
Abstract
Poor sleep in persons with Alzheimer’s disease (AD) is a common stressor for family caregivers. Retrospective reports support associations between sleep disturbance in persons with AD and worse caregiver mood; however, prospective associations between sleep in persons with AD and caregiver outcomes have not been studied. The current study determined associations between affect and sleep of persons with AD and their caregivers using daily diary data. Multilevel mediation models indicated that sleep in persons with AD is linked to caregiver affect; furthermore, these associations are mediated by sleep characteristics in caregivers and affect in persons with AD. Daily fluctuations in sleep behaviors in persons with AD—rather than average values—were most strongly associated with caregiver outcomes. Interventions to improve sleep in persons with AD may decrease their negative affect and improve caregiver mood.
An estimated 5.5 million individuals in the United States are diagnosed with probable Alzheimer’s disease (AD), and this number is projected to grow to 13.8 million by 2050 (Hebert et al., 2013). AD is a significant public health concern due to the high costs associated with caring for persons with the disease. In the United States, family members provide the majority of care for persons with dementia (Friedman et al., 2015). Caring for a family member with AD is stressful and is associated with psychological and emotional hardship for caregivers (Mausbach et al., 2013; Richardson et al., 2013). Caregiver burden is a common reason to institutionalize persons with AD (Gallagher et al., 2011; Peter-Derex et al., 2015).
Sleep disturbance affects 25% to 50% of persons with AD (Carpenter et al., 1995; Hope et al., 1998; Lawlor, 1994; Lyketsos et al., 2012; McCurry et al., 1999; Moran et al., 2005). Caregivers of persons with AD report a wide variety of sleep problems in their care recipients, including difficulty falling asleep, nighttime awakenings, wandering, early morning awakening, and excessive daytime sleepiness (McCurry et al., 1999; Rose et al., 2011; Tractenberg et al., 2005).
Sleep disturbance is one of the most prominent stressors for family caregivers of persons with AD. Based on the transactional theory of stress (e.g., Barber et al., 2014; Lazarus & Folkman, 1984), the daily stress associated with sleep disturbance in persons with AD is hypothesized to have adverse consequences for caregiver sleep and mental health. Indeed, up to 63% of spousal caregivers of persons with AD reported disturbed nighttime sleep due to sleep behaviors (Creese et al., 2008). Caregivers for persons with dementia report more sleep disturbances compared to noncaregiving peers, especially with regard to nighttime awakenings and difficulty falling asleep (Fonareva et al., 2011).
With regard to mood disturbances among caregivers for persons with AD, poor sleep is associated with greater severity of depressive symptoms, increased caregiver burden, and poorer quality of life (e.g., Allegri et al., 2006; Gehrman et al., 2018). Prospective reports of sleep and affect indicate that sleep disturbance in caregivers is associated with greater caregiver negative affect (NA; Liu et al., 2015; McCrae et al., 2016). The current prospective study builds on this work by providing some of the first prospective data to determine how daily sleep characteristics in persons with AD affect caregiver outcomes.
The Current Study
The current daily diary study determined associations between sleep, NA, and positive affect (PA) in persons with AD and the daily sleep, NA, and PA of their family caregivers. Consistent with the transactional theory of stress (e.g., Lazarus & Folkman, 1984), we conceptualized sleep disturbance in persons with AD as a daily stressor that is associated with poor mental health outcomes in caregivers (Allegri et al., 2006; McCurry et al., 2007). Specifically, we hypothesized that sleep disturbance in the person with AD would be associated with greater NA and lower PA in the caregiver the following day. To more closely probe the association between sleep in persons with AD and caregiver mood, we examined caregiver sleep and affect of the person with AD as mediators between sleep in persons with AD and caregiver daily mood. For these mediational analyses, we hypothesized that sleep disturbance in the person with AD would be associated with sleep disturbance in the caregiver, which would in turn result in greater NA and lower PA for the caregiver the following day. Likewise, we hypothesized that sleep disturbance in the person with AD would be associated with greater NA and lower PA in the person with AD, which would in turn result in poorer caregiver affect (e.g., greater NA and/or lower PA). More information about the daily fluctuations in sleep and affect in persons with AD—and subsequent effects on caregiver outcomes—will lay the foundation for development of interventions to improve caregiver affect and potentially postpone institutionalization for persons with AD.
