
Abstract
Inconsistent outcomes of oral hygiene interventions require testable theories combining cognitive and behavioral domains to guide intervention and improve results. This article evaluates the integrated model as a cognitive-behavioral approach to improve oral health clinical outcomes in ethnically diverse low-income older adults. Baseline data from a clinical trial utilizing the integrative model (IM) model evaluated predictors of gingival index (GI) and plaque score (PS). Individual logistic regression was performed for all predictors in relation to GI and PS. Multiple logistic regression was performed with significant predictors of GI and PS only. Greater locus of control and more brushing predicted lower GI; greater locus of control predicted lower PS. Both cognitive and behavioral domains impact GI, requiring more prolonged effort for improvement while locus of control, a cognitive variable, predicts PS, immediately improved by daily brushing/flossing. A streamlined IM including locus of control and tooth brushing should improve oral hygiene of low-income older adults.
Introduction
The prevalence of oral health diseases including decay, periodontal disease, and edentulous, and its consequences for overall health and quality of life of older adults is well established (Dietrich et al., 2013; Scannapieco & Cantos, 2016; Wilder & Bray, 2016). Oral health is reciprocally related to systemic health (Kane, 2017), and physiological declines associated with aging (Zhang et al., 2018), including cognitive function, dementia, xerostomia, cancer treatment, and diabetes, have all been associated with poor oral health (Eke et al., 2016; Kang et al., 2020; Luo et al., 2015; Petersen & Ogawa, 2012). Significant disparities exist with respect to the burden of oral disease, oral health care, and oral health-related quality of life by race/ethnicity; social class; and medical, functional, and psychological comorbidities (Huang & Park, 2015; Hybels et al., 2016; Lamster & Northridge, 2008; Shelley et al., 2011). Improving oral health in vulnerable older adults should have a significant impact on oral health related quality of life and severity of chronic diseases.
Although structural factors such as financial barriers to treatment and limited-quality dental care are correlates of oral health disparities (Vujicic et al., 2016), individual-level factors such as limited oral health literacy, misinformation, inadequate oral hygiene skills, concerns about good oral hygiene, actual brushing and flossing practices, and diet also act as barriers to good oral hygiene (Anagnostopoulos et al., 2011; Ghaffari, Rakhshanderou, Ramezankhani, Buunk-Werkhoven, et al., 2018; Ghaffari, Rakhshanderou, Ramezankhani, Noroozi, & Armoon, 2018; Listl, 2018).
Behavioral interventions that focus on brushing and flossing instruction result in some improvements in oral hygiene (Sakashita et al., 2017). Earlier systematic reviews of behavioral intervention effectiveness, primarily tooth brushing in reducing plaque and gingivitis, demonstrated some reductions in plaque and improved gingival health (Deacon et al., 2010; van der Weijden & Hioe, 2005). An oral hygiene behavioral instructional program for older community dwelling adults with xerostomia improved oral health outcomes significantly (Ohara et al., 2015) and another reduced plaque significantly though not completely (Nihtilä et al., 2017). These studies show that significant reductions in plaque and gingivitis can be achieved with manual tooth brushing and careful instruction.
In spite of these achievements, most behavioral interventions have small or short-term effects on clinical outcomes, suggesting that other factors come into play in oral hygiene improvement (Komulainen et al., 2015). Jönsson and colleagues’ (2010) randomized controlled trial evaluated an individually tailored intervention plus motivational interviewing in participants with periodontitis (n = 113) with significant and sustainable differences in the treatment versus the control group over two follow-ups 3 and 12 months post baseline. A recent review concludes that goal setting, self-monitoring, and planning can be effective in improving oral hygiene for patients with periodontal disease along with knowledge of the importance of hygiene for health (Newton & Asimakopoulou, 2015). Carra et al. (2020) reinforce this notion but suggest that as yet there is no scientific evidence to suggest that cognitive variables have any consistent impact on clinical outcomes. To better understand the links among behavioral and cognitive interventions and clinical outcomes requires rigorous research designs as well as better links between theory and mechanisms of intervention (Werner et al., 2016), a conclusion supported by others (Bartholemew & Mullins, 2011; Newton & Asimakopoulou, 2015; Wilder & Bray, 2016).
Fischbein’s integrative model (IM) of Behavioral Prediction integrates prior reason-based cognitive intervention models (Ajzen, 2002; Ajzen & Fishbein, 1980; Fishbein, 2008; Fishbein & Yzer, 2003; McCaul et al., 1988). It includes knowledge (Firmino et al., 2018), beliefs, self-efficacy (Ohara et al., 2017), and intentionality/planning/goal-setting (Lee, 2018; Newton & Asimakopoulou, 2015), variables that have been used to explain oral hygiene behaviors (McCaul et al., 1988; Tedesco, 1991; Tedesco et al., 1992). These factors, when built into interventions to improve self-care regimens, are shown to have short-term positive effects on cognitive domains and brushing/flossing and longer term improvements in clinical outcomes such as tooth decay, calculus, plaque, and bleeding (Ghaffari, Rakhshanderou, Ramezankhani, Buunk-Werkhoven, et al., 2018). In addition, the IM adapted for oral hygiene education includes oral health locus of control (Messadi et al., 2018), oral health social norms (Atchison & Dolan, 1990; Brein et al., 2016), as well as proper brushing, flossing, and cleaning dentures with a trusted role model (Karami Joyani et al., 2018). The IM thus provides an integrated cognitive and behavioral theoretical framework for implementing and evaluating oral hygiene interventions with older adults that also includes important background characteristics known to be associated with aging and oral health including physical functioning (Zhang et al., 2018), age, gender, race/ethnicity education level, depression, and perceived oral health status. This article utilizes the baseline data collected from a community-based clinical trial with older adults in income-subsidized senior housing to evaluate the IM adapted for oral health, examining whether and in what combinations IM constructs predict clinical outcomes (gingival status, plaque).
