
Abstract
Music & Memory (M&M) is a passive music intervention that uses personalized music playlists delivered on digital music players. This program has been increasingly adopted in nursing homes across the United States to facilitate communication, engagement, and socialization among persons with dementia (PWDs); however, few studies have evaluated the program’s effect on PWDs’ outcomes. In the present study, a randomized controlled crossover design was used to examine the impact of the M&M program on 59 PWDs in 10 nursing homes over a 14-week period. Residents’ evaluated outcomes included agitation, behavioral symptoms, and use of psychotropic medications. Although trends supported the positive effects of M&M, no statistically significant differences were found in any of the outcomes measured over time. Methodological limitations withstanding, these findings call into question the effectiveness of the M&M program and the ability of facility staff to implement this intervention with fidelity.
Background
More than five million Americans, nearly one in every nine older adults, are living with Alzheimer’s disease or another form of dementia (Alzheimer’s Association, 2016). In cases of Alzheimer’s disease, dementia’s most common form, impairments occur in cognitive ability, memory, language, reasoning, and judgment. Up to 90% of persons with dementia (PWDs) experience secondary behavioral or psychological symptoms, which become more prevalent in dementia’s advanced stages (Lyketsos et al., 2011; Trivedi et al., 2013). Secondary behavioral symptoms affect 75% of nursing home residents with dementia, with the most frequent problems being apathy (36%), depression (32%), and agitation/aggression (30%; Lyketsos et al., 2002). These problems are challenging and distressing not only to PWDs but also to family and professional caregivers, and they are often cited as the key reason for institutionalization (Agency for Healthcare Research and Quality [AHRQ], 2014; Gaugler, Kane, Kane, & Newcomer, 2005). They are further associated with care-related stress by staff and increased costs of care in the nursing home environment.
A common approach to managing behavioral symptoms associated with dementia in nursing homes is the use of psychotropic medication. It has been estimated that 33% of residents with dementia receive such medication (Kamble, Chen, Sherer, & Aparasu, 2009). In the past, typical anti-psychotics such as haloperidol and thioridazine were the most common treatments. However, meta-analyses of randomized controlled trials (RCTs) showed modest efficacy of typical anti-psychotic treatments for PWDs, and these treatments were known to have serious adverse side effects such as tardive dyskinesia and acute extrapyramidal symptoms (Kamble et al., 2009; Lanctôt et al., 1998; Schneider, Pollock, & Lyness, 1990).
Given the evidence for limited efficacy and serious potential side effects of pharmacological treatments, there has been an increasing effort to develop and implement non-pharmacological interventions to address the behaviors targeted by medications. The risks associated with these non-pharmacological treatments, such as increased agitation in some residents, are less frequent and severe than the risks associated with anti-psychotic medications (e.g., mortality; AHRQ, 2014). One non-pharmacological approach to improve behavioral outcomes is to use music interventions. Three broad categories of music interventions have been studied with PWDs: active music therapy, music-based interventions, and individualized music listening (ILM; McDermott, Crellin, Ridder, & Orrell, 2013; van der Steen et al., 2017; Vink, Bruinsma, & Scholten, 2003). Active music therapy is characterized by direct involvement between the patient(s) and a qualified music therapist, whereas music-based interventions are structured musical activities (e.g., rhythmic use of instruments, singing, movements associated with music) that are addressed to patient groups without requiring specific therapeutic goals or the presence of a structured therapeutic setting. The goal of ILM interventions is to help PWDs relax and experience a positive mood, thereby reducing agitation or behavioral problems. Key to this approach is the use of music preferred by the PWD; it does not require a trained music therapist or structured activities (Vink, Bruinsma, & Scholten, 2003).
Despite the progressive decline of cognitive functions in PWDs, receptivity to music among PWDs appears to remain until dementia’s late phases (Aldridge, 1996). Studies have reported that people with moderate to severe dementia (Norberg, Melin, & Asplund, 2003) are able to perceive pitch and melody (Vanstone & Cuddy, 2010), recognize titles of familiar songs (Johnson et al., 2011), and recall familiar lyrics (Prickett & Moore, 1991). Studies of individuals without cognitive impairment have shown that listening to favorite music selections is associated with retrieving memories (Wilkins, Hodges, Laurienti, Steen, & Burdette, 2012) and eliciting emotional engagement (Janata, 2009; Pereira et al., 2011). Hsieh, Hornberger, Piguet, and Hodges (2011) found that persons with Alzheimer’s disease maintained some ability to attach emotional meaning to music when they listened to famous tunes. Thus, for PWDs, familiarity with the music may activate cognition, establishing an emotional connection with the autobiographical past (Pereira et al., 2011).
Building on the potential of music to enable PWDs to retrieve memories and elicit positive emotions, ILM interventions involving PWDs’ listening to their preferred music aim to promote relaxation and enhance their emotional state. Ever since Gerdner’s (2000) seminal study showed positive effects of IML for reducing agitation among PWDs in nursing homes, IML programs have been used increasingly in long-term care facilities, in part owing to their low cost and ease of delivery. Yet, despite a substantial literature concerning the therapeutic effects of music, surprisingly few rigorous empirical evaluations of IML have been conducted. A recent review of empirical research on music therapy or listening programs with PWDs (van der Steen et al., 2017) found only 17 RCTs that tested music interventions. Of those studies, only three directly tested the effects of IML (Clark, Lipe, & Bilbrey, 1998; Guétin et al., 2009; Sakamoto, Ando, & Tsutou, 2013). Van der Steen et al. (2017) found support for positive effects of music-based interventions consisting of at least five sessions on reducing depressive symptoms, but not on other symptoms such as agitation, aggression, or cognition. The three RCTs of IML showed varying degrees of positive effects, such as reduced agitation and aggression (Clark et al., 1998; Sakamoto et al., 2013) or anxiety and depressive symptoms (Guétin et al., 2009). A recent evaluation of the Music & Memory (M&M) IML intervention, by Thomas et al. (2017), reported positive associations between M&M and reductions in anti-psychotic medication use, anxiolytic medication use, and behavioral and psychological symptoms among PWDs in nursing homes. However, Thomas et al.’s study was a retrospective analysis of the Minimum Data Set (MDS) without a randomized control group, and it lacked data on M&M implementation (e.g., which residents received the intervention and when they received it).
