
Abstract
This community-based cluster randomized trial evaluated the efficacy of a 4-week multimedia educational intervention followed by telephone consultations at Weeks 12 and 24 on the selection of a hospice program for end-of-life care and completion of an advance directive (AD) in case of future advanced dementia. One hundred twenty-three cognitively intact older adults from five community centers in Taiwan were randomly assigned to two groups. The study showed that 100% of participants in the intervention group (two community centers, n = 52) selected hospice program care for end-of-life care and signed ADs, whereas those in the control group were less likely to do both (p < .001). Participants in the intervention group also had a positive change in knowledge, subjective norms, perceived behavioral control, and behavioral intention of advance care planning (ACP) for advanced dementia. The theoretically based multimedia educational program was effective in assisting ACP implementation and completing ADs among community-dwelling older adults.
Introduction
Attention over recent decades has focused on the growing number of people with dementia because of the rapidly increasing older population worldwide. A new case of dementia is estimated to be diagnosed every 3 s (World Health Organization [WHO], 2017). The WHO also estimates that 63% of people with dementia live in low- and middle-income countries (WHO, 2017). Taiwan became an aged society with 14% of its population older than 65 in March 2018. By 2026, the older population will be over 21% of Taiwan’s total population, making Taiwan a hyper-aged society (National Development Council, 2016). The rate of aging population in Taiwan is faster than that in Japan, the United States, and the United Kingdom (National Development Council, 2016).
A nationwide survey of the Taiwanese population aged ≥ 65 years showed that the prevalence of mild cognitive impairment was 18.7% and for all-cause dementia it was 8.04% (Sun et al., 2014). Dementia is a syndrome caused by a variety of brain illnesses that affect memory, other cognitive abilities, and behavior (WHO, 2017). Most dementias are incurable, with many comorbid diseases, and it may ultimately lead to severe disability (Chen et al., 2017). Previous studies have revealed that age and apolipoprotein E genotype were strongly associated with dementia (Baumgart et al., 2015). In addition, accumulating evidence has shown that hypertension, diabetes mellitus, hyperlipidemia, and cerebrovascular disease are associated with dementia (Chen et al., 2017). Furthermore, dementia causes severe stress and places a burden on socioeconomic and health care systems; thus, improving awareness and understanding of dementia at all levels of society can improve quality of life for those with dementia and their families.
Patients’ dignity and autonomy have long been advocated in the health care system in Taiwan. In 2015, the Patient Autonomy Act was implemented, which grants adults full rights to document advance directives (ADs) specifying their wishes for treatment should they become unable to communicate them (Ministry of Health and Welfare, Taiwan, R.O.C., 2015).
Adults, especially older adults, should learn more about advance care planning (ACP) to help them determine their preferences for end-stage treatment. ACP is defined as “a voluntary process of discussion between an individual and their care providers to consider how their condition may affect them in the future and, where appropriate, make choices and plans for their future care” (ACP Project Management Group, 2015).
Education regarding ACP for advanced dementia is especially crucial among older adults and their families to reduce burden and improve quality of life (Detering & Silveira, 2017). However, few people know about ACP (Teixeira et al., 2015). Although over 70% of low-income community-dwelling older adults in the United States were willing to complete ADs (Ko, Lee, & Hong, 2016), only 14% of individuals living in rural counties had completed ADs (Ashcraft & Owen, 2016). Promoting ACP requires long-term implementation strategies and continued support systems (Ampe, Sevenants, Smets, Declercq, & Van Audenhove, 2017; Bardach, Dunn, & Stein, 2017).
A significant research gap exists regarding the effectiveness of ACP intervention on end-of-life care of dementia (Alzheimer Disease International, 2016). ACP has emerged as a topic of interest for the health care industry worldwide; however, sensitivity regarding end-of-life care in Taiwanese society and difficulty accessing the degree to which health care professionals are educated on ACP have led to a low rate of AD completion (Lin & Hu, 2016). A systematic review on the effectiveness of decision aids in assisting older patients during end of life revealed that proof of their effectiveness is mainly based on low-quality evidence, which suggests that further exploration of the use of decision aids in ACP is required (Cardona-Morrell et al., 2017).
Although ACP has been demonstrated to positively affect the quality of end-of-life care, other review studies have suggested that studies on ACP interventions in different settings (e.g., in the community) are required (Brinkman-Stoppelenburg, Rietjens, & van der Heide, 2014; Detering & Silveira, 2017). Researchers (Brinkman-Stoppelenburg et al., 2014) reviewed 113 studies concerning the effects of types of ACP. The findings revealed that most studies were observational and conducted in the United States. Nearly half of the studies were performed in hospitals, and one third were conducted in nursing homes. Most importantly, compliance with patients’ end-of-life wishes was increased through complex ACP interventions. Thus, they suggested that further studies with experimental designs using complex ACP interventions in community settings are warranted.
Recently, emphasis in ACP has changed from the completion of ADs to the discussion of ACP with physicians and family members (Hanson et al., 2019; Noh, 2017; Sudore & Fried, 2010). Health care providers who play a critical role in disseminating health policy and communicating policy with the general public are considered some of the most suitable personnel for implementing ACP in the community (Lin & Hu, 2016). Video decision aids to assist with ACP have drawn increasing interest. Another systematic review concluded that video decision aids may improve some ACP-related outcomes; however, before the media can be used in practice, more studies are required to confirm the impact of video decision aids (Jain et al., 2015).
