
Abstract
Nursing home resident obesity increases the complexity of nursing care, and nursing homes report avoiding residents with obesity when choosing which prospective residents to accept. The objective of this study was to examine the associations between nursing home obesity prevalence rate and nursing home organizational, staffing, resident, and geographic factors within a profit maximization framework. The study cohort included U.S. Centers for Medicare and Medicaid Services data from U.S. nursing homes in 2013. Study findings supported hypothesized associations between obesity prevalence rate and higher occupancy, higher bed capacity, and multi-facility affiliation, but findings did not support a relationship between obesity prevalence rate and for-profit status.
Keywords
Background and Objectives
An important and underrecognized demographic shift in nursing homes has been a higher prevalence of obesity among nursing home residents. Obesity in adults is generally defined as a body mass index (BMI) of 30 kg/m2 or greater by the World Health Organization (WHO), and in the United States, obesity has increased among adults from 12% in 1991 to 38% in 2014 (Flegal, Kruszon-Moran, Carroll, Fryar, & Ogden, 2016; Mokdad et al., 1999). As people with obesity make up a greater proportion of the overall elderly and disabled population, they constitute an increased proportion of the nursing home population. In a sample of U.S. nursing home residents from 2000 to 2008, the prevalence of obesity increased from 17% to 26% (Cai, Rahman, & Intrator, 2013). Many of these residents have moderate (BMI 35-39.9 kg/m2) to severe (BMI ≥40 kg/m2) levels of obesity; the prevalence of moderate to severe obesity was 12% by 2008.
This rise in obesity among nursing home residents poses numerous difficulties for facilities (Harris & Castle, 2017). Residents with obesity have different needs than residents of normal weight, and these different needs require unique resources to manage properly. They may need special equipment, including patient lifts, as well as larger beds, walkers, chairs, treatment tables, doorways, and bathrooms (Dimant, 2005; Gallagher, 2005). They are more likely to need two or more people to assist them with all activities of daily living (Harris, Engberg & Castle, 2018). Furthermore, the time needed for staff to perform duties like bathing is increased, usually doubling the time needed to perform tasks (Felix et al., 2009). Residents with obesity are more likely to have a longer length of stay, more likely to be readmitted to a hospital, and less likely to be discharged back to the community (Kosar, Thomas, Gozalo, Ogarek, & Mor, 2018). Nursing home administrators have recognized these challenges and take obesity into account when considering a possible resident for admission to their nursing home. A survey of nursing home administrators in Arkansas and Pennsylvania found that extreme obesity, defined in the study as someone weighing 325 pounds or more, was considered a barrier to admission for two thirds of administrators (Felix, Bradway, Ali, & Li, 2016). Specifically, they reported concerns about the availability of equipment and staff as important reasons why they may decline admission to a prospective resident with extreme obesity. In summary, the custodial and rehabilitation care for residents with obesity requires more resources in terms of staff number, staff hours, and facility equipment (Harris & Castle, 2017).
The cost of these increased services and resources and the question of whether payers adequately reimburse for these extra services and resources also is a concern to nursing home administrators. The Medicare Resource Utilization Group (RUG) payment system does not explicitly factor for obesity. RUG does factor in activity of daily living (ADL) impairment relating to bed mobility, toileting, and transferring, but residents with obesity generally have lower levels of ADL impairment than nonobese residents (especially eating-related ADL) and so may qualify for lower payments than less obese residents (who may have more medical conditions, lower cognitive status; Kosar, Thomas, Gozalo, & Mor, 2018; Harris et al., 2018). While there is little research focused on costs and payments related to residents or patients with obesity, there is a high degree of concern for this in multiple survey studies. In the survey of nursing home administrators, 43% of respondents noted that lower reimbursement for services often or always acts as an admission barrier for prospective severely obese residents; when they asked hospital case managers, 57% of respondents thought that lower reimbursement for services for residents with obesity was often or always acts as a barrier to placement in a nursing home (Miles et al., 2012). Every nurse in a 25-subject study of nurses who provide long-term care reported that reimbursement was a significant challenge; also participants discussed the difficulty in receiving reimbursement for extra-large equipment necessary for providing good care (Gallagher, 1998). A case report, extrapolating the cost of bathing care for a single resident with severe obesity, found that this would amount to an extra US$1,190 per resident per year compared with a similar resident of normal weight (Felix et al., 2009). These increased costs make the care of residents with obesity less profitable, further decreasing the small profit margins associated with most nursing home businesses (Bowblis, 2015; Eljay LLC, 2009).
