
Abstract
In a context of growing demand for home-based direct care services, the need to retain direct care workers (DCWs) is clear. The Patient Protection and Affordable Care Act, changes to the Fair Labor Standards Act, and state-level changes in Medicaid support for home-based care together have affected agencies that hire DCWs, with implications for an issue that affects worker satisfaction: scheduling. Many home-based aides employed by agencies cannot count on consistent or sufficient hours. Hours shortfall and instability have been recognized as important issues for retail and restaurant workers, but focused on less for care aides. This study uses semistructured interviews with agency representatives to examine these issues from an employer perspective, with a focus on how the competing influences of health care, labor, and employment policy shape scheduling and a review of how recommendations for changes in policy and practice in other sectors might apply to home care.
The need to recruit and retain direct care workers (DCWs) working in homes is clear. Two direct care occupations—personal care aide (PCA) and home health aide (HHA)—are projected to grow 26% and 38%, respectively, from 2014 to 2024 and currently employ over two million people. 1 Aides in both occupations care for persons with chronic illness, disability, or dementia who need assistance with daily living tasks; HHAs also perform some delegated nursing tasks under the supervision of nurses for home health agencies and receive additional required hours of training. The growth in home and community based services (HCBS) drives much of this labor demand. Given population aging, increased life expectancy, and older adults’ desires to remain in their communities, some researchers and policymakers have predicted dire occupational shortages (Stone & Harahan, 2010). Although health care policy is now in flux, recent policy incentives to expand home health care and promote alternative models of health care service delivery and payment are likely to foster continued experimentation that will add to home care demand.
Researchers concerned about retention have highlighted poor quality of direct care jobs, including low wages, limited benefits, and heavy workloads (Chou, 2012; Chou & Robert, 2008; Morgan, Dill, & Kalleberg, 2013; Yamada, 2002). More recently, research has highlighted inconsistent hours, which Butler, Brennan-Ing, Wardamasky, and Ashley (2014) found were a primary reason, along with wages, that shorter-term home care workers left their jobs. DCWs working in the home are likely to experience unstable hours and are more likely than those in other settings to be given part-time work from any one employer. Scheduling affects consistency of earnings for this group disproportionately as they often have no paid time off (Stacey, 2011). Scheduling also affects worker outcomes (e.g., job satisfaction, turnover, worker health, and families) and organizational outcomes (e.g., productivity, engagement, and quality of care; Chuang, Dill, Morgan, & Konrad, 2012; Jacobs & Padavic, 2015). Schedule control has also been found to affect quality of care in nursing homes (Hurtado, Berkman, Buxton, & Okechukwu, 2016).
Research has examined problems with scheduling and hours in retail and restaurant work (Alexander, Haley-Lock, & Ruan, 2015; Haley-Lock, 2011, 2012; Luce & Fujita, 2012; Ruan & Reichman, 2014). This issue has been less studied for home care jobs, which are shaped by an interplay among policy and employer practices described in the context of other low-wage work by Haley-Lock (2012) and Haley-Lock and Shah (2007) and of social care employment by Rubery and Urwin (2011). Policy effects may be greater in home care, which is affected not only by labor and employment policy, but also health care policy, because public funding supports the majority of home-based care services in the United States (Paraprofessional Healthcare Institute [PHI], 2014a).
Changes to the Fair Labor Standards Act’s (FLSA) “companionship exemption” and clarifications of hours worked rules expand the law’s coverage of PCAs and HHAs and could affect how employers organize work. A shift to mandatory Managed Long-Term Care (MLTC) approaches to Medicare- and Medicaid-funded home care services is underway in many states (Saucier, Kasten, Burwell, & Gold, 2012). MLTC changes the way agencies are reimbursed for services from a traditional fee-for-service model to bundled or capitated payments for members. This model incentivizes agencies to coordinate care in ways that reduce per member costs such that the capitated payment covers or exceeds expenses for individual clients. This change in payment structure could affect how aides are deployed to serve clients. New approaches to Medicare/Medicaid payment for hospitals and Accountable Care Organization’s quality improvement initiatives also increase pressure on health care organizations to improve coordination and integration. Finally, the Affordable Care Act required that more employers provide health insurance for their full-time workers. This constellation of policies may affect employers in terms of reimbursement levels, penalties, or compensation (e.g., overtime payments and mileage reimbursements) and thus in terms of work scheduling. In this article, we identify and describe hours and scheduling practices from home health employers’ perspective, with a focus on the complicated context resulting from the interaction of labor and employment and health care policy. We seek to catalog the current and projected hours and scheduling practices of employers and describe the employers’ understanding of how new or impending labor and health care policy changes influence the way they are structuring jobs of DCWs.