The potential effects of IML on improving quality of life among PWDs are promising. However, the evidence for the efficacy of IML or the M&M program is far from conclusive. In the present study, we use a randomized controlled crossover design to test the M&M program’s efficacy. This line of research is important, because M&M has been widely touted in the public media as wildly effective, even though the scientific literature has yet to show this to be the case. More studies are needed to clarify our understanding.
Method
Design
This crossover study was conducted to examine the efficacy of the M&M program for improving resident outcomes among 59 residents from 10 nursing homes over a 14-week observation period.
Sample
Stratified random sampling was used to select 10 nursing homes in four southeastern Wisconsin counties from 18 nursing homes in those counties that were participating in a statewide initiative to implement M&M. Participating nursing homes were Title 19 or Title 18/19 (medical assistance or Medicaid) facilities, had a minimum of 15 residents with a diagnosis of Alzheimer’s disease or other dementia as of the most recent MDS 3.0 census, and could not be under a Chapter 50 foreclosure. Strata were formed based on the size of facility, urban/rural location, and public/private ownership status. Within each facility, six long-term nursing home residents with dementia (mild, moderate, or advanced) were randomly selected out of the pool of all eligible residents.
To be included in the study, the residents had to meet the following criteria:
Be randomly selected from a pool of 15 or more potential participants from each of the 10 participating nursing home facilities,
Have a confirmed diagnosis of dementia or Alzheimer’s disease, and
Be a long-term resident (i.e., stayed in the nursing home for more than 30 days or have been determined as a long-term stay resident by the nursing home).
No other inclusion or exclusion criteria were used.
Residents were randomly assigned to one of two conditions (see Figure 1 for the study’s crossover design). Condition 1 received treatment-as-usual plus the M&M intervention for a 6-week period (Phase 1) followed by a 2-week washout period and a third period (Phase 2) during which only treatment-as-usual was provided for 6 weeks. Condition 2 received only treatment-as-usual during Phase 1 and the 2-week washout period but received the M&M and treatment-as-usual during Phase 2.
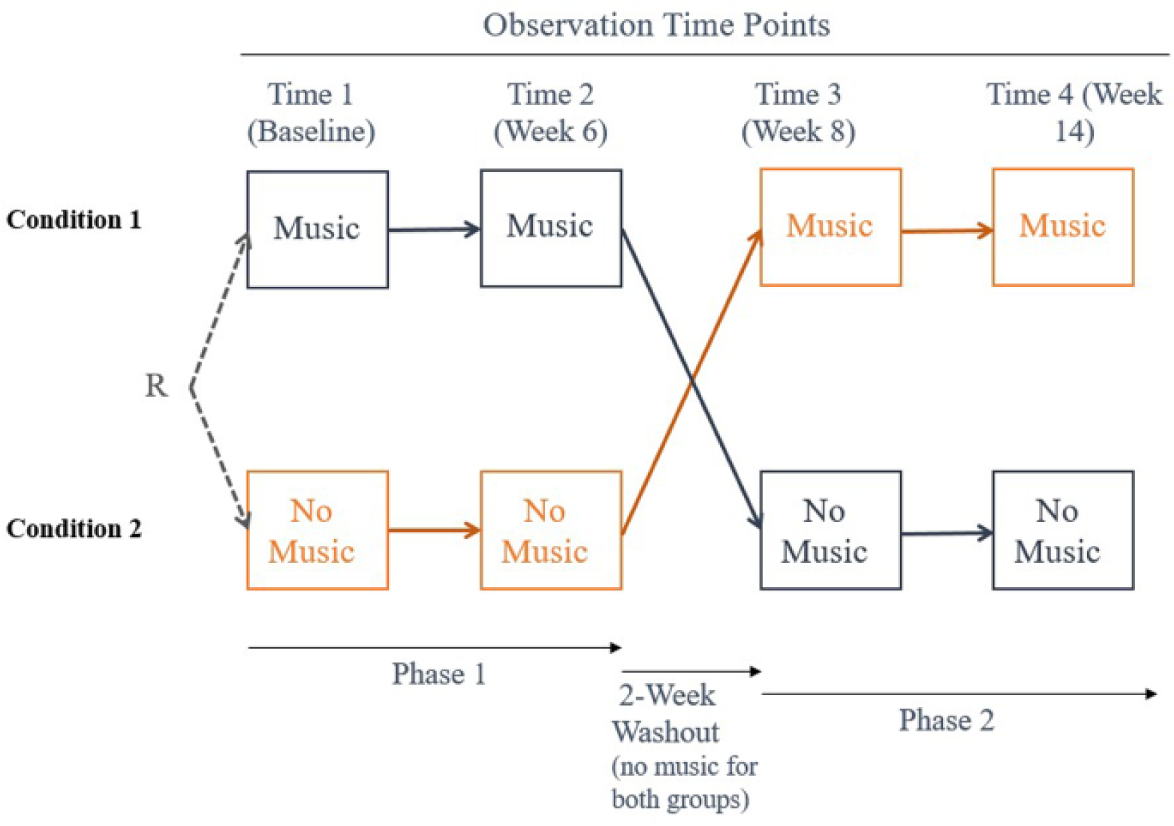
M&M cross-over study design.