Thus, the primary aim of this study was to investigate the effects among community-dwelling older adults of a multimedia educational intervention on the selection of a hospice program for end-of-life care and completion of an AD in case of future advanced dementia. The secondary purpose was to examine the effects of the educational intervention on cardiopulmonary resuscitation (CPR)-related knowledge, attitudes, subjective norms, perceived behavioral control, and behavioral intention of ACP for advanced dementia.
Method
This study was a community-based cluster randomized controlled trial with a longitudinal research design, which we conducted between October 2017 and April 2018. Ethical approval for the study was provided by the research ethics committee of the hospital. Written informed consent was obtained from the participants, who voluntarily participated. Data were collected at baseline (Week 0) and Weeks 2, 3, 4, 12, and 24, dependant on the corresponding variables based on the transtheoretical model (TTM; Prochaska & Velicer, 1997).
Sample and Setting
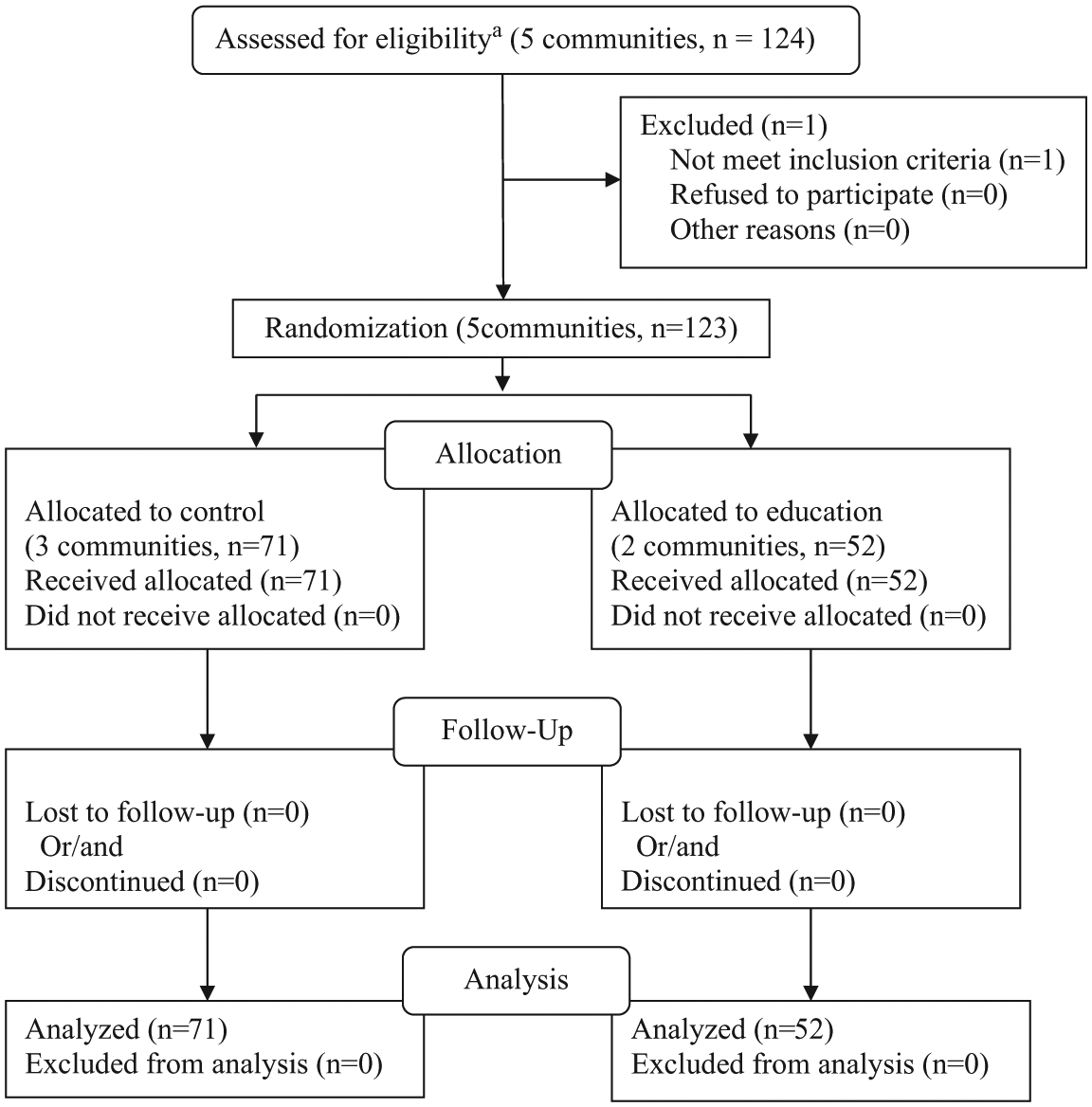
The participants were recruited from five community centers located in remote areas with low average income; the centers are operated and managed by a Catholic district teaching hospital in southeast Taiwan. The community centers were randomized and assigned to intervention (two community centers with 52 participants) and control groups (three community centers with 71 participants) using random numbers generated by computer. The allocation results were disclosed to the nurse educator to implement the interventions. To be eligible for the study, participants had to be aged ≥55 years if they were aboriginal (which is the age that aboriginal people qualify to have the same welfare as older adults in Taiwan) or ≥65 years old, have a Short Portable Mental Status Questionnaire (SPMSQ) score ≥8 (Pfeiffer, 1975), be able to read, and not yet have signed an AD. We excluded those who had organic brain syndromes diagnosed by physicians at the study hospital and those aged <55 years for aboriginal people or aged < 65years for nonaboriginal people. The recruited older adults attended the centers regularly for social activities and health promotion. We therefore chose to randomize the community centers rather than the individuals for ethical considerations.
