
Abstract
Introduction
Sexual minority populations (e.g., gay/lesbian and bisexual) in the United States (U.S.) may be at increased risk for multimorbidity (defined as the co-occurrence of two or more chronic diseases) as they experience significant health disparities compared to their heterosexual counterparts across the life span (Johnston et al., 2019; National Institutes of Health, 2020; Office of Disease Prevention and Health Promotion, 2020). The minority stress model is the predominant explanation for these health disparities (Brooks, 1981; Meyer, 2003). The minority stress model postulates that exposure to unique minority stressors (e.g., sexual orientation–based discrimination, bias-motivated violence, and expectations of rejection) contributes to negative health outcomes among sexual minority individuals. A growing body of research indicates that sexual minority adults have a higher prevalence of current tobacco use (Blosnich et al., 2013), heavy drinking (Caceres, Makarem, et al., 2019; Dermody et al., 2014), and short sleep duration (Butler et al., 2020; Caceres, Hickey, et al., 2019) relative to heterosexual adults. In addition, sexual minority adults report higher rates of mental health conditions (e.g., depression, anxiety, and suicidal ideation) (Plöderl & Tremblay, 2015).
The aforementioned disparities in health behaviors and mental health can increase risk for chronic disease in sexual minority adults as they age. Multiple studies indicate sexual minority adults have a higher prevalence of diabetes (Fredriksen-Goldsen et al., 2013; Gupta & Sheng, 2020; Liu et al., 2019), cardiovascular disease (Caceres, Makarem, et al., 2019; Gupta & Sheng, 2020), cancer (Gonzales & Zinone, 2018), asthma (Fredriksen-Goldsen et al., 2017; Simoni et al., 2017), and chronic obstructive pulmonary disease (Ward et al., 2015) than heterosexual adults. The prevalence of overweight and obesity is also higher among sexual minority women (Caceres et al., 2018a; Caceres, Markovic, et al., 2019; Fredriksen-Goldsen et al., 2013) and bisexual men (Caceres et al., 2018b) than their heterosexual peers.
Medical advances and demographic changes (such as increased life expectancy) over the past century have contributed to an increased prevalence in noncommunicable diseases worldwide (Kochanek et al., 2020; World Health Organization, 2014). Moreover, between 2018 and 2060, the population of adults over the age of 65 years in the U.S. is anticipated to increase by more than 50% (Administration for Community Living, 2020). Aging overall increases the susceptibility for the development of multimorbidity, which presents a growing challenge for patients, their families, and the healthcare system in the U.S. (Afshar et al., 2015; Fabbri et al., 2015; Sakib et al., 2019). Consistent with increases in the older adult population in the U.S., the prevalence of multimorbidity among American adults has increased from 45.7% in 1988 to 59.6% in 2014 (King et al., 2018). In addition to age, factors associated with increased risk of multimorbidity include a racial/ethnic minority identity (Lim et al., 2018; Quiñones et al., 2019; Tann et al., 2007), lower educational attainment (Jackson et al., 2016), greater socioeconomic disadvantage (Gallacher et al., 2018; Katikireddi et al., 2017), and cigarette smoking (Gallacher et al., 2018; Jackson et al., 2016).
Adults with multimorbidity have complex care needs due to increased treatment burden and often conflicting treatment recommendations (Aldridge & Bradley, 2017). Multimorbidity is also associated with greater healthcare utilization (Bähler et al., 2015; Picco et al., 2016) and functional impairment (Fox & Reichard, 2013; Griffith et al., 2017). In 2017, approximately, 68% of Medicare beneficiaries who had two or more chronic diseases accounted for nearly 94% of total Medicare spending (Centers for Medicare and Medicaid Services, 2017). This contributes to a significant portion of healthcare spending in the U.S. (Hartman et al., 2020).
Multimorbidity is also associated with increased mortality in middle-aged and older adults. Analyses of data from the Health and Retirement Study found that among adults over the age of 50 years, those with two or more chronic diseases were more than five times as likely to die within the next two years than those with no chronic disease (Koroukian et al., 2015). Similarly, analyses of Medicare claims data found among Medicare beneficiaries over the age of 67 years, each additional chronic disease reported was linked with an average of 1.8 -year decline in life expectancy (Dugoff et al., 2014).
Increasing understanding of the epidemiology of multimorbidity and addressing disparities in multimorbidity have been identified as objectives of the U.S. Department of Health and Human Services (Parekh & Goodman, 2013). The increase in the proportion of older adults and corresponding increase in the prevalence of multimorbidity has led to calls to identify groups at greatest risk for multimorbidity and develop strategies to mitigate the burden of multimorbidity among adults (Fabbri et al., 2015). Despite a growing understanding that sexual minority adults have higher risk for chronic disease than heterosexual adults, multimorbidity in this population is understudied. Two analyses of data from the National Health Interview Survey found sexual minority adult and older adult women may have a higher prevalence of multimorbidity than heterosexual women (Fredriksen-Goldsen et al., 2017; Gonzales et al., 2016). In contrast, analyzing data from the National Survey of Drug Use and Health, researchers found that among adults over the age of 50 years, gay men as well as bisexual men and women had approximately two to three times higher odds of multimorbidity than heterosexual adults of the same sex (Han et al., 2020). However, no differences between lesbian and heterosexual women were identified. Given these conflicting findings, additional research examining multimorbidity in sexual minority adults is needed to determine which subgroups may be at greatest risk.
