
Abstract
Using Andersen’s health behavioral model as a framework, this study examined factors associated with the completion of advance directives and the behavior of sharing them with one’s family and health care providers. Data were from the 2014 United States of Aging Survey (N = 1,153; aged 60 or older), and multinomial logistic regression was used for analysis. We found that 73% of respondents had advance directives. However, 28% have not shared their advance directives with anyone. The sense of having completed a great deal of preparation for the future and the number of illnesses were found to be relevant to the behavior of sharing advance directives. Existing educational training and interventions can be expanded to increase public awareness and encourage people to share their completed advance directives with others. Policies mandating physicians to engage in advance directive conversations with patients during annual checkups might improve completion and sharing of advance directives.
Advance care planning (ACP) is the process of planning for future medical care in the event that a person becomes unable to make decisions or speak for oneself. It is an opportunity for individuals to express what type of medical treatment they wish or do not wish to receive for their end-of-life care during an irreversible, terminally ill condition. ACP involves various types of communication, such as informal discussions with family members and health care providers, advance directives, and the Physician Orders for Life-Sustaining Treatment (POLST) form (Holley, 2012). Advance directives are legal documents that take two forms: a living will and a durable power of attorney for health care (DPAHC; also referred to as a health care proxy; Carley et al., 2014). A living will is a written document that specifies the types of medical care a person does or does not want to receive under certain circumstances. A DPAHC is a designated individual permitted to make health care decisions for an incapacitated person when decisions have to be made that are not covered in the living will. The POLST form is a medical order that is signed by both the doctor and patient or legal surrogate (Carley et al., 2014). One of the critical differences between advance directives and the POLST form is their target population. While the POLST form is used only for seriously ill or frail patients, all adults are encouraged to complete advance directives regardless of their health status (Carley et al., 2014).
In 1990, Congress passed the Patient Self-Determination Act (PSDA) to encourage people to plan their end-of-life care so that their autonomy, the right to self-determination, is protected. Under the PSDA, health care institutions certified by Medicare and/or Medicaid are required to provide their clients with written information on advance directives at the time of enrollment. Research findings indicate that the PSDA has been successful at increasing public awareness and the completion of advance directives, especially among older adults and people in declining health (Bradley, Wetle, & Horwitz, 1998; Resnick, Schuur, Heineman, Stone, & Weissman, 2009). Along with the government’s efforts, the importance of advance directives has been well documented in the literature. First, completing advance directives is a means to respect a person’s autonomy. Second, having advance directives in place reduces surrogate decision makers’ emotional burden (Braun, Beyth, Ford, & McCullough, 2008). Finally, documenting advance directives can help avoid unnecessary or unwanted medical treatment in end-of-life care (Mack, Weeks, Wright, Block, & Prigerson, 2010; Zhang et al., 2009).
Many studies have examined factors that promote or hinder the completion of advance directives, although many of these studies used a small sample size drawn from a geographically constrained or institutionalized population (e.g., Alano et al., 2010; Carr & Khodyakov, 2007; Dobalian, 2006). Furthermore, in contrast to an extensive number of studies focusing on the completion, little research has examined whether completed advance directives have been shared with family members and health care providers. Sharing this information is a critical step to take in order to have one’s wishes carried out. Inaccessibility to and unawareness of existing advance directives have been reported as barriers to effective and timely implementation of ACP (Weinick, Wilcox, Park, Griffey, & Weissman, 2008; Wilkinson, Wenger, & Shugarman, 2007). Therefore, using the Andersen’s (1995) behavioral model as a framework, this study examined factors that were associated with the completion of advance directives and the behavior of sharing the completed advance directives with one’s family and health care providers by analyzing the data from the United States of Aging Survey, which includes nationally representative samples of Americans 60 years and older.
Conceptual Framework
Andersen’s health behavior model has been widely used to investigate health service utilization. Although this study does not directly analyze the use of health services, the model still offers insight into health-related human behavior, explaining why people take certain courses of action. Thus, to examine a person’s completion and sharing behavior of advance directives, this study used three major components of Andersen’s behavioral model: predisposing, enabling, and need factors.
Predisposing Factors
According to the conceptual framework, predisposing factors contribute to a person’s tendency to choose a specific behavior. Such predisposing factors pertain to demographic and sociostructural characteristics, such as age, gender, race, and income. These factors have been extensively examined in relation to the completion of advance directives. Previous research has found age, race, and income as robust predictors: A person who is older, identifies himself or herself as White, and has a higher level of income is more likely to complete advance directives than a person who is younger, a person of color, and with limited income Carr, 2012; Carr & Khodyakov, 2007; (Moorman & Inoue, 2013; Pollack, Morhaim, & Williams, 2010).