Medicaid Policies
The recent transition of Medicaid-supported long-term care services 2 to MLTC plans (PHI, 2012) in New York is similar to policy initiatives affecting Medicaid in many states (Saucier et al., 2012). New York historically provided more care outside of institutions such as nursing homes than other states, but many states are “rebalancing” care toward home- and community-based rather than institutional settings. New York is, therefore, a valuable case study despite factors differentiating it from other states including relatively generous authorization of services through Medicaid, service delivery and aide employment primarily through agencies, and the history of unionization especially of PCAs based in New York City (Adelman, Kitchener, Ng, & Harrington, 2012). In short, New York’s example provides an excellent opportunity to explore how health care policies and FLSA rules may affect aides’ schedules as well as how agencies can staff for service delivery into the future. The shift to mandatory MLTC rolled across the state, beginning in New York City, in late 2012. It has reached all counties, but at the time of research did not yet affect all Medicaid-funded programs.
The perspective of agencies has resonance nationwide: While some state programs allow clients to hire aides directly with the support of public funds, agencies employ the majority of aides in the United States (Howes, 2014). In a home care agency setting, aide schedules depend on how agencies allot home care hours to patients, how they schedule care for multiple patients cared for by individual workers, and how they assign cases to aides. A client’s death, change in health, or sudden admission to the hospital changes an aide’s schedule. Total work hours are limited by what public programs permit and thus are affected by policy.
Agency employers are affected by minimum and living wage laws in some states and localities. In New York City and some surrounding counties, a wage policy called “wage parity” was adopted as part of the managed care initiative. The policy change has raised wages incrementally for HHAs employed by certain types of agencies to bring their pay up to par with that of home attendants (PCAs). PCAs in New York City have earned more due to their unionization history and further, aides working for agencies that contracted with the city were covered by the City’s Living Wage Law; until they had to transition to managed care, many long-term care clients receiving only personal care services provided by a New York City fee-for-service program and funded under Medicaid were cared for by PCAs covered by this law (PHI, 2014b). The final step in 2014 moved wages for HHAs providing Medicaid-supported care to US$14.09, including an hourly wage of US$10 and an additional US$4.09 that can include wages, paid time, and benefits.
FLSA
Home care agencies can no longer claim a companionship exemption under the FLSA for home care workers. Essentially, the new FLSA rule extended agency-based home care workers the same rights to overtime and minimum wage as the majority of hourly workers (U.S. DOL, 2013a). Before, home care workers were classified as “companions,” which meant they were not afforded the same rights to overtime and minimum wage protections. Furthermore, although no changes were proposed to FLSA rules on compensable time as they relate to travel time, paid waiting time, and sleeping time, many who commented in the rulemaking process leading to the companionship exemption change referred to how they apply to home care (Application of the Fair Labor Standards Act to Domestic Service, 2013). As part of its effort to plan for implementation of the companionship rule, the U.S. Department of Labor (DOL) has clarified “hours worked” rules as they apply specifically to the home care sector (U.S. DOL, 2013c). Despite several challenges, new regulations took effect in October 2015 with full enforcement in January 2016.
Under the new rules, home care aides must earn one and a half times their regular wages for each hour beyond 40 per week. Second, aides’ travel time between clients of one employer, but not to and from work, must be covered as work time. Third, time during which workers are “engaged in waiting,” such as time spent at the client’s home or employer site waiting between tasks, must be compensated unless the employee is completely relieved from duty. Finally, sleeping time, which is important when overnight care is provided, may only be excluded from pay if workers have at least five hours uninterrupted rest and adequate sleeping facilities (U.S. DOL, 2013b).
Method
Sample
Research was conducted in two stages. The first comprised 12 key informant semistructured topical interviews (Rubin & Rubin, 1995) with employer and worker association representatives and provided a broad picture of the policy context, industry, and challenges faced by aides. This informed the design of a semistructured interview schedule for agency representatives.
In phase two, 30 agency representatives from 17 agencies were interviewed. Nine agencies were identified by key informants or contacted through an employer association. To increase sample variation, the remaining agencies were systematically sampled from NY Department of Health listings of Licensed Home Care Services Agencies (LHCSAs) in Manhattan (using a list of 108 agencies) and the Bronx (72 agencies). In total, 54 agencies were referred and/or contacted via email or telephone. Of these, 37 declined to participate; nine reached through referral or at the conference agreed to participate, and eight recruited through the DOH list agreed to participate. All participating agencies were serving Medicaid-supported clients and operating in NY State.