Method
Recruitment and Enrollment
Three hundred and thirty one participants from six low-income senior housing buildings in Connecticut enrolled in a group randomized trial between 2015 and 2017 (see Supplemental Figure 1). Qualified apartment renters were 18 years and over, and either aged 62+ years or people with disabilities who met income qualifications for their buildings. Residents were either English- or Spanish-speaking or both. Eligibility criteria were 18+ years, two+ teeth, no conservator; able to comprehend consent form. Exclusion criteria were temporary or short-term building resident; under conservatorship; cognitively unable to give informed consent or respond to five questions about the study; edentulous (none or one tooth); history of infective endocarditis, prosthetic cardiac valve replacement in past 6 months, insertion of an arterial stent or myocardial infarction in past 6 weeks; on dialysis. Eligible volunteers in each building group signed consent forms, or if unable to sign, approved orally and signed with the letter X. Oral approvals were co-signed by the consenter and an independent witness using an institutional review board (IRB) approved process. Once consented, they were recruited either to a face-to face 1-hr oral health counseling session (AMI) tailored to the mediating domains in the adapted IM (see Figure 1) or an Oral Health Campaign (three oral health fairs) in which dental hygienists presented information in English and Spanish on oral health and the benefits of hygiene improvement and resident peer educators engaged attendees in discussions and interactive learning experiences based on messages derived from the study’s theoretical model (IM).
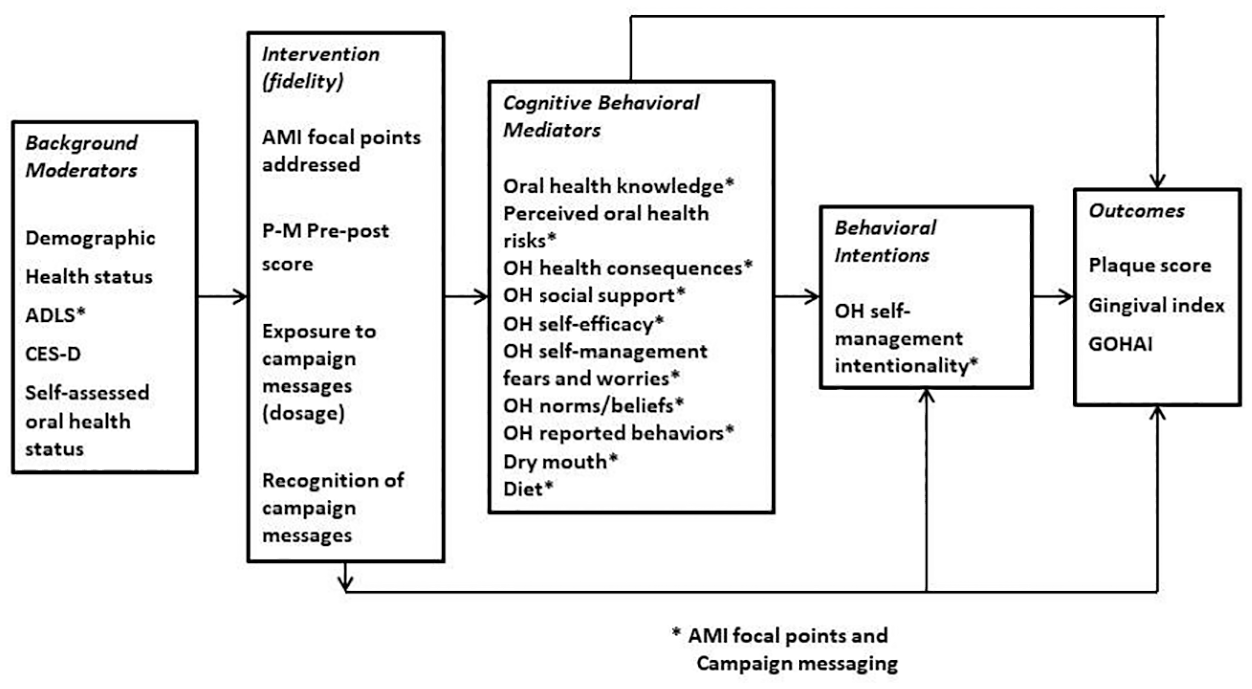
Integrated model of behavioral change.
The studies were approved annually by the study’s university partner’s IRB and deferred to by other partners. The IRB application final approval number is 14-1990-6.1, IRB Panel 1. In addition, the clinical trial protocol and IRB application were reviewed and approved annually by the National Institute for Dental and Craniofacial Research (NIDCR).
Survey Data Collection Process
A survey administered by English or Spanish speaking interviewers assessed demographic characteristics, perceived health and oral status and diagnosed health problems, health insurance, dental care history, and cognitive-emotional and preventive behavioral domains in the adapted IM. Two bilingual trained and calibrated dental hygienists conducted clinical assessments with enrolled participants to measure gingival status and plaque. Data were collecting digitally, using QDS software and an Access database developed for the study. The principal investigators (PIs) identified clinically relevant cutoff points for each of the theoretical domains measured, based on the IM model, below which participants were determined to need individually tailored AMI intervention (Reisine et al., 2020; Schensul, Reisine, et al., 2019).
Measures
Moderators included sex, age, income, education, and self-assessed oral health status rated on a 4-point Likert-type scale as poor (1), fair (2), good (3), or excellent (4) (Locker et al., 2000; Locker & Slade, 1994). Self-assessed oral health status was treated as both a continuous and bivariate variable, dichotomized as poor/fair versus good/excellent.