Using data from the 2014–2018 Behavioral Risk Factor Surveillance System (BRFSS), the objective of the present study was to investigate sexual identity differences in multimorbidity among cisgender (individuals whose sex assigned at birth matches their gender identity) adults in the U.S. Based on previous evidence, we hypothesized that cisgender sexual minority adults would have higher odds of multimorbidity than cisgender heterosexual adults of the same sex. Further, because multimorbidity increases with age (Gallacher et al., 2018; Schiøtz et al., 2017), we conducted exploratory analyses examining whether the hypothesized differences in multimorbidity between cisgender sexual minority and heterosexual adults differed across age-groups. We hypothesized cisgender sexual minority adults would have higher odds of multimorbidity relative to heterosexual adults of the same sex across all age-groups.
Methods
Sample
The BRFSS is a nationally representative cross-sectional telephone survey that assesses health behaviors, chronic diseases, and healthcare utilization patterns among adults in the U.S. Data are collected every year from more than 400,000 noninstitutionalized adults (aged 18 years and over) living in private homes across all 50 states, the District of Columbia, and three U.S. territories. Adults living in nonresidential settings (e.g., military bases, college dormitories, nursing homes, and prisons) are not eligible for inclusion in the BRFSS. To select potential participants, the BRFSS uses random digit dialing techniques. State health departments, with assistance from the Centers for Disease Control and Prevention, conduct telephone interviews in English and Spanish (depending on participant preference) continuously throughout the year using cellphones and landlines. Between 2014 and 2018, cellphone response rates for the BRFSS ranged from 40.2% to 47.2%. Landline response rates ranged between 2014 and 2018 ranged from 45.3% to 48.7%. The BRFSS response rates are generally higher than other national population-based studies (e.g., the National Immunization Survey and the National Adult Tobacco Survey) (Centers for Disease Control and Prevention, 2015a, 2015b, 2017, 2018b, 2019a).The BRFSS methodology has been described in detail previously (Centers for Disease Control and Prevention, 2018a).
For the present study, we combined data from the 2014–2018 BRFSS surveys. In 2014, the Centers for Disease Control and Prevention gave individual states the option of completing a module that included questions on sexual orientation and gender identity. This module is currently one of the 25 optional modules that are selected by states each year. The sexual orientation and gender identity module was used by 19 states in 2014, 22 states in 2015, 25 states in 2016, 27 states in 2017, and 30 states in 2018.
Sample Selection
Our objective was to examine differences in multimorbidity between cisgender sexual minority and heterosexual adults. The present analysis included all adult participants in the 2014–2018 BRFSS with complete data for sexual identity and all study variables. Transgender adults (individuals whose sex assigned at birth does not match their gender identity) were excluded from this analysis. Data from cohort studies indicate that more than half of transgender adults are currently on gender-affirming hormones (James et al., 2016; Kidd et al., 2019). Given that the BRFSS does not include data on gender-affirming hormone use, a potential contributor to chronic disease development in transgender adults (Braun et al., 2017; Caceres et al., 2020), we excluded all transgender participants (n = 3524), regardless of their sexual identity. To reduce potential misclassification of transgender persons as cisgender, we also excluded participants who responded do not know (n = 5740) or refused (n = 7453) to the gender identity item. Therefore, this analysis compared cisgender sexual minority adults to cisgender heterosexual adults that participated in the BRFSS (2014–2018).
Measures
Independent variable
Participants were asked to report their sexual identity with the following question: “Do you consider yourself to be straight, lesbian or gay, bisexual, other, do not know, or not sure?” We excluded participants who provided the response “do not know or not sure” or refused to answer this item. Those who identified as “straight” were categorized as heterosexual. Participants who identified their sexual identity as “other,” meaning something other than heterosexual, lesbian, gay, or bisexual were included in a separate category.
Dependent variable
In the BRFSS, participants were asked whether a healthcare professional had ever diagnosed them with any of the following chronic diseases: arthritis (e.g., rheumatoid arthritis, osteoarthritis, gout, lupus, and fibromyalgia), asthma, cancer, kidney disease, chronic obstructive pulmonary disease (i.e., emphysema or chronic bronchitis), coronary heart disease or angina, depressive disorder (i.e., depression, major depression, dysthymia, or minor depression), diabetes, heart attack, high cholesterol, hypertension, and stroke (yes vs. no). In addition, obesity (body mass index ≥30 kg/m2) was calculated based on participants’ self-reported height and weight (Centers for Disease Control and Prevention, 2020). We then created a variable to account for multimorbidity, defined as the presence of two or more chronic diseases, with “0” indicating no chronic diseases, “1” indicating at least one chronic disease, and “2” indicating multimorbidity.