Theoretical Framework
The conceptual framework for this study was derived from the theory of planned behavior (TPB; Ajzen, 1991) and the concept of stages of change based on the TTM (Prochaska & Velicer, 1997). Ajzen (1991) stated that attitudes, subjective norms, and perceived behavioral control drive people’s intention to perform a behavior, which in turn influences whether they engage in the behavior. TPB has been increasingly applied to the study of human behavior over recent decades. The ultimate goal of health education is to change behavior. Behavior change is a dynamic process that can be divided into five stages: precontemplation, contemplation, preparation, action, and maintenance (Prochaska & Velicer, 1997). According to the TTM (Prochaska & Velicer, 1997), the stages of change do not occur in a linear progression but in a spiral pattern. For the purpose of behavioral change, several strategies can be applied to deliver education that meets people’s needs at different stages (Prochaska & Velicer, 1997). Given that the purpose of this study was to increase ACP and uptake of ADs among older adults using a multimedia education program, we combined both the TPB and TTM to design a program and then examined its efficacy.
Intervention
The designed intervention was a 4-week multimedia ACP educational program followed by telephone consultations at Weeks 12 and 24 conducted between June 2017 and May 2018 (Figure 1). The program was developed based on the TTM (Prochaska & Velicer, 1997). The content of the program was selected on the basis of a previous study (Wang et al., 2015). ACP pamphlet used in the program was published by the Hospice Foundation of Taiwan (Wang, 2013). Because it is designed for general consumption, the content of the ACP pamphlet is easily understood by untrained individuals. The ACP pamphlet was distributed to each of the participants in both groups.
Survey data collection at each point during the 24-week study.
The ACP pamphlet is 26 pages long with the following content: introduction to ACP, end-of-life care, medical decisions related to end-of-life care, surrogate medical decision makers, discussions with health care providers and family, and wills. Table 1 presents the context of the education program, and the attached Online Appendix lists the URLs for each video used in the education program. In addition to the major content of the ACP pamphlet, material on advanced dementia was added to the education program.
Multimedia Education Program for ACP.

Note. Classes between Week 1 and Week 4 lasted 50 min each. ACP = advance care planning; PPT = PowerPoint; AD = advance directive; CPR = cardiopulmonary resuscitation; ICU = intensive care unit.
The teaching strategies of the education program were lectures, watching videos (Hanson et al., 2017), group discussions, counseling, support, and values clarification. The education program included four weekly sessions. Each weekly session was conducted in the community centers and was delivered by a senior nursing educator specialized in hospice care and geriatric nursing with >20 years’ experience. Each weekly class lasted for 50 min and included various activities (Table 1). Most participants had opportunities to have face-to-face discussions with the educator. Telephone follow-up evaluations were conducted after Weeks 12 and 24, which enabled the educator to contact participants from both groups and answer all questions concerning the ACP and signing an AD, or to check with participants whether their willingness to sign an AD had changed.
The participants in the control group did not receive the education program, but they undertook their usual community activities. However, they were given the same ACP pamphlet and were instructed to read it as well as to ask any questions that they may have had.
Procedures
Four nursing educators and one physician reviewed and edited the content of the questionnaires to ensure general appropriateness and applicability. The ACP pamphlet (Wang, 2013) was distributed to all participants in both groups, and a presentation providing a preliminary introduction to ACP was delivered to both groups to provide them with basic knowledge regarding ACP. A series of structured questionnaires were administered by research assistants in the classroom of each community center to assess the following: participants’ demographic characteristics (Table 1; baseline; Week 0), CPR-related knowledge and attitude toward ACP (baseline and Week 2), subjective norms and perceived behavior control (baseline and Week 3), behavioral intention (baseline and Week 4), and preference for AD and signing an AD (baseline, Week 4, Week 12, and Week 24). All data were collected immediately after a 15-min tea break of that week’s class, except for demographics, which were collected at baseline. The collection of different data at different points was designed based on the TTM (Prochaska & Velicer, 1997).
The control group received the ACP pamphlet. If they had questions regarding the content of the pamphlet, the educator provided oral explanations. The times of data collection for the control group were the same as for the intervention group. All patients were followed up for 24 weeks over the study period. After study completion, the same educational program was provided to the control group.
Measurement Instruments
The instruments used to measure the primary (the selection of a hospice program for end-of-life care and completion of an AD) and secondary outcomes (knowledge, subjective norms, perceived behavioral control, and behavioral intention of ACP for advanced dementia) were self-developed on the basis of previous studies related to ACP (El-Jawahri et al., 2010; Epstein et al., 2013; Fried et al., 2012; Medvene, Base, Patrick, & Wescott, 2007; Morrison & Meier, 2004; Sudore et al., 2014) and the concept of constructing questionnaires for the TPB (Ajzen, 2002).
Uptake of AD was determined by whether an AD document had been signed (Wang, 2013), which was determined by asking a single question with a yes/no answer. Preference for ADs (Volandes et al., 2011; Wang, 2013) was measured by asking one single-choice question: “What kind of advance directives would you prefer when in the terminal stage of dementia with only a few weeks left to live when you are unable to make decisions regarding medical treatment for yourself?” Four choices were provided: “try as many methods as possible to prolong life,” “stop treatment only when all treatments have failed,” “accept only noninvasive treatment,” and “accept only hospice care.” This question was then recoded as a dichotomous option of the first two and last two choices combined into “selecting treatment” and “selecting hospice program care,” respectively. The content validity was 0.93.