There is a wide variation in obesity prevalence rate among nursing homes, which may suggest that residents with obesity select or are selected into certain types of nursing homes. When nursing homes in New York State that had a greater-than-average resident obesity prevalence rate were compared with those with less-than-average resident obesity prevalence rate, there were significant differences in financial resources, staffing levels, occupancy rates, for-profit status, and chain affiliation (Zhang, Li, & Temkin-Greener, 2013). Furthermore, nursing homes with a greater-than-average prevalence of obesity are associated with low metrics of quality (i.e., administrative deficiencies) compared to nursing homes with a less-than-average prevalence of obesity (Zhang, Lu, Xu, & Gurwitz, 2016).
For these reasons, we need a greater understanding of the characteristics of nursing homes that are more likely to care for this growing demographic. Previous work in this area explained associations between obesity and nursing home characteristics as a response to changes in market demand and did not address the lower profitability of residents with obesity. Previous research has other important limitations, including using data limited to a single state, did not separately analyze short- and long-stay residents, and not accounting for geographic variation in resident and nursing home characteristics—for example, county obesity prevalence rate or the proportion of older adults with income below poverty level. The objective of this study was to test hypotheses based on profit maximization theory to explain associations between nursing home organizational characteristics and higher prevalence of obesity within short- and long-stay resident populations in U.S. nursing homes.
Research Design and Method
We derived our conceptual framework for understanding the effect of obesity on facility characteristics from profit maximization theory. Profit maximization theory holds that rational organizations will determine the price and output quantity that leads to the greatest profit (Penner, 2004). Assuming residents with obesity require more resources (e.g., staff members, staff time, and equipment), using more resources increases costs to the nursing home, and reimbursement does not increase proportionally with the higher costs, care for residents with obesity is a low or negative profit margin activity. Our overall hypothesis is that because residents with obesity have a lower profit margin than similar residents with normal weight, residents with obesity will not be accepted by nursing homes that can accept another, more profitable resident, but will be accepted by facilities that have staffing or equipment availability or flexibility to make the care for such residents more profitable. Care for short-stay residents, often admitted for post-acute, rehabilitation care, is frequently reimbursed at rates which are much higher than long-stay rates (MedPAC, 2015). To account for this difference in behavior related to short- and long-stay status, we analyzed these two groups separately. Utilizing this profit maximization framework, the following hypotheses relate facility characteristics to nursing home obesity prevalence rate:
Data Sources
The Centers for Medicare and Medicaid Services (CMS) Minimum Data Set (MDS) from 2013 was used to define obesity prevalence rate for each nursing home in the United States. MDS includes all residents of U.S. nursing homes accepting federal funding. Its data have been validated in its clinical accuracy and relevance in comparison with research nurse assessments, and the reliability of the MDS has been studied many times and has generally been noted to be good (Hawes et al., 1995; Poss et al., 2008; Saliba & Buchanan, 2012). It includes nearly 400 data elements for each assessment, including biometrics (height and weight), demographics, health conditions, cognitive function, functional status, services received, continence status, and skin assessments. The MDS was completed for all residents on at least three occasions: on admission, annually, and if the resident shows significant change. A subset of MDS fields must be completed quarterly. To define the study sample, we limited the cohort to residents present on the first Thursday in April 2013 (April 4, 2013). This methodology is used to standardize measurements of nursing home populations between years, including the Long-Term Care Focus data set from Brown University (LTCFocus, 2018; Tyler et al., 2013).
Nursing Home Compare is a data set of facility characteristics and ratings maintained by CMS and published on Medicare.gov to help prospective residents and their families evaluate nursing homes in the United States. These data were compiled from nursing home survey data collected by CMS, including the Certification and Survey Provider Enhanced Reporting (CASPER) system. We used this data to identify facility characteristics, including for-profit status and staffing levels. Additional facility information came from publicly available Long-Term Care Focus data produced at Brown University.