As people get older, they experience losing family members and friends, which may make them more aware of the inevitability of death. This can lead them to think about advance directives. Racial discrepancies in the completion of advance directives have often been explained by distrust of the medical system and cultural differences (Johnson, Kuchibhatla, & Tulsky, 2008; Kwak & Haley, 2005). Negative perceptions of advance directives, such as viewing them as a means to deny the medical care, are more prevalent among African Americans than Whites. Family-centered decision making instead of self-determination is more common among Hispanics and Asians than Whites.
Although income is usually examined as one of the enabling factors in Andersen’s behavioral model, income was assessed as a predisposing factor in the current study. Previous studies have consistently found income as another robust predictor of the completion of advance directives: A person with higher income is more likely to obtain advance directives (Moorman & Inoue, 2013). Carr (2012) argued that the conversation about advance directives is often brought up when people document a financial will; thus, those who are economically advantaged are more likely to complete advance directives. Therefore, in the context of this study, income fits better with predisposing factors that influence a person’s propensity to complete and share advance directives.
The influence of gender is inconclusive. Although Carr and Khodyakov (2007) reported that men are more likely than women to obtain advance directives, Inoue (2016) and Alano et al. (2010) reported the opposite. A person’s demographic and sociostructural characteristics have been important variables in previous studies examining the completion of advance directives; these characteristics are also vital in analysis assessing the next important step of sharing one’s completed advance directive.
In addition, Andersen added the psychological characteristics of attitudes and values as predisposing factors in the revision of his model in 1995 (Andersen, 1995). Thus, such characteristics of the individual that are associated with advance directives are also important to consider. Because advance directives are completed in preparation for the future, the current study takes into account a person’s sense of preparedness for the future. It is assumed that people with a greater degree of sense of preparedness for the future are more likely to have completed advance directives and shared them with other people.
Enabling Factors
Resources that facilitate a behavior are called enabling factors. Social relationships were added to the model as enabling factors in the revision of Andersen’s model because social support and networks can facilitate or impede taking action (Andersen, 1995). Applying this framework to the current study, being connected with others can offer a person more opportunities to learn about the benefits of advance directives and the importance of sharing them. It is logical to assume that people who are not lonely or isolated have more communication with others, which can promote the completion of and sharing one’s advance directives.
Need Factors
The presence of illnesses or disabilities and perceived health service needs have been used as need factors when examining the use of health services because people do not need to access health services when they are healthy. The same trend has been observed in the previous research on the completion of advance directives: People who perceive their health status as poor are more likely to document advance directives. Similarly, it is expected that a person’s poor health motivates him or her to discuss advance directives with family members or health care providers.
In sum, the research question of this study pertained to factors that were associated with the completion of advance directives and the behavior of sharing those with one’s family and health care providers. Based on the literature review, it was hypothesized that among those aged 60 or older, increased age, White race, higher income, a greater sense of preparedness for the future, lack of loneliness/isolation, and perception of poor health are associated with greater likelihood of completing advance directives and sharing those with their family members and health care providers.
Method
Data and Sample
Data were from the 2014 United States of Aging Survey, which is based on 3,250 phone interviews conducted between April 3, 2014, and May 6, 2014, by the National Association of Area Agencies on Aging, the National Council on Aging (NCOA), UnitedHealthcare, and USA Today (NCOA, 2014). Consisting of 107 questions, the original purpose of data collection was to examine older Americans’ perspectives on a variety of issues, such as health, finance, and formal and informal support. The current study examined a subsample of 1,153 older adults aged 60 or older and were randomly selected from 3,250 individuals to be asked questions related to ACP. One question asked whether a respondent had been involved in different types of ACP. The question included multiple items to check, such as whether a respondent had an informal conversation about wishes for end-of-life, documented advance directives (a living will and DPAHC), and/or shared advance directives with their health care team or loved ones.
