
Abstract
Although several studies have examined individual-level correlates of cannabis use in later life, there is scant evidence identifying heterogeneity among older users. Using data from Colorado, this study examines variability in lifespan patterns of cannabis use among individuals aged 60 years and older. Sample respondents reported cannabis use in the past year and frequency of use in four periods of adulthood. Analyses used a multi-way contingency table to identify mutually exclusive subgroups of cannabis users based on lifetime reports of use and linear probability models to identify predictors of group identity. Three subgroups of older cannabis users were identified: new users, stop-out or intermittent users, and consistent users. The three groups varied on current use frequency and method of ingestion, as well as social and health characteristics. Screening for past history of cannabis use may help health care providers identify older adults who need health information and monitoring related to cannabis use.
Introduction
The older adult population in the United States is projected to expand dramatically in the upcoming decades. By 2030, all baby boomers will be older than age 65 and about one in every five residents will be retirement age (U.S. Census Bureau, 2019). In addition, the United States is also experiencing changes in the legalization, perceptions, and use of cannabis. As of June 2019, 34 states and the District of Columbia (DC) had approved comprehensive medical marijuana laws (MMLs) and 13 states and DC had laws legalizing recreational cannabis for adult use (Karmen Hanson, 2019). Concurrently, several studies have documented that cannabis use among late middle-aged and older adults has soared in recent years (Han et al., 2017; Salas-Wright et al., 2017). Data from the National Survey on Drug Use and Health demonstrates that over a 7-year period ending in 2013, the past-month use rates reported by persons over age 50 in the United States increased by 58%, while those over age 65 reported a 250% increase (Han et al., 2017).
Typically, older cannabis users are more likely to be male and less likely to be married or partnered (Choi et al., 2016; Han & Palamar, 2018; Salas-Wright et al., 2017). The race and ethnicity of cannabis users has differed in epidemiological studies (Choi, Marti, et al., 2017; Salas-Wright et al., 2017). Although some studies have shown that many older persons use cannabis for recreational purposes (Black & Joseph, 2014; Lum et al., 2019; Wu & Blazer, 2011), others have determined that older adult cannabis users are more likely to report its use for medical reasons (Choi, DiNitto, & Marti, 2017). In terms of outcomes, some studies have found higher rates of injury and emergency department use (Choi, Marti, et al., 2017), as well as a higher prevalence of alcohol use disorder, nicotine dependence, cocaine use, and prescription drug misuse among older users as compared to nonusers in the same age range (Han & Palamar, 2018). Alternatively, others have shown that a majority of older users report no adverse effects of cannabis use and, instead, perceive it to be helpful for managing a variety of symptoms and conditions, including anxiety, sleep, pain, and nausea (Lum et al., 2019; Reynolds et al., 2018). These findings suggest a potential for significant heterogeneity across older adults who use cannabis. However, very little research exists on describing the identity of users in late life and determining if they separate into distinct groups.
A key dimension in which older cannabis users might vary is their lifetime pattern of past use. There is some evidence that older adults who currently use cannabis tended to have also used when they were 21 years of age or younger (Han & Palamar, 2018). Using data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), Choi et al. (2016) examined patterns of cannabis use among adults over age 50 by comparing current users and ex-users by initiation age, duration of use, and amount of use during peak periods. The authors found that compared with current users, ex-users on average smoked cannabis less often, smoked fewer joints, and smoked for a shorter length of time during their peak cannabis use period. More than half of ex-users quit in their 20s, suggesting they were likely to have been experimental users in their youth, while almost a quarter quit after age 40, showing that they continued cannabis use in middle age and beyond. Using cross-sectional data, researchers have also observed significant differences in frequency and intensity of cannabis use and mode of ingestion across older, midlife, and younger users (Haug et al., 2017). Young users reported similar frequency of use as middle-aged and older adults but higher dosages and greater problems related to use. Older adults were more likely to prefer oral methods of ingestion as compared to younger and middle-aged adults. However, in light of limitations of cross-sectional data, it is uncertain if historical preferences at younger ages are associated with intensity of use and mode of ingestion later in life.