The secondary outcome was CPR-related knowledge, for which there were five questions. Three response options were offered for each question: “yes,” “no,” or “unsure.” The following two items were the example questions used to assess the participants’ knowledge about CPR: (a) Advanced dementia patients are able to speak and eat on their own when they are on a mechanical ventilator. (b) Most advanced dementia patients who get CPR in the hospital survive and get to leave the hospital. A correct response received 1 point. The total scores were between 0 and 5. A higher score indicated that they were more knowledgeable about CPR. The content validity was 0.90, and the Cronbach’s alpha of the CPR scale in this study was .72.
The other secondary outcome variables were attitude toward ACP (seven items), subjective norms (eight items), behavioral intention (eight items), and perceived behavior control (four items). The definition of attitude toward ACP was a participant’s cognition or value in choosing ACP; subjective norms of ACP were defined as the effect of significant others in decision making regarding ACP; perceived behavior control of ACP was defined as an individual’s perception of his or her ability to perform ACP, and behavioral intention was defined as whether an individual planned to perform ACP. These secondary outcome variables were all measured using a 7-point Likert-type scale, with a higher score for variables indicating more or higher level corresponding variables. The content validity for attitudes, subjective norms, behavioral intention, and perceived behavior control was 0.94, 0.92, 0.91, and 0.94, respectively; the Cronbach’s alpha was .85, .88, .81, and .88.
Data Analysis
All analyses were undertaken using SPSS (Version 18.0). Descriptive statistics were employed to describe the homogeneity of the demographic data and outcome variables between the intervention and control groups at baseline. Generalized estimating equations (GEEs), a robust analysis method in the analysis of longitudinal data, were used to examine the effects of the intervention on participants’ CPR knowledge, attitude, subjective norms, perceived control, behavioral intention, intention of selecting hospice program care, and completion of an AD. A significance level of p < .05 indicated statistical significance. When necessary, the p value was adjusted using the Bonferroni correction for multiple comparisons.
Results
Participant Characteristics
Over the study period of 24 weeks, 124 potential participants were recruited from five community centers, and only one was disqualified because of an SPMSQ score < 8. The remaining 123 participants all completed the study (Figure 1). Table 2 presents the characteristics of the study sample and differences between the intervention and control groups at baseline. The participants were aged between 56 and 96 years (mean age = 75.72 years). The majority were married. Most participants were women, had Catholic religious belief, and had a primary-level education. The mean number of chronic diseases among the participants was 1.35 (SD = 0.75). Notably, all participants had heard about ACP and ADs, but they were unclear as to what they were. Several variables were significantly different between the two groups’ baseline characteristics, indicating that the two groups were not comparable at baseline.
Participant Profile and Scores of Outcome Parameters at Pretest by Group (N = 123).
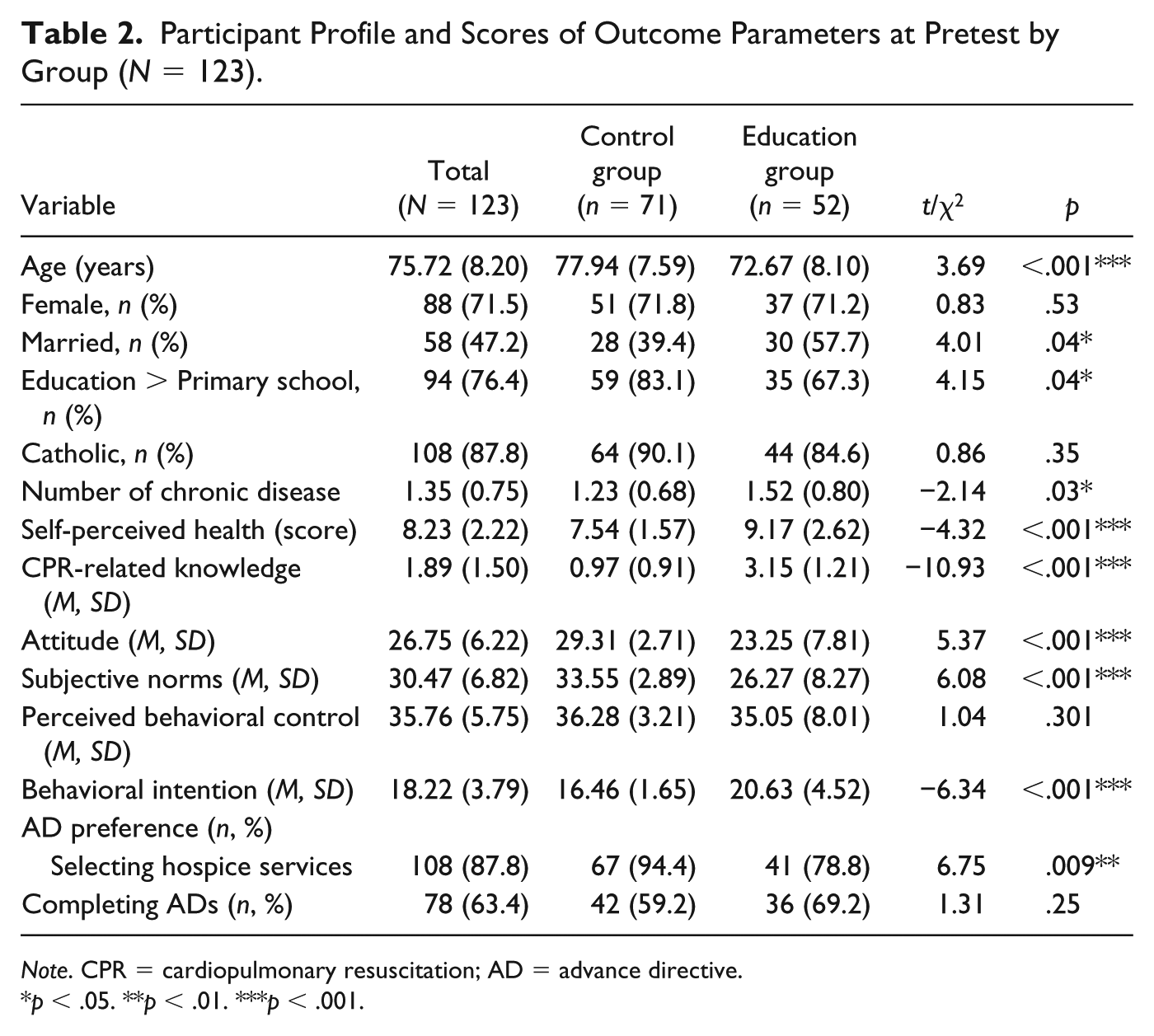
Note. CPR = cardiopulmonary resuscitation; AD = advance directive.