Variables
Dependent variable
The dependent variable, shared advance directives, was a nominal variable with the following three categories: those who had no advance directive, those who had an unshared advance directive (reference group), and those who had an advance directive that had been shared with their loved ones or health care team. This variable was derived from participants’ responses to the following statements: (a) “Created advance directives such as a living will,” (b) “Designated a power of attorney or surrogate for health care,” (c) “Shared your advance directives with your health care team,” and (d) “Shared your advance directives with loved ones.” A person who answered “no” to both the first two statements was categorized as no advance directive. A person who answered “yes” to both or either of the first two statements and also answered “no” to both of the third and fourth statements was considered to be a person with an unshared advance directive. A person who answered “yes” to both or either of the first two statements and also answered “yes” to both or either of the third and fourth statements was considered to be a person with shared advance directive.
Independent variable
Age, gender, race, and income were included as predisposing factors. Age was a continuous variable measured in year. Gender was a dichotomous measure, coded 1 for female. Race was categorized into three groups: White (reference group), Black/African American, and Other. Annual household income was an ordinal variable with 13 categories; the smallest category was less than US$5,000 and the largest category was US$200,000 or more. After checking the distribution, these income categories were further collapsed into a low-income group with less than US$20,000 (bottom one third), middle-income group between US$20,000 and US$49,999 (middle one third), and high-income group with more than US$50,000 (top one third). A middle-income group was used as a reference group. One’s sense of preparation for the future was assessed as a predisposing factor. The variable of a sense of preparation for the future was derived from the following question: “How much preparation have you done for your senior years?” The answer categories included no preparation, little preparation, some preparation, and a great deal of preparation. Those who answered no preparation or little preparation were combined and used as a reference group. The survey did not define whether preparation was specific to certain aspects of life, such as financial planning or health care planning; instead, the survey asked general outlook for the status of the future preparation. Although preparation is not specific to advance directives, a person’s preparation trait or behavior is assumed to transfer to the completion and sharing behavior as well.
Whether a person has a sense of loneliness/isolation was included as an enabling factor. This variable was assessed by the following question: “How often do you feel lonely or isolated from others?” The answer categories included never, rarely, sometimes, and often. Those who answered never or rarely were combined and categorized as lack of loneliness/isolation, and the other two categories were combined and categorized as feelings of loneliness/isolation (reference group). The number of illnesses was a continuous variable and was included in the analysis as a need factor. Its response categories were 0, 1, 2, 3, 4, and 5 or more.
Analytic Strategy
There were 130 respondents who answered that they did not have any type of advance directives but answered that they shared advance directives with either their health care team or loved ones. Because of the inconsistency with their responses, those 130 people were excluded from the analysis. Income had the most missing observations of 127 (12%). After confirming the unpatterned nature of missing observations, listwise deletion (only using cases that have a complete set of data) was used. Analyses began with descriptive statistics to summarize the respondents’ characteristics. Multinomial logistic regression was executed to test the research question. After the listwise deletion, the final sample size for multinomial logistic regression analysis became 869. As a sensitivity analysis, authors also performed multiple imputation for missing data and ran the same statistical analyses. Because the results stayed the same, findings from complete case analysis are reported. All statistical analyses were performed using the statistical software package STATA 13.
Results
Descriptive Statistics
Table 1 summarizes the sample characteristics of the study. The majority of respondents (53%; n = 461) had shared their advance directive(s) with their health care team and/or loved ones, but 27% (n = 231) did not have any form of advance directive. Respondents’ age ranged from 60 to 100 years old with a mean of 73.2 (SD = 8.4). The majority were female (65%; n = 564) and White (81%; n = 705). Approximately one third of the respondents fell in each income category: US$0 to US$19,999 (36%; n = 310), US$20,000 to US$49,999 (33%; n = 292), and US$50,000 or more (31%; n = 267). Nearly half of respondents (45%; 389) answered they had done some preparation for their senior years, but 26% (n = 224) had done no or little preparation while 29% (n = 256) had a great deal of preparation. Approximately three quarters of respondents were considered to be socially connected (73%; n = 634); they reported that they never or rarely felt lonely or isolated. The average number of illnesses that respondents reported was 2.9 (SD = 1.7). Among those who have shared their advance directives with someone (n = 461), 244 people shared with both a loved one and a health care team, and 189 people shared only with a loved one. Only 28 people shared their advance directives with a health care team but not with a loved one.
Respondent Characteristics (n = 869).

