thing we love [working with the residents].”
In spite of these challenges, their macro interventions included both advocating for the resident experiencing compromised behavioral responses, even risking conflicted relationships with other staff, and working with nursing care staff to improve their responses to the residents. As noted in other studies (Lachs et al., 2016), nursing facility social workers in our sample equipped direct care staff to address resident behavioral health. A prominent aspect of the interviewees’ contribution to resident behavior modification was the instruction and role modeling they provided to direct care staff to improve care planning and resident engagement. This finding is congruent with multiple studies cited in the review of literature, which report that compromised behaviors are more effectively managed when staff members are instructed in various methods of intervention. Kolanowski et al. (2010) posited that although additional staff training would be helpful in decreasing problematic behavior situations, time and financial constraints are frequently cited as making the training difficult to achieve.
The relatively informal coaching approach to training demonstrated by the social workers in our sample may be a way to address these constraints. An additional benefit of training staff in best practices for preventing and managing behavioral disruptions is improvement in overall staff job satisfaction. The evidence that leadership in staff development is a natural component of the social worker’s behavioral health role suggests that this topic needs to become an integral part of BSW and MSW curricula and continuing education offerings.
Educational Initiatives
Nursing facility social workers in our sample called for new educational initiatives to strengthen competency in resident behavioral health management. Fortunately, social workers, administrators, researchers, and educators involved in residential long-term care have the benefit of comprehensive and helpful guides for social work practice in this setting (Beaulieu, 2012; Brody, 1974; Perrin & Polowy, 2008; Sahlins, 2010). Social workers responsible for managing compromised residential behaviors can also benefit from knowledge of therapeutic pharmacological and nonpharmacological interventions. Although resources for the nursing facility social worker are readily available, our interviewees reported a significant interest in greater preparedness and instruction to increase their capacity to effectively address compromised behaviors. The majority of social workers interviewed indicated that the skills they use in the management of compromised behavior were acquired through years of work experience rather than during their social work degree programs. Those interviewees who felt most prepared had previously served in another social work capacity, such as working with juveniles, in a prison, or in a mental health setting.
Social work education cannot prepare current and future practitioners for every unique occurrence, which they may face in enacting the behavioral health role. To the extent that the findings of this study are validated by further research, educators will be provided with evidence to inform educational initiatives around preparation for effective resident behavioral health practices. For example, educational offerings may focus on managing compromised behaviors involving physical and verbally aggression (Table 1), enacting the care manager and educator dimensions of the behavioral health role (Table 2), and practicing affirmation, active learning, and assessment skills (Table 3). It is essential that instructional and internship learning aimed at readiness for practice include demonstration of behavioral interventions and opportunities for feedback on skill performance.
Although the gap between learning needs and educational resources hinders effective practice in this area (Bern-Klug et al., 2016), the profession has an educational infrastructure in place to respond to the specialized knowledge and skills requirements. For example, social work education and the NASW are making significant contributions toward preparing generalist and specialized practice students for social work in an aging society. We echo the call by Bern-Klug et al. (2016) for heightened attention to preparing social work students for practice within residential, long-term care settings.
Continuing education offerings can be effective avenues for instructional support for the unique demands of behavioral health within the nursing facility context. Educational preparation needs to be based upon a clearer understanding of the key knowledge, competencies, components, ethical dilemmas, and skills related to the behavioral health role. Several of our interviewees reported application of cognitive behavioral therapy (CBT), solution-focused, crisis intervention, and behavior modification approaches. Social work students and graduates will benefit from direct exposure to practice proficiencies of experienced practitioners through guest lecturers, internship supervision, and case studies.
These practical and accessible continuing education opportunities are just as essential as the formal course offerings in a BSW or MSW degree plan. Interviewees identified the following as priority areas for continuing education: family dynamics, counseling, de-escalation techniques, disease processes, death and dying, personality disorders, behavior modification, geriatric psychology, and the basics of documentation. State and local professional associations, administrators of nursing facilities, medical centers interested in reducing readmissions, or social work education programs may provide the resources needed to energize collaborative meetings that offer a venue for consultation and conversation about best practices as well as relational support for one another.
Educational technologies contribute significantly to the development and delivery of practice content and learning opportunities. Web-based and other platforms for distance education offer asynchronous or synchronous instruction that go a long way in overcoming time and distance barriers. For example, substantive and relevant webinars that address behavioral management for nursing home social workers are offered by University of Iowa; see https://clas.uiowa.edu/socialwork/nursing-home-social-work-network. Blogs and other communication threads can overcome the challenges of solo practice and disseminate innovations in real time. Visual skill demonstrations can be produced, with proper protection of resident confidentiality, utilizing digital recording and even virtual reality technologies. Fortunately, a widely utilized and very informative national list serve is available as an access point for colleague expertise and support: http://www.uiowa.edu/wsocialwk/NursingHomeResource/index.html
Proposed Competencies
More precision in identifying best practices and developing competency are contributions of this line of research. Historic and current practice standards and competency statements provide general guidelines for the social worker’s specialized behavioral health role (Harahan, Stone, & Shah, 2009; National Association of Social Workers, Massachusetts Chapter, 1997; Simons, Bern-Klug, & An, 2012). NASW’s (2003) standards for social work services in long-term care facilities prescribe guidelines that broadly govern behavioral health interventions by social workers. Also, there are competencies for gerontological social work practice in general (not setting specific) that have been rated by practicing social workers (A. L. Rosen, Zlotnik, Curl, & Green, 2000).