Cognitive mediators to be targeted by the intervention included Oral Hygiene Self-Management Worries Scale (OHWSMS) consisting of 19 statements about specific worries management of oral hygiene and consequences of poor management, derived from formative work with the study population and validated (Schensul, Salvi, et al., 2020) with responses rated 1 most to 4 least worried (Cronbach’s α = .93); intentionality, a six-question scale with responses rated as 0 (no intention) to 2 (high intention) (α = .72); perceived oral health risks (chances of getting specific health problems because of oral health mismanagement), five questions with responses rated 1 to 4 with 4 as least chances (α = .76); fear of oral diseases, four items rated 1 to 4, with 4 as no fear (α = .82); oral health self-efficacy (five items, α = .603); locus of control (seven items, α = .72) with responses as 4-point Likert-type scales ranging from 1 to 4 with 4 as high in both scales, adapted from Sherer et al. (1982); and importance of oral health behavior, nine items from 1 (not important) to 5 (important); alpha = .672. (See Schensul, Reisine, et al., 2019, for more detail on cognitive mediators.)
Behavioral mediators included sugar intake, five questions asking about frequency of consumption of sugar and starch (0 = never to 4 = more than 5 times a day); brushing often (1 = under twice a day, 2 = twice and over); and flossing often (less than once a day vs. once or more a day).
Outcomes included the gingival index (GI) and plaque score (PS) assessed by two trained dental hygienists calibrated each year based on comparison with an experienced dental examiner. The GI (Löe & Silness, 1963) assessed the status of gingiva associated with six surfaces of each tooth, three buccal and three lingual by scoring for gingival inflammation scored 0 = no visual signs of inflammation, 1 = slight change in color and texture of the gingiva but no bleeding, 2 = visual sign of inflammation and bleeding upon swiping, and 3 = overt inflammation and spontaneous bleeding. The index was calculated by summing each surface GI and divided by the total number of surfaces (mean value). Individual scores were summed to obtain a mean. The PS is a plaque scoring scheme (O’Leary et al., 1972), consisting of dichotomous presence or absence scores for bacterial plaque on each of six tooth surfaces using erythrosine disclosing solution. The number of surfaces stained red is calculated over the total number of surfaces, and PS is expressed as a percentage of surfaces with plaque or a ratio. At baseline T0, Kappa ranged from 0.46 to 0.78 for PSs and 0.45 to 0.54 for the GI. With continued training prior to TI, Kappa improved to 0.77 to 0.94 for PSs and 0.72 to 1.00 for the GI. Measures are further defined elsewhere (Schensul, Reisine, et al., 2019).
Cutoff score rankings
To tailor the face-to-face intervention, a cutoff score on each of the IM cognitive domains in the survey was established based on clinical judgment, below which the participant was deemed to require attention (Schensul, Reisine, et al., 2019). Domains were ranked by the frequency with which participants required intervention analytic procedures (see Table 1).
Percentages of Main IM Cognitive and Behavioral Domains Below Intervention Cutoff Point.
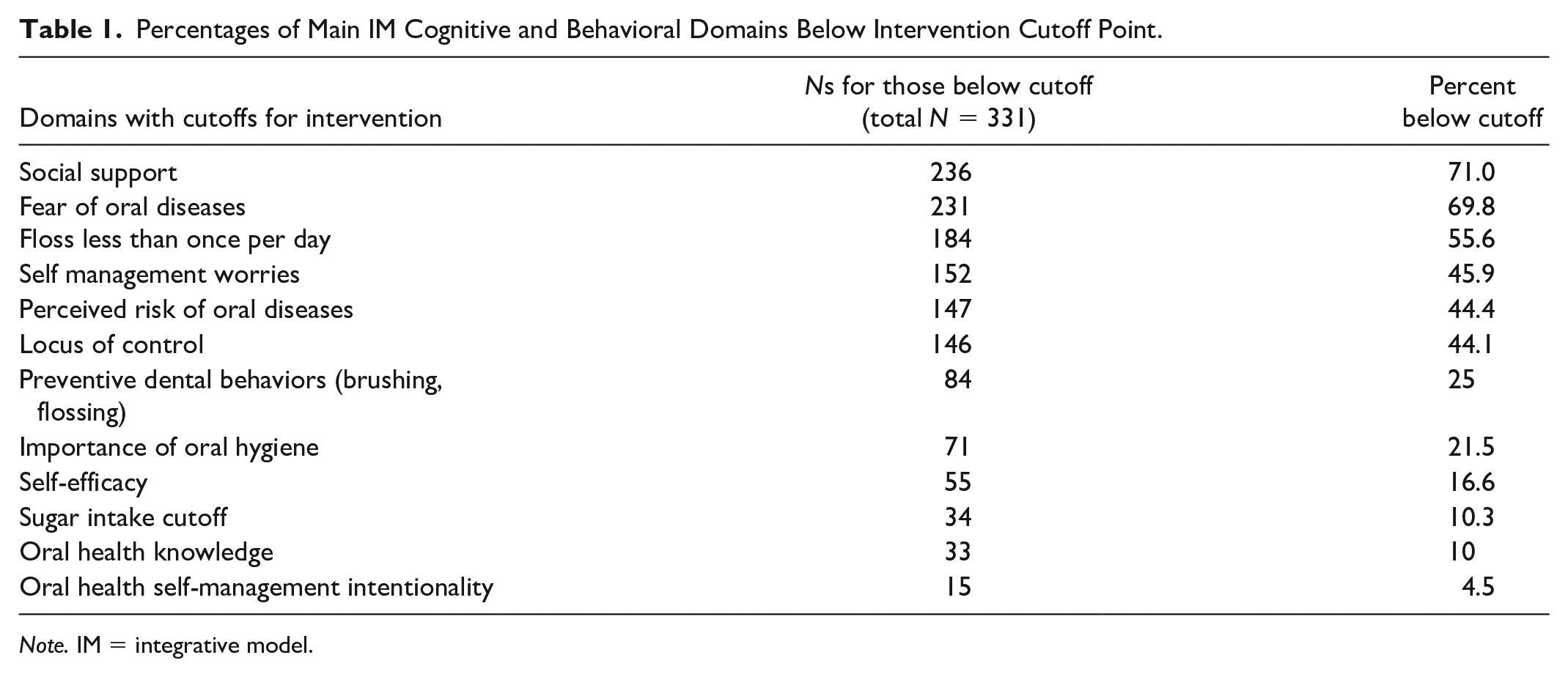
Note. IM = integrative model.