County-level metropolitan-status geographic characteristics concerning obesity, population size, poverty, rural location, and nursing home competition were collected from the Area Health Resources files, a database maintained by the U.S. Department of Health and Human Services’ Health Resources and Services Administration. County-level age-adjusted obesity rates were collected from the Centers for Disease Control and Prevention’s Diabetes Surveillance System.
Study Sample
All U.S. nursing homes in 2013 met the inclusion criteria. When calculating nursing home obesity prevalence rate, all nursing home residents with missing information on height and weight were excluded (n = 36,781, 2.2% of MDS residents). Within each nursing home, height and weight were consistently reported (the median prevalence of residents with missing height or weight within a nursing home was 0.4%, mean 1.4%, standard deviation 2.1%), and therefore no nursing homes were excluded due to excessive missing values of resident height or weight. Nursing homes with missing data on organizational, staffing, resident, and geographic factors were excluded (n = 301, 2.0% of nursing homes). The final sample size was 14,812 nursing homes.
Dependent Variable Definitions
Obesity is defined by the WHO as a BMI of 30 kg/m2 or greater. The dependent variable for this analysis was the nursing home obesity prevalence rate defined as the proportion of residents who were obese in each nursing home calculated using resident-level data from the MDS. We calculated this for all short-stay residents (length of stay <100 days) and all long-stay residents (≥100 days) separately. As a sensitivity test of this definition, we repeated the analysis with a more extreme definition of obesity: the prevalence of severe obesity, BMI of 40 kg/m2 or greater, within each nursing home.
Independent Variable Definitions
Organizational independent variables included the dichotomous variables for-profit status, hospital-based affiliation status, multi-facility affiliation status, the presence of special care units, and continuing care retirement community. Other organizational and staffing variables included total bed capacity, occupancy rate (proportion of beds occupied), the proportion of Medicare residents, and the proportion of Medicaid residents. Staffing variables included nurse aide, licensed practical nurse (LPN), registered nurse (RN), and physical therapist staffing hours (hours per resident per day).
Resident demographic-related independent variables included the proportion of residents in each nursing home with the following characteristics: female gender, Black, Medicare insurance, Medicaid insurance, and Alzheimer’s disease. Other resident variables include the mean acuity index and the mean age of residents for all residents. The mean acuity index is a standard measure of resident case-mix that combines ADL dependencies and special treatment measures for all residents in each facility, reported as a weighted sum of specific resident characteristics; it is calculated from CASPER (Feng, Grabowski, Intrator, & Mor, 2006).
County-level geographic independent variables included age-adjusted mean obesity prevalence rate, proportion of county residents 65 years and older who live in deep poverty (income ≤50% of federal poverty level), proportion of county residents 65 years and older who are Medicaid eligible (income ≤135% of federal poverty level), the Herfindahl–Hirschman Index based on beds per facility, and mean population of county residents 65 years and older.
Statistical Methods
Descriptive characteristics of all study variables were reported by tertile of nursing home obesity prevalence rate. Significance between nursing home obesity prevalence rate and covariates was evaluated using bivariate linear regression models separately by short- or long-stay status. Independent associations between organizational, staffing, resident, and geographic factors and nursing home obesity prevalence rate were evaluated using multivariable linear regression with Huber–Eicker–White robust standard errors to adjust for county-level clustering of nursing home characteristics present in the collected data (White, 1980). In a sensitivity analysis, the estimates were repeated using nursing home severe obesity prevalence rate. Stata 15.1 software was used for all analyses. This study and data were deemed exempt from human subject review by the University of Pittsburgh Institutional Research Board (PRO10010141).
Results
The final cohort included 14,812 nursing homes. The mean nursing home obesity prevalence rate in nursing homes was 31.1% (SD = 8.8); the prevalence of BMI 30 to <35 kg/m2, 35 to <40 kg/m2, and ≥40 kg/m2 was 16.5%, 7.7%, and 6.9%, respectively. There is a wide range of nursing home obesity prevalence rate among U.S. nursing homes: The interquartile range of the nursing home obesity prevalence rate was 25.4% to 36.4%, and the 5th to 95th percentile range was 17.3% to 45.8%.
