
Abstract
Introduction
The statistic of one in three community-dwelling adults aged 65 and older falling each year is well cited (Stevens, Baldwin, Ballesteros, Noonan, & Sleet, 2010). Despite a growing understanding of fall incidence and risks (Stevens et al., 2010), national assessments of the burden of falls among residents of residential care settings are insufficient. Studies have identified risk factors for falls among residential care facility (RCF) residents, including disease and drug side-effects (Kallin, Jensen, Olsson, Nyberg, & Gustafson, 2004), which in some cases are predictable using a fall risk index (Rosendahl et al., 2003). In addition, fall patterns vary by location within facilities such as in nursing homes (e.g., in resident rooms or bathrooms) and during different activities (e.g., transfers, walking (Rapp, Becker, Cameron, König, & Büchele, 2012)). Fall incident rates likely differ when comparing across settings given differences in mobility and frailty (Vu, Weintraub, & Rubenstein, 2006). For example, earlier evidence suggests the rate of falls in nursing homes (50%-75%) was nearly twice that of community-dwelling adults (30% (Rubenstein, 1997)). Residential care facilities are along the continuum between living in one’s own private home in a community setting and living in a nursing home. More specifically, residential care facilities provide limited assistance for activities of daily living (ADLs), but do not provide more advanced skilled care as one may receive in a nursing home (Towne, Lee, Li, & Smith, 2015). Thus, those entering these facilities may choose to do so based on potential need of assistance with ADLs, which is also predictive of greater fall risk (Stenhagen, Ekström, Nordell, & Elmståhl, 2014). Furthermore, facility characteristics such as size, ownership type, and other factors have been shown to be associated with differences in the types of resources (e.g., electronic health records, electronic health information exchange with pharmacies and physicians) available to residents of residential care facilities; (Caffrey et al., 2012; Park-Lee, Rome, Caffrey, & Harris-Kojetin, 2013; Towne et al., 2015)). Thus, structural and organizational facility characteristic may be associated with the resources available to care for residents of residential care facilities. These may also include fall prevention strategies.
Fall prevention efforts in residential care facilities have been shown to be effective in Europe (Jensen, Lundin-Olsson, Nyberg, & Gustafson, 2002a; Jensen, Nyberg, Gustafson, & Lundin-Olsson, 2003), yet more work is needed across the United States. There is, however, a large and robust body of literature that highlights the critical need and potential solutions to falls among community-dwelling older adults. Many transferrable lessons can likely be gleaned from these efforts. The national dissemination of evidence-based fall prevention programming is one example of multicomponent solutions. In particular, A Matter of Balance has been highlighted as an evidence-based health and wellness program targeting cognitive restructuring to improve older adults’ confidence in their ability to prevent falls (National Council on Aging, Center for Healthy Aging, n.d.; Smith, Ory, Belza, & Altpeter, 2012; Tennstedt et al., 1998) and has been disseminated nationally (Towne, Smith, et al., 2015). In addition, Tai-Chi Moving for Better Balance has also been shown to be associated with improvements in participants’ functional status and other health-related outcomes related to falls and has been successfully delivered in a community setting (Ory et al., 2014). In addition, multifactorial fall prevention programs have been shown to be effective (e.g., improved balance, mobility) for older community-dwelling adults (Shumway-Cook et al., 2007) and have been shown to be effective for older adults with a history of falls (Costello & Edelstein, 2008). Fall prevention efforts can also extend into other settings outside the community.
Fall prevention efforts have been targeted by clinicians (Shubert, 2011) in clinical settings. Otago, a program targeted at fall prevention, has been successfully translated from New Zealand and delivered by physical therapists in the United States (Shubert et al., 2014). In addition, STEADI (Stopping Elderly Accidents, Deaths, and Injuries) has been developed as a toolkit for clinicians used in clinical settings for fall prevention (Stevens & Phelan, 2012). Thus, fall prevention efforts have been successfully targeted at multiple settings (e.g., facility, community-based, clinical).
More research is needed to identify the burden of falls in RCFs, especially as the population ages and more older adults are residing in these care facilities (Spillman, 2008). Those in older age groups are more vulnerable to functional decline, especially if they have comorbid conditions (Colón-Emeric, Whitson, Pavon, & Hoenig, 2013). Thus, RCF residents, the majority of whom are older, may be a particularly vulnerable population (Caffrey et al., 2012). Additional efforts are needed to examine the magnitude of injurious falls among this population, recognize risk factors, and identify solutions to prevent such occurrences. This is especially important as this population represents well over 700,000 individuals (Caffrey et al., 2012) or nearly 2% of those aged 65 and older in the United States (U.S. Census Bureau, n.d.-a).