Scale scores were used as continuous variables unless otherwise indicated. Clinical outcomes were treated as categorical variables dichotomized at the median in individual and multiple logistic regressions to maintain consistency with the analysis of moderators and outcomes. GI and PS scores were fit to standard logistic and linear regression models for individual mediators and multiple logistic and linear regression models for all mediators found significant in individual associations. MPlus8 (Muthén & Muthén, 2017) was used to generate structural equation models for pathways connecting significant moderators, mediators, and each of the study outcomes.
Results
Characteristics of participants in relation to outcomes are shown in Table 2.
Participant Characteristics and M (SD) Scores on the Gingival Index and Plaque Scores.
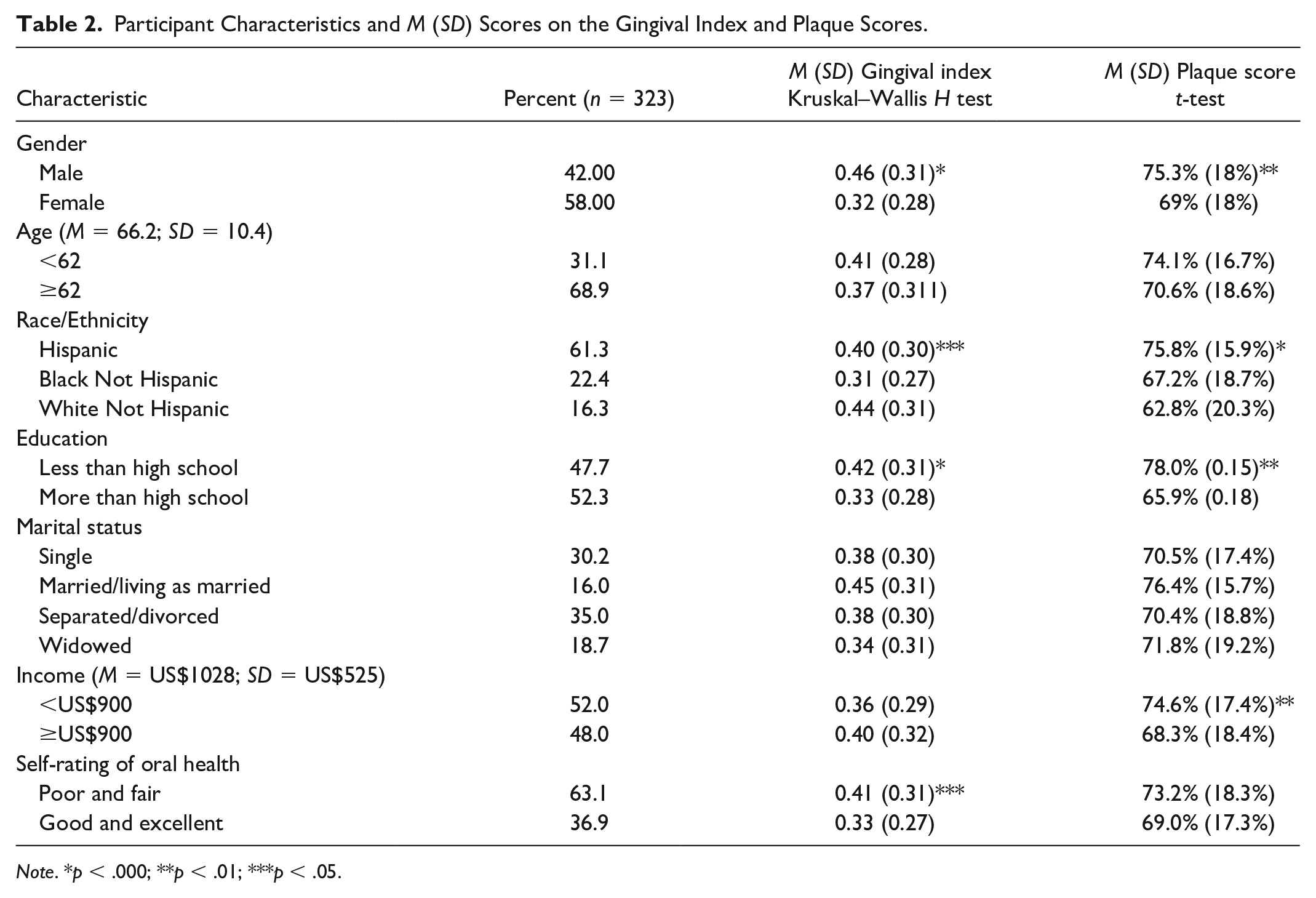
Note. *p < .000; **p < .01; ***p < .05.
Cutoff Points at Baseline
Domain for which 40% or more of participants needed intervention included four cognitive mediators—locus of control (44.1%), worries about self-management of oral hygiene (45.9%), perceived risk of oral health problems (44.4%), and fear of oral disease (69.8%). The list also included flossing less than once a day (55.6%). Other domains appeared less frequently (see Table 1).
Regression Analyses
Tables 3 and 4 show the results of individual logistic regression analyses for mediators. For GI, the significant cognitive predictors were intentionality and locus of control. Greater intentionality and higher locus of control were associated with lower GI scores. Significant behavioral predictors were brushing and flossing frequency—those who brushed and flossed more frequently had lower GI scores. Lower fears and worries about self-management and higher locus of control predicted lower PS scores. No behavioral predictors were significant (see Tables 3 and 4).
Predictors of GI: Individual Logistic Regressions Dichotomized at the Median Greater Than .34.