The characteristics of the nursing homes are shown in Table 1 by nursing home obesity prevalence rate tertile. Bivariate regression of nursing home obesity rate with each characteristic noted small but significant trends for most characteristics. Related to the study hypotheses, nursing home occupancy decreased (84.2% in the low nursing home obesity prevalence rate tertile compared with 80.5% in the high tertile, p < .001) and the proportion with for-profit status increased (64.2% in the low tertile compared with 72.9% in the high tertile, p < .001). The proportion of short-stay residents decreased (24.6% in the low tertile compared with 22.1% in the high tertile). The proportion of nursing homes having hospital-based affiliation increased (4.9% in the low tertile compared with 6.8% in the high tertile, p < .001), the proportion with multi-facility affiliation increased (49.6% in the low tertile compared with 59.4% in the top tertile, p < .001), and nursing home bed capacity decreased (105 beds in the low tertile compared with 100 beds in the high tertile, p < .001).
Nursing Home Characteristics by Obesity Prevalence Rate Tertile.
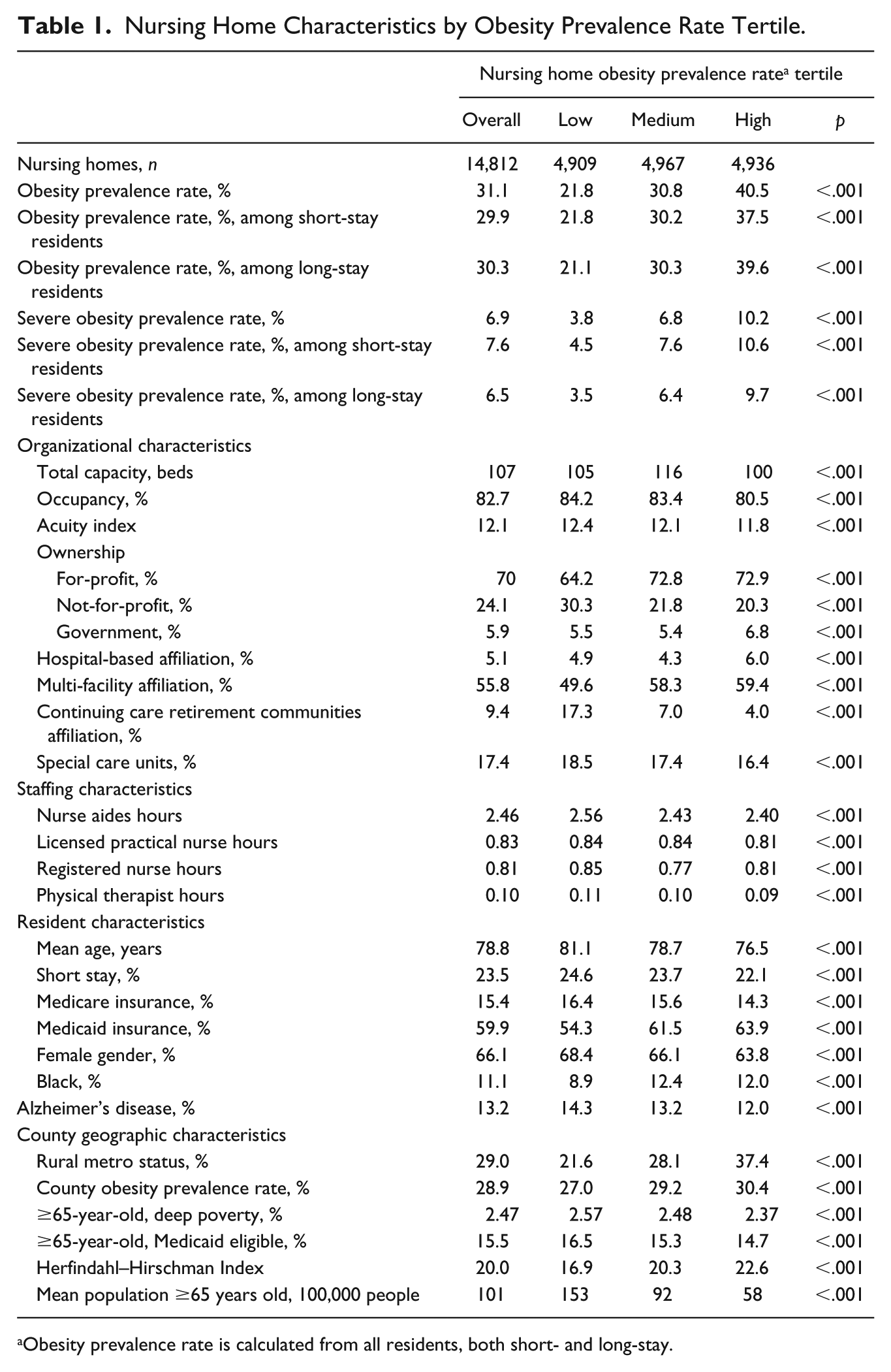
Obesity prevalence rate is calculated from all residents, both short- and long-stay.