In 2010, approximately a quarter million adults over the age of 65 experienced a hospitalization related to a hip fracture (National Hospital Discharge Survey, National Center for Health Statistics, n.d.; Stevens & Rudd, 2013). The rate of hip fractures is expected to rise by almost 12% from 2010 to 2030 for those aged 65 and older (Stevens & Rudd, 2013). Hip fractures are among the most commonly occurring fall-related injuries, yet other fractures and injuries occur (e.g., upper and lower extremity injuries, traumatic brain injury, chest injury, spine fracture, rib fracture (Soffer et al., 2006)). Risk factors for hip fractures and other fall-related injuries are similar to that of falls, in general, and include advanced age, impaired cognition, and disease (Soffer et al., 2006; Taylor et al., 2004), which are common among residents of a RCF (Caffrey et al., 2012). While the risk of serious injuries related to a fall is present, the majority of injurious falls may result in less severe injuries (Jensen, Lundin-Olsson, Nyberg, & Gustafson, 2002b; Sadigh, Reimers, Andersson, & Laflamme, 2004).
Objective
Health-related outcomes are an interaction between one’s individual characteristics and one’s environment (Bandura, 2001; McLeroy, Bibeau, Steckler, & Glanz, 1988). Thus, identifying characteristics of individuals and facilities at multiple levels provides a more complete picture (e.g., capturing factors that may be associated with our outcome), than failing to account for contextual characteristics in analysis of individuals’ outcomes. The current study sought to evaluate the latest available data on RCF residents, highlighting rates of injurious falls among this vulnerable population. This population is understudied relative to community-dwelling adults or residents of skilled nursing facilities (Mei, Marquard, Jacelon, & DeFeo, 2013). Nationally representative studies of residents of RCFs have only recently been made available. To our knowledge, this is one of the first nationally representative studies measuring injurious falls among residents of RCFs. Thus, this study has the potential to make a significant contribution to the scientific literature about injurious falls in RCFs across the US.
Materials and Method
Study Subjects, Data, Study Design
This study used a nationally representative sample of RCF residents. A RCF was operationally defined as “assisted living residences, board and care homes, congregate care, enriched housing programs, homes for the aged, personal care homes, and shared housing establishments”(Mei et al., 2013). The 2010 National Survey of Residential Care Facilities (NSRCF) public-use file was used to conduct a cross-sectional analysis. The data were collected as part of a Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) study to survey RCFs and residents. A stratified two-stage probability sampling design was employed with the first stage including facility sample selection (sampling frame, n = 39,635) and the second stage consisting of resident sample selection (sampling frame, n = 733,309; Moss, 2011). The unit of analysis was the adult resident (unweighted n = 8,094; weighted n = 733,309). In our fully adjusted analysis, we excluded adults under 65 years of age, which in combination with missing values for our other independent variables reduced our final sample size to 387,873 individuals (unweighted n = 4,841). This allowed us to focus on older adults, those most at risk for falls (Stevens et al., 2010). All analyses were carried out with public-use files available on the CDC website (http://www.cdc.gov/nchs/nsrcf.htm) in accordance with NCHS, CDC guidelines. No human subjects were enrolled or contacted by the research team.
Measures
Dependent variable
The outcome of interest was whether a resident experienced a fall with an injury in the past 12 months. RCF staff were prefaced with the following “This question refers to the past 12 months/# months since sampled resident moved into this residential care facility” which was then followed up with a question about falls (CDC, 2014). The two fall-related questions asked through the NSRCF included “During this time, has [RESIDENT INITIALS] had a fall that caused an injury other than a hip fracture?” and “During this time, has [RESIDENT INITIALS] had a fall that caused a hip fracture?”(CDC, 2014). Resident data were obtained from either facility directors or caretakers with reference to a resident’s medical or other records where appropriate to limit potential recall bias. Due to the small number of hip fractures (n = 130, unweighted), we combined two variables, falls resulting in hip fractures and falls resulting in injuries without hip fractures (n = 1,021, unweighted) into one variable. This provided a dichotomous outcome of experiencing an injurious fall or not experiencing an injurious fall in the past 12 months or the time since the resident entered the facility (i.e., if they lived in the RCF for less than 12 months). Here, only injurious falls that occurred while a resident of the RCF were recorded. The type of injury resulting from a fall is not provided in the public-use file used in our analysis.