To our knowledge, no previous study has examined the extent to which older adults who currently use cannabis used it continuously or sporadically through life. Furthermore, we know very little about the characteristics of the growing number of older adults who initiate cannabis use for the first time in late life. It also remains unclear how lifetime patterns of cannabis use relate to current cannabis use characteristics, including frequency, mode, and purpose of cannabis use. Although longitudinal prospective studies across the lifespan of recent cohorts would be an ideal way to investigate changes in cannabis use patterns over adulthood, such studies do not exist. Furthermore, the rapidly changing legal and social contexts of cannabis would not yield comparable meaning to data points collected over the lifespans of the current cohort of older adults. Older adults living in a context of reduced social stigma that led voters to legalize cannabis use for both medical and recreational purposes have the greatest freedom to report their use, both current as well as that in previous periods.
Purpose of the Study
Using retrospective reports from a sample of older adults living in Colorado where cannabis may be accessed legally for medical or recreational purposes, this exploratory study assesses heterogeneity in older cannabis users by examining patterns of use throughout the adult lifespan. The aging of the American population increases the urgency of clinical consideration of the lifespan history of cannabis use. Providers are increasingly likely to encounter older cannabis users as more states legalize medical cannabis (Cerdá et al., 2012; Philpot et al., 2019) and support grows for the medical use of cannabis for symptom management (Briscoe & Casarett, 2018) despite limitations in the data on effectiveness (National Academies of Sciences, Engineering, and Medicine, 2017). Screening this population for past history of cannabis use may help clinicians identify older users who are at greater risk for adverse health outcomes and those who need health information and monitoring related to cannabis use.
Methods
Participants
A cross-sectional survey of older Coloradans conducted during June 2017 through November 2017 generated a purposive sample of 274 English-speaking adults aged 60 years and older. The sample was recruited from senior centers, a university research volunteer list, health clinics, and other locations where older adults typically obtain services and information as identified by local leaders of 13 of the state’s 16 Area Agencies on Aging (AAA). The use of the aging services network for recruitment established a basis for choosing to recruit persons aged 60 years and older, which is the age range for their services. Intentional efforts were made to survey both cannabis users and nonusers; thus, participants were also recruited from state-registered cannabis clubs, retail shops, and dispensaries. Detailed recruitment and sampling procedures and strategies are described elsewhere (Arora et al., 2020; Lum et al., 2019). The project was approved by the Institutional Review Boards at University of Colorado Colorado Springs and the University of Iowa, and all participants reviewed an informed-consent document before participating.
Only current cannabis users who provided retrospective reports of their frequency of use across different time periods were included in the present study. Of the 274 survey respondents, 198 individuals responded to the question of whether they used cannabis over the past year. Among these, 45% (N = 89) provided a positive report of past-year cannabis use, of whom 80 provided complete data (had no more than one missing observation across the four time periods) on cannabis use during adulthood. These 80 individuals comprise the sample for this study.
Measures
The survey consisted of 83 questions on a variety of topics, including attitudes, prevalence, predictors, patterns, and health outcomes associated with cannabis and its use. This present study only focuses on lifespan patterns of cannabis—analysis of other survey questions is covered elsewhere (Arora et al., 2019; Lum et al., 2019). Past-year use was assessed with one question, “In the past year, did you use marijuana?” with the following response options: “Medical purposes only,” “Recreational purposes only,” “Both medical and recreational purposes,” and “I have never used marijuana.”
Frequency of use across the lifespan was asked of participants who reported using cannabis in the past year. Participants reported frequency of use at five different time points over the life course: less than age 18, 18 to 30 years old, 31 to 49 years old, 50 to 64 years old, and age 65 and over. The upper age range of age 65 and older was selected to align with the age commonly identified with entrance into old age, as specified in Medicare policy and the original Social Security policy. Specifically, participants responded to a question, “How frequently did you use marijuana when you were . . .” with rows for the five age periods. Response options for each time period were “None,” “A few times a year,” “1–3 times a month,” “1–4 times per week,” and “5–7 times per week.” We combined the last two categories into one to reflect the highest frequency of cannabis consumption (“weekly or daily”). This article examines cannabis use over the adult lifespan, ignoring reports of use prior to age 18.