Controlling for organizational, staffing, resident, and geographic factors, Table 2 presents the results of the multivariable models. Related to the study hypotheses, occupancy was associated with higher nursing home obesity prevalence rate (p = .020) among long-stay residents, but not short-stay residents (Hypothesis 1). For-profit status was not associated with higher nursing home obesity prevalence rate (Hypothesis 2). Multi-facility affiliation was associated with higher nursing home obesity prevalence rate (p < .001 for short-stay residents and p = .003 for long-stay residents), but higher bed capacity was associated with higher obesity prevalence rate (<.001) but only for short-stay residents (Hypothesis 3).
Adjusted Coefficients for the Relationship Between U.S. Nursing Home Characteristics and Obesity Prevalence Rate (n = 14,812).
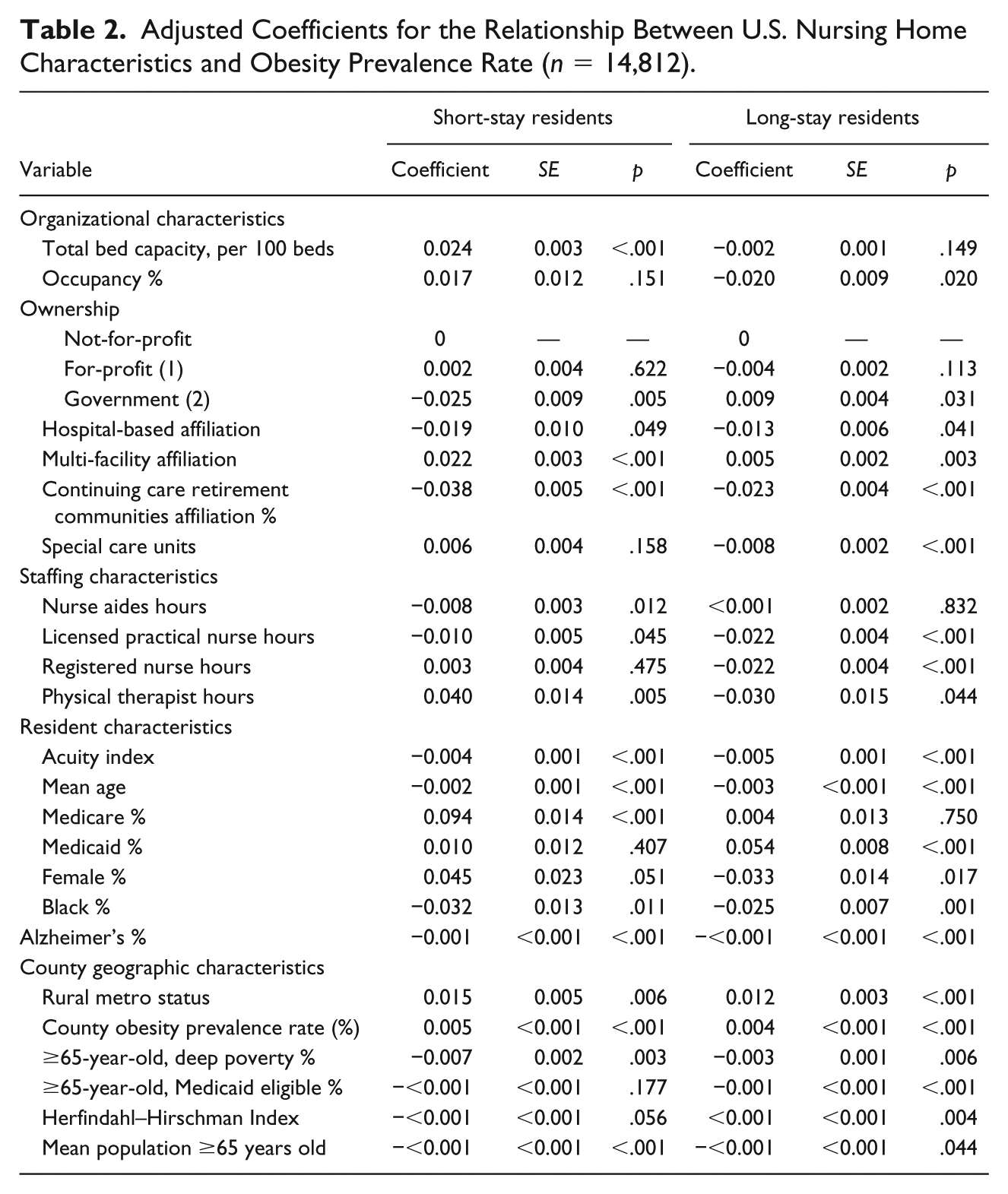
Nursing homes with higher LPN and RN staffing hours were associated with lower nursing home obesity prevalence rate. In rural counties, higher community-levels of obesity, moderate to severe levels of poverty, smaller elderly populations, or a lower number of nursing homes were all associated with higher nursing home obesity prevalence rate.