p < .05. **p < .01. ***p < .001.
Effect of Education Intervention on Selection of Hospice Care and Completing ADs
The percentage of participants selecting hospice program care by group and over time is plotted in Figure 2. The average percentage of participants selecting hospice program care in the intervention group significantly increased from 78.8% at Week 0 to 100% at Week 12, which was maintained to Week 24; however, the average percentage in the control group remained the same from 94.4% at Week 0 and Week 4, but it significantly decreased to 67.6% at Week 12, with a sustained decrease to 22.5% at Week 24. The average percentages of participants selecting hospice program care were significantly different at Week 12 and Week 24 between the experimental and control groups (p < .001).
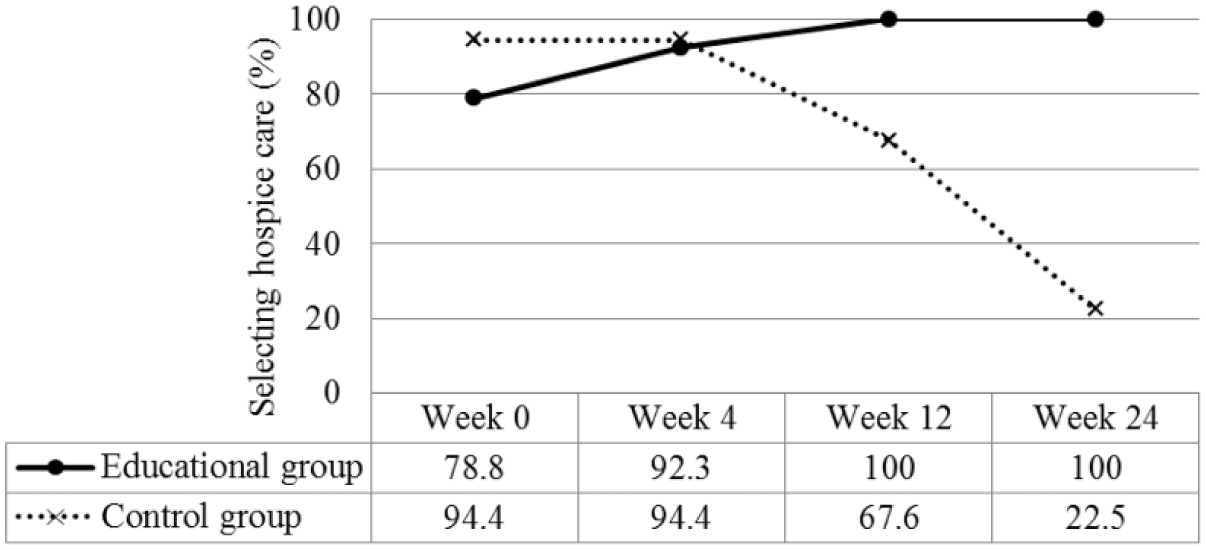
Percentage selecting hospice program care in the education group was significantly increased at Week 12 and Week 24.
Regarding similarities in the patterns of change, we found that the percentage of participants for completing ADs was significantly increased at each posttest point to Week 0 in the intervention group (p < .001), whereas slightly increased percentage was observed in the control group over the 24-week period (Figure 3). Significant differences were also discovered at each posttest point between groups (all p < .001). The Bonferroni correction (α/4 = .012) was used to examine group differences in percentage of completed ADs at each point.