Statistical Analysis
Descriptive statistics are used to report sample characteristics. To understand how this subsample of users who reported on lifespan use may differ from the overall study sample, we compare summary results with that of the overall sample. We also examine the cross-sectional distribution of cannabis use frequencies across the four age categories (18–30 years old; 31–49 years old; 50–64 years old; and 65 years and older).
Next, we use retrospective reports of cannabis use frequency to examine lifespan patterns of use within individuals. For each time period, the frequency of use rating was simplified into a binary measure that assesses whether the respondent reported use during a particular time period. In this way, each individual’s lifespan record contained an indication of cannabis use/nonuse in four periods. Next, we use a four-way contingency table to produce cross-tabulations between reports of cannabis use at these four time periods. This contingency table provides us with a frequency of various combinations of cannabis use over the lifespan. Based on the frequency of occurrence of these lifespan use combinations, we identify most commonly occurring subgroups of older cannabis users. Cannabis use characteristics (past-year frequency of use, mode of ingestion, and purpose of use) are analyzed for each group.
Finally, we use linear probability models (LPMs) to examine associations between membership in each group and various individual characteristics. Covariates include sociodemographic and health characteristics, including age, gender, PROMIS (Patient-Reported Outcomes Measurement Information System) scores for mental and physical health (Cella et al., 2010), education, employment status, whether the respondent was currently married or partnered, and whether the respondent was currently providing informal care to an adult over age 60. LPM