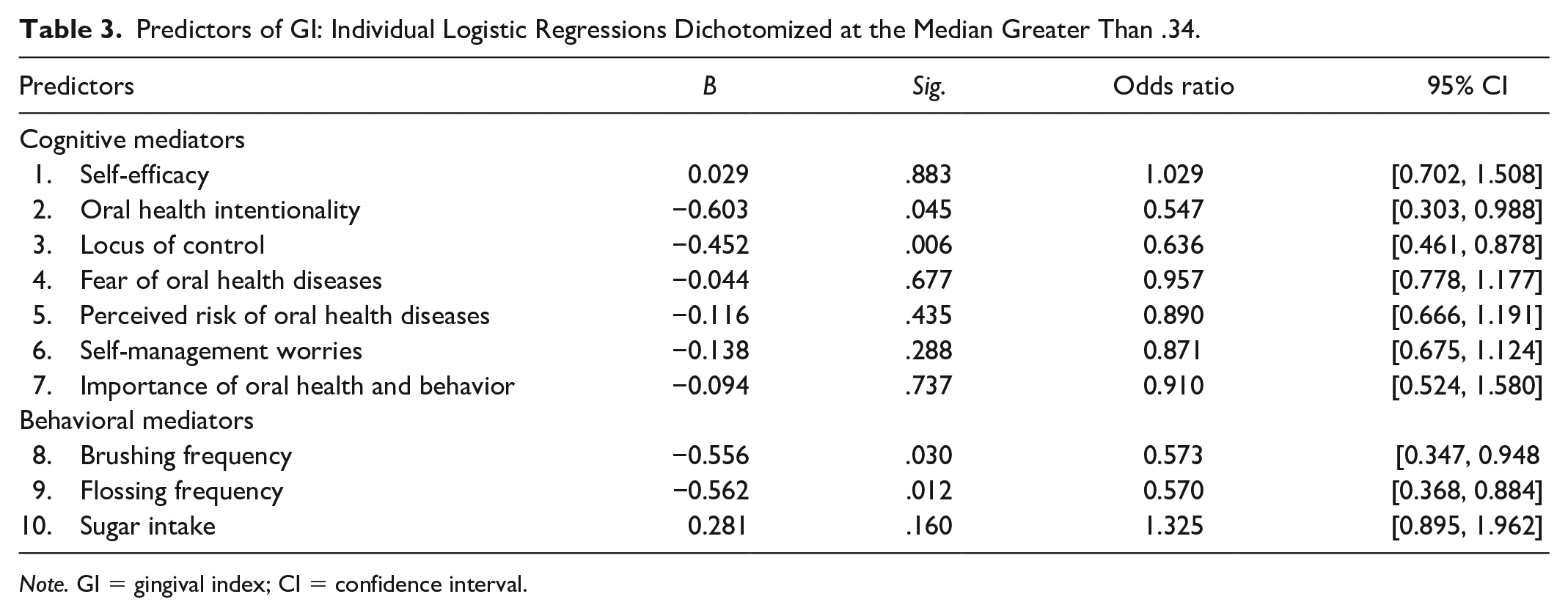
Note. GI = gingival index; CI = confidence interval.
Predictors of PS: Individual Logistic Regressions Divided at the Median (74%).
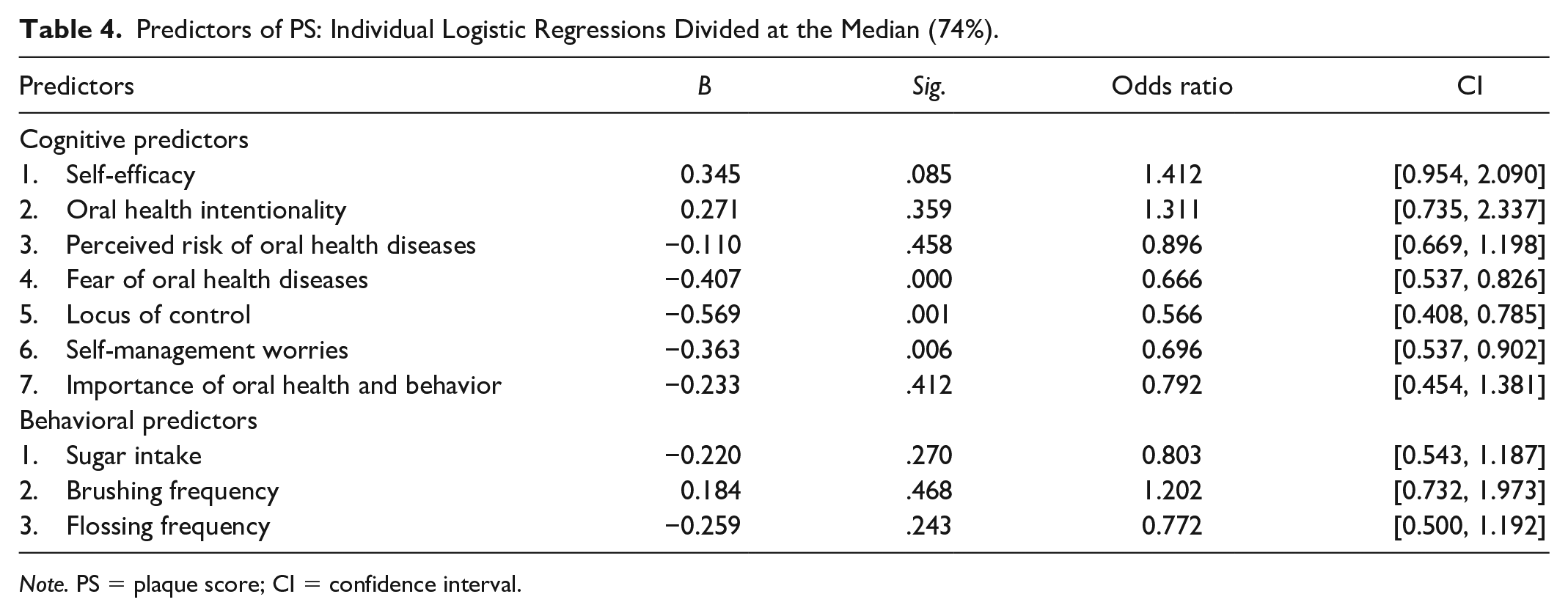
Note. PS = plaque score; CI = confidence interval.