The Music & Memory Intervention
The M&M intervention is an IML program developed by Music & Memory, a nonprofit organization in New York (http://musicandmemory.org). The program uses personalized music playlists delivered on iPods or other digital devices, which are set up by care staff trained in the program’s use. M&M emphasizes creating a playlist based on music that has personal meaning. The program suggests that PWDs (if they can communicate) or family members are the best source for identifying an individual’s music preferences as well as songs significant to that person’s life experience. M&M also suggests that in case a person is no longer communicative and family members have little information about their relative’s music preferences, caregivers can play music popular from the time the individual was a child or young adult, including music played on the radio or in popular television shows, and judge what is preferred based on the individual’s reaction to the music.
The general guidelines for implementation, from How to Create a Personalized Playlist for Your Loved One at Home (https://musicandmemory.org/training-publications/request-guide/), suggest that families should create a schedule for delivering the music, that it should be delivered at targeted times throughout the day (particularly for those with dementia), and that if the music does not seem to be effective, to try changing the selection. The guide also provides basic steps for compiling music playlists, such as asking the older adult relative questions about the types of music he/she listened to when young, finding music from particular relevant decades, or soliciting the assistance of another family member to build playlists. Similar guidelines were provided to staff members during their M&M training for the present study.
For this study, the M&M intervention was implemented solely by participating nursing home staff who were trained in the M&M program. The research team did not implement or provide ongoing fidelity checks to facilities during the study period. An important aspect of the M&M program, also possibly a reason for its popularity and rapid adoption by numerous nursing homes, is that it encourages and allows a great flexibility for facility staff to use their own clinical judgment and knowledge of their residents to tailor and implement M&M for each resident. Because such flexibility is an important aspect of the M&M program and the purpose of the study was to evaluate M&M’s implementation in nursing homes across the state, the research team did not want to alter how M&M was implemented by offering ongoing fidelity checks. At the same time, to assess the content, frequency, and dosage of the M&M intervention delivered to each resident by staff, the research team collected music listening data. Each iPod used for the study had an installed application that recorded a date/time stamp whenever the iPod was started, at the beginning of each song played, and when the music was paused or stopped. It further recorded the song title and name of the artist. These data allowed us to calculate durations of use by date and time for each resident.
In some homes, a single staff member was responsible, while in other homes, several staff and/or volunteers assisted with implementation. The M&M program provided training to at least one staff member from each nursing home and certified those staff in M&M’s use. The training was conducted via three 90-min webinar sessions in October 2013. Participants in the training were also granted access to a shared file system that contained documents with information that the staff could use to help create playlists for residents as well as maintain other aspects of the program, such as tips for maintaining and storing the equipment. Certified staff were encouraged to share updated versions of materials with staff from other agencies via the shared file system, which allowed for the development of a user community. Additionally, certified staff could access support from the M&M organization, as well as via regularly scheduled webinars.
Staff worked with the residents and their families, when possible, to create personalized playlists for each resident. After creation of the playlists, various staff members were responsible for administering the intervention to each resident. In some cases, a single staff member, typically the staff responsible for administering the intervention, would ensure its delivery to the participating residents. In other cases, staff, such as certified nursing assistants, who had not participated in the creation of the playlists, would assist with ensuring delivery to the residents. M&M’s delivery was determined on a resident by resident basis by the staff responsible for the intervention. While the dosage and frequency were partially based on what was deemed to be best for the individual resident, it was also dictated by the needs and staffing of the nursing home. The staff who were responsible for the M&M program at each home were instructed as part of their M&M training to update the playlists for each resident as needed to ensure that the music choices were enjoyed by the resident and were not causing distress.
Outcome Measures
Agitation was measured with the 29-item long form of the Cohen-Mansfield Agitation Inventory (CMAI; Cohen-Mansfield, Marx, & Rosenthal, 1989). The CMAI is typically used to examine agitation caused by cognitive impairment such as dementia. Survey items included agitated behaviors such as hitting, kicking, and biting, with the frequency of these behaviors over the past 2 weeks scored on a 7-point scale ranging from 1 = never to 7 = several times an hour. The CMAI’s four subscales represent physical aggressive, physical non-aggressive, verbal aggressive, and verbal non-aggressive behaviors, which we analyzed both comprehensively and distinctly.
Dementia-related cognitive–behavioral issues were measured using an abridged version of the Neuropsychiatric Inventory–Nursing Home Version (NPI-NH; Wood et al., 2000), which assesses 12 symptom categories: delusions, hallucinations, agitation/aggression, depression, anxiety, elation/euphoria, apathy, disinhibition, irritability/liability, lability, aberrant motor behavior, and appetite changes. For each symptom category, three questions assessed whether or not a symptom was present (yes, no, or not applicable), and if so, the frequency of occurrence within the past week (rarely to very often, 4-point scale) and the severity of the symptom (mild, moderate, or severe).