Covariates
We assessed age (18–29; 30–39; 40–49; 50–59; 60–69; 70–79; and ≥80 years), race/ethnicity (white; Black; Latino/a; Asian/Pacific Islander; other race), income (<$15,000; $15,000–$24,999; $25,000–$34,999; $35,000–$49,999; and ≥$50,000), education (did not graduate high school; graduated high school; attended college/technical college; and graduate college/technical college), relationship status (married/partnered; divorced/separated; widowed; and single), and employment status (employed/self-employed; unemployed; homemaker; student; retired; and unable to work). We assessed participants’ smoking status (current smoker; former smoker; and never smoker). Existing evidence suggests that sexual minority adults, in particular bisexual adults, are more likely to delay care due to costs than heterosexual adults which may be associated with underreporting of chronic diseases (Caceres, Makarem, et al., 2019; Dahlhamer et al., 2016). Therefore, we assessed variables related to healthcare access and utilization including whether participants had current healthcare coverage (yes vs. no), delayed health care in the past year due to costs (yes vs. no), and had a routine checkup within the past year (yes vs. no).
Statistical Analyses
Stata version 16 was used for all analyses. BRFSS 2014–2018 survey data were combined, and survey weights were applied based on analytic recommendations from the Centers for Disease Control and Prevention (2018c). Heterosexual participants were the reference group for all analyses. All analyses were sex-stratified. We used the Rao–Scott chi-square test to examine differences between sexual minority and heterosexual participants across study variables. A significance level of p < .01 was used for bivariate analyses to account for multiple comparisons.