Mediators found significant in the individual logistic regression analyses for GI and PS were utilized in the multiple logistic regression analyses for each clinical outcome. Multiple regression analyses were conducted for both GI and PS with these specific cognitive and behavioral variables, controlling for selected moderators found to be significant predictors of GI and PS outcomes (Reisine et al., 2020). Controlling for education, income, and perceived oral health status, higher locus of control (odds ratio [OR] = 1.408; confidence interval [CI] = [0.992, 1.998], p = .055) and more brushing (OR = 1.840, CI = [1.039, 3.258], p = .036) predicted lower GI score. Controlling for education, gender, and income, high locus of control (OR = 1.471, CI = [1.027, 2.107], p = .035) predicted lower PS; no behavioral mediators were significant (see Table 5).
Logistic Regression With Dependent Variables Gingival Index, Dichotomized at the Median (0.34) and Plaque Score, Dichotomized at the Median (74%).
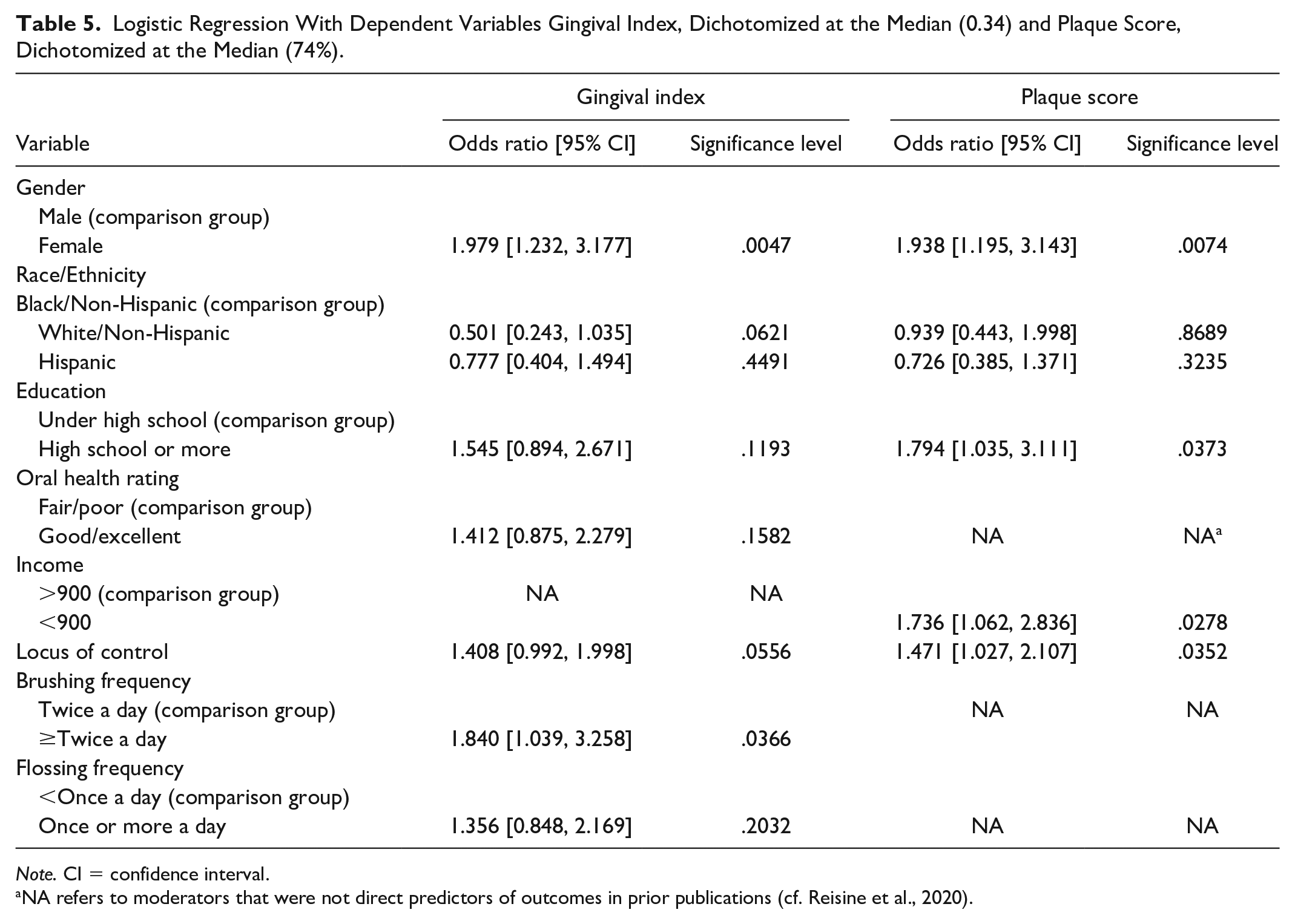
Note. CI = confidence interval.
NA refers to moderators that were not direct predictors of outcomes in prior publications (cf. Reisine et al., 2020).
Path Analysis
Path analytic modeling was performed to test the hypothesized models for both GI and PS with all mediators and moderators. Standardized coefficients (β) for all paths were estimated. The goodness-of-fit of models was assessed by a non-significant χ2 value, root mean square error of approximation (RMSEA) ≤ 0.06, Tucker–Lewis Index (TLI) ≥ 0.90, and comparative fit index (CFI) ≥ 0.95 (Bryan et al., 2007; Hu & Bentler, 1999). As the model did not fit well with all mediators included for either of the outcomes, we reduced variables one by one in the originally hypothesized models for both GI and Plaque and found that the following models fit the data well (see Figure 2).