was chosen as the estimation strategy instead of a logistic regression because Long (1997) recommends a minimum of 100 cases for a maximum likelihood estimation such as a logistic regression. Furthermore, we use LPM because of its computational efficiency and easy interpretation (Wooldridge, 2001). Robust standard errors were used in all models to address heteroscedasticity inherent in LPM models. Statistical analysis was conducted using SAS version 9.4 and Stata version 15.
Results
Summary statistics for the sample of older cannabis users analyzed in this study as well as that of the overall sample are presented in Table 1. As compared to the full sample, cannabis users were slightly younger and more likely to have received college and graduate degrees. Users were more likely to be married/partnered (69% vs. 55% of the full sample), and a higher percentage of cannabis users were male as compared to the full sample (45% vs. 35%). Furthermore, relative to the full sample, a higher percentage of cannabis users identified themselves as caregivers.
Sample Characteristics.
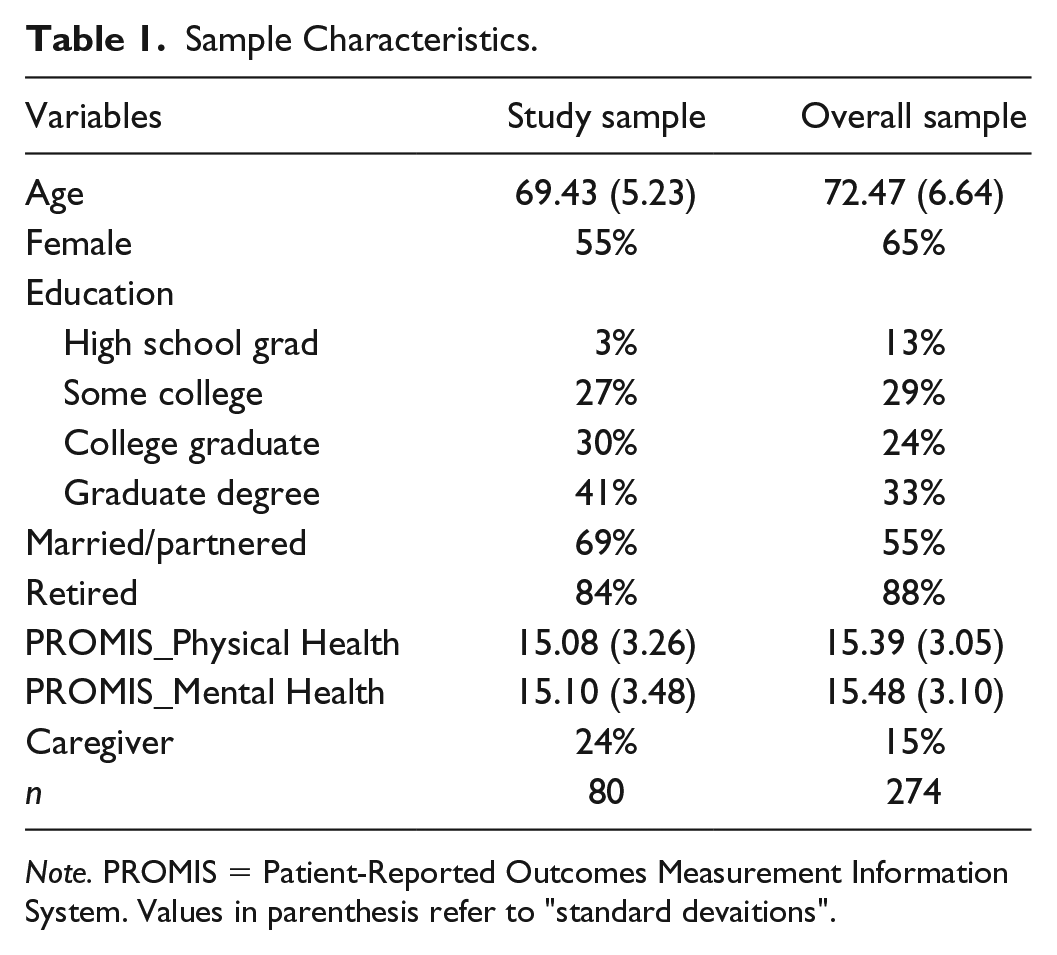
Note. PROMIS = Patient-Reported Outcomes Measurement Information System. Values in parenthesis refer to “standard devaitions”.
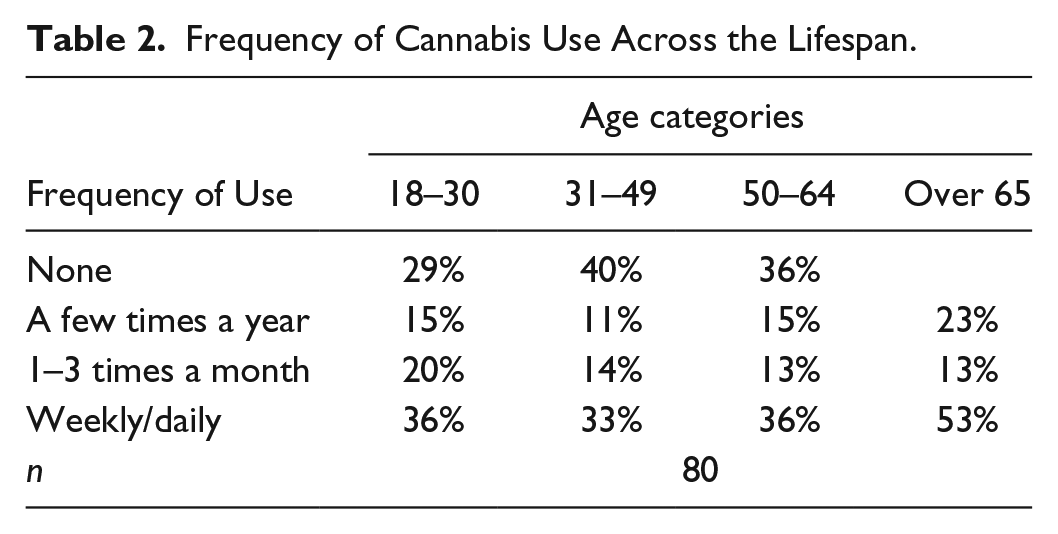
The cross-sectional frequency of use across the lifespan is presented in Table 2. About half of those aged 65 years or older reported consuming it at the highest frequency (weekly or daily) in the past year, while 23% reported using it a few times a year and 13% said they used it 1 to 3 times a month. This varied in comparison to other points in the lifespan where approximately 33% to 36% reported weekly or daily use at each previous period. The peak period of nonuse was during early midlife (ages 31–49) when 40% of the sample recalled not using and late midlife (ages 50–64) when 36% were not using.