We then used sex-stratified multinomial logistic regression models to estimate the odds ratios with 95% confidence intervals for the association between sexual identity with multimorbidity. Model 1 was unadjusted. Model 2 added adjustment for a priori covariates including age, race/ethnicity, income, education, relationship status, employment status, smoking status, survey year, and state. Model 3 added healthcare coverage, healthcare delayed in the past year due to costs, and routine checkup in the past year. Last, we used sex-stratified multinomial logistic regression models to conduct exploratory analyses examining differences in multimorbidity between sexual minority and heterosexual participants within the same age-group (i.e., 18–29; 30–39; 40–49; 50–59; 60–69; 70–79; and ≥80 years) adjusted for covariates.
Results
The sample included 687,151 adults with a mean age of 49.1 years. Approximately, half of participants were female (50.1%), 68.3% identified as white, 61.8% had greater than a high school education, 52.3% had incomes greater than $50,000 per year, 60.1% were employed, and 58.5% were married. The prevalence of multimorbidity in the total sample was 42.8%. The prevalence of multimorbidity was positively associated with age. The prevalence of multimorbidity was 18.0% for participants between ages 18 and 29 years, 25.8% for ages 30–39 years, 35.4% for ages 40–49 years, 48.7% for ages 50–59 years, 60.7% for ages 60–69 years, and 70.0% for both participants 70–79 years and those over the age of 80 years.
Sexual Identity Differences for Demographic Characteristics, Smoking Status, Healthcare Utilization, and Multimorbidity among Women, Behavioral Risk Factor Surveillance System 2014–2018 (N = 375,609).
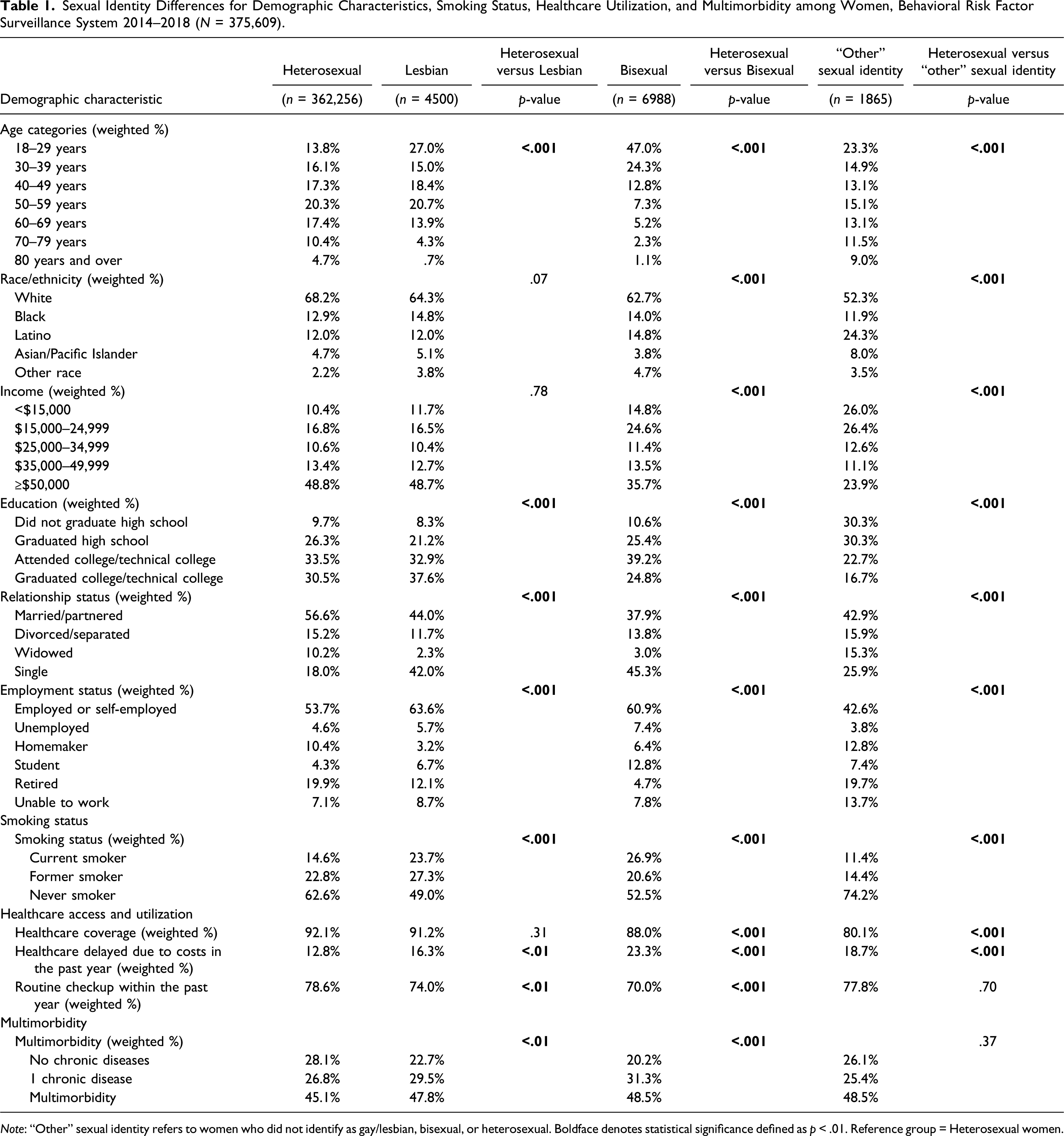
Note: “Other” sexual identity refers to women who did not identify as gay/lesbian, bisexual, or heterosexual. Boldface denotes statistical significance defined as p < .01. Reference group = Heterosexual women.
Sexual Identity Differences For Demographic Characteristics, Smoking Status, Healthcare Utilization, and Multimorbidity among Men, Behavioral Risk Factor Surveillance System 2014–2018 (N = 311,542).
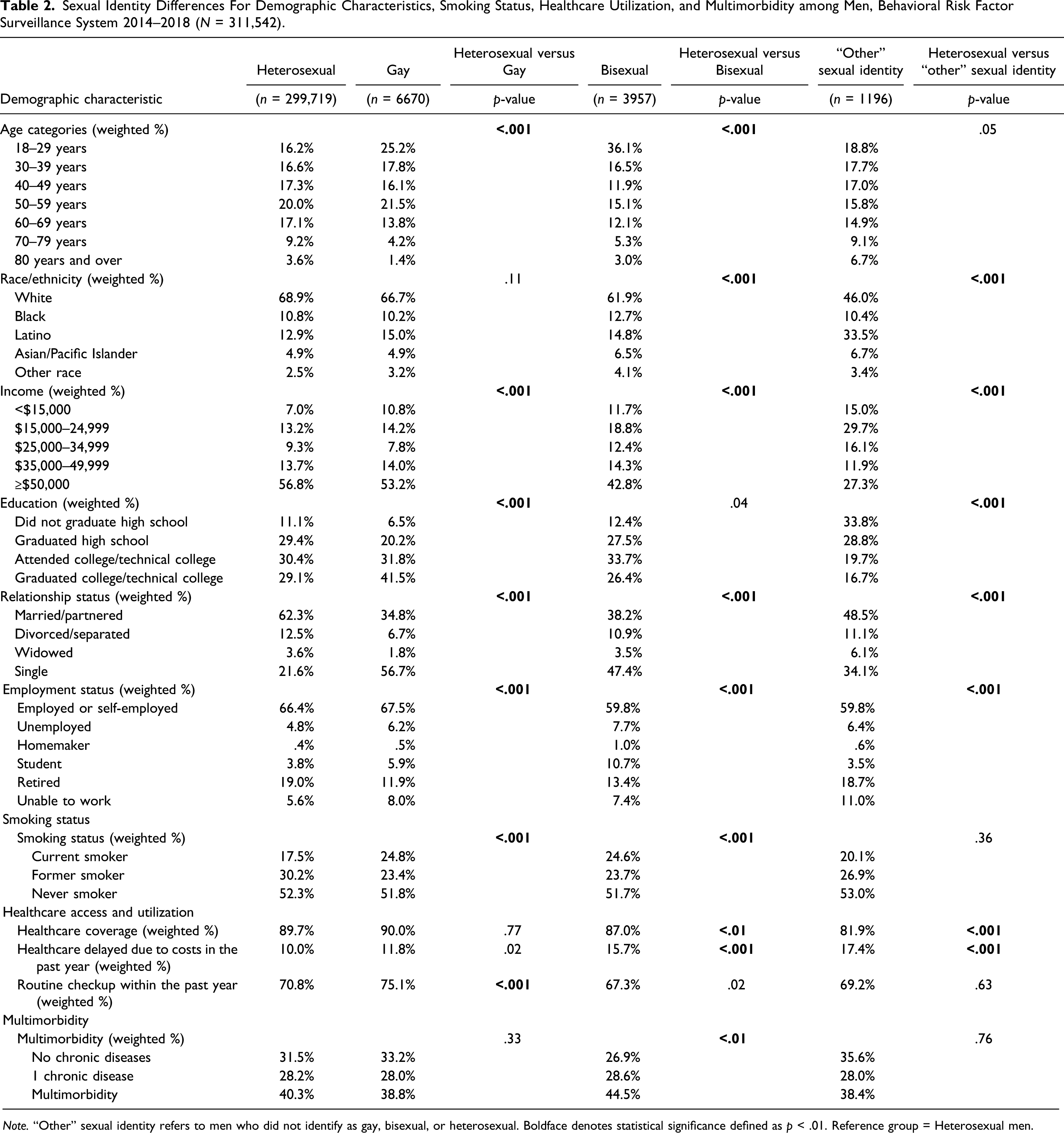
Note. “Other” sexual identity refers to men who did not identify as gay, bisexual, or heterosexual. Boldface denotes statistical significance defined as p < .01. Reference group = Heterosexual men.