Multivariate Analyses
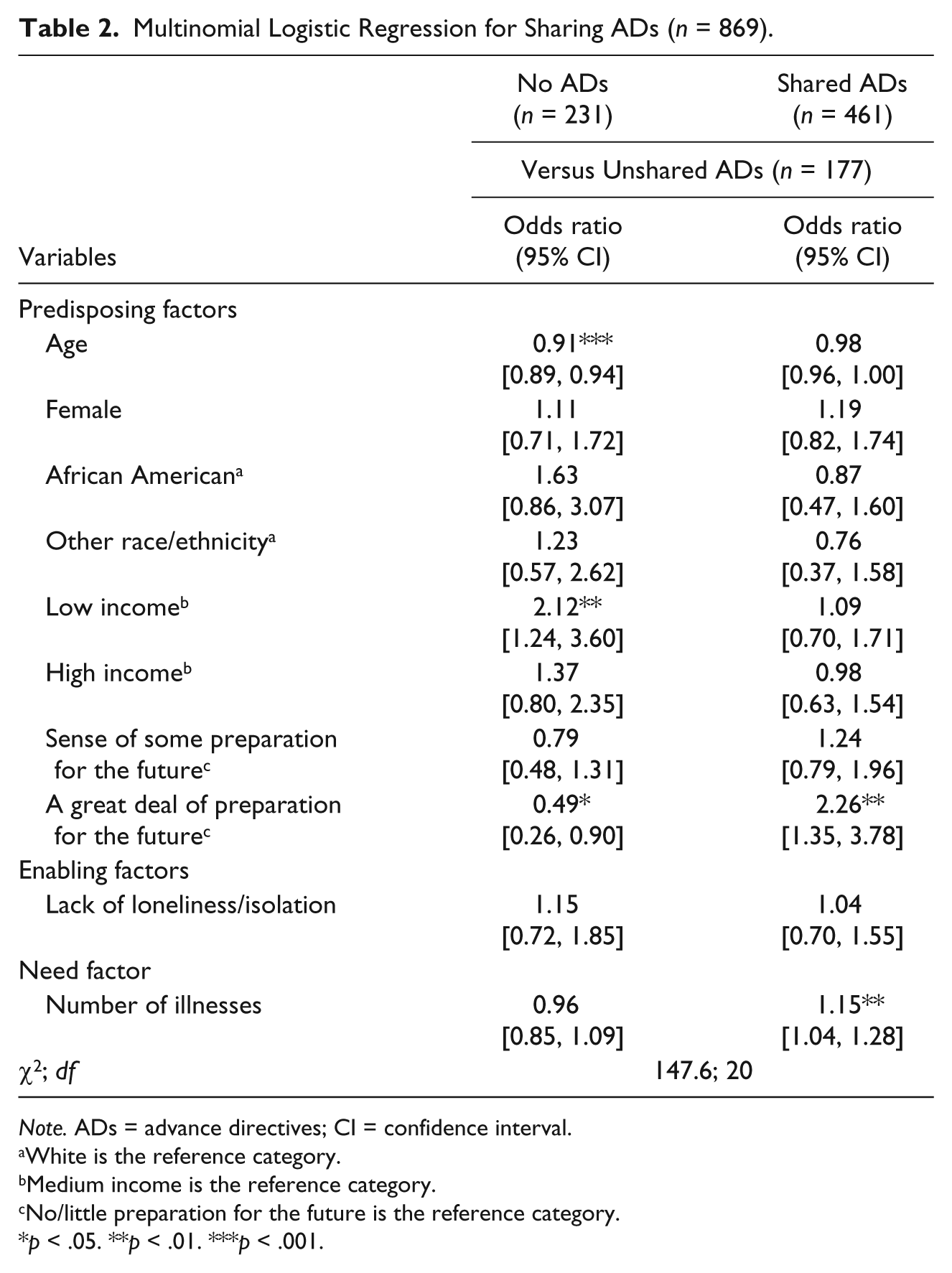
Table 2 summarizes the multinomial logistic regression results. The category of having advance directive(s) that had not been shared was used for the baseline comparison group.
Multinomial Logistic Regression for Sharing ADs (n = 869).
Note. ADs = advance directives; CI = confidence interval.
White is the reference category.
Medium income is the reference category.
No/little preparation for the future is the reference category.
p < .05. **p < .01. ***p < .001.
Predisposing factors
Age, income, and a sense of preparation for the future were associated with the completion of advance directives. Increased age was associated with the decreased relative probability of not having an advance directive rather than having an unshared advance directive (odds ratio [OR] = 0.91, p < .001). In contrast, the relative probability of not having an advance directive rather than having an unshared advance directive was 2.12 times higher for people with low income than people with medium income (OR = 2.12, p < .01). Compared with people with no or little preparation for the future, people with a great deal of preparation for the future were less likely to say that they did not have an advance directive rather than that they have an unshared advance directive (OR = 0.49, p < .05).