Medication use was measured by using a standardized form to record medication use from chart reviews, detailing the dose and type of medication used. These data were gathered via review of monthly medication reports. Patient chart data indicated that 214 different medications and supplements were prescribed to the 60 residents. Both the count of all the medications of a particular type (such as number of anti-anxiety medications) and the total medication count were used as final variables.
Background Characteristics
Demographic characteristics and diagnosis of behavioral disorders were gathered from chart reviews. Levels of activities of daily living dependence were assessed with the Katz Index (Wallace & Shelkey, 2008), which measures level of dependence (0) and independence (1) on six areas of activities of daily living, with possible scores ranging from 0 to 6. Progression of dementia was measured with the Clinical Dementia Rating Scale (Berg, 1988). The scale is used to examine the severity of six separate domains: memory, personal care, home and hobbies, community affairs, orientation to time and space, and judgment and problem solving. These domains are rated on a 5-point scale: none (0), questionable (0.5), mild (1), moderate (2), and severe (3), with possible total scores ranging from 0 to 18.
Intervention Exposure
Each iPod continually recorded events as the iPod was used. Specifically, the application entered a date/time stamp in a data file when the music player was started, at the beginning of each song played, and when the music was paused or stopped. It further recorded the song title and name of the artist. From this information it was possible to track all use of the devices for music listening and calculate durations of use by date and time.
Data Collection and Analysis
Residents were observed at baseline (Time 1), at the end of the 6th week (Time 2), after the 2-week washout, at the end of the 8th week (Time 3), and at the end of the 14th week (Time 4). At each point of the data collection, staff assessed and reported on residents’ behavioral indicators using the CMAI, NPI–NH, and Clinical Dementia Rating Scale; research assistants collected medication data.
Data summaries were created using univariate descriptive statistics (see Table 1). The CMAI total score and NPI-NH subscores were analyzed using general linear models (when the dependent variable was normally distributed) and generalized linear models (when the dependent variable was following another distribution type that could still be analyzed using linear methods). The models included both condition and time effects, as well as a condition by time interaction effect. Dependent variables that were not normally distributed were transformed using a power transformation method when possible, and those that did not transform well were re-examined using a randomization test based on a resampling approach to confirm the results.
Demographic Characteristics of Residents.
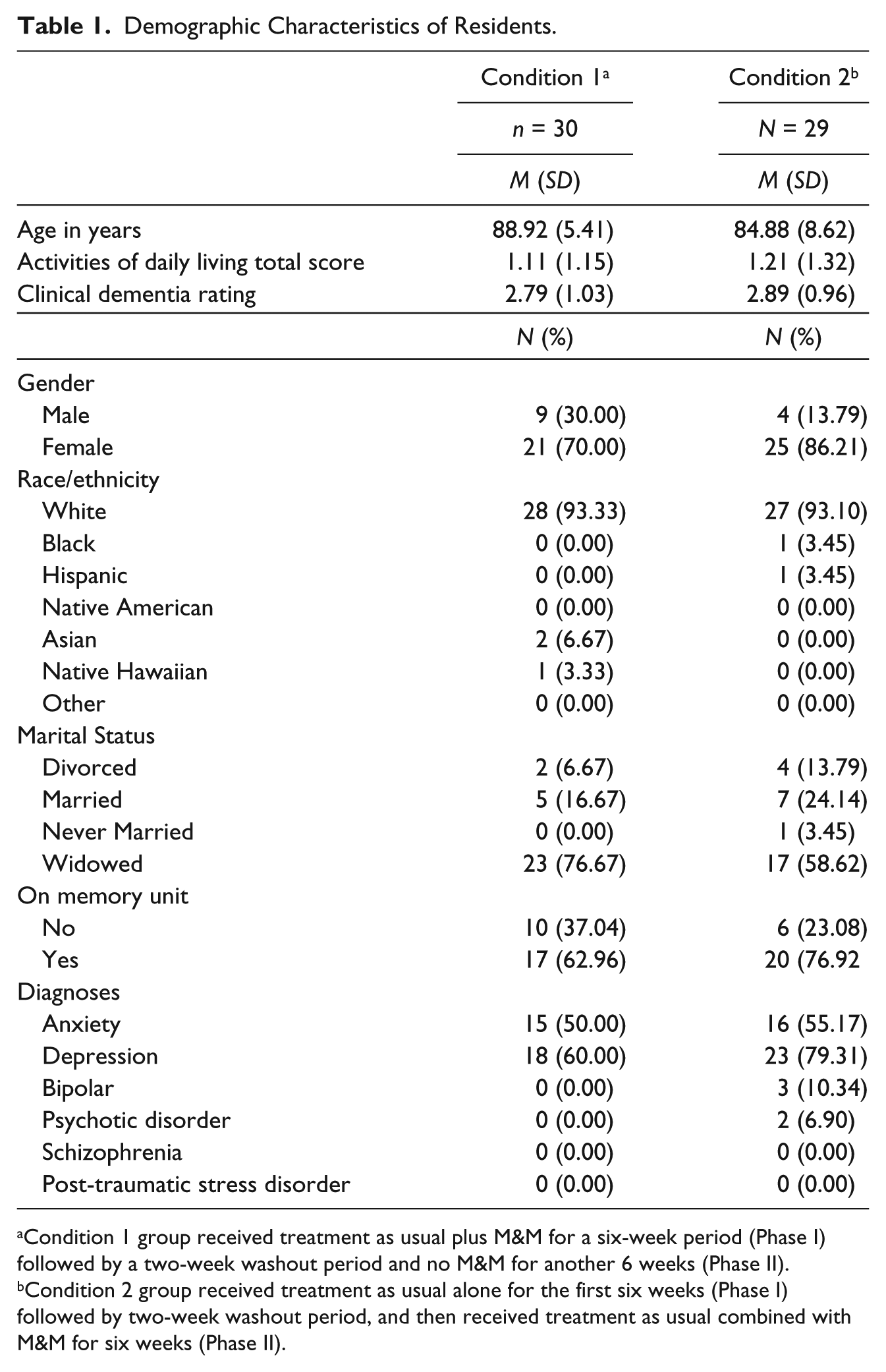
Condition 1 group received treatment as usual plus M&M for a six-week period (Phase I) followed by a two-week washout period and no M&M for another 6 weeks (Phase II).