Interviews and Analysis
LHCSA directors and staff are uniquely positioned to discuss how a confluence of policies affects hours, scheduling, and wage-setting because they hire and train workers and coordinate service delivery. We first interviewed a senior-level staff person in each agency about recent operational challenges, which policies affected them most, and characteristics of their organizations vis-à-vis long-term care service provision including income sources, size, organizational history, recruitment approaches, and strategies for hiring and managing aides. We then requested interviews with staff from human resources and operations and finance and coordinators. We stopped recruiting when content saturation was achieved.
Audiofiles were transcribed verbatim. As a first step in analysis, one researcher conducted a first round of coding within each case (agency) to identify major threats to agency operations and policy concerns and constructed a matrix to capture agency characteristics such as sources of funding, size of staff, union status, and for-/nonprofit status. Next, interviews were open-coded to identify employer practices in response to policy change, among which scheduling and hours stood out. Following a second round of coding and analysis within cases to further examine scheduling concerns, a second matrix was constructed that allowed for cross-case comparison (Huberman & Miles, 1998) of employer practices in relation to policy concerns and scheduling problems. In an iterative process, researchers consulted the interviews repeatedly during write-up to verify information contained in the matrix.
Results
We first provide a broad overview of our sample of 17 agencies and then further illustrate the range of agency structures and employment contexts using more in-depth portraits of four of these. Subsequently, we draw from our full sample of 17 to detail agency practices that affect hours and schedules, first practices employers use in reaction to and influenced by the policy context, and then others that are innovative, unrelated to policy, or show promise as models for agencies.
Table 1 summarizes characteristics of agencies, which were dispersed across the state, a mix of for- and not-for profit organizations, and primarily small to medium-sized as measured by staff size. We recruited five larger agencies to insure variation on that dimension.
Agency Characteristics.

Agencies hired a range of seven to 1,400 aides, the majority fewer than 600. Most hired only HHAs. Three received income from one of two Medicaid “waiver” programs that was not yet at this time covered by the managed care mandate, one providing services to individuals with brain injuries and another nursing home diversion program. Respondents worked at senior management levels in administrative, operations, finance, or clinical director positions (n = 22) or in coordinator, human resources, or clerical positions (n = 8), including two HHAs working in office positions.
A Range of Challenges: Agency Examples
Sample agency characteristics varied, including for-profit and nonprofit status, level of sophistication in operations, links with other entities that could provide referrals, organizational histories, type of clientele, and source of revenue or funding (see Table 2). Here we describe the way in which four agencies, selected to represent a variety of agency characteristics such as New York City versus upstate, for- and not-for-profit, and different size types, were dealing with the challenges they identified in this policy environment.