Independent Variables
We included several variables into our multivariate analysis identified using the Social Ecological Theory first proposed by McLeroy and colleagues (1988) and later refined by numerous researchers (Satariano, Ory, & Lee, 2012). In our model, we used individual characteristics (age, sex, race/ethnicity, education, Medicaid status, and need of assistance with ADLs), interpersonal factors (participation in social activities), institutional factors (size, chain affiliation and ownership type), and community factors (rurality). Individual characteristics were reported through health care workers or other facility representatives on behalf of the resident. Age was grouped in the public-use file for those 18 to 64 and those 85 and older. We separated age into the following categories: 65 to 74 years of age, 75 to 84 years of age, and 85 years of age and older. Race/ethnicity was defined as Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, or non-Hispanic Other. Education was defined as having a high school diploma or less versus some college or more. Medicaid status was defined as having any of the residents’ long-term care services at the facility paid by Medicaid in the past 30 days. Need of assistance with ADLs was defined as needing assistance with at least one ADL or not.
Staff was asked about the resident’s participation in 14 activities (playing board games, making arts and crafts, exercising or participating in sports, playing or listening to music, reading/writing, doing spiritual or religious activities, shopping or going on trips, watching television, leaving the facility grounds, talking with friends or relatives, going out to the movies, gardening, taking care of pets, other hobbies; participation defined as at least twice a month), each of which was scored dichotomously (yes/no). For the purposes of this study, social engagement of the residents was of interest; thus, activities performed independently were excluded (e.g., taking care of pets, leaving the facility grounds, watching television). Only six activities deemed to be interpersonal and not limited to leaving the facility grounds were identified for inclusion in study analyses, which was then confirmed using exploratory factor analysis (EFA). The six social engagement activities included playing games (e.g., cards, puzzles), making arts and crafts (e.g., knitting, painting), exercising or participating in sports, playing or listening to music, doing spiritual or religious activities, and talking with friends or relatives. EFA was performed using a varimax rotation in SPSS. Only one factor was identified with 40.11% of the total sum of eigenvalues. Internal consistency reliability analysis of these six activities yielded a coefficient of α = .70. Participation in activities were summed to create a score ranging from 0 to 6, where 0 was assigned for no participation, while a 1 was assigned for participating in only one activity and so forth, up to six. The average of this measure was 3.54 for all age groups; 3.19 for those 65 to 74 years of age; 3.55 for those 75 to 84 years of age; and 3.61 for those aged 85 and older.
Institutional factors included characteristics of the facility. Facility size was defined as small (4-10 beds), medium (11-25 beds), large (26-100 beds), and extra large (more than 100 beds). However, analysis that includes rurality excludes extra large facilities, as these facilities were assigned a missing value for rurality in the public-use file. Chain affiliation was defined as whether the facility was owned by a chain, group, or multifacility system. Ownership type was defined as either private, for-profit versus private, non-profit or state/county/local government. Rurality was used as a proxy for the community setting of facilities. This was separated in a two-level variable. We defined rural as being located in a non-metropolitan statistical area, whereas urban was defined as being in a metropolitan statistical area(U.S. Census Bureau, n.d.-b).
Statistical Analysis
Analyses were performed with SAS 9.4 (SAS) using procedures to account for the complex sampling frame of the NSRCF data (Chen, 2006). All analyses were conducted with appropriate survey methodology, while incorporating the nested nature of individuals within facilities. Specifically, the Facility Identification (ID) Number was used as the cluster variable in SAS survey procedures. We used multivariate logistic regression to assess the likelihood of our outcomes (i.e., predicting a fall with an injury). Chi-square tests were used for bivariate comparisons.
Study Results
Table 1 provides selected characteristics of residents of RCF. Overall, the majority of RCF residents were female (69.6%), had a high school education or less (59.4%), and were White individuals (91.1%). Approximately 19% of residents of RCF had some portion of their bills paid by Medicaid in the past 30 days. The majority of residents were in need of at least one ADL regardless of older age, where 69.2% of residents were in such need.
Sample Characteristics by Age Group.