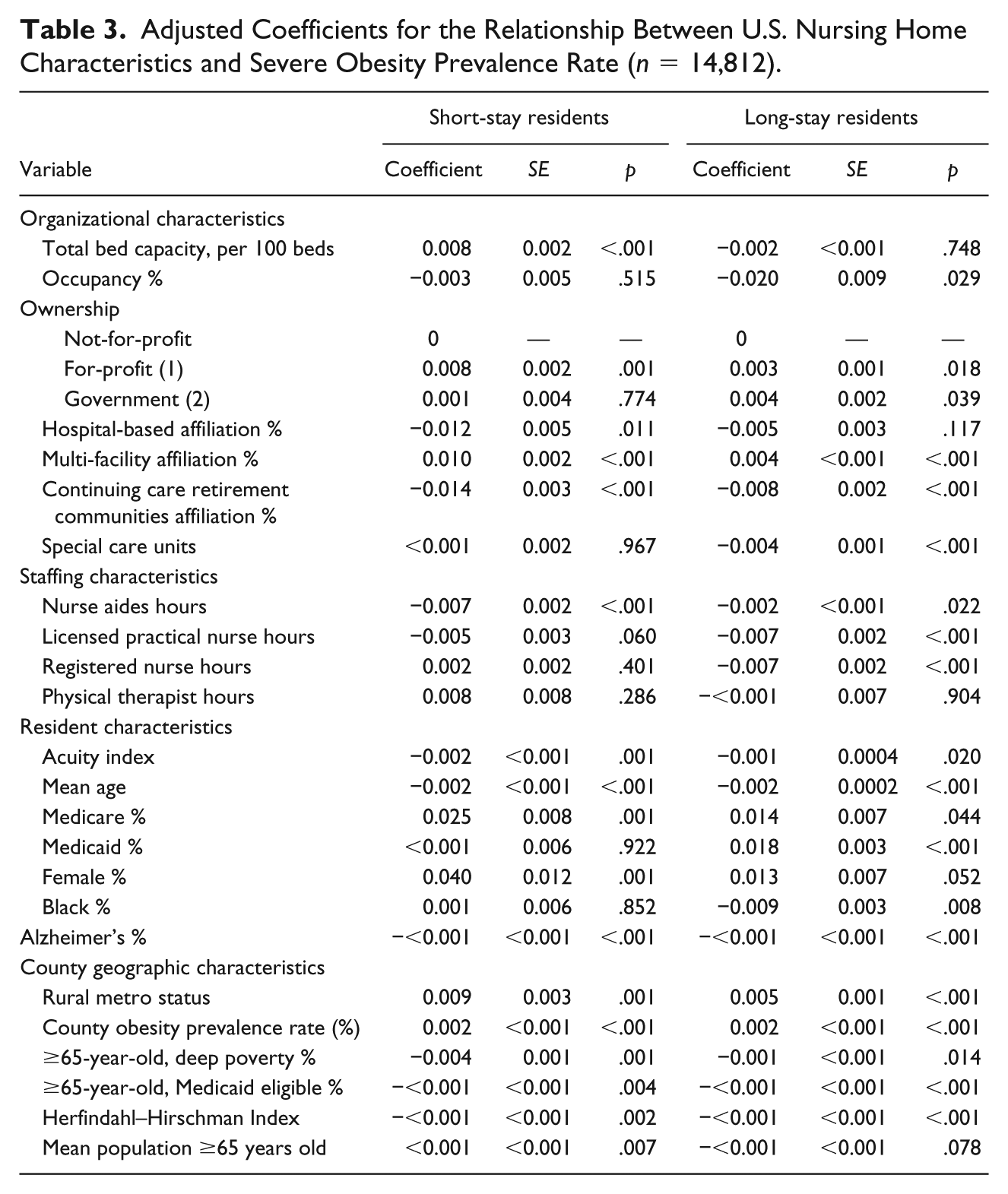
When the prevalence of severe obesity was used as the outcome, many of the effect sizes of these factors increased and some characteristics, which were not significantly associated with nursing home obesity prevalence rate, were associated with severe obesity prevalence rate (Table 3). Of note, for-profit ownership was also associated with higher nursing home severe obesity prevalence rate (p < .001 for short-stay residents and p = .018 for long-stay residents).
Adjusted Coefficients for the Relationship Between U.S. Nursing Home Characteristics and Severe Obesity Prevalence Rate (n = 14,812).
Discussion and Implications
Using national data on organizational, staffing, resident, and geographic factors, we examined the characteristics associated with higher nursing home obesity prevalence rate. In summary, higher obesity prevalence rate was strongly associated with increased occupancy, multi-facility affiliation, and bed capacity supports Hypotheses 1 and 3. However, higher obesity prevalence rates were associated with for-profit status, which did not support Hypothesis 2.
While we found some supporting evidence for the profit maximization relating to obesity care, it seems overly simplistic to view all residents with obesity as undesirable from the perspective of nursing home profit-maximization. Many residents with obesity may have a variety of other positive characteristics which may incline a nursing home to admit them. First, accepting any resident, except for one where care will result in a large negative profit margin, is often preferable to an empty bed (Span, 2018). Furthermore, our understanding of the profit calculations for these residents may be inaccurate in some circumstances, for instance, among short-stay residents and, more surprisingly, residents with severe obesity. Associations between obesity prevalence rate and lower occupancy were only found in long-stay resident (Hypothesis 1), and obesity prevalence rate was only increased among larger nursing homes in short-stay residents (Hypothesis 3). This suggests that residents with obesity may be attractive to nursing homes as short-stay residents (likely due to improved profit margins), but not as long-stay residents due to a combination of higher costs and lower reimbursement. While there was no association between for-profit status and nursing home obesity prevalence rate, there was a strong association between severe obesity prevalence rate and for-profit nursing homes among both short- and long-stay resident populations, opposite our proposed hypothesis (Hypothesis 2). For-profit nursing homes may have greater incentive to accept residents with severe obesity to increase occupancy or because these residents are more profitable than we hypothesize.
Other characteristics of residents with obesity that may increase the attractiveness to prospective nursing homes include lower acuity (and often, related younger age and lower levels of dementia) which may be associated with lower care costs. In addition, Hypothesis 3 assumes that efficiencies in care will be related to having more available resources or better processes, but costs of care can be cut in a variety of ways that may improve margins but decrease the quality of care. There is significant evidence that nursing homes with a high prevalence of obesity have lower quality and that nursing home residents with obesity have worse outcomes, such as pressure injuries and readmissions (Cai et al., 2013; Kosar, Thomas, Gozalo, Ogarek, & Mor, 2018; Zhang et al., 2016). Our conceptual model does not account for the real possibility that nursing homes may provide less care or lower quality care to cut costs and so improve profit margins for residents with obesity. Further research must examine the relationship between the cost of care and the quality of outcomes for residents with obesity.