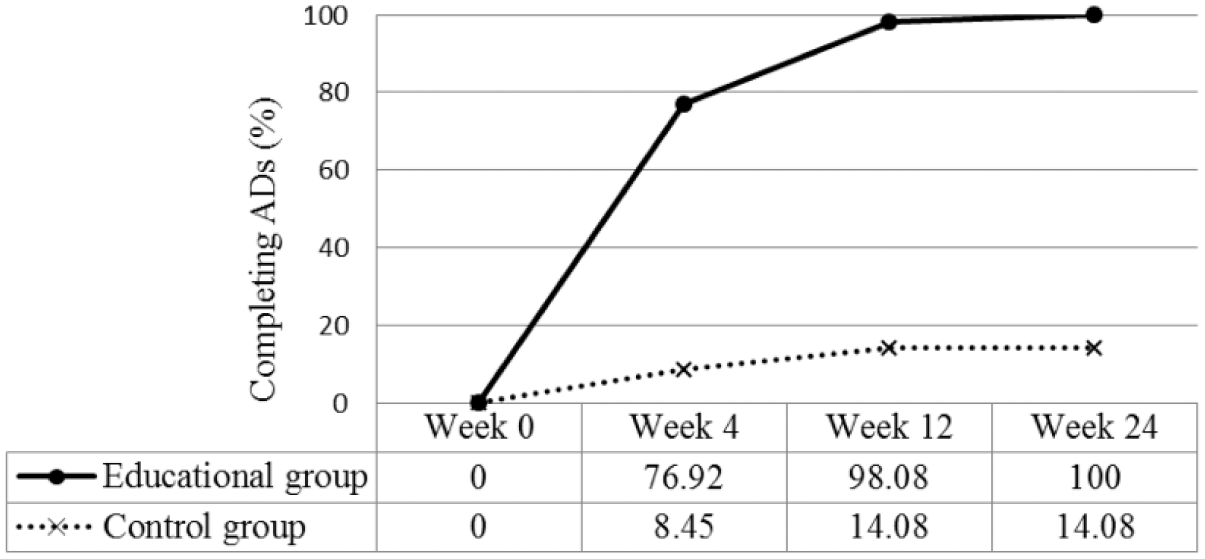
Percentage completing ADs in the educational group significantly increased over time; the percentage completing ADs was significantly different at each point of posttest between groups.
GEEs could not be performed to further examine the changes for selecting hospice program care and completing ADs by group over time because the percentages for both reached 100% in the intervention group at Week 12 and Week 24, respectively. However, the findings indicated that the education intervention improved rates of selecting hospice program care and completing ADs.
Effect of Education Intervention on the Secondary Outcomes
The GEE model results showed that—after controlling in the model for age, marriage, education level, religious belief, chronic disease, and self-perceived health—change in CPR-related knowledge, subjective norms, behavioral intention, and perceived behavioral control were significantly different between groups (all p < .001; Table 3, Figure 4a and 4c-4e). The findings revealed that compared with the control group, the intervention group exhibited significant improvement in the level of each parameter both during and after the educational program when adjusting for age, marriage, education, number of chronic diseases, and self-perceived health (Table 3). However, the difference in attitude between the intervention and control groups was nonsignificant in the second week.
GEE Estimation of Group Differences (n = 123).
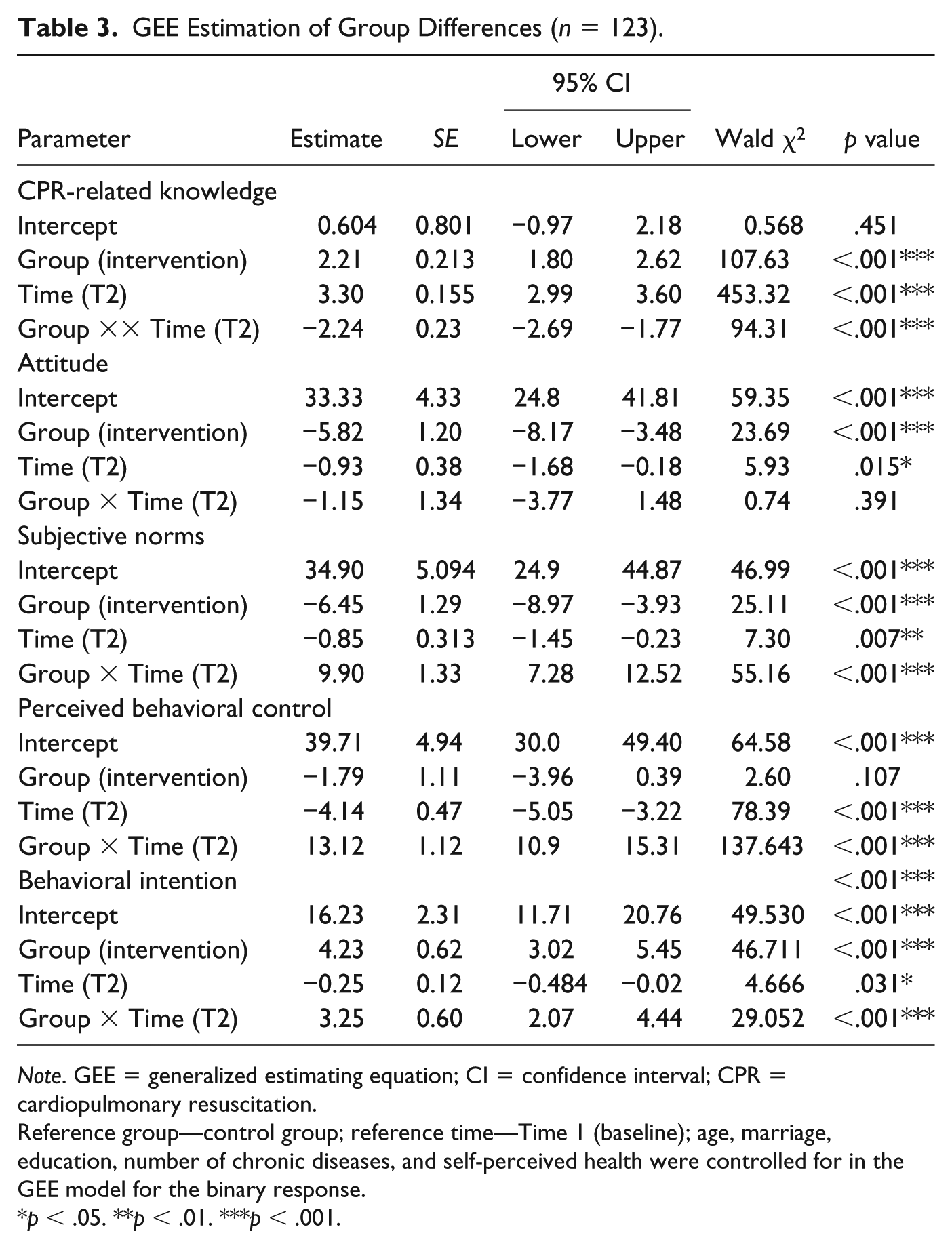
Note. GEE = generalized estimating equation; CI = confidence interval; CPR = cardiopulmonary resuscitation.