Table 2 provides the rates of injurious falls by selected characteristics. Males had lower rates of injurious falls by a margin of 5.6% when compared with females. Black or African American Adults had the lowest rates of injurious falls, when compared with all other racial or minority groups at 5.5%. Adults in need of assistance with at least one ADL living had higher rates (17.5%) of injurious falls when compared with those not requiring ADL (9.4%). Adults participating in social interactions had higher rates of injurious falls (15.7%), compared with those not participating in these activities (12.1%). In addition, residents in smaller facilities (small or medium) had lower rates of injurious falls (11.2%) as compared with those that were in larger facilities (large or extra large; 15.9%).
Frequency of Injurious Falls by Selected Characteristics.
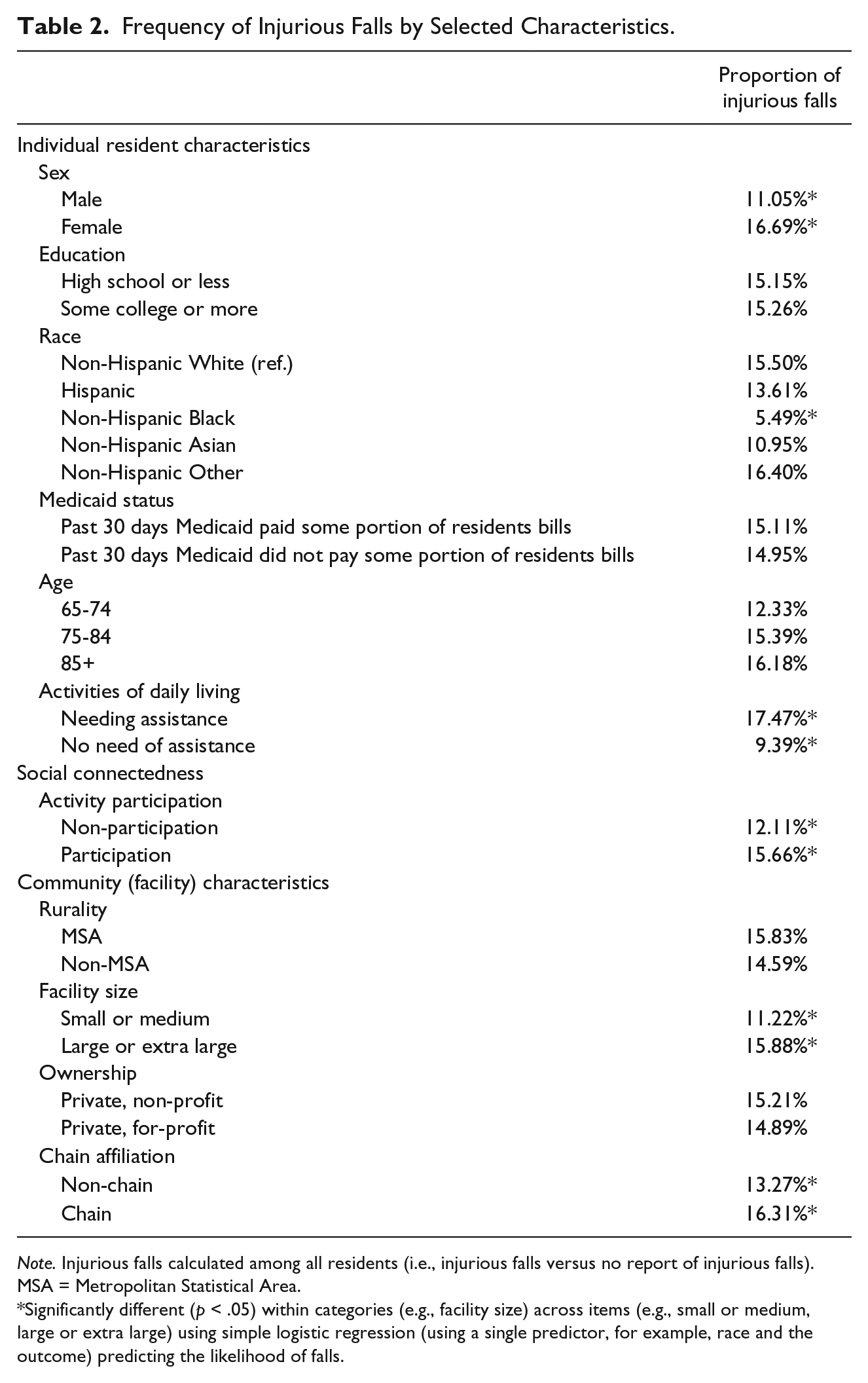
Note. Injurious falls calculated among all residents (i.e., injurious falls versus no report of injurious falls). MSA = Metropolitan Statistical Area.