A sense of preparation for the future was the only significant predictor for sharing an advance directive. Compared with people with no or little preparation, people with a great deal of preparation for the future were more likely to have had a shared advance directive than an unshared advance directive (OR = 2.26, p < .01).
Enabling factors
Social connection was not a significant predictor for the completion of an advance directive or the shared advance directive.
Need factor
The number of illnesses was a significant predictor for a shared advance directive. A greater number of illnesses was associated with greater odds of having a shared advance directive than having an unshared advance directive (OR = 1.15, p < .01).
To see whether sharing advance directives with a loved one and sharing advance directives with a health care team would yield different results, two separate multinomial logistic regression analyses were conducted. The same variables became significant with the same direction in each model (results available upon request).
Discussion
Guided by Andersen’s behavioral model, this study examined predisposing, enabling, and need factors that are associated with the completion of advance directives and the behavior of sharing those with one’s family and health care providers. Increased age and a sense of having completed a great deal of preparation for the future were less likely to be associated with lack of advance directives. Older adults with low income were more likely than those with medium income to say that they had not completed an advance directive. The sense of having completed a great deal of preparation for the future and the number of illnesses were found to be relevant to the behavior of sharing an advance directive. Findings indicated that 27% (n = 231) did not have advance directives. Among the remaining 73% (n = 638), 177 people had an advance directive but had not shared it with anyone. This indicates that even if people documented advance directives, 28% (177/638) have not shared their advance directives with their loved ones or health care providers. Without having one’s wishes known, there is a possibility that his or her right to direct medical treatment can be compromised.
The findings from multinomial logistic regression analysis on age and income were consistent with previous studies (Moorman & Inoue, 2013; Carr, 2012; Dobalian, 2006). Older age and higher income have been robust predictors of the completion of advance directives. However, they are not associated with the behavior of sharing advance directives with one’s family and health care providers. Among the predisposing factors, only a person’s sense of preparation for the future was significantly associated with both the completion of advance directives and sharing them with others. Compared with those who think they have done no or little preparation for the future, people who believe that they have completed a great deal of preparation for the future are more likely to have documented advance directives and have shared them with others. The purpose of advance directives is to ensure that a person’s wishes for future medical decisions will be honored and carried out even when the person becomes incapable of speaking for oneself (Snyder, 2012). Therefore, people may perceive completing and sharing advance directives as essential activities for their future preparation. An alternative explanation would be that completing and sharing advance directives offer people a sense of great deal of preparation for the future. Because the study design was cross-sectional, it cannot establish causality; it is unknown if people who want to be better prepared for the future are motivated to complete and share their advance directives or if people feel prepared for the future because they have completed and shared their advance directives. Either way, documenting advance directives and sharing them with others are associated with one’s view on the future preparation because knowing that their wishes are known and will be taken care of in the future may bring them peace of mind (Booij, Engberts, Rödig, Tibben, & Roos, 2013).
The number of illnesses (a need factor) is significantly associated with the behavior of sharing advance directives with others. People with more illnesses are more likely to share their advance directives with others. One of the common reasons for not engaging in ACP was that a person still has good health (Carr, 2012; Pollack et al., 2010). In other words, people are less likely to talk about their end-of-life care preferences with their families and health care team until they become sick. These study findings also indicated that unless people have many health problems, they do not talk about the content of their advance directives with others. However, sudden, unexpected medically serious conditions can happen to anyone. Such conditions may not offer people time to inform others of their advance directives. As a result, they miss the opportunity to inform their family members who will likely to be surrogate decision makers or health care providers who will likely to assist family members in decision making. Making decisions for someone is an emotionally stressful process, and many surrogate decision makers report family conflicts and burden when a dying person’s preferences are unclear (Braun et al., 2008; Kramer, Boelk, & Auer, 2006). Therefore, the process of sharing advance directives with others should happen once people have documented them to have their wishes known to their loved ones and health care providers.
Limitations
Although this study was able to make a contribution to knowledge by examining the behavior of sharing advance directives with others, which is an important step to take after completion, a few limitations of the study should be noted. First, because of its cross-sectional design, the study could not establish causal relationships between predictor and outcome variables. It was impossible to assess if and how changes in the predisposing, enabling, and need factors influence people’s completion and sharing advance directives over the course of their lives. Second, because the data were based on self-reports, it is important to be aware of potential social desirability bias that might have influenced the results (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003); the completion and sharing of advance directives may be overestimated.