Selected Agency Profiles.
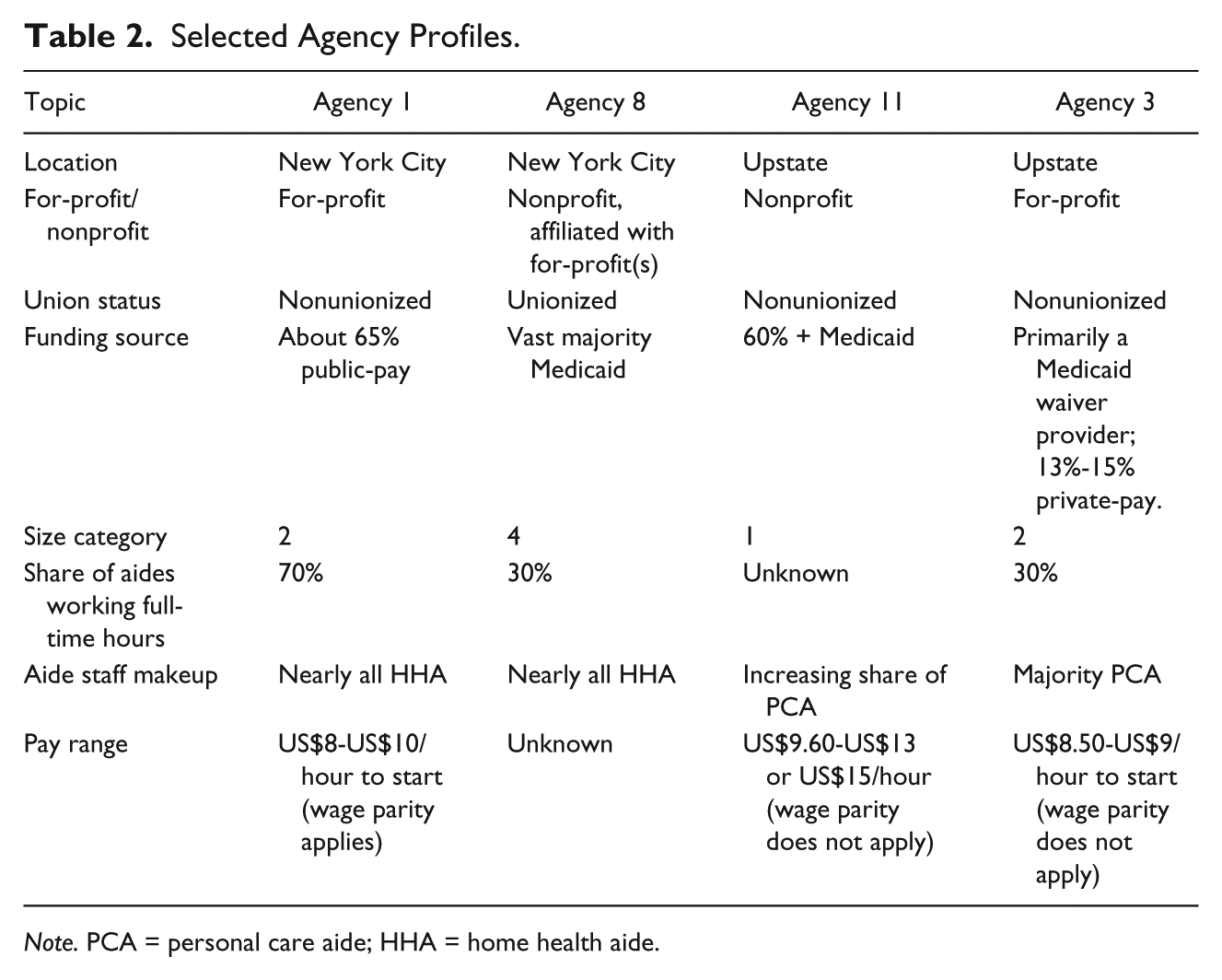
Note. PCA = personal care aide; HHA = home health aide.
Agency 1, a for-profit, small to medium (250-500 aides), nonunionized agency in New York City, received 65% of its revenue from public sources including Medicaid. Although many view managed care as a threat to the survival of their organizations, this agency concentrated on expanding public-pay clients and identifying different revenue streams (e.g., hospice) as a source of growth. The biggest challenge cited by a senior operations employee was wage parity and the resulting mandated raises for HHAs, which they said they managed with strong negotiation of reimbursement rates with contracting agencies to prevent wage increases from cutting too deeply into profits. Several employment practices at Agency 1 were unusual and had independent bearing on compensation: Employees paid for the physical and drug screening required for employment, aides traveled to the agency to pick up their checks, and aides earned more working in Medicaid-funded than private-pay cases (US$10 vs. US$8 per hour), a result of wage parity, which mandated that affected agencies pay a floor of US$10 per hour for Medicaid-financed care (PHI, 2014b).
Agency 11, a small nonprofit in upstate New York with a relatively rural clientele, was not unionized. Medicaid accounted for more than 60% of its revenue. Respondents cited challenges including stagnant or reduced reimbursement rates alongside rising expenses and declining volume and difficulty attracting new hires because of travel to remote clients and low pay. In terms of Medicaid managed care, just one managed care organization (MCO) was in the area, which was “still learning the personal care business,” resulting in slow paperwork. Due to recruitment difficulty and issues concerning public funding, they were unable to provide care to some clients seeking it. In response to the budgetary environment, they had closed one office, ended a weekend differential rate, and curtailed regular raises previously given to aides, who had recently been given a 25 cent hourly increase. This agency was not affected by wage parity because it was located out of New York City and paid from US$9.60 to US$15 an hour.
Agency 8 was a large unionized nonprofit organization. Medicaid funded the majority of its client care. Two senior respondents put policy affecting wages at the top of the list of challenges. One mentioned only wage parity and minimum wage standards and a new, stronger, union contract. The first also noted a new billing system introduced to implement managed care and policy changes that affect “how they pay:” the impending FLSA requirement to pay one and a half times the usual hourly wage for overtime and “the new signal that DOL will enforce aspects of wage and hour laws no one knew about [that are] not reimbursable,” such as calling aides in for meetings or paying for travel time as required under DOL’s clarification of FLSA coverage for home care. In response, they were reducing administrative costs and overtime and considering new scheduling practices.