Significantly different (p < .05) within categories (e.g., facility size) across items (e.g., small or medium, large or extra large) using simple logistic regression (using a single predictor, for example, race and the outcome) predicting the likelihood of falls.
In 2010, 15% of RCF residents had an injurious fall. Rates of injurious falls were 16.2% for those aged 85 and older. We used logistic regression predicting the presence of an injurious fall. The fully adjusted model accounted for several social ecological factors (Table 3). The increased presence of a injurious fall was associated with being female (less likely for males, aOR = 0.7, confidence interval [CI] [0.57, 0.91]); being in need of assistance with at least one ADL (aOR = 1.9, CI [1.43, 2.41]); and residing in a facility that was large or extra large (less likely for small facilities, aOR = 0.7, CI [0.55, 0.84]), even after controlling for individual characteristics (race, sex, education, age, need of ADL, and Medicaid status), interpersonal factors (participation in social activities), institutional factors (size, chain affiliation, and ownership type), and community factors (rurality).
Adjusted Analysis Predicting the Presence of a Fall Resulting in an Injury in the Past 12 Months.
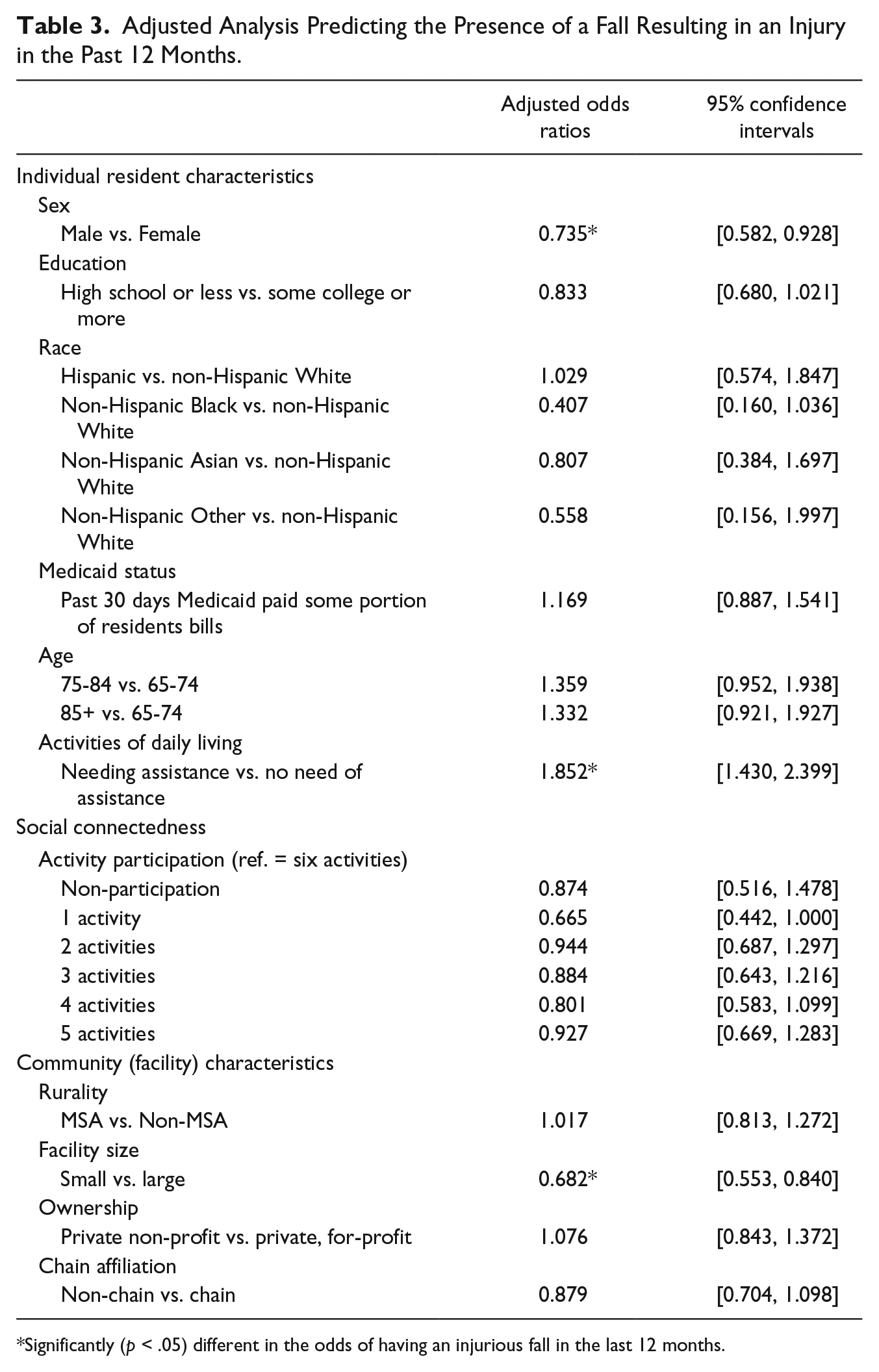
Significantly (p < .05) different in the odds of having an injurious fall in the last 12 months.