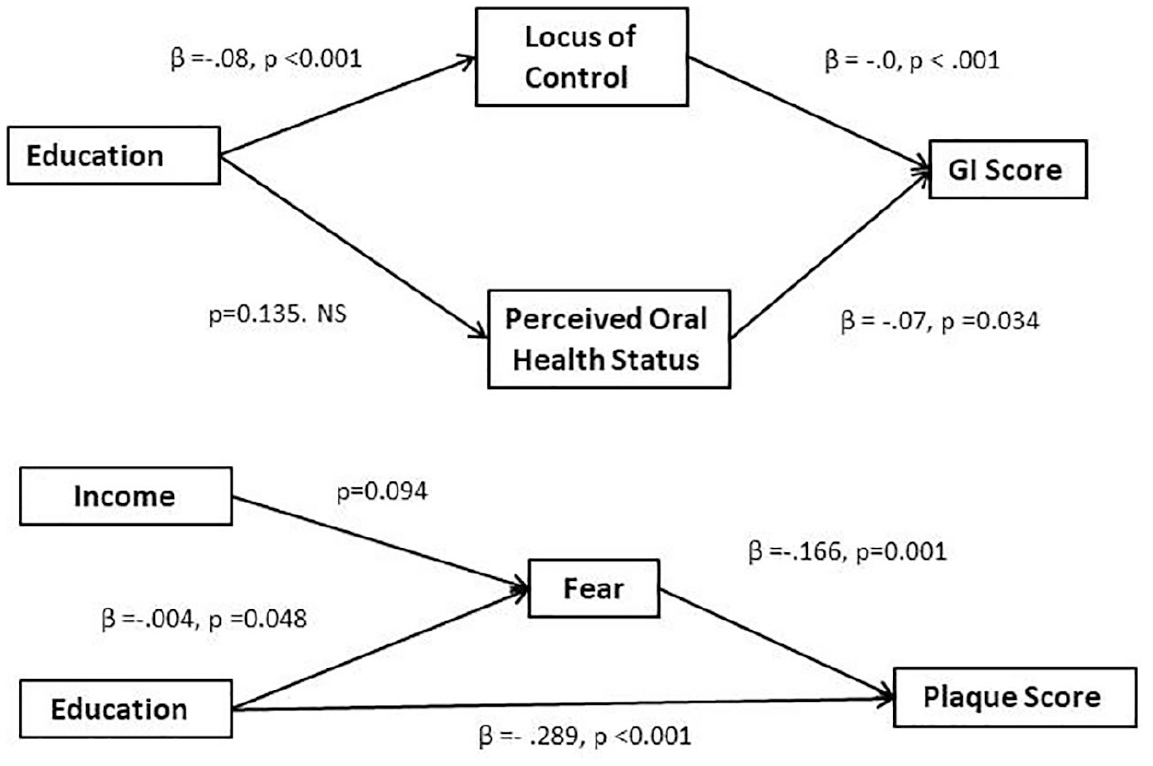
Path analysis for GI and PS.
GI score
The path analysis showed that the hypothesized model fits the data: χ2(2) = 1.22, p = .54, CFI = 1.00, TLI =1.04, standardized root mean square residual (SRMR) = .02, RMSEA ≤ 0.05 = .75, 90% CI = [0.000, 0.094]. Higher GI score was significantly associated with lower locus of control (β = −.0, p < .001) and lower perceived risk of oral health problems (β = −.07, p = .034). Indirect effects were tested on the mediating effect of locus of control and oral health perceived risk of oral health problems on the relationship between education and GI score. More education predicted lower GI score via higher locus of control (β = −.08, p < .001). However, the indirect effect of education on GI score via perceived risk of oral health was not significant (p = .135).
PS
The path analysis showed that the hypothesized model fits the data: χ2 (1) = 0.52, p = .473, CFI = 1.00, TLI =1.045, SRMR = .012, RMSEA ≤ 0.05 = .63, 90% CI = [0.000, 0.129]. Higher PS was significantly associated with less fear (β =−.166, p = .001) and less education (β =− .289, p < .001). Indirect effects were tested for the mediating effect of fear in the relationship between age, income, and PS. The effect of education on PS was mediated by fear of oral diseases (β = −.004, p = .048). However, fear did not mediate the effect of income on PS (p = .094).
Discussion
This article evaluates the potential contributions of cognitive and behavioral mediators included in an adaptation of Fischbein’s IM that guided a clinical trial to improve oral health and hygiene self-management in older adults. This article assesses the associations among moderators (background factors), mediators, and clinical outcomes at baseline.
Most of the oral health intervention literature shows that improved brushing and flossing of teeth often improves oral health outcomes. Many of these studies do not include any form of cognitive counseling (Watt & Marinho, 2005). There are studies that are suggestive of the importance of cognitive counseling but more recent reviews suggest that the results have been inconclusive (Carra et al., 2020). Analysis of the baseline data from this study allows us to assess the relevance of the theoretical model on a naïve population, and to address the question of whether addressing psychosocial factors as well as behavior (brushing, flossing, dentures cleaning) in oral health interventions adds to the improvement of oral health outcomes and which domains are most salient in the absence of intervention. It also allows us to examine how demographic or other moderators indicative of disparities that are known to have a direct impact on clinical outcomes interact with cognitive and behavioral mediators.
Intentionality to perform oral hygiene activities, and locus of control over oral health activities, mediators, and brushing regularly and flossing, both behavioral mediators, independently predicted gingival status. Locus of control measures the degree to which people feel they have control over their behavior (Ajzen, 2002). Participants with more control had better GI outcomes. Intentionality measures the level of intention to engage in oral hygiene behaviors; furthermore, in the IM, intention is the primary domain that bridges norms, beliefs, attitudes, and behaviors leading to improved oral health. Participants with higher intentionality to maintain good oral health behaviors had lower GI scores. Participants who brushed and flossed regularly also had lower GI scores. Intentionality is an addition to the list of cognitive predictors of oral health outcome though it resembles goal directedness and planning (Newton & Asimakopoulou, 2015), while locus of control resembles self-efficacy, which has been shown to be important in oral hygiene status and improvement (Messadi et al., 2018).