Frequency of Cannabis Use Across the Lifespan.
Analysis of the multi-way contingency table produced three mutually exclusive groups with each group containing a homogeneous set of cannabis users. Individuals in these three groups combined comprised 90% (n = 72) of the cumulative percentage of the entire study sample. These groups differed from each other based upon pattern of use over the lifespan. Specifically, the three groups included (a) New Users (those who reported using cannabis for the first time after age 50), (b) Stop-Out Users (intermittent users who reported use in early and late adulthood but no use during midlife, that is, ages 31–49 or ages 31–64), and (c) Consistent Users in adulthood (i.e., those who reported some frequency of cannabis use in all periods of adult life).
The groups differed in sample size and in cannabis use characteristics, as evident in Table 3. Almost all New Users reported first time cannabis use at or after age 65 with the remainder beginning between ages 60 and 64. This group represented 26% (N = 19) of those placed in the three subgroups. About half of Stop-Out Users reported use in early adulthood (ages 18–30) and late life (ages 65 and older), but no use in midlife (ages 31–64). The other half reported use in early adulthood (ages 18–30), late midlife (ages 50–64), and older ages (ages 65 and above), but no use in early midlife (ages 31–49). Stop-Out Users represented 21% (N = 15) of those placed in the three subgroups. The Consistent Users group was the largest of the three, comprising 53% of those placed in the three subgroups, with 38 members who reported lifelong use in adulthood.
Three Groups of Cannabis Users Based on Pattern of Use.

In terms of past-year frequency, about 60% of New Users used cannabis only a few times a year (Column 1, Table 3). In contrast, a majority of Stop-Out and Consistent Users reported using cannabis at least weekly or daily (Columns 2 and 3, Table 3). Over 30% of Consistent Users used cannabis weekly or daily since age 18. In fact, 63% of Consistent Users reported using the substance at least monthly in all time periods of adulthood. The three groups also varied in terms of past-year mode of cannabis ingestion and purpose of use. New Users were more likely to have used alternative/nonsmoking methods (vaporizer, capsules, edibles, cream-ointment, liquid tincture, dabbing, and so on) to ingest cannabis, whereas Consistent Users were more likely to have used smoking or inhalation methods to ingest cannabis. Approximately, half of the Stop-Out Users reported smoking cannabis. The distinction between groups was also evident in their purposes of use. New Users almost exclusively used cannabis in the past year for medical purposes, whereas Stop-Out Users and Consistent Users were more likely to have used it for both medical and recreational purposes.
Table 4 presents results from multivariate analyses exploring associations between individual characteristics and group membership. A separate LPM was estimated for each group, with the dependent variable coded as “1” if an individual belonged to that group and “0” otherwise. The results of the multiple regression analysis in column 1 indicate that the 10 predictors explained 31% of the variance in the probability of belonging to the New User group. Specifically, the probability of belonging to this group was greater among women (as compared to men) (β = .25, p < .01). Better physical health was associated with a lower probability of being a New User (β = –.05, p < .05).
Linear Probability Models Predicting Group Membership.