Condition 2 group received treatment as usual alone for the first six weeks (Phase I) followed by two-week washout period, and then received treatment as usual combined with M&M for six weeks (Phase II).
Results
Baseline Characteristics
At baseline, a total of 59 residents participated in the study (see Table 1). The majority were female, white, widowed, and housed in a memory unit in their respective facilities. The primary psychiatric diagnoses at baseline included anxiety (52%) and depression (68%).
The majority of the residents, 85%, had adequate hearing or was able to hear with only minimal difficulty. The remaining participants, who had hearing difficulty and wore hearing aids, wore headphones over their hearing aids as recommended by the M&M program. Most participants were able to participate directly in creating their playlists; 67% of the sample were said to have clear speech, and 62% were able to make themselves understood and either understood others or usually understood others (data not shown).
M&M Intervention Exposure
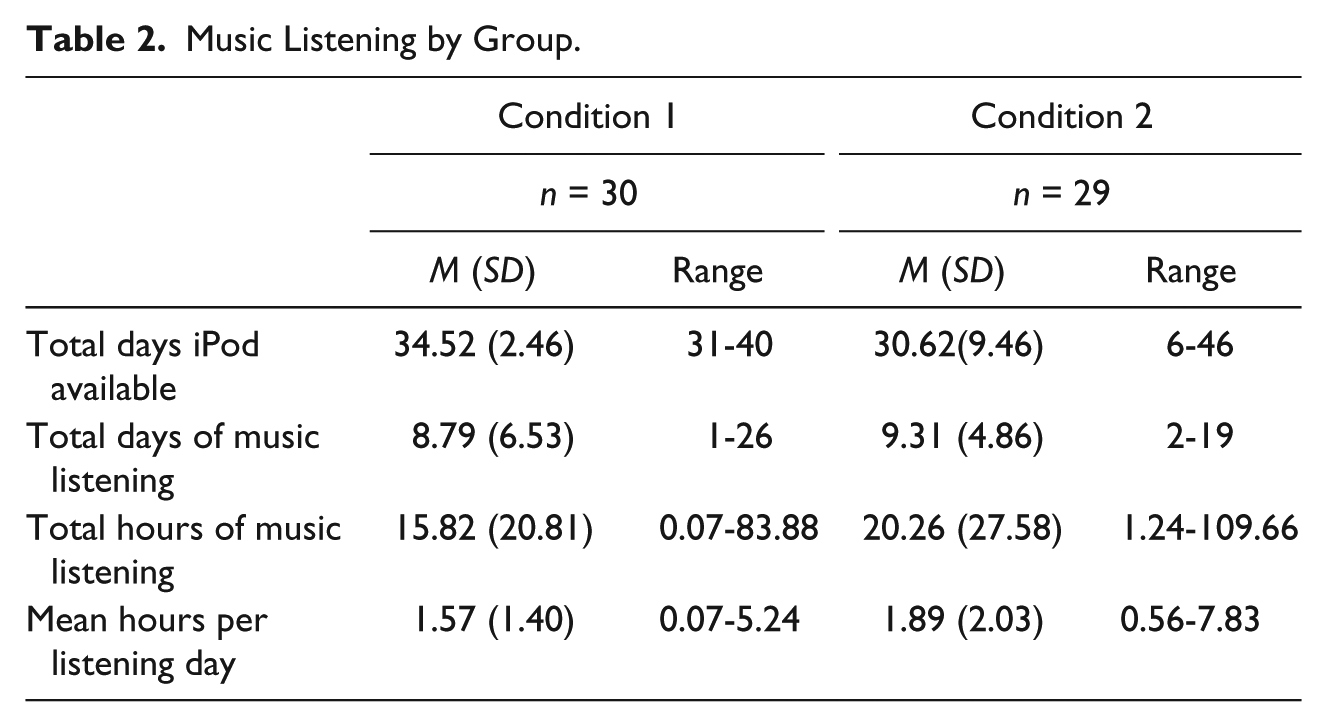
Participation rates and exposure to the M&M program are summarized in Table 2. On average, participants in Condition 1 (receiving M&M in Phase 1) used their iPods for 8.79 days (SD = 6.53) out of a total of 34.52 days (SD = 2.46) available, and those in Condition 2 (receiving M&M in Phase 2) used their iPods for 9.31 days (SD = 4.86) out of a total of 30.62 days (SD = 9.46) available. The total hours of music listening were 15.82 (SD = 20.81) for Condition 1 and 20.26 (SD = 27.58) for Condition 2. The mean hours of listening per listening day were 1.57 (SD = 1.40) for Condition 1 and 1.89 (SD = 2.03) for Condition 2. The SD and range values for various measures of music listening indicated considerable variability among residents in M&M program participation rates and exposure.
Music Listening by Group.