Discussion
Conclusions
We identified, throughout the United States, three out of 20 RCF residents experienced an injurious fall in 2010. While we do not have data on the type of injury, analysis of falls in community-dwelling older adults (aged 65 and older) indicates falls (n = 204) result in physical injury in almost 70% of fall cases, whereas only 5.9% result in major injury and 35.3% experienced functional decline (Stel, Smit, Pluijm, & Lips, 2004). Residents of nursing homes experienced significant injuries from falls at a rate of 11% in early studies (Rubenstein, 1997) and may result in hospital admission or fractures for 10% to 25% of nursing home residents (Rubenstein, Josephson, & Robbins, 1994; Vu et al., 2006) and may be higher among women (Benzinger et al., 2013). The settings vary (i.e., community-dwelling or nursing homes versus RCF) and likely result in differing outcomes heavily influenced by resident’s baseline demographic and health characteristics. However, we posit that injurious falls in RCF are likely somewhat similar with regard to the type of injury sustained from falling among older adults with similar characteristics. The impact of falls resulting in injury can be measured with regard to the actual medical costs for fall-related treatment (Smith et al., 2010) or in the time needed for recovery or other non-medical costs.
To our knowledge, our findings are the first to be drawn from a nationally representative sample of RCF residents. Thus, these findings shed greater light on a relatively understudied population. Those most at risk for injurious falls included females, those in need of assistance with at least one ADL, and those residing in larger facilities. Our study identifies facility size as a possible predictor of falls, which is a novel finding, as less research focuses on facility characteristics. More research is needed to identify why smaller facilities serve as a protective factor for injurious falls (e.g., ability to monitor and track residents easier (Struksnes, Bachrach-Lindström, Hall-Lord, Slaasletten, & Johansson, 2011)). Furthermore, understanding the role of staffing ratios in relation to facility size should also be explored in future research given the differences in facility size and fall risk in the current analyses. In addition, staffing protocols and other policies may differ among facilities and settings. This level of detail was not available in the data from the NSRCF and therefore we were unable to incorporate these nuances in the current study. In prior research focusing on nursing homes, successful multifaceted falls prevention programs included staff education among other targets (e.g., environmental assessments, environmental modifications), which indicate the importance of staff engagement in fall prevention efforts (Vu et al., 2006). Further research should incorporate information on these facility characteristics where possible. In addition, identifying what can be done to aid those in need of assistance with ADLs to prevent injurious falls may shed light on strategies to reduce the overall rate of injurious falls among this population.
Evidence-based programs have been shown to improve falls efficacy and reduce fall risks among community-dwelling older adults including those with multiple chronic conditions and functional limitations (Smith, Ory, & Larsen, 2010), whereas other studies have shown the utility of falls prevention interventions in nursing homes (Vu et al., 2006). What is unknown and remains to be further studied is whether interventions traditionally seen in community-dwelling adults—or those in skilled nursing facilities—will be equally effective in a RCF. Evidence from the Administration on Aging’s national dissemination of chronic disease self-management education (CDSME) programs shows that residential facilities account for almost 20% of the delivery sites, which suggests there may be growing receptivity to evidence-based disease prevention programs in RCFs (Smith et al., 2014).