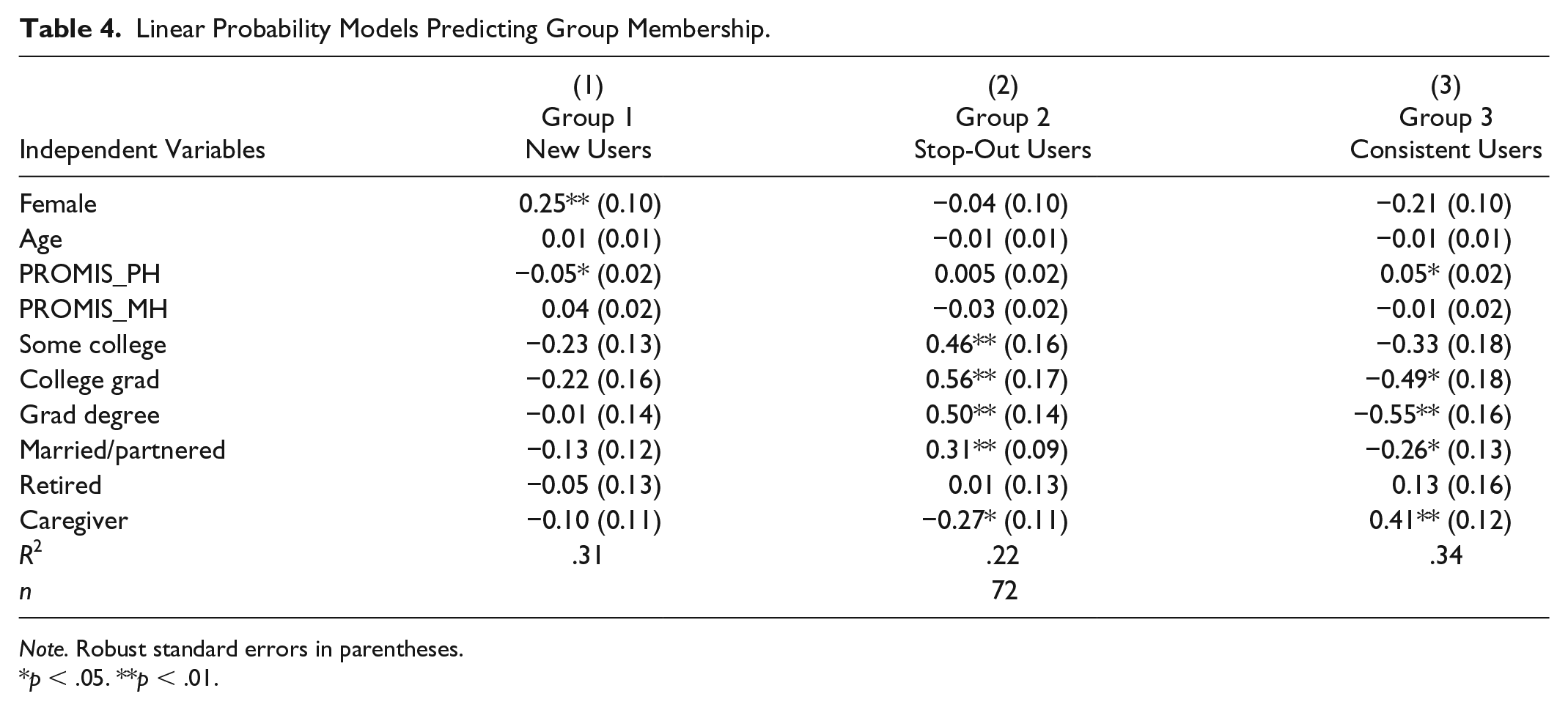
Note. Robust standard errors in parentheses.
p < .05. **p < .01.
The results of the multiple regression analysis in column 2 indicate that the 10 predictors explained 22% of the variance in the probability of belonging to the Stop-Out User group. Greater educational attainment was positively associated with belonging to this group. Specifically, relative to being a high school graduate, having completed some college (β = 0.46, p<.01), having a college degree (β = .56, p < .01) or a graduate degree (β = .50, p < .01) was positively associated with being Stop-Out User. Being married/partnered also positively predicted the probability of being a Stop-Out User (β = .31, p < .01). Conversely, being a caregiver was associated with a reduced probability of being a Stop-Out User (β = –.27, p < .05).