Agency 3 was a small, for-profit agency located upstate, which was largely funded through Medicaid “waiver” programs that were not affected by managed care. This agency had 13% to 15% private-pay clients and employed primarily PCA aides, who can provide care under waiver programs, but had just added an HHA training program. Challenges cited included static reimbursement rates alongside increasing training requirements. The agency paid above minimum wage and employed many people who were Medicaid-eligible or declined agency-provided coverage. However, a senior staff person expected wage practices mandated downstate would spread to influence other areas and said the Affordable Care Act’s requirement that employers provide health insurance coverage to aides working 30 hours a week was “the largest thing . . . hitting agencies.” Consequently, they were doing more with less and avoiding expansion to limit overhead. They also planned to offer more services and train aides to a higher level, expecting that contracting entities would want “one-stop shopping.”
These examples demonstrate the complex web of health and labor policy factors that influence operations and how agencies respond to policy. The effects of multiple simultaneous policy changes are uncertain. The next section describes commonly cited policy changes and modifications of employment practices and staff reorganization in reaction.
Policy-Related Changes in Quantity of Services Authorized
Informants from agencies in operation for more than a few years perceived a reduction in the care hours and/or number of patients authorized for publicly funded care. Respondents cited a long-term trend with varied causes. One who had worked in operations at a small agency said authorization had become more difficult in terms of being “harder to get a Medicaid application and to get the hours” (Agency 13), meaning that gaining approval for an individual’s Medicaid-supported long-term care services had become more difficult and that authorizations tended to cover fewer hours. Another human resources staff person (Agency 5) reported less available work and had told aides they needed to share the wealth, temporarily. Noting that “[h]ours of care are down tremendously,” a senior-level employee of a large agency (8) said shorter visits were being authorized for new patients coming in under managed care. Some time slots are also hard to fill because aides do not want shorter hours or times such as late afternoon (when their children are out of school) (Agency 13). Aides who need full-time hours often must patch work together. A coordinator described the hardship of working for multiple clients: “some of the agencies are piggybacking cases, so you’d have four hours here, four hours there. It’s just . . . more onerous on the caregiver, because they’re running around from place to place” (Agency 13). A New York City respondent thought reductions in hours for individual clients would be limited: “Say if the average number of hours was six-seven, now it’s five-six. However, there are fewer patients getting services. [I’m] not sure why, if it’s not enough nurses to do the authorization . . . or less authorizing” (Agency 14). Other factors inherent to home care interacted with policy change to affect schedules, including the time of day when care is typically needed. A senior staff person at this agency noted that aide hours fit around day programs for many waiver patients: “the aide gets them ready for [the program]. Someone might stay the night shift. [It’s] very difficult if you don’t want to work weekends or want to put kids on the bus.” Another respondent said clients might attend a center just two days, leaving aides without work some days (Agency 8).
Several respondents said authorization of two 12-hour aide shifts for patients who need round-the-clock care had dropped. Instead, “live-in” aides were now typically compensated 13 hours to stay 24. This change was made based on the assumption that the aide can sleep. Most attributed this change to preference for live-in over “split-shift” to managed care, indicating that MCOs are pushing agencies in this direction. Four respondents described this 13-hour compensation practice as a labor law or a requirement of the DOL. One was required by the agency’s union contract to pay 15 rather than 13 hours for these overnight cases. Another characterized the perception of DOL’s approach to live-in aides differently and predicted a contrasting trend, saying that DOL had “started clarifying” that live-ins were to get eight hours of sleep, five uninterrupted, and “the aide has to get a break three times a day for mealtime . . . You can’t leave the client, but you can put the client in bed or at rest while you go take an hour for meals.” The respondent said more cases would be split shift because aides were not able to take these breaks or get the hours of sleep.
If the patient needs you every five minutes, the aide is supposed to contact us, and according to the Department of Labor, if they can’t get those rest times, the hour off plus time at night, we have to pay them. That’s what’s going to happen. We’re only billing 13 hours on a live-in. We can’t pay people for way more hours than we’re billing so these cases are no longer going to be able to be live-in (Agency 8).
Describing a situation in which a family wanted a live-in aide to turn one patient every two hours, this respondent said there was “an impasse” and indicated they would have to revisit their contract with the union. There may also be an impasse with managed care companies that are unwilling to authorize split shift.
Also noted were poor conditions for live-in assignments. A senior-level employer from a New York City nonprofit believed views of acceptable sleeping arrangements had changed: . . . all the split shifts were going live-in. . . . But they call adequate live-in arrangements maybe where . . . the patient is in the room, and you pull a curtain there, and there is a cot . . . . That’s ridiculous, back in the day if it was not a room available for the aide it was [not] a live-in. Now everything is a live-in, even if they have to sleep on a couch (Agency 12).
Finally, several mentioned travel time compensation rules as a concern compounding other wage changes. The rule clarifications were perceived by some respondents as new rules.