Method
Participants
Participants were 40 family caregivers of persons diagnosed with possible or probable AD by a physician (as reported by the caregiver; Table 1). Participants were recruited via flyers and press releases at senior centers and via talks at local organizations, including support groups for caregivers of persons with AD and the Alzheimer’s Association Massachusetts and New York City chapters. This study used part of the eligibility criteria from the Resources for Enhancing Alzheimer’s Caregiver Health (REACH II) study (Belle et al., 2006) for caregiver inclusion criteria. Caregivers needed to provide care for a relative with diagnosed AD for at least 4 hours per day for at least the past 6 months, live with the person with AD, and be able to report on their own and the person with AD’s sleep. Caregivers were excluded for cognitive impairment and/or a diagnosis of a primary sleep disorder apart from insomnia (e.g., narcolepsy, sleep apnea). Caregivers were compensated with a $10 gift certificate and were entered in a lottery to win one of four $50 prizes.
Demographic Characteristics of Participants.
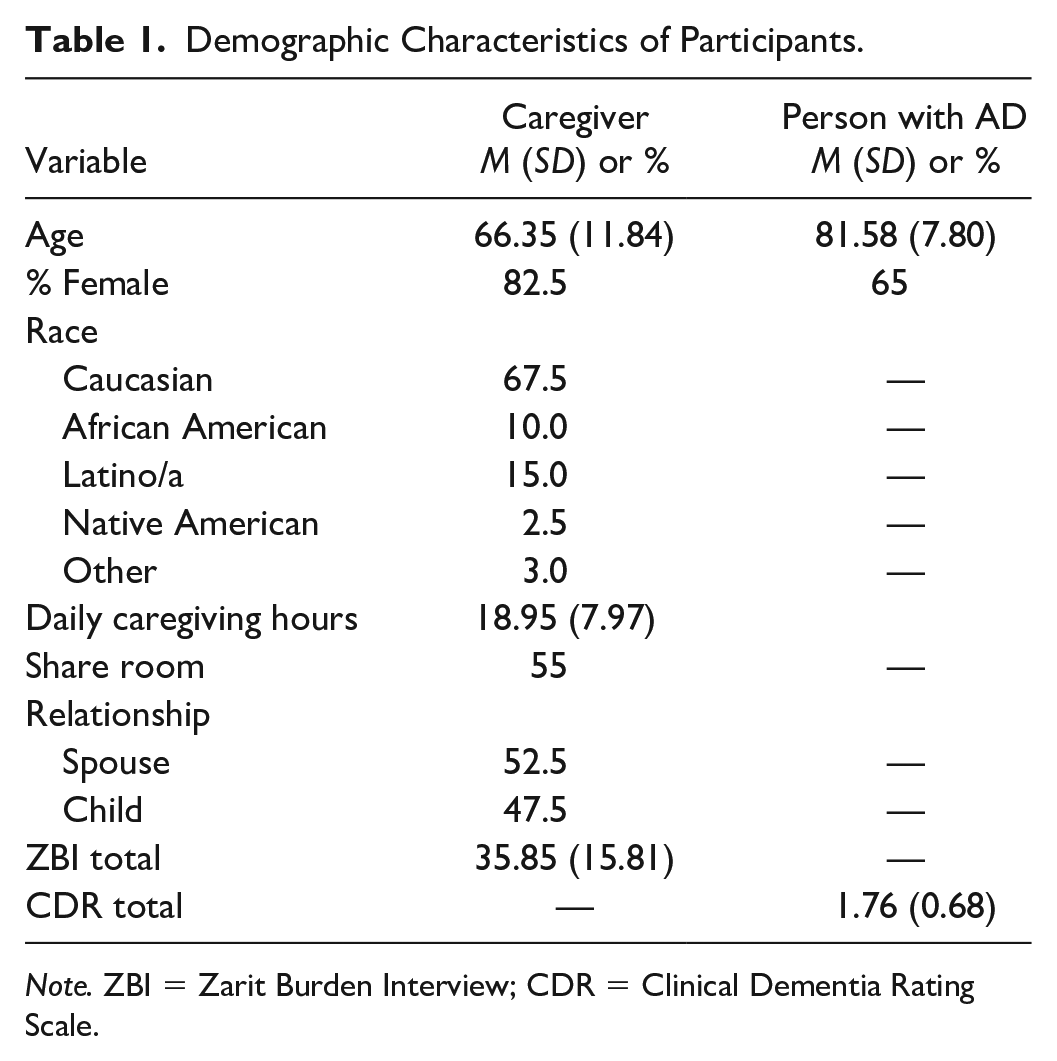
Note. ZBI = Zarit Burden Interview; CDR = Clinical Dementia Rating Scale.
Procedures
Recruitment and screening
After providing verbal consent, caregivers were screened for cognitive impairment using the Telephone Interview for Cognitive Status-Modified (TICS-m; Lines et al., 2003). Caregivers who met inclusion criteria and did not show evidence of cognitive impairment were invited to participate in the study and an initial meeting was scheduled. Study procedures were approved by the University of Massachusetts Amherst Institutional Review Board (Protocol #2009-0237), and all caregivers provided informed consent.
Initial assessment
The caregiver was interviewed about caregiver burden and the severity of symptoms in the person with AD. Caregivers completed self-report measures about their health, depressive symptoms, and overall sleep quality, as well as about neuropsychiatric symptoms (NPS) and activities of daily living for the person with AD.