The results of the multiple regression analysis in column 3 indicate that the 10 predictors explained 34% of the variance in the probability of belonging to the Consistent User group. Better physical health was positively associated with being a Consistent User (β = .05, p < .05). Relative to being a high school graduate, having a college degree (β = –.49, p < .05) or a graduate degree (β = –.55, p < .01) was inversely associated with being a Consistent User. Being married/partnered also lowered the probability of belonging to this group (β = –.26, p < .05). Interestingly, being a caregiver was associated with an increased probability of being a lifelong cannabis user (β = .41, p < .01).
Discussion
Previous research has shown that cannabis users in late life differ substantially from nonusers in the same age range. This study adds to the empirical base by demonstrating the presence of considerable heterogeneity across older cannabis users. We find that the current cohort of older adult cannabis users have highly varied, lifespan cannabis experience and should not be viewed as a homogeneous group. Three pathways to use across the lifespan were identified: new users in late life, stop-out or intermittent users (whose later life use represents a return to use from earlier periods), and consistent/lifelong users. These pathways were heterogeneous in terms of participants’ frequency of use, mode of ingestion, purpose of use, health status, and other sociodemographic characteristics.
New Users were predominantly women (15 of the 19 New Users in our sample identified themselves as women) who used almost exclusively for medical reasons. This group was more likely to have poor health, and use cannabis at low frequency with nonsmoking modes. This finding on gender contrasts with a recent study that found that women over age 35 were less likely than men to be new users (Agrawal & Lynskey, 2009). However, the large age range for defining older adult in that study (age 35 and older) may mask any distinct pattern in older women using for medical purposes after the onset of chronic disease. From a clinical perspective, new users represent a key population of interest primarily because they are employing means of ingestion that are particularly challenging to dose (e.g., salve, oils, and edibles) safely. Edibles also are challenging for users to monitor, especially with respect to new users, due to variation in the speed of effect that may lead users to ingest more to achieve the desired effect faster, risking an overdose (Murphy et al., 2015). Furthermore, recognizing the motives and patterns of older persons who only started using cannabis for a medical purpose may help public officials and program administrators better target cannabis policy.
Stop-Out Users were more likely to have higher educational attainment, be married, and less likely to be caregivers. This group ceased using cannabis for several years in midlife, perhaps because they were investing in education or occupational success or marriages that position them now for more discretionary time in which to use cannabis both recreationally and medically. Because the concentration of THC (the psychoactive component of cannabis) has increased considerably over the past several decades (ElSohly et al., 2016), this group may be more familiar with lower potency cannabis than what is available today. Psychological and physical changes associated with aging coupled with stronger potency cannabis could pose a higher risk in this population, and thus, Stop-Out Users may benefit from more education and counseling on cannabis dosage and administration.
Consistent Users were less likely to have college or graduate degrees or be married, a profile generally congruent with national data on older users (Choi et al., 2016; Han & Palamar, 2018; Salas-Wright et al., 2017). This group typically consumed cannabis at a high frequency, employed smoking methods to ingest cannabis—likely reflecting historical patterns of use—and reported using cannabis for both medical and recreational purposes. Interestingly, our results indicated a positive association between physical health and lifelong cannabis use among this sample of older cannabis users from Colorado. The PROMIS Physical Health measure used in this analysis captures four health indicators: self-perceived physical health status, physical functioning/mobility, fatigue, and pain interference. In comparing means of each of the four individual indicators, we found that Consistent Users had lower scores on fatigue relative to all other users in the sample (t = −2.06, p < .05). The other three indicators of physical health were not detectably different among Consistent and Non-Consistent users. It is possible that lifespan cannabis use may be positively associated with some measures of physical health but not with others. This explanation notwithstanding, a positive association between physical health and cannabis use differs from findings in some previous studies (Choi, Marti, DiNitto, & Choi, 2017) and should be interpreted with caution. It is also possible that it is only specific to the Coloradan context or a result of sample bias due to the small sample. Our results also indicated that lifelong cannabis use was negatively associated with the PROMIS Mental Health measure; however, this result was not statistically significant in the LPM regression.