This analysis does provide useful information to help understand what nursing home characteristics are associated with high nursing home obesity prevalence rate. First, nursing homes with a high obesity prevalence rate are more likely to care for younger and less disabled (including cognitive impairment such as Alzheimer’s disease) than nursing homes with a low nursing home obesity prevalence rate. This suggests that these nursing homes may be providing care to residents, including many residents with obesity, who may be transitioned to home and community-based services (HCBS). HCBS are an alternative to residential services such as nursing homes for people with disabilities, and are generally less expensive as well as most appropriate for lower acuity residents who are presently in nursing homes (Szanton, Leff, Wolff, Roberts, & Gitlin, 2016; Wysocki et al., 2015). HCBS certainly may need to be enhanced to meet the specific needs of people with obesity, especially as research has shown that people with obesity after hip fracture are less likely to return to the community compared with people of normal weight (Kosar, Thomas, Gozalo, Ogarek, & Mor, 2018). If HCBS address the needs of this population, it will reduce the number of people needing to move into nursing homes and improve the ability of residents with obesity to be transitioned back into the community after functional improvement.
Next, it is notable that nursing homes with a higher prevalence of residents with obesity and severe obesity often have lower staffing levels of nurse aides and licensed nurses. The literature often remarks on the need for extra staffing to care for people with obesity because care requires extra hands or more time to provide the same service as a normal weight resident. Most residents with obesity are, however, living in facilities with less available staffing than facilities with a lower prevalence of obesity. Higher staffing is commonly noted to be associated with improved outcomes, and this has been noted in care for residents with obesity as well (Cai et al., 2013). This paradox of low staffing levels for this population that needs higher staffing levels likely has to do with the lower general acuity in nursing homes with a high prevalence of obesity. Clearly, these acuity measures like RUG ADL scores do not describe the specific and complex needs of residents with obesity. There is a need for metrics that better describe the nature of the care provided for people with obesity. Metrics are needed that describe the real differences in ADL assistance between a resident weighing 100 pounds and 300 pounds. Such metrics may help provide evidence to decision makers for reformed payment models to account for the challenges related to the obesity epidemic in long-term care.
This study has clear limitations. The main outcome, nursing home obesity prevalence rate, may not specify the population of interest most effectively—the residents with obesity who have care needs that require the most resources and facilities. We did a subgroup analysis examining the prevalence of severe obesity in nursing homes, and our results were generally similar with some exceptions, noted above. Some organizational characteristics can change over time and confound hypothesized associations. For example, higher occupancy in nursing homes may be achieved in many ways: They may admit all types of residents or they may have an excess of applications and can be very selective while having high occupancy. Next, some of our predictor variables may incompletely specify the underlying organizational characteristics. For instance, a factor like for-profit status may not fully describe organizational values and business practices. But these factors are widely used in nursing home literature and represent clearly defined characteristics of these facilities. There are no variables existing that describe the availability of obesity-care equipment (such as Hoyer lifts), the presence of staff training related to obesity care, or special obesity-care units. Other variables were not available in the current data set such as occupational or speech therapist level which may be important factors. Finally, there may be unmeasured confounding by other medical conditions associated with obesity and nursing home profitability.
The strengths of this study are its recent time-frame, national scope, and clear accounting for important geographic and market variables. National data allow for a large sample and generalizability to national trends. This analysis adjusts for geographic differences related to obesity prevalence rate in the general population, but even controlling for the geographic confounding between obesity and facility characteristics, there were strong associations between many nursing home variables and higher nursing home obesity prevalence rate. Finally, it is a strength that this work is based on an established conceptual model that helped predict, in part, the findings of this study.
This study provides more evidence about how nursing homes interact with the resident population with obesity. The complex care needs of residents with obesity raises additional questions as to how nursing homes are adapting to this need and whether care is equitable and efficient. Residents with obesity are not equally distributed among all nursing homes. Instead, certain types of nursing homes (higher proportions of short-stay residents, lower levels of nurse aid staffing) are accepting residents with obesity at higher rates than other nursing homes. Further research will be needed to understand the effect of organizational factors and admission practices on the quality of care for residents with obesity. How does accepting a greater proportion of residents with obesity improve the care of these residents by allowing specialization or degrade their care by consolidating residents in lower quality nursing homes? How does good or bad obesity care affects the financial health of the facility? These difficult questions require a broader scope of research strategies—that is, beyond administrative data analyses—so qualitative studies of resident, staff, and administrator views will be important in understanding the underlying demands, opportunities, and pitfalls of nursing home care for residents with obesity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [K12HD063087].