A lack of some potentially influential variables due to the use of secondary data was another limitation. For example, some previous studies have reported that people with higher educational attainment (e.g., Alano et al., 2010; Moorman & Inoue, 2013) and higher sense of control (Inoue, 2016) are more likely to document advance directives than those with lower income or sense of control. If available, these variables could have been included as predisposing factors to see whether they are significant predictors for sharing advance directives. A person’s belief that physicians, rather than patients, should make health care decisions has also been reported as an influential variable for the completion of advance directives (Carr & Khodyakov, 2007). If a person wants a doctor to decide his or her medical treatment, even if the person had completed advance directives, he or she might not see the benefits of sharing their treatment preferences with a loved one or doctor. Having been able to include one’s belief about who should make decisions as a need factor in the analysis might have yielded different results.
Implications
There have been efforts implemented to encourage people to think about end-of-life care preferences and complete advance directives (Tamayo-Velázquez et al., 2010). The Conversation Project (2015) and Respecting Choices® (Gundersen Health System, 2017) are examples of such efforts. The Conversation Project has gained positive recognition for encouraging people to discuss their end-of-life care wishes with others (Flowers & Howe, 2015). Respecting Choices® has been reported to be effective in changing health care institution practices and improving the prevalence of advance directives (Pecanac, Repenshek, Tennenbaum, & Hammes, 2014). While it is important to continue these efforts, as the findings indicate that increasing awareness and completion of advance directives among younger people and people with limited income is essential considering these populations’ lower completion rates. Organizing community educational events might be helpful to directly reach these populations.
The current study findings also suggest that there is a clear gap between the completion of advance directives and the process of sharing them with others. Existing interventions to increase public awareness of advance directives can be expanded and used for encouraging people to take the next step of sharing their completed advance directives with others. For example, an educational component emphasizing the importance of sharing advance directives with others can be added to the current efforts of Respecting Choices® (Gundersen Health System, 2017).
As previous literature suggests, there is a discrepancy in the prevalence rates of advance directives between people with higher socioeconomic status and those with lower (Carr, 2012; Carr & Khodyakov, 2007; Moorman & Inoue, 2013; Pollack et al., 2010). Finding and accessing resources available online such as The Conversation Project might be easier for people with resources than those without. Therefore, reaching out to those with fewer resources would be important. One suggestion is to educate staff members in agencies serving older adults by using The Conversation Project Starter Kit so that they can reach out to their clients. This Starter Kit is designed to help people to talk about their end-of-life care, as well as help people who want to assist someone to share their preferences, because completing and sharing advance directives may involve an emotionally charged conversation, which is often difficult and uncomfortable (Stuart, Volandes, & Moulton, 2017). Flowers and Howe (2015) examined the effects of The Conversation Project Starter Kit on agency staff in terms of their willingness to discuss end-of-life issues with their clients, and they found its positive impacts. Therefore, implementing The Conversation Project in agency settings to train and educate staff members serving older adults would be a good intervention. In this way, clients’ wishes will be shared with staff members, who can file such wishes.
With regard to policy, the enactment of the PSDA in 1990 has increased the completion rates of advance directives (Bradley et al., 1998; Resnick et al., 2009). Therefore, federal laws seem to have an impact on people’s health behaviors. Implementing policies that encourage the process of sharing advance directives would make positive changes. On January 1, 2016, Medicare began reimbursement to physicians who provide an ACP consultation to their patients (Centers for Medicare & Medicaid Services, 2016). This policy was introduced with the expectation that physicians would be encouraged to talk about ACP with their patients although an early evaluation conducted 3 months after the implementation found no significant changes in ACP practice among physicians (Tsai & Taylor, 2017). Whether a physician has an ACP conversation with a patient is currently optional. Therefore, implementing a policy that mandates physicians to bring up this topic at an annual checkup would change their practice and may be effective in increasing patients’ completion rates of advance directives and sharing them with physicians. In this way, people will have more opportunities to think about completing and sharing advance directives before becoming too ill.
Finally, more studies including potentially influential variables on the process of sharing advance directives will be needed, such as a person’s education level, sense of control, and belief that physicians should make end-of-life care decisions. Longitudinal data collection will also help shed some light on this area by examining changes in people’s completion and sharing behavior over the life course as their predisposing, enabling, and need factors change.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.