Outcomes
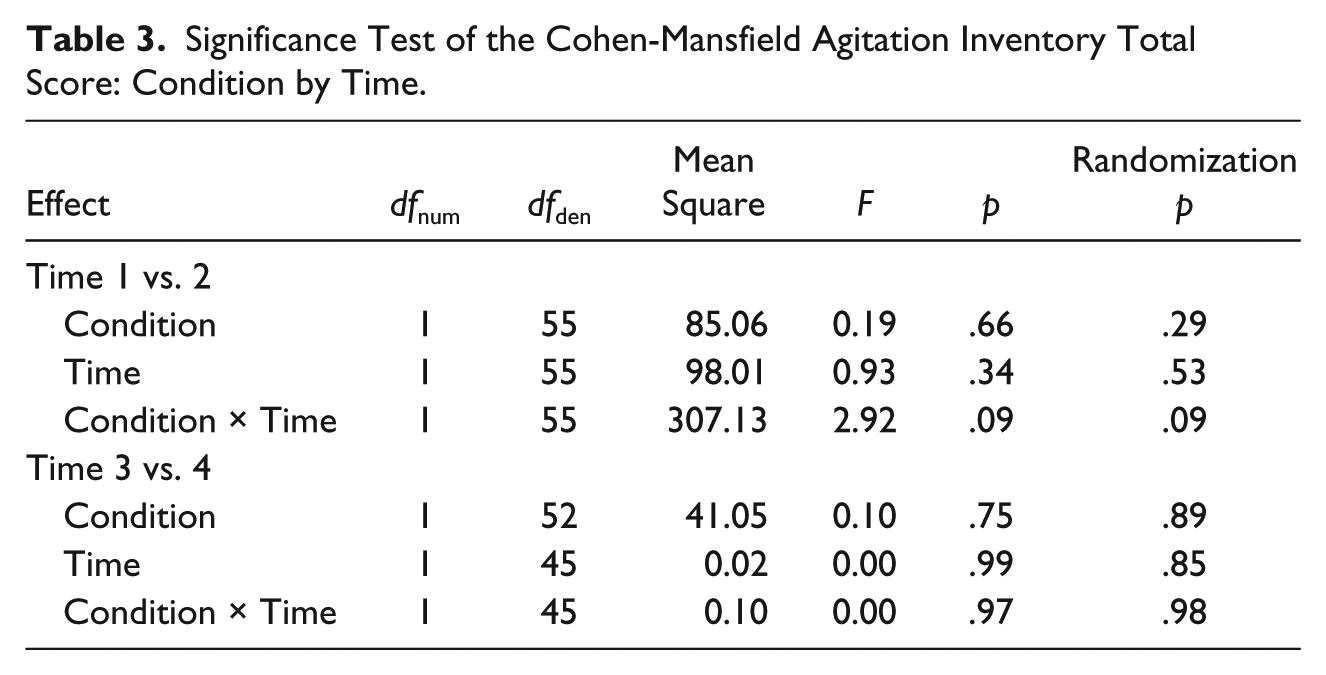
Overall, the results for three outcomes were contrary to what would be expected if the M&M intervention were positively influencing resident behaviors. For Phases 1 and 2, no effects of M&M were significant for the CMAI total score or any of the subscale scores (see Table 3, which reports the results on the total score only).
Significance Test of the Cohen-Mansfield Agitation Inventory Total Score: Condition by Time.
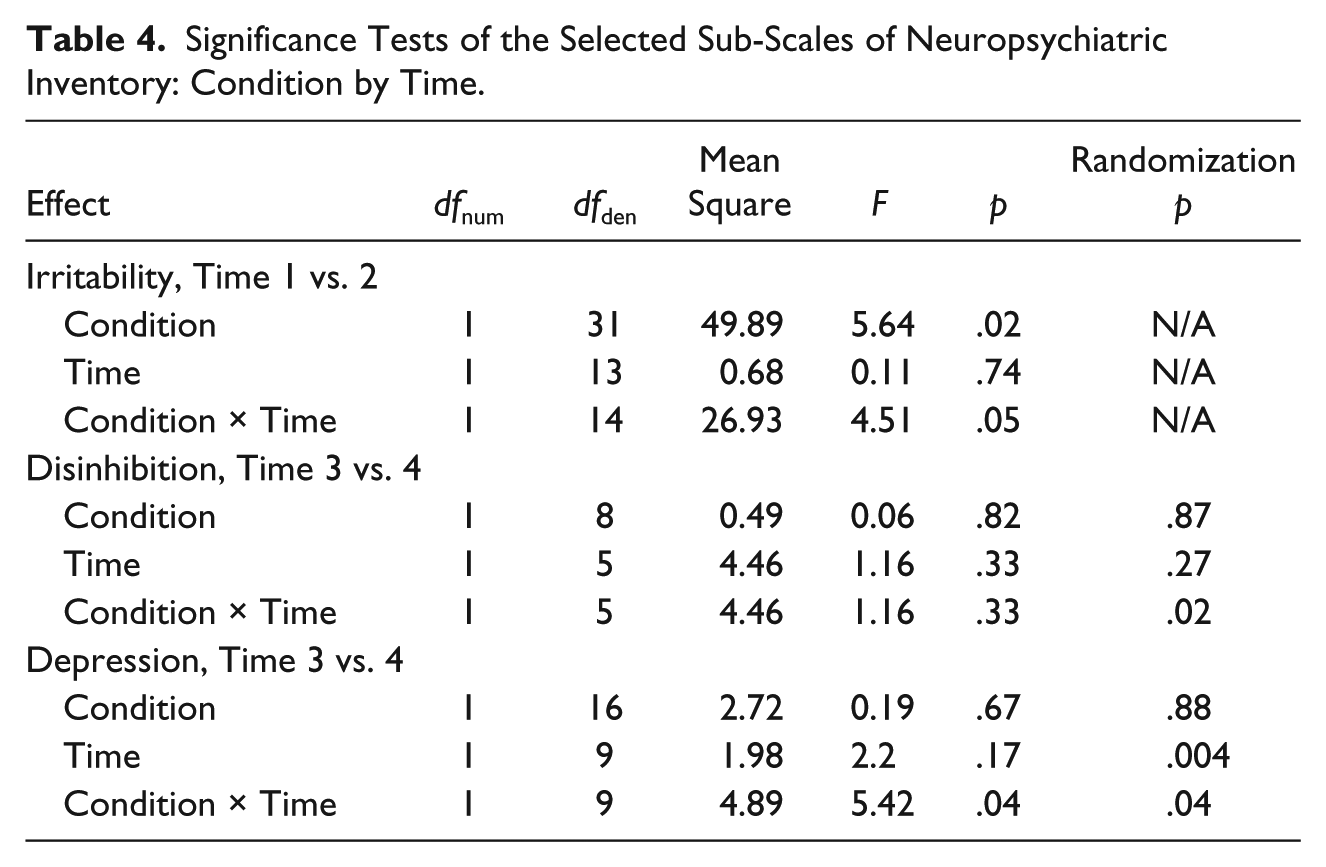
Among NPI subscales, effects were significant for irritability in Phase 1 and disinhibition and depression in Phase 2 (Table 4). Condition 1 in Phase 1 (M&M) showed increases over time for irritability while Condition 2 showed decreases. Disinhibition decreased from Times 3 to 4 in Condition 1 (treatment-as-usual) and increased in Condition 2 (M&M) in Phase 2. However, the condition by time interaction for NPI depression during Phase 2 was significant, indicating an increase in depression over time in Condition 1 (treatment-as-usual) and a decrease in depression in Condition 2 (M&M).
Significance Tests of the Selected Sub-Scales of Neuropsychiatric Inventory: Condition by Time.
Lastly, no significant effect was observed on use of medication (data not shown). None of the condition by time interaction effects reached significance for the medication total or any of the medication indexes.
Discussion
M&M is a popular intervention program that has been increasingly adopted in nursing homes to support PWDs. M&M’s underlying premise is that musical favorites tap into deep memories that have not been lost due to dementia, and that this can facilitate resident communication, engagement, and socialization. In this study, we evaluated the M&M program using a prospective RCT design. In addition, unlike Thomas et al. (2017), we collected music listening data to assess dosage and frequency of the M&M intervention among residents. Overall, the results from this crossover study suggest that, contrary to our expectations and the findings of Thomas et al., M&M had little or no effect on improving resident outcomes in the areas of agitation, mood, and medication. Hence, the data from participants in the present study question the efficacy of the M&M program in affecting the outcomes that we measured. There are several possible explanations for our results.