Unfortunately, these standards and competencies do not clearly define expectations and competencies for the nursing facility social worker involved in resident behavioral health. This study’s description of the functions of the behavioral health role and the skills used to implement them begins to addresses this need for greater clarity.
The findings provide initial evidence for developing competencies relevant for the educational preparation of nursing facility social workers enacting the behavioral health role. These competencies are applicable for specialized MSW practice preparation or a specialized practice certificate offering. The following are examples of these competencies along with instructional suggestions:
Recognize and respond effectively to resident behaviors that adversely affect their behavioral health. Applying the typology of compromised behavioral responses (Table 1), provide opportunities for students to experience simulations of each response and participate in demonstrations and skill development aimed at informing an immediate response.
Apply generalist practice micro skills of engagement, assessment, and intervention to promote resident behavioral health. Use the evidence-based, helping skills typology developed by Shulman (2016) to provide students with a range of helping skills to support the enactment of the dimensions of the behavioral health role identified in Table 2. These skills include focused listening, questioning, demand for work, reframing, and contracting that center the behavioral health social worker on the needs, assets, and aspirations of the resident, and increase the likelihood of meaningful engagement.
Create and sustain effective transactions between the resident and the care environment. Applying the ecological perspective, provide case illustrations of how nursing facility social workers work with an interdisciplinary team to match resident needs/interests/assets with the resources and limitations of the care environment, thereby increasing the likelihood of healthy behavioral responses.
Review and critically evaluate evidence-informed approaches for promoting resident behavioral health. Offer knowledge and skills that support students’ capacity to locate, evaluate, and consider implications for their practice of models and research related to resident behavioral health.
Improve the capacity of direct care staff to nurture and sustain resident behavioral health. Using training materials and instructional strategies that work in the complex context of the nursing facility, teach students how to engage staff in ways that motivate learning, address the administrative and organizational barriers, and increase the likelihood of application to residents.
In addition, the findings can inform discussions between social workers and facility administrators to help reduce some administrators’ uncertainty about the role of social workers in fulfilling the organization’s responsibility to attend to the psychosocial needs of residents (Bern-Klug & Kramer, 2013). These findings can inform discussions among facility administrators and social workers about the appropriateness of direct social worker involvement in behavioral health and their competency to perform this function. Clarifying social workers’ scope of practice within this setting can decrease social workers’ vulnerability to facility-imposed role restrictions.
Limitations of the Study
Two facets of the research methods restrict the extent to which the narratives of the interviewees are representative of the experiences of their peers in other residential long-term care settings and locations. Although at least one social worker was enlisted from the four main types of 120-bed LNFs (private, nonprofit; private, for-profit individually owned/limited partnerships; private, for-profit corporately owned; private, and for-profit medical center–affiliated), the sample was drawn from only one catchment area in a southwestern region of the United States. Also, the significance of the social worker’s training and experience in dealing with compromised resident behaviors was not considered in the analysis.
Even in the context of these important cautions, the in-depth reports from interviewees who were immersed in the realities of this practice setting provided in-depth insight to the compromised behaviors they experienced and responses they enacted in a way unprecedented in the literature. The findings from this qualitative study provide a sturdy platform for more representative studies that broaden the scope of inquiry with a mixed-method design, so this line of research will have greater impact within the field.
Conclusion
Based on the findings from 20 in-depth interviews in residential long-term care facilities, licensed BSW and MSW social workers are actively engaged in addressing compromised resident behaviors and play a key role in a facility’s mandate to provide the highest practicable level of resident psychosocial well-being (Bonifas, 2015). A close examination of their narratives reveals that they offer unique assets as behavioral health managers that include the following: balanced attention to transactions between the resident and the care environment, effective relational skills, capacity to identify behavioral strengths and triggers, delivery of behavioral change technologies, staff education and motivation, and participation in team initiatives to prevent occurrence or recurrence of unacceptable behaviors. With adequate training, prevention of compromised and difficult-to-manage behaviors can result in an increase in both resident quality of life and staff employee satisfaction, as well as substantially improve the facility’s climate. Interviewees find satisfaction in this aspect of their work when they experience support from other staff and facility leadership. Full activation of these assets is constrained by significant barriers that include insufficient preparation for competent behavioral health responses, lack of uniformity in responsibilities across facilities, inadequate educational support, and uncertain competency performance expectations.
In spite of these and other constraints, such as overwhelming caseloads and staffing reductions, the social workers in the study documented time and time again their commitment and competency when called on to address challenging resident behaviors. Increased numbers of more competent social workers will be required to engage the behavioral health needs of the wave of aging Baby Boomers already transforming nursing facility operations and care. The first step in unleashing these assets is to fully understand and empower social workers as resident behavioral health managers. The findings of this study were intended to contribute to this vital enterprise.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.