Results of Multinomial Logistic Regression Models Examining Sexual Identity Differences in Multimorbidity in Men And Women, Behavioral Risk Factor Surveillance System 2014–2018 (N = 687,151).
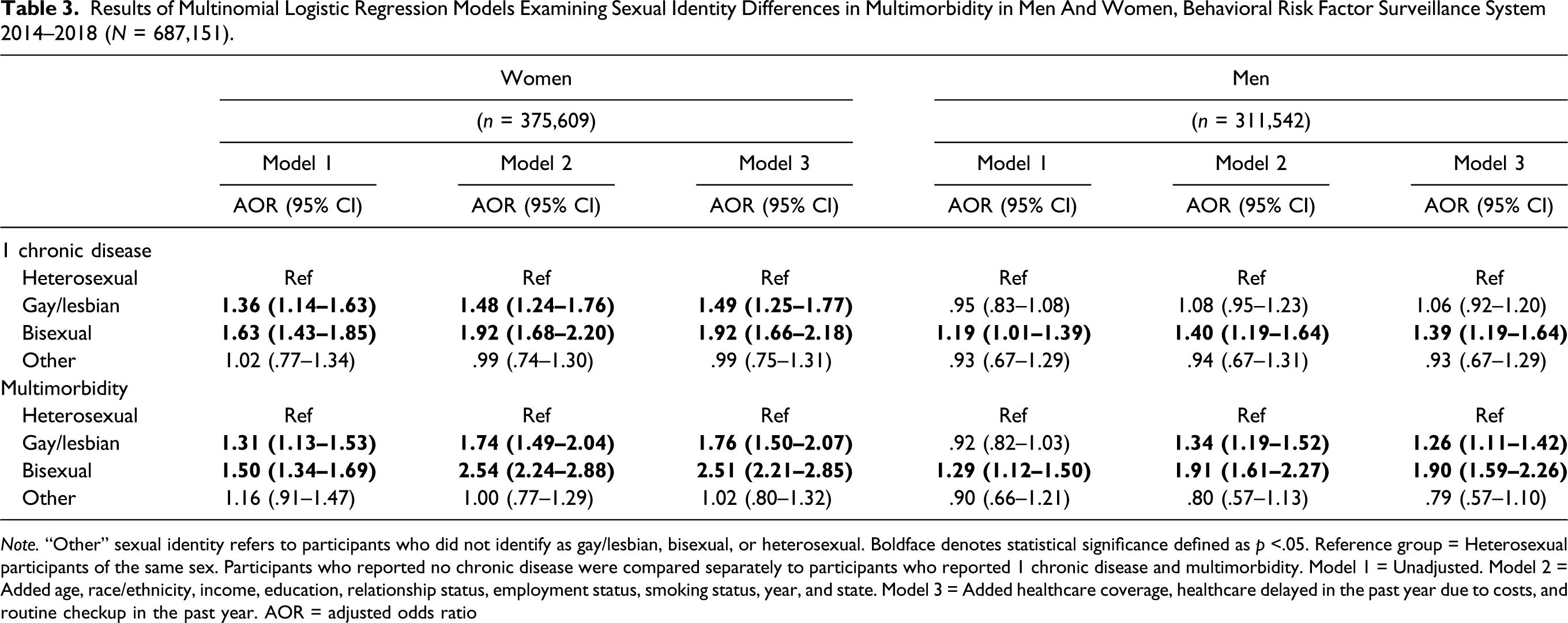
Note. “Other” sexual identity refers to participants who did not identify as gay/lesbian, bisexual, or heterosexual. Boldface denotes statistical significance defined as p <.05. Reference group = Heterosexual participants of the same sex. Participants who reported no chronic disease were compared separately to participants who reported 1 chronic disease and multimorbidity. Model 1 = Unadjusted. Model 2 = Added age, race/ethnicity, income, education, relationship status, employment status, smoking status, year, and state. Model 3 = Added healthcare coverage, healthcare delayed in the past year due to costs, and routine checkup in the past year. AOR = adjusted odds ratio
Supplementary Table presents results of multinomial logistic regression models examining differences in multimorbidity between sexual minority and heterosexual participants within the same age-group. Lesbian (ages 18–29 years: AOR 1.59, 95% CI = 1.08–2.33; ages 30–39 years: AOR 1.65, 95% CI = 1.15–2.38; ages 40–49 years: AOR 2.18, 95% CI = 1.53–3.10) and bisexual women (ages 18–29 years: AOR 2.87, 95% CI = 2.36–3.48; ages 30–39 years: AOR 4.20, 95% CI = 3.14–5.62; ages 40–49 years: AOR 2.39, 95% CI = 1.76–3.25) in the youngest three age-groups were more likely to report multimorbidity than heterosexual women of the same age. Also, between the ages of 50–59 years, lesbian women had higher odds of reporting multimorbidity than heterosexual women of the same age (AOR 1.80, 95% CI = 1.29–2.51), whereas no differences were noted between bisexual and heterosexual women. This pattern was reversed among women between ages 60 and 69 years with no difference found between lesbian and heterosexual women (AOR 1.43, 95% CI = .94–2.17), but bisexual women were nearly twice as likely as heterosexual women to have multimorbidity (AOR 1.92, 95% CI = 1.34–2.75). No differences were observed between sexual minority and heterosexual women at ages 70–79 years, but lesbian women over 80 years of age were less likely to report multimorbidity (AOR .27, 95% CI = .11–.67) than heterosexual women. Between the ages of 18 and 29 years, women who identified their sexual identity as “other” had higher odds of multimorbidity than heterosexual women (AOR 2.13, 95% CI = 1.23–3.70), but this difference was attenuated at older ages.
Bisexual men in the youngest three age-groups had higher odds of multimorbidity than their heterosexual peers (ages 18–29 years: AOR 3.48, 95% CI = 2.53–4.78; ages 30–39 years: AOR 1.80, 95% CI = 1.26–2.57; ages 40–49 years: AOR 1.63, 95% CI = 1.11–2.40). No differences were found between bisexual and heterosexual men from ages 50–59 and 60–69 years, but bisexual men ages 70–79 years were more likely to report having multimorbidity (AOR 1.76, 95% CI = 1.01–3.08). Gay men in the 30–39 (AOR 1.41, 95% CI = 1.03–1.92) and 60–69 years of (AOR 1.47, 95% CI = 1.09–1.99) age-groups were more likely to report multimorbidity than heterosexual men. Compared to heterosexual men, men who