Limitations
This study looks at injurious falls dichotomously and cannot ascertain factors associated with multiple falls or the severity of injuries. The survey assessed falls that “caused an injury other than a hip fracture” and those that did cause a hip fracture; however, the specific type of injury (e.g., leg fracture) was not recorded. This limited our ability to assess common injuries caused by falls, although it still enabled us to identify injurious falls versus all else (CDC, 2014). The number of comorbidities, the number of previous falls beyond a year or even before living in RCF, the number/type of medications, and information about current fall prevention initiatives or programs at facilities or staff training in falls prevention is missing from the survey and suggest areas for additional study. We were unable to identify potential environmental risk factors (e.g., lighting, bathroom modifications) within facilities, and recommend this requiring further study. Furthermore, these questions were asked of facility staff and not reported by individuals. However, the questions were consistent (e.g., same definitions/wording for questions) across respondents. In addition, facility staff referred to residents’ medical charts where appropriate which reduces the likelihood of recall bias. Given the possibility of cognitive impairment seen in some older adults residing in residential facilities, this is likely more accurate, even with possible underreporting of less severe falls (Department of Health and Human Services, 2007) or incomplete data in incident reports (Silva-Smith, Kluge, LeCompte, & Snook, 2013). Finally, this study was cross-sectional, which prevented causal interpretation or analysis of trends over time. However, this is the first nationally representative data set measuring health outcomes of RCF residents, which allows us to provide analysis on a scale not previously available.
Implications and Practical Applications
The number of older adults in RCFs is expected to grow dramatically over the next few decades (O’Keeffe, O’Keeffe, & Bernard, 2003). As this population grows, the need to understand what works in preventing falls, and by extension injurious falls, is critical for maintaining older adult’s health and functioning. Despite comprehensive reviews of evidence-based fall prevention interventions, there is a lack of conclusive research surrounding the effectiveness of multifactorial falls prevention programs in RCFs (Cameron et al., 2012). It is promising that multifactorial falls prevention programs have been shown to result in reduced falls and reduced falls risk in other settings (Ory et al., 2010). This includes multifactorial interventions in nursing homes, which have been shown to be associated with reduced recurrent falls (Ray et al., 1997). Preventing falls among adults aged 65 years and older in RCF has been shown to be effective using multidisciplinary fall prevention programs in a small study in Sweden (Jensen et al., 2002a). Future studies are needed to identify whether multifactorial fall prevention programs are successful at reducing falls in residential long-term care settings throughout the United States. This information may be used to inform interventions at the local level where fall prevention programs are being implemented, often promoted by state fall prevention coalitions (National Council on Aging, n.d.).
Clinical guidelines (2010) with regards to assessments (during encounters with providers) and screening (e.g., yearly screening for history of falls and gait/balance difficulties) may play a critical role in successful falls interventions in clinical settings, especially among geriatricians (Kenny et al., 2011). Other research suggests participation in exercise physical therapy–based falls prevention interventions is effective at preventing falls among older adults (Michael et al., 2010). Thus, better coordination of clinical interventions into RCF settings has the potential to improve falls prevention among older adults living at high risk for injurious falls.
Falls among older adults are estimated to cost (direct and indirect costs of fall injuries) $67.7 billion by 2020 (CDC, n.d.; Englander, Hodson, & Terregrossa, 1996). Thus, policy makers are very interested in finding ways to lessen fall-related expenditure. Medicare funding for evidence-based fall prevention programs has been suggested as a cost-effective strategy to lower annual health care costs (Wu, Keeler, Rubenstein, Maglione, & Shekelle, 2010). More broadly, Rand Corporation modeled the potential cost-effectiveness of a falls prevention rehabilitation program which included multifactorial risk assessments and tailored recommendations, in addition to supervised exercise programs among Medicare beneficiaries (Shekelle et al., 2003). While dated, results of this analysis indicated that 542,000 falls with injury could be prevented at a cost of $500 (average cost per fall prevented) with an annual net cost of $272 million to Medicare in 2002 (Shekelle et al., 2003). In addition, a recent report to Congress presented cost savings (i.e., less unplanned hospitalizations and lower inpatient costs) for A Matter of Balance (AMOB), an evidence-based fall prevention program (Centers for Medicare and Medicaid Services, 2003). Falls prevention interventions that focus on the aging population and those on Medicare also target individuals who may benefit most from improvements in fall prevention strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Cooperative Agreement from the Centers for Disease Control and Prevention (CDC) to one Prevention Research Center participating in the Healthy Aging Research Network Special Interest Projects, the Texas A&M University (CDC #U48 DP001924). The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the CDC.