Consistent Users were also more likely to be informal caregivers—a result previously unestablished in the literature. It is possible that this finding reflects self-selection into the role of informal caregiving. Those with lower educational attainment are also likely to have a lower opportunity cost of time and thus, may be more available to provide care. Alternatively, those with established coping strategies (such as through lifelong cannabis use, for instance) may be more likely to take on the responsibilities of informal caregiving, a role that can be associated with substantial emotional and physical tolls (Schulz & Beach, 1999). This association between cannabis use and informal caregiving can benefit from additional study in the future, especially given that this study obtained no specific information about care recipients’ identities or needs. Overall, given their relative size and potential risk of adverse health outcomes, lifelong users are an important group of older users for clinicians to screen.
Our study also sheds light on reasons for increasing cannabis use among older adults. Given the strong association with gender and nonsmoking modes of use, it is possible that new cannabis use is on the rise because it is viewed as an alternative therapy by older women who tend to embrace alternative therapies at a higher rate than men (Rhee & Harris, 2017). This likely supplements other previously illuminated reasons such as age-related changes (onset of chronic disease and freedom from parenting/employment roles) or period effects (policy changes relating to cannabis legalization as well as greater availability and accessibility of nonsmoking products) that may have also simultaneously encouraged new use of cannabis in late life (Kaskie et al., 2017).
Conclusion
The findings from this study suggest the presence of distinct groups of older adult cannabis users. Older adult patterns of cannabis use are sufficiently variable in frequency, purpose, and history that health providers need to assess and screen older patients to identify new and resumed use patterns. With medical purposes a priority for new users, and a shared purpose with recreational use for resumed and lifelong users, providers can anticipate questions about dosages, strains of plant, forms of ingestion, and risk factors. This is especially relevant in light of recent findings that older consumers want information about medical cannabis use to come from the health providers with whom they have an ongoing relationship (Bobitt et al., 2019). However, providers acknowledge significant knowledge gaps and report continued need for training on the topic (Carlini et al., 2017; Philpot et al., 2019).
Limitations
Although deliberate recruitment efforts yielded a demographically diverse sample, the effects of selective participation that draws willing and interested participants whose biases are unknown cannot be addressed without systematic, representative sampling. The small size of this sample adds further cause for caution in our ability to generalize these results. Sample size considerations also led to the use of LPM models instead of logistic regressions. However, as is well known, a LPM model may generate predicted probabilities beyond the 0–1 range, making out of sample predictions problematic.
The use of self-report survey data that relies on recalled rates of use during previous periods of adulthood may be systematically biased by memory inaccuracy although the nature and intensity of the bias is unknown until characteristics of the measures and the sample are known (Althubaiti, 2016). The sample was drawn from Colorado whose population was among the earliest in the United States to legalize medical and recreational cannabis use, a factor known to be associated with more positive attitudes toward cannabis (Schuermeyer et al., 2014), which may have influenced participants’ willingness to report previous use in ways that would not generalize to other locations.
Recommendations for Future Research
Building on these initial data, research on cannabis use in late life needs to investigate pathways to use across the lifespan, determine the population prevalence of these pathways, and identify variations in use intensity over time as well as predictors and outcomes of each pathway. Existing longitudinal studies may contain data on use at multiple time periods, but their value is limited because the rapidly changing social norms and legal contexts of cannabis use will confound any effort to map a lifespan developmental framework for past and current cohorts of older adults. Prospective studies of successive cohorts need to be launched in regions where cannabis is legal for both medical and recreational use, with careful attention to disentangling lifespan developmental processes from cohort and period effects in explaining cannabis use patterns across the lifespan. Short-term longitudinal studies of multiple cohorts may be helpful to model use patterns across adulthood until prospective studies of young adults are completed over time.
Footnotes
Acknowledgements
The authors acknowledge Divya Bhagianadh for assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Colorado Department of Public Health and Environment.
Institutional Review Board Approval
The study was approved by the University of Colorado Colorado Springs (UCCS) Institutional Review Board (IRB# 17-088) as well as University of Iowa Institutional Review Board (IRB# 201601761 IRB-02).