identified their sexual identity as “other” had higher odds of reporting having multimorbidity between the ages of 18 and 29 years (AOR 2.51, 95% CI = 1.18–5.31), the youngest age-group. Although no differences were found between heterosexual men and men who identified their sexual identity as “other” between the ages of 30–39 and 40–49 years, at ages 50–59 (AOR .30, 95% CI = .15–.62) and 70–79 years (AOR .28, 95% CI = .13–.60), men who identified their sexual identity as “other” were less likely to have multimorbidity.
Discussion
This study contributes to our understanding of multimorbidity among sexual minority adults of various ages. Consistent with our hypothesis, our main analyses found that gay, lesbian, and bisexual participants had higher odds of multimorbidity than heterosexual adults of the same sex. Our exploratory analyses examining sexual identity differences in multimorbidity by age-groups found the odds of multimorbidity were higher among lesbian women under the age of 60 years and bisexual men and women under the age of 50 years. Despite higher odds of reporting multimorbidity between the ages of 18 and 29, men who identified their sexual identity as “other” had similar or lower multimorbidity than heterosexual men as they aged.
Our findings corroborate previous evidence that bisexual women are more likely to have multimorbidity than heterosexual women. Previous studies have reported conflicting evidence for differences in multimorbidity when comparing lesbian women and sexual minority men to heterosexual adults of the same sex. Analyzing data from the National Health Interview Survey, Gonzales et al. (2016) and Fredriksen-Goldsen et al. (2017) found that lesbian and bisexual women were more likely than heterosexual women to report having two or more chronic diseases. However, they found no differences between sexual minority and heterosexual men. In contrast, Han et al. (2020) found that gay men as well as bisexual men and women, but not lesbian women, were more likely to report multimorbidity than their heterosexual peers. Altogether, the existing evidence has consistently found elevated odds of multimorbidity among bisexual women.
Further, lesbian, gay, and bisexual adults in the present study had higher odds of reporting multimorbidity than their heterosexual peers, but the magnitude of this association was consistently greater among bisexual adults. One possible explanation is that bisexual adults experience stigma and rejection from both heterosexual and gay/lesbian communities and peers that can increase their risk for negative health outcomes (Bostwick, 2012). Previous work has found that bisexual adults experience worse health outcomes than heterosexual and gay/lesbian adults, including mood disorders (Bostwick et al., 2010), short sleep duration (Caceres, Hickey, et al., 2019; Caceres & Hickey, 2019), substance use (Talley et al., 2016), and higher cardiovascular disease risk (Caceres et al., 2018a, 2018b). Our findings indicate that bisexual adults may be at greatest risk for multimorbidity. Future studies should assess factors that contribute to this observed difference to better understand how to prevent multimorbidity in bisexual individuals.