Agency Responses to Policy and Industry Changes
Respondents discussed strategies for coping with a cost squeeze and diminished or changed hours of care. Many had cut administrative costs and laid off office staff. In addition, there were reports of agency closings or purchases likely to precipitate different organization of staff. These policy responses affect organizational viability and, perhaps indirectly, schedules or hours. One concern is whether these changes will push more aides into less than full-time schedules. However, in the agency context, determining whether an aide is full- or part-time is difficult, as is determining what share would prefer part-time work. Aides need to meet certain hours thresholds to qualify for benefits. Employers monitor hours to determine which workers reach them. Similarly, aides’ status as temporary or long-term workers is hard to define: One operations manager’s comment (Agency 8) that “permanent only means until they go to the hospital” refers to the common occurrence of the death or hospitalization of “permanent” clients, after which an aide’s earnings and schedule may not get back on track for a long time.
Cutting hours, travel time rules, and avoiding overtime
Respondents commonly expected agencies to sharply curtail scheduling of overtime hours in reaction to policy. Most said they had cut or planned to cut employee hours to remain at 40 per week. Many were planning for the FLSA change then anticipated to be effective January 1, 2016, although New York already required at least one and a half times the legal minimum wage, but not of any higher wage for overtime. Agency 9 expected to keep hours down “because MLTCs are not going to pay us,” echoing others who said time and a half pay is not built into reimbursement. Another respondent (Agency 8) attributed hours restrictions to pay increases due to wage parity and minimum wage, noting that three aides rather than two were now assigned to live-in cases. Others identified new travel time regulations and cost cutting as incentivizing these changes.
Some described strategies for cutting hours. One respondent had stepped up hiring with the goal of having sufficient employees to keep everyone at 40 hours or fewer (Agency 3). A small employer in New York City had instructed coordinators to slowly diminish hours: “People will start feeling the pinch . . . because there were people working 70 hours a week, I said bring it down gradually so they don’t feel it so much” (Agency 9). The following comment, from a rural agency having difficulty recruiting enough aides to cover its clients, illustrates how policies overlap in their influence on employer decisions: We have overtime we have to pay, and now we have to pay travel time, which is big. So that means we have to give them less hours because we have to add travel time to their amount of hours, and either they cut back on cases, because they’re going to be on overtime, or you pay overtime. We want them to take more cases, but it’s costing us more money and more money. It’s frustrating actually (Agency 11).
The agency had begun paying wages for time travelling between clients in January 2015 but had stopped paying fuel costs for this travel due to cost pressures, while still covering costs of driving for clients’ errands. The agency reported that aides were unhappy about these changes. These changes have an important impact in a rural area with significant travel between clients. Another larger agency (16) outside the city had held off on cutting hours for “prime” aides to await the outcome of the FLSA court challenge, in the hopes that the result would overturn the requirement to pay more for overtime hours. Now some aides were splitting time between two agencies. Agency 16 tried to initiate job sharing with other agencies, but a problem emerged: . . . if they wanted to work with the same patient, . . . say for instance . . . an insurance company . . . would not split the authorization, so we lost some cases and some workers . . . a lot of aides sought out a different type of work, more permanent, Wal-Mart, or something like that . . . We can’t pay what we don’t have. If we don’t get reimbursed we can’t pay, and it almost shot us in the foot. You’re going to have less aides wanting to do this if you can’t work over 40 hours. (Agency 16)
Factors limiting cuts to worker hours
One respondent had heard that other employers were trying to keep aides below the 30-hour threshold at which employers must provide insurance under the Affordable Care Act mandate. She said she could not imagine how agencies could manage this. In fact, several employers said it would be difficult to cut hours. Patients do not like having numerous caregivers. A respondent at Agency 8 was reviewing cases to see which patients most needed to have the same aide present (e.g., those with dementia). At a small city-based agency, a staff member described the example of a 48-hour case and indicated it might not be worth it to schedule a second aide, because the patient would be dissatisfied, and it is hard to find someone who will “do that little extra bit of hours” (Agency 13). An upstate employer said Agency 6 would maintain overtime if FLSA went into effect because it had always paid time and a half wages to attract aides—“these agencies that paid time and a half way back when were the places to go.” The respondent later said she was trying to limit overtime, but “we still end up, even with about 1,700 hours a week we end up with at least 200 hours of overtime . . . you gotta cover the shifts.” Overall these discussions indicate not only that employer practices will change in response to policy, but also that some workers will still benefit from FLSA changes and enforcement.