Reference group—control group; reference time—Time 1 (baseline); age, marriage, education, number of chronic diseases, and self-perceived health were controlled for in the GEE model for the binary response.
p < .05. **p < .01. ***p < .001.
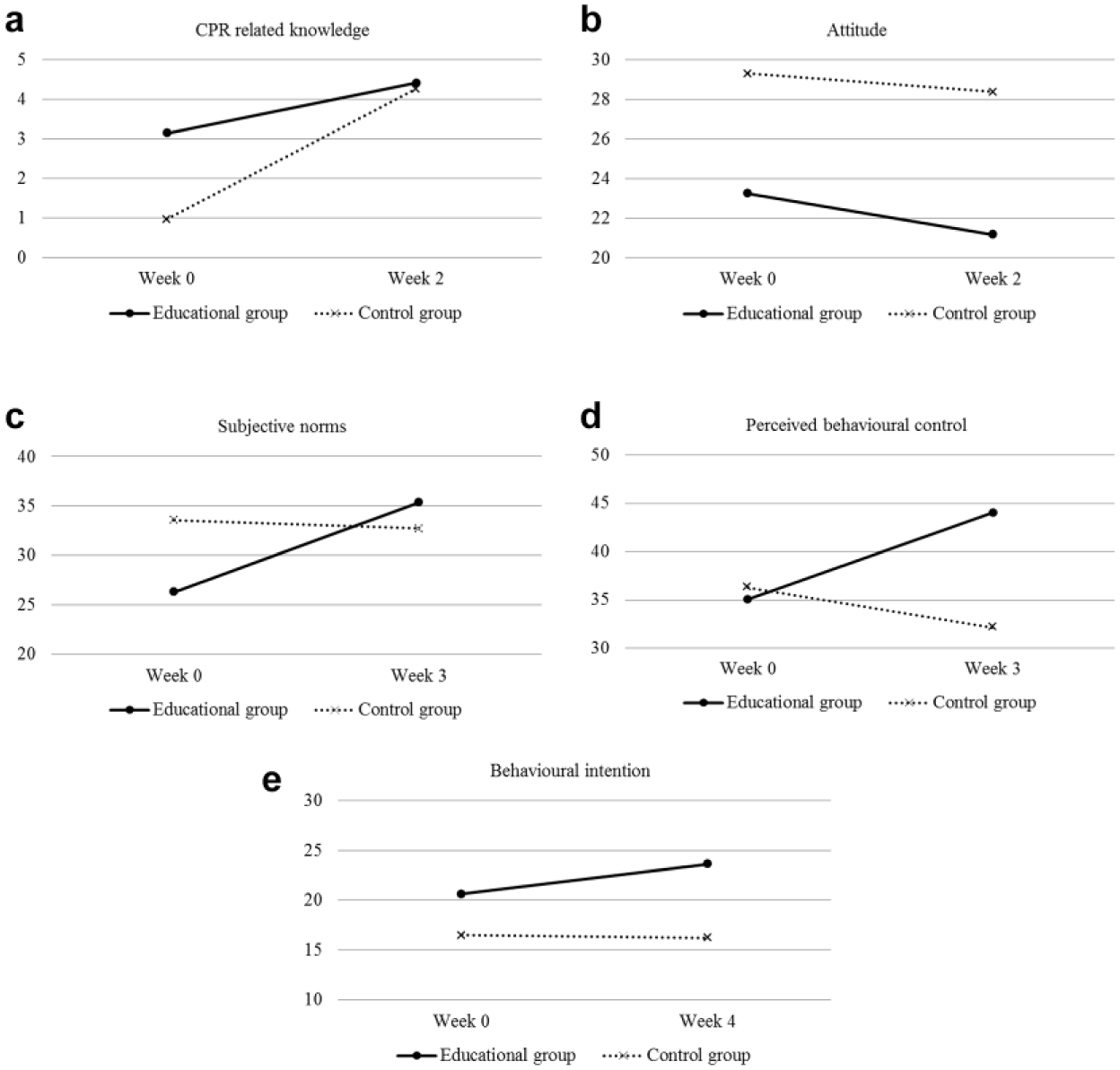
Values of (a) CPR knowledge, (b) attitude, (c) subjective norms, (d) perceived behavioral control, and (e) behavioral intention at different points between groups.
Discussion
The present study conducted in Taiwan revealed that a 4-week multimedia educational program followed by telephone consultations for another 20 weeks achieved a 100% completion rate of ACP and ADs regarding advanced dementia among community-dwelling older adults (Figures 2 and 3). By contrast, a significant decrease was found in selecting hospice program care over time for the control group from Week 0 to Week 24. The explanation concerning the high rate of selecting hospice at baseline was possibly because the control group was older and less healthy, which might influence its selection of AD preference (Inoue, Ihara, & Terrillion, 2019). Another possible explanation for our study finding is provided by the observation of Boucher (2017) who stated that older adults’ decision making of ACP can be influenced by family involvement. In addition to the primary outcomes, the findings showed a significant increase in knowledge, subjective norms, perceived behavior control, and behavioral intention in the intervention group compared with the control group after controlling for other demographic characteristics (Figure 4a and 4c-4e).