Diary data collection
Daily diary data were collected for eight consecutive days, beginning the morning following the initial assessment. Caregivers reported on their sleep and the sleep of the person with AD during the previous night during a morning phone call, and reported on their PA and NA, as well as PA and NA for the person with AD, during an evening phone call. Affect was measured in the evening to allow for participants to report average NA and PA over the course of the day.
Screening Measure
Telephone Interview for Cognitive Status—Modified (TICS-m)
The TICS-m is a 13-item telephone interview that assesses language, attention/orientation, and memory (Lines et al., 2003). Higher scores indicate better cognitive functioning. Cut-off scores for cognitive impairment on the TICS-m range from 28 to 34 (e.g., Cook et al., 2009; Knopman et al., 2010; Seo et al., 2011); all caregivers scored 30 or higher on the TICS-m. The TICS-m demonstrated good test–retest reliability across two administrations separated by 15 months in nondemented and demented older adults (Plassman et al., 1994). The TICS-m demonstrates convergent validity because it is significantly correlated (r = .57) with the MMSE, another screening tool for cognitive functioning (de Jager et al., 2003).
Baseline Measures
Clinical Dementia Rating Scale (CDR)
The CDR is a global rating of dementia severity (Hughes et al., 1982). The rating covers six domains of cognitive and functional performance including, memory, orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care. The person with AD is rated on a 5-point scale (0 = healthy, 0.5 = very mild, 1 = mild, 2 = moderate, 3 = severe dementia) with higher values indicating increased severity of dementia (Morris, 1993). The CDR has good interrater reliability of .62 (Rockwood et al., 2000). CDR scores for persons with AD in the current sample ranged from 0.5 to 3, with the majority of caregivers caring for persons with mild (32.5%) to moderate (52.5%) AD.