First, the sample size in this crossover study may have been too small to achieve statistical significance. For example, the CMAI total score for Phase I showed changes consistent with positive effects of M&M, but none of the statistical tests’ results were significant. In preparation for this study, we performed our power analysis on the basis of studies that prescribed the use of music to specifically target behaviors such as agitation. The effect sizes reported in that research were moderate in size on the low end. For example, a meta-analysis by Vasionyte and Madison (2013) concluded that music interventions with PWDs produced a large positive effect on behavioral, cognitive, and physiological outcomes, and a moderate effect for affect. Individual music interventions have further been shown to obtain a larger effect than have group sessions. In this evaluation, however, the failure to replicate similar patterns of change during Phase 2 suggests that even the patterns observed in Phase I should be interpreted with caution. This fact, coupled with the inconsistent trends observed over the aggregate set of measures, does not support an inference of failure to observe change due to low statistical power alone.
A second possible explanation is our use of global measures of functioning collected over several week intervals. Some prior research that has measured change in behaviors in close proximity to music listening found that behaviors such as agitation decreased for up to an hour after listening ended (e.g., Gerdner, 2000). However, some of these studies (Park & Pringle, 2009) also measured agitation more globally, using instruments based on CMAI, and found lasting effects even when listening occurred only a few times each week. Guétin et al. (2009) reported that participants in an individual music listening group had lower anxiety scores at Weeks 4, 8, and 16 in comparison with a control group. Given the findings of other investigators, it is doubtful that the length of observation period for our evaluation contributed significantly to the lack of statistically significant results.
A third possible explanation might be our reliance on staff reports on key resident outcome measures such as the CMAI and the NPI-NH. The evaluation team asked participating facilities to identify direct care staff who were most familiar with and had the most frequent interaction with residents participating in the study. The identified staff then reported on these measures. Despite our request, the best staff may not have been identified to complete the measures. Hence, there is a possibility of reduced reliability and validity of staff reports on these measures.