GI scores reflect the consequences of ongoing regular oral hygiene practices requiring intentionality and self-control to actualize planned behavior such as brushing and flossing regularly. In this study, baseline GI scores were overall lower than expected (Li et al., 2010; Weyant et al., 2004), partially explained by the fact that a high proportion of the population was covered by dental insurance through Medicaid and some private insurance and many participants had seen a dentist in the past year (Reisine et al., 2020). However, the above-mentioned cognitive and behavioral variables were sufficiently important to contribute to better gingival health despite the narrow range of variation in GI outcome scores.
The result of the individual PS logistic regressions showed that only cognitive domains—more fears of oral diseases, less locus of control over oral hygiene behavior and more worries about self-management of oral hygiene—were associated with higher (or poorer) PS scores. Higher PS scores are markers of failure to brush and floss the teeth in the days and hours prior to the clinical assessment perhaps resulting from avoidance due to fear of painful or damaging consequences of inappropriate or inadequate oral hygiene practices. The individual regressions suggest that counseling to reduce fears and worries, improve locus of control, and intention to perform good oral hygiene along with brushing and flossing should lead to improved GI and PSs. Intervention cutoff scores were heavily weighted in favor of fears, worries, and locus of control, confirming the centrality of these domains in the model.
In this study PSs were comparable to other similar older adult populations (Brennan et al., 2017, #353). It is a somewhat unexpected finding that overall, only cognitive mediators were significant predictors of PS although those that emerged as significant were explainable. Fears and worries are closely associated, and those with fewer worries and fears about oral health and greater locus of control would be expected to have lower PSs. In addition, locus of control is associated with regular flossing (r = .210, sig. < .001; ρ = .194, sig. < .001) suggesting the possibility that locus of control might lead to flossing, which might help to reduce PSs although this mediational hypothesis was not demonstrated in the path analysis.
Multiple logistic regression results further reinforce the importance of combining cognitive and behavioral domains, especially in reducing GI. The combination of greater locus of control and more frequent brushing predicted lower GI score. For PS, only higher locus of control predicted lower PS. These results highlight the importance of locus of control in promoting improved oral hygiene in vulnerable older adults. The IM is based on the central role of intention as a mediator of other cognitive and behavioral variables. In this analysis, at baseline, intention appears to play a less important role in comparison with locus of control. This is unsurprising because a number of researchers have questioned either the directionality of behavior and intentions, or the consistency of intention in predicting specific behaviors (Ajzen, 2015; Sniehotta et al., 2014).
In the final models, several demographic variables were significant predictors in addition to cognitive and behavioral variables. For GI, gender outweighed race and class, with women faring better than men for both GI and PS, consistent with other research on gender differences (Wiener et al., 2012). For PS, race/ethic disparities disappeared in the face of gender (female) and class differences (higher income and more education). Other studies show that women have better oral health than men (Wiener et al., 2012). Class disparities are known to be associated with poor access to dental treatment, information about oral health and hygiene, and lower oral health status (Griffin et al., 2019; Huang & Park, 2015; Patrick et al., 2006).
The study conceptual model did not specifically hypothesize which of the mediators with the exception of intention would have the most impact on the clinical outcomes. The path analysis hypothesized pathways through which moderators that predicted GI and PS were mediated by the cognitive and behavioral variables. The final results show that education, a key moderator, is mediated by cognitive variables—locus of control (GI) and fear of oral diseases (PS) further highlighting the importance of cognitive variables in achieving oral health outcomes. Beyond gender and ethnicity, tailoring to the education level of participants is critical for potentiating key mediators to improve oral health outcomes.
Limitations of the article include lower than expected GI scores with responses skewed toward the positive. We adjusted for this using the median in the primary logistic regression analyses for both GI and PS. To avoid losing power in the path analysis, we utilized the continuous form of these outcome variables which produced richer results. For PS, participants may have inflated reports of frequency of brushing and flossing or mentioned frequency of brushing and flossing in general rather than in the past day or two limiting the impact of these measures as predictors of PS.
This was a cross-sectional analysis evaluating an intervention theory. The study responded to the call by many reviewers for a comprehensive integrated cognitive/behavioral theoretical framework for predicting and guiding oral health outcomes in older adults (Simpson, 2011), and the need for more attention to cognitive variables to explain intervention outcomes (citations). It highlights the main cognitive, emotional, and behavioral variables that have an effect on outcomes, examines the effects of demographic differences on these variables, and points to the importance of combining counseling with behavioral interventions to improve oral health indicators in low-income older adult populations. Finally, the results suggest that that special consideration should be given to men, Latinos, and those with limited education. Future analyses will assess whether tailoring to theoretical domains and relevant moderators will achieve improved oral health outcomes as predicted.
Supplemental Material
sj-pptx-1-jag-10.1177_0733464820974920 – Supplemental material for Evaluating Cognitive/Emotional and Behavioral Mediators of Oral Health Outcomes in Vulnerable Older Adults
Supplemental material, sj-pptx-1-jag-10.1177_0733464820974920 for Evaluating Cognitive/Emotional and Behavioral Mediators of Oral Health Outcomes in Vulnerable Older Adults by Jean J. Schensul, Apoorva Salvi, Toan Ha, James Grady, Jianghong Li and Susan Reisine in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors acknowledge the contributions of members of the study team, Amauri Barbosa, Rita Bodea, Joanna Douglass, Colleen Foster-Bey, Ruth Goldblatt, Rosely Gonzalez, Rajesh Lalla, Zahira Medina, Kim Radda, Eduardo Robles, Lucy Rohena, and members of the Oral Health Campaign Committees in all study buildings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Dental and Craniofacial Research Grant #5U01DE024168.
IRB Review
The studies were approved annually by the UCONN Health Center IRB, final IRB approval number 14-1990-6.1, IRB Panel 1; and the Institute for Community Research IRB deferred to the UCONN Health Center IRB.
Trial Registration
Clinicaltrials.gov: NCT02419144.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.