Our exploratory analyses stratified by age found the higher odds of multimorbidity observed in lesbian women, and bisexual participants in the main analyses were attenuated with age. Lesbian women over the age of 60 years and bisexual participants over the age of 50 years had no differences in multimorbidity compared to heterosexual peers. There are several possible explanations for these results. First, given the higher rates of multimorbidity among lesbian women under the age of 60 years and bisexual men and women under the age of 50 years, it is possible that due to greater exposure to adverse life experiences such as minority stressors, these populations experience higher mortality rates prior to entering old age. Although we were unable to assess minority stressors in the present study, data from population-based studies indicate that exposure to greater perceived discrimination is associated with higher mortality in the general population (Barnes et al., 2008; Farmer et al., 2019). Previous evidence has identified higher mortality rates among sexual minority women than heterosexual women. Using data on postmenopausal women (ages 50–79 years) from the Women’s Health Initiative, investigators found sexual minority women had higher rates of all-cause and cancer-specific mortality relative to heterosexual women (Lehavot et al., 2016). Previous studies have also found sexual minority women have higher breast cancer mortality than heterosexual women (Boehmer et al., 2013; Cochran & Mays, 2012). To date, no studies have examined discrimination or other minority stressors as predictors of multimorbidity or mortality in sexual minority adults. Older sexual minority participants in our study might represent a subset of individuals that were generally healthier across the life course than sexual minority individuals who did not survive into old age. As age is a strong predictor of multimorbidity, it is also possible that as sexual minority and heterosexual participants age, the differences in multimorbidity we observed in younger group may attenuate.
Moreover, our measure of multimorbidity included depressive disorder. Depression and other mental health diagnoses are commonly included in multimorbidity measures (Afshar et al., 2015; Johnston et al., 2019; Schiøtz et al., 2017). However, there is evidence that older sexual minority adults (defined as ≥50 years old) report a lower prevalence of depression than their younger counterparts (Monin et al., 2017). Crisis competence theory posits that as they age, sexual minority adults develop coping skills that buffer the negative effects of stress on their well-being. Greater crisis competence has been identified as a potential explanation for differences in mental health outcomes between older and younger sexual minority adults (Caceres & Frank, 2016; Friend, 1991). We conducted additional analyses to identify if a higher prevalence of depressive disorder among lesbian women under the age of 60 years and bisexual adults under the age of 50 years explained the higher odds of multimorbidity found in those groups. We found that lesbian women and gay and bisexual men had a higher prevalence of depressive disorder than heterosexual adults of the same sex at all ages, except age ≥80 years. Bisexual women had a higher prevalence of depressive disorder than heterosexual women at all ages, except age ≥70 years. We conclude that depressive disorder alone does not explain the sexual identity differences in multimorbidity we found across age-groups. Future research should replicate our analyses to investigate whether sexual identity differences in multimorbidity are consistent across different samples and to investigate potential explanations for these differences.
Our findings contribute to understanding of the health of individuals who identify their sexual identity as something other than gay/lesbian, bisexual, or heterosexual. To our knowledge, this is the first study to examine multimorbidity in that group. We found no differences in multimorbidity between women who identified their sexual identity as “other” relative to heterosexual women over the age of 30 years. Among men, we found that those who identified their sexual identity as “other” had lower odds of multimorbidity relative to heterosexual men between ages 50–59 and 70–79 years. Reasons for these differences are not well understood and should be investigated further. However, it is likely that misclassification of sexual identity may have occurred among individuals who identified their sexual identity as “other.” For instance, in the BRFSS, these individuals were generally older than their heterosexual counterparts. Also, individuals that comprised this group may represent a number of sexual identities (e.g., queer and questioning) who may differ from one another in significant ways. The response options provided for the sexual identity item in the BRFSS are not inclusive of all sexual identities. This is especially true for younger sexual minority adults who are more likely to identify their sexual identity as queer (Goldberg et al., 2020). Therefore, more research is needed to understand characteristics of individuals that identify their sexual identity as “other” in nationally representative surveys such as the BRFSS.
Implications for Practice and Research
These data highlight the importance of targeted preventive efforts for sexual minority adults. Clinicians should screen young sexual minority adults for risk factors for the development of chronic disease and multimorbidity (e.g., tobacco use and short sleep duration). It is also important that clinicians understand the environments and communities that their young sexual minority adult patients interact with on a daily basis. Sexual minority adults experience pervasive marginalization when compared to their heterosexual peers and are more likely to be victims of hate crimes and verbal, physical, and sexual abuse over their lives (Flores et al., 2020; Katz-Wise & Hyde, 2012). Strengthening resiliencies (e.g., community connectedness) have been suggested as a strategy to potentiate the effectiveness of health promotion interventions among sexual minority individuals (Herrick et al., 2014). Clinicians should additionally educate sexual minority adults on their risk factors for development of multimorbidity while assessing their access to important supports (e.g., mental and emotional). Assessment of sexual orientation in clinical settings has been identified as a challenge to providing culturally competent care for sexual minority adults (Bosse et al., 2018). Routine assessment of sexual orientation among clinicians is critical to providing culturally appropriate care to patients who identify as a sexual minority and determining which sexual minority individuals are at greatest risk for multimorbidity.