Taiwan’s government has sought to promote quality end-of-life care for patients by improving patients’ capacity to make their own AD through ACP, particularly since the Patient Self-Determination Act became law in 2015. Compared with that in other countries, ACP in Taiwan is still in its infancy. To our knowledge, this study is the first to explore the efficacy of a longitudinal educational program on ACP for advanced dementia among community-dwelling older adults. Although a systematic review has demonstrated that ACP increases hospice use (Brinkman-Stoppelenburg et al., 2014) and a meta-analysis has revealed that video decision aids may improve some ACP-related outcomes (Jain et al., 2015), the quality of evidence has been low because of study design (Jain et al., 2015), and more studies targeting advanced dementia end-of-life care (Hanson et al., 2017) in community populations are required (Brinkman-Stoppelenburg et al., 2014). The findings of the present study help fill the gaps of these previous studies and add knowledge regarding the efficacy of education programs in implementing ACP among older adults.
We developed this interventional program based on the TTM (Prochaska & Velicer, 1997), which is demonstrated in the program’s recursive pattern, shaped repetitions, and participants’ learning through experiencing, reflecting, and acting. The decision to use a randomized controlled design with pre- and posttests and adopt ACP-related outcome variables based on the TPB model (Ajzen, 2002) to measure program efficacy ensured the quality of evidence in the present study. Moreover, no attrition was noted during the 24-week period of our study.
Although signing AD documents is not considered the ultimate goal of ACP (Sudore & Fried, 2010), the positive intervention effect of our education program on AD uptake was reflected by significant improvement in the proportion of participants completing ADs at the end of the intervention period, as well as the group differences from Week 2 to Week 24. The implementation of the educational program for ACP requires long-term follow-up and continuous support for older adults and their families to ensure successful ACP (Boucher, 2017). However, whether the trend toward AD uptake maintains or changes with time requires further observation in other longitudinal studies. Follow-up research is also required to examine whether older adults’ wishes for end-of-life care are a response to actual receipt of medical care.
According to the TPB, attitude is a predictor of behavior. However, changes in participants’ attitudes toward ADs were not significantly different across time between groups after adjusting for all confounding factors in the analysis model (Table 3 and Figure 4b); nonetheless, behavioral intention was significantly different between groups (Table 3 and Figure 4e). A possible explanation for this finding is that attitudes and actual behavior are not always parallel (Chaiklin, 2011).
An unexpected finding was that the proportions of participants selecting hospice program care significantly decreased in the control group over the course of the 24-week study period. Although the control group did not receive the education program during the study, the pamphlet regarding ACP (Wang, 2013) was distributed to them. All the participants thus had access to the health-related knowledge in the pamphlet. Providing popular editions of educational pamphlets to communities or patients is one strategy for disseminating health-related knowledge. The reason that this proved ineffective in the present study requires further examination.
Health care providers play a vital role in helping patients and clients discuss ACP with their families and thus prepare for any future medical decision making. Because there is a lack of high-quality evidence in the literature regarding ACP implementation, researchers can take leading roles in studying the effectiveness of ACP programs that meet the requirements of community-dwelling older adults.
This study had several limitations. First, the participants were recruited from a rural community in Taiwan, which limits the generalizability of the results. Second, the small sample size reduced the power of the study. Third, we implemented a 4-week educational program with multiple follow-up periods for assessing the efficacy of the intervention on ACP. Although the optimal goal was reached by the end of the program, whether the effect on participants was maintained long term can only be determined through continual observation and support from health care providers. Fourth, GEE analysis for the primary outcomes could not be performed as mentioned above, thus the study validity could be influenced by the differences of the participants’ characteristics at baseline. Moreover, social desirability bias could also have interfered with the interpretation of average tendencies between groups and individual differences. Thus, the interpretation of the study outcomes should be made with caution.
Conclusion
The present study discovered that a theoretically based educational program improved AD uptake and selection of a hospice program as end-of-life care among rural-community-dwelling older adults. The program also improved participants’ knowledge, subjective norms, perceived behavior control, and behavioral intention of ACP for advanced dementia. The implementation of ACP is an area of increasing focus in contemporary health care because of its ability to improve the quality of end-of-life care and overall quality of life for patients and their families. Moreover, ACP helps in the effective use of medical resources, which in turn creates a “win-win” health care environment. The designed multimedia education program is an effective method of assisting ACP implementation among community-dwelling older adults.
Supplemental Material
Appendix – Supplemental material for Advance Care Planning and Advance Directives: A Multimedia Education Program in Community-Dwelling Older Adults
Supplemental material, Appendix for Advance Care Planning and Advance Directives: A Multimedia Education Program in Community-Dwelling Older Adults by Chiu-Hsiang Chiu wu, Shoa-Jen Perng, Chun-Kuan Shi and Hui-Ling Lai in Journal of Applied Gerontology
Footnotes
Acknowledgements
We thank the older adults who participated in this study.
Authors’ Note
Chun-Kuan Shi and Shoa-Jen Perng should be considered joint second authors. Ethical approval for the study was provided by the research ethics committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (IRB106-99-A).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.