Fourth, it may be that the M&M program was not implemented according to the guidelines recommended by the M&M organization or that the M&M guidelines are insufficient in comparison with evidence-based practice guidelines for the implementation of IML programs. A primary research basis for the M&M program is the work of Gerdner and Schoenfelder (2010). However, our observations during data collection and the analysis of the music data suggest low fidelity among the facilities to the M&M program guidelines and especially to evidence-based practice guidelines available in the literature (e.g., Gerdner & Schoenfelder, 2010). Gerdner and Schoenfelder (2010), who outlined specific steps for the use of IML interventions, specified a protocol for developing individualized musical playlists as well as the need to audit the processes that are central to this approach. Information from the M&M program website (http://musicandmemory.org) indicates that some specific direction is given to facility teams to be certified for the program regarding music selection and delivery protocol as well as acquisition of iPods and fundraising. However, it is unclear whether the M&M program has developed or implemented fidelity checking and ongoing assessment in M&M-certified facilities to ensure that the recommended guidelines are followed. Moreover, data on music listening duration and frequency show that the implementation of M&M varied considerably from facility to facility and from person to person within each facility. Although the variation itself is unsurprising, given that the program is meant to be person centered, it is unclear how much work is done to ensure that the dose and frequency provided to each participant are in fact correct for that participant.
Despite the lack of significant findings, the present study has importance for practitioners and, to a larger extent, researchers. The anecdotal evidence of the impact that M&M can have on older adults with cognitive impairment may hold the key to interpreting and applying our findings. The widely viewed 2014 documentary Alive Inside showed previously non-responsive nursing home residents literally enlivened when exposed to their favorite music via M&M. Previous studies, although lacking in rigor, have also demonstrated positive benefits from M&M (van der Steen et al., 2017). Practitioners currently using or considering using the M&M intervention are encouraged to do so based on this evidence, the intervention’s low cost, and its risk-free nature. As previously mentioned, fidelity appears to be critical, and practitioners should receive training, support, and ample time to administer M&M as it was designed and intended. When interventions such as M&M are introduced as “additional tasks” for frontline staff, fidelity may be compromised. Practitioners should also work closely with researchers to help identify potential outcomes of the M&M program. Engagement in a more interactive translational and participatory research process could remedy this issue.
Moreover, the M&M program may benefit from future research to identify specific methods to aid staff in the individualized selection of music, as well as in the measurement and titration of the dose and frequency of the program to optimize its effects. For instance, PWDs can have a variety of triggers for agitation (e.g., time of day, events, or tasks); observation and assessment of those triggers might help staff identify appropriate periods for targeted music listening. In addition, the protocols for developing individualized musical playlists, for auditing use designed around specific periods of agitation, and for ongoing assessment should be clearly presented to facilities participating in training and demonstration. Goals and the assessment of progress toward meeting them should be discussed and coordinated with other care team members routinely within facilities.
The findings of this study also highlight the challenges both of conducting applied research with PWDs, especially with regard to identifying subgroups of PWDs most likely to benefit from an intervention, and of determining appropriate outcome measures for PWDs. A more targeted approach to identify a subgroup of PWDs for music interventions may be needed. Hsieh et al. (2011), for example, found that persons with Alzheimer’s disease were more likely to maintain some ability to attach emotional meaning to facial expressions or music when listening to familial music (hence, they were more likely to experience positive emotions) than were persons with semantic dementia. Future studies with larger samples of those with different types of dementia could help identify PWDs more suited for music interventions.
Identifying the key target areas for M&M intervention is another important consideration for future research. Effective non-pharmacological interventions for PWDs are directed at single behaviors such as agitation. PWDs manifest varying types and degrees of challenging symptoms. Some PWDs may have more reserved memory and cognitive abilities than others, and for them, improving or maintaining cognitive function may be the desirable outcome. For others with more advanced stages of dementia, the targeted areas might be agitation, aggression, anxiety, depression, or apathy. Thus it would be important to identify and target one or two key symptoms that seem to affect the individual the most.
M&M seems to hold the potential to improve moments within the lives of PWDs, but the findings of this study suggest that M&M may not have the potential to improve well-being over the long term. As such, outcome measures should be time-sensitive and data collection should be designed to capture moments of improved mood. In addition to quantitative measures, researchers should consider the use of qualitative and more refined observational measures, such as facial reactions and body posture. Other researchers have acknowledged this challenge with psychosocial interventions for PWDs and have suggested that simply bringing moments of joy rather than changing lives may be a more appropriate and realistic goal (Gridley, Brooks, Birks, Baxter, & Parker, 2016). Given consistent findings that support the short-term efficacy of a variety of music interventions to improve behavioral outcomes among PWDs (McDermott et al., 2013), the challenge lies with researchers and practitioners to better understand how to implement and measure M&M’s potential to improve domains of quality of life that for PWDs are meaningful.
Footnotes
Acknowledgements
We would like to thank Mike Brondino, PhD for methodological design and statistical analysis support for the project, Chris Cho, MS for statistical analysis support for the manuscript, and undergraduate project assistants and the University of Wisconsin-Milwaukee Undergraduate Research Fellows (SURF) Award program for assistance with data collection.
Author Contributions
Jung Kwak contributed to the study’s conception and design, the interpretation of results, and the drafting and editing of the manuscript.
Keith Anderson contributed to the interpretation of results and writing of the manuscript.
Katherine O’Connell Valuch contributed to the study’s design, acquisition of data, and writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study received approval from the University of Wisconsin-Milwaukee Institutional Review Board, IRB Approval # 14.270.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data used in the study were collected with grants from the Bader Philanthropies, Claude Pepper Center, Florida State University, My Choice, Family Care, and Wisconsin Department of Health Services (Civil Money Penalty (CMP) Funds). Editorial support with manuscript development was provided by the Cain Center for Nursing Research and the Center for Transdisciplinary Collaborative Research in Self-management Science (P30, NR015335) at The University of Texas at Austin School of Nursing.