Our findings have important implications for future research on multimorbidity in sexual minority adults across the life course. Despite higher rates of risk factors for chronic diseases including tobacco use (Blosnich et al., 2013), heavy drinking (Caceres, Makarem, et al., 2019; Dermody et al., 2014), and sleep disturbances (Butler et al., 2020; Caceres, Hickey, et al., 2019), the study of multimorbidity among sexual minority adults is limited. Even fewer studies have examined the experiences of sexual minority adults with multimorbidity. Findings from qualitative studies indicate that sexual minority adults living with chronic disease face unique challenges related to chronic disease management as they age, such as discrimination from healthcare professionals, decreased social support from biological families, financial insecurity, and isolation from the sexual minority community and other sexual minority adults living with chronic disease (Grigorovich, 2015; Jowett & Peel, 2009). Findings from previous studies combined with our findings indicate this is an important area of future research as sexual minority adults may have increased barriers that may limit their access to appropriate care and resources to manage multimorbidity, such as higher rates of poverty (Badgett et al., 2019) and delays in seeking medical care due to concerns over costs (Dahlhamer et al., 2016).
Limitations
Despite its strengths, the study has several limitations. The cross-sectional nature of the BRFSS limits our ability to determine causality and precludes the examination of potential mediators of the identified associations between sexual minority identity and multimorbidity (e.g., chronic disease self-management). The limited response options to the sexual identity item in the BRFSS warrant additional work focused on better understanding individuals that comprise the “other” sexual identity group.
Given that the BRFSS does not include measures of minority stress, we were unable to examine associations between minority stressors and multimorbidity. It is possible that the higher rates of multimorbidity observed among sexual minority adults in the present study may be attributed to exposure to minority stressors. Indeed, analyzing data from the National Health, Aging, and Sexuality Study, investigators found that among sexual minority older adults, those with greater concealment and internalized homophobia were more likely to report a higher number of chronic diseases (Hoy-Ellis & Fredriksen-Goldsen, 2016). That work supports the need to examine the link between minority stressors and multimorbidity in sexual minority populations.
Our measure of multimorbidity included 13 diseases; therefore, the addition of other chronic diseases may produce different results. For instance, HIV status was not assessed in the BRFSS. Due to evidence of higher rates of HIV among gay and bisexual men (Centers for Disease Control and Prevention, 2019b) and the high prevalence of multimorbidity among people living with HIV (Chichetto et al., 2020; Navon, 2018), it is likely that we underestimated the prevalence of multimorbidity among these groups. Similarly, consistent with previous studies on multimorbidity in the general population, we included obesity (as determined by BMI) in our measure of multimorbidity (Koyanagi et al., 2014). However, recent meta-analyses concluded that despite its widespread use in clinical practice and research, BMI is an inaccurate measure of abdominal obesity (Ashwell et al., 2012; Sommer et al., 2020). Other indices of body fat (such as waist-to-hip ratio) may be better screening tools for obesity. Future work is needed to determine whether inclusion of obesity, based on elevated BMI, in multimorbidity measures is appropriate.
Moreover, although there is evidence that transgender adults have higher multimorbidity than their cisgender heterosexual peers (Dragon et al., 2017), the focus of this article was on cisgender adults. Future research should replicate our analyses in a sample of transgender adults. In particular, it is important to examine whether odds of multimorbidity differ between transgender sexual minority adults versus their transgender heterosexual peers.
Conclusion
In a population-based sample, we found higher odds of multimorbidity among cisgender gay, lesbian, and bisexual participants in our main analyses. However, our exploratory analyses found that sexual identity differences in the odds of multimorbidity differed by age. Most notably, differences in multimorbidity between cisgender sexual minority and heterosexual participants were greater among lesbian women under the age of 60 years and bisexual men and women under the age of 50 years than heterosexual adults within the same age-group and of the same sex. This study highlights the need for early prevention of chronic disease risk factors among young sexual minority individuals. Clinicians should be aware of sexual minority adults’ increased risk of multimorbidity. Future research should investigate potential reasons for the sexual identity differences in multimorbidity identified in the present study.
Supplemental Material
sj-pdf-1-jah-10.1177_0898264320983663 – Supplemental Material for Differences in Multimorbidity among Cisgender Sexual Minority and Heterosexual Adults: Investigating Differences across Age-Groups
Supplemental Material, sj-pdf-1-jah-10.1177_0898264320983663 for Differences in Multimorbidity among Cisgender Sexual Minority and Heterosexual Adults: Investigating Differences across Age-Groups by Billy A. Caceres, Jasmine Travers and Yashika Sharma in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute (K01HL146965) to Dr. Billy A. Caceres.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.