Zarit Burden Interview (ZBI)
The ZBI is a self-report inventory that measures caregiver burden in the past week (Zarit et al., 1980, 1987). The revised version contains 22 items that assess the degree to which caregivers perceive the responsibilities associated with caregiving to have a negative impact on their health, emotional functioning, finances, and personal and social life (Zarit et al., 1985). Each item is rated for discomfort on a 5-point scale (0 = never; 4 = nearly always); four items are reverse-scored (Zarit et al., 1980). The ZBI has been found to have good internal consistency reliability (α = 0.89; Zarit et al., 1987). The ZBI demonstrates good convergent validity (rs>.6) with measures of caregiver life quality and depression and functional abilities in care recipients (Visser-Meily et al., 2004).
Daily Diary Measures
Sleep measures
The Morin sleep diary (Morin, 1993) was adapted to provide information about sleep patterns for the caregiver and person with AD for the diary study. The Morin sleep diary includes questions about bedtime, wake time, sleep-onset latency, number and duration of awakenings, time of last awakening, naps, medication intake, and overall sleep quality. Caregivers completed sleep diaries upon awakening to increase the accuracy of their recall when they were interviewed in the morning. The independent variables in the sleep diary for the caregiver were bedtime, time of awakening, time to fall asleep (sleep latency), time being awake after sleep onset (WASO—wake after sleep onset), number of times being awakened by the person with AD, sleep quality (1–5, “very poor” to “very good”), and feeling well rested from sleep (1–5, “not at all” to “very much”). Sleep timing variables were used to calculate the total sleep time, TST = (time of awakening—bedtime)—sleep latency—WASO.
The caregiver rated the same items for the person with AD, but with some changes. The caregiver noted sleep period time for the person with AD, (i.e., time of awakening—bedtime), and estimated sleep quality and appearance of being rested for the person with AD.
Positive and Negative Affect Schedule (PANAS)
Each evening, caregivers reported on their affect and the affect of the person with AD using the PANAS, a 20-item mood scale that measures PA and NA (Watson et al., 1988). Items are rated for the past day on a 5-point scale (1 = very slightly or not at all; 5 = extremely). The PA and NA scales are quasi-independent, with correlations ranging from –.12 to –.23 across different time frames (Watson et al., 1988). The PANAS has demonstrated high internal consistency reliability, with .90 for PA and .87 for NA for different today ratings.
Analytic Strategy
Due to the nested structure of the data (i.e., repeated measures at Level 1 nested within individuals at Level 2), we used multilevel structural equation modeling in Mplus version 7 (Muthén & Muthén, 1998–2012) to test our hypotheses. For each model, the a path modeled the association of the focal sleep characteristic of the person with AD with the mediator (i.e., caregiver sleep characteristic or affect in the person with AD), and the b path modeled the association between the mediator and the outcome (i.e., caregiver affect). The key test of mediation—the indirect effect (i.e., a*b paths)—was assessed in each model. Whereas traditional approaches to mediation require that both “a” and “b” pathways be significant to test for a significant indirect effect, newer approaches argue that significance in the “a” and “b” paths is not a prerequisite for mediation (e.g., Hayes, 2009). Multilevel mediation analyses followed the guidelines described by Preacher and colleagues (Preacher et al., 2010). This analytic approach allows for decomposition of the observed data into within- and between-person levels, and for testing for mediational processes at each level of analysis (Figures 1 and 2). Thus, we are able to separately examine whether within-person or between-person variation in sleep in the person with AD is associated with within- and between-person variability in caregiver mood in each model. All variables (i.e., predictors, mediators, and outcomes) were assessed at Level 1, creating 1–1–1 mediation models. Level 1 variables were disaggregated before being entered into the models such that Level 2 values represent person-specific means and Level 1 values represent deviation from those individual means. Confidence intervals for indirect effects were generated using Monte Carlo simulations in Mplus to appropriately test for significance. We used the Benjamini–Hochberg procedure to control for family-wise error for the remaining parameter estimates in mediation models (e.g., a, b, and c’ paths).