Other Sector Employment Practices
In this section, we review additional employer choices not necessarily related to policy that affected hours and scheduling. These practices both raise concerns and potentially provide models that could help employers improve job quality. One of these appeared to be related to size and location: larger, city-based agencies may be more likely than smaller agencies to have many aides on the roster who were not scheduled. Agencies want to avoid declining cases due to the inability to match aides to cases. The owner of Agency 9 said, “ . . . there is enough [workers] within the system . . . they come here every minute to fill out the application,” but for some hard-to-reach areas they might need to see if they have an aide before taking the case. A recruiter at Agency 1 in New York City aimed for a “constant flow” of workers because the agency simply could not turn down cases. This recruiter seemed resigned to having surplus labor on the roster, but a more senior-level employee of this agency thought that, although coordinators believe they have too few aides, instead they did not have enough hours. Some research participants indicated that workers will leave quickly for a better case or wages elsewhere—or describe the situation as very fluid, saying workers “come and go.”
Practices that engage workers
A few agencies had created roles to engage workers. Several assigned aides as mentors who talk through challenges and encourage newer hires. They reported discussing how to work with the coordinator in the process of assigning cases. This role may improve engagement of mentors and improve support for newer hires. Agency 8 promoted at least one aide to a full-time in-house “senior home health aide” position. This person could serve as a replacement worker or go out on new cases that cannot be immediately covered and does office work at other times. This strategy addresses scheduling difficulties while providing more stable work for a handful of aides. This provides a nine to five schedule with a guaranteed income and pay for hours that exceed full-time work.
New scheduling practices
A few agencies were also making administrative changes that affect coordinator workloads and considering or adopting different approaches to scheduling that could be more systematic but may reduce flexibility. Two respondents mentioned the number of cases each coordinator (who assigns work to aides) managed. One large company (Agency 15) was in the process of acquiring a new agency in which the coordinators had a caseload of 45 as compared with 125, the norm in their company. Due to new budget constraints, Agency 8 had slowed the rate of hiring new coordinators. An increased workload could affect the ability of coordinators to work with aides on developing good schedules. Different practices for assigning cases to aides may also affect schedules and job quality. A specific coordinator may or may not be assigned to each aide, which affects whether aides are free to call more than one person if they are dissatisfied with schedules. One human resources staff person had assigned aides to a new coordinator in cases of conflicts to retain workers. In addition, scheduling organization can vary across agencies. For example, Agency 3, employing over 300 aides, has on-call weekend schedulers.
The combination of agency structure, managed care, and FLSA regulations could precipitate new approaches to scheduling. Some coordinators seemed to expect aides to clamor for more hours as a driver for assigning aides to work. A senior financial officer at Agency 11 said they might adopt a different approach due to FLSA changes: “we have certain people that take whatever that you hand them, which historically we’ve just sort of done . . . but as soon as we lose that exemption, overtime expenses are going to be a bear for us.” A representative from Agency 8 was considering using mapping software, to “schedule people with less travel, rather than giving work to the most eager worker.” As employers try to constrain hours, they may also seek to have more workers on the books to cover shorter shifts. This could exacerbate worker surplus and hours shortfall.
Some agencies seem to be experimenting with ways to improve scheduling, an effort that may be circular. For example, an agency focused on retention may not only try to give aides more hours, but also restrict them to 40, which increases the likelihood aides may sign on with two agencies. Then employers must work extra hard to get newly trained aides scheduled quickly enough not to lose them. An Agency 1 recruiter said aides do not want to “hear about” short cases. As noted, a stable schedule is only dependable when a client’s health status is stable, no matter how good the employer, or how much the aide likes the schedule. The owner of Agency 4 said the chances of throwing a worker into a tenuous situation when a patient’s status changes might be reduced with more of a “boutique” agency, or a smaller agency that maintains a relationship with aides and therefore is better able to match aides to new clients after they lose existing ones.
Some emerging types of care arrangements offer different schedules. First, two agencies reported employing aides in buildings where multiple patients live, so that aides can drop by for shorter visits, thereby putting together more work and billing shorter hours. One is a provider for another new model of Medicaid health homes under the state’s health home initiative targeting high-risk, high-cost Medicaid consumers (Patchias, Detty, & Birnbaum, 2013). In a different sharing model, aides working for more than one Service Employees International Union-organized agency can combine hours across them to meet benefits eligibility requirements.
Discussion
These findings highlight how agency employers are struggling to find practical solutions to the problems introduced by a changing policy landscape and show that practices employers say they are adopting would have a mixed impact on workers in home and community settings. Employers funded primarily by public sources reported that they generally feel forced to make changes to scheduling and assignment practices because of the widespread perception that reimbursement rates from payers will not cover overtime and substantial wage and benefit increases. One strategy to comply with new policies is to overrecruit aides so that there is a surplus of workers. Although this does not appear common in rural areas where shortages exist, some urban agencies are using the strategy. This generally reduces work per aide with any one employer, but the common practice of working for multiple employers may protect aides from adverse impacts on hours. In most cases, however, this means aides do not qualify for benefits at either employer. Some rural aides may benefit from FLSA by receiving overtime in the short run, but employers claim this threatens agencies’ economic viability.
Recommendations for ameliorating hours shortfall and instability for low-wage workers in other service sectors have included public policy recommendations, suggestions for employers, and the encouragement of worker advocacy. Policy recommendations include strengthening or expanding existing state laws or collective bargaining agreements that regulate call-in and send-home practices and amending the FLSA to regulate scheduling practices, set wages that compensate workers for risk, or change the interpretation of “waiting time” that is compensable (Alexander et al., 2015). Alexander et al. (2015) pointed out that the effectiveness of this strategy depends on whether workers make claims of violations. Employers argue that these changes, without changes to reimbursement policy, may also be untenable for agencies’ bottom lines. In fact, the state established a program in 2014 to encourage MCOs to pay higher reimbursement rates to agencies and in 2016 provided funds to cover FLSA overtime costs (Nisbet, 2017).
Others have proposed changing laws governing employer-provided (Ruan & Reichman, 2014) and government-provided benefits (Lambert & Henly, 2009) to enhance benefits coverage of part-time workers. By setting a 30-hour coverage threshold, the Patient Protection and Affordable Care Act adopted in 2010 diminished the vulnerability of some workers. However, because HHA and PCA hours are unstable and often spread across different employers, this safety net may be insufficient for these workers. If coverage is affordable or sufficiently subsidized through Medicaid expansion, individually held coverage may be the most attainable for these low-wage and precariously employed workers. Similarly, structures that allow employers to work together to gain economies of scale in obtaining benefits for workers may also improve worker health benefit access. Haley-Lock (2012), noting that small and independent businesses have difficulty benefitting from economies of scale, has suggested employer collectives might address this challenge.
Right-to-request legislation adapted to the needs of hourly workers and minimum-hours legislation would encourage employers to reduce flexibility and post schedules farther in advance, while potentially creating a trade-off of lost worker influence over schedules in exchange for predictability (Haley-Lock, 2012; Lambert & Henly, 2009). It is unclear how minimum-hours or notice requirements would apply to a sector driven by unpredictable client needs and compensated by public funds. However, in this study, we see some employers experimenting with new positions that offer flexibility in allocating work (e.g., combining administrative and clinical work; peer mentors, and fill-in roles) and minimum hours, somewhat in keeping with Lambert, Haley-Lock, & Henly’s (2012) recommendation that employees be cross-trained to ensure productivity during down times. In home care, these solutions affect a fraction of workers. Finally, scholars have urged workers to attend to schedules and hours through unions, worker centers, or other collective action (Alexander et al., 2015; Ruan & Reichman, 2014). The data presented here suggest that some workers have benefited from wage parity and living wage/minimum wage laws. Given declining unionization rates, occupation-specific policy such as New York’s wage parity policy or changes to minimum wage laws may be a more feasible solution than union-based collective bargaining for most workers.
This analysis illustrates the overlapping and evolving influences of policy, employer practices, needs of clients, and desires of workers on schedules and hours and thus on both job quality and agency viability. Employer responses vary widely, and more research is needed to capture factors that predict these responses. This is, to our knowledge, the first study to explore the relationship between public policies and hours and scheduling from the point of view of HHA/PCA employers. Although the issues of scheduling, consistency of hours, and low-wage work have been explored in the literature, it has been largely focused on retail or service sector jobs and has not emphasized public policy. This study draws attention to the way labor and employment policy and health policy interact to influence employer decision-making around hours and scheduling.
This study had a few limitations. It focused on one state, New York, which is arguably at the vanguard of implementing these policies, but also somewhat unique. First, the City and the rest of the state comprise at least two separate labor markets. This overview is not focused on the differences between the two labor markets but rather treats it as one context for purposes of this article. Furthermore, New York has a higher unionization rate than most states, which particularly affects this sector. Obviously, union contracts affect worker agreements and scheduling for unionized aides, and a handful of interviews touched on contractual influences on decision-making about some scheduling issues. Finally, despite a concerted attempt at obtaining sampling variation, there is an element of selection bias based on whether agencies were willing to speak openly about policy and employment practice. Replicating this work in other contexts would add further insight to the research questions.
Footnotes
Acknowledgements
The authors thank the research participants for their contribution to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by PSC-CUNY under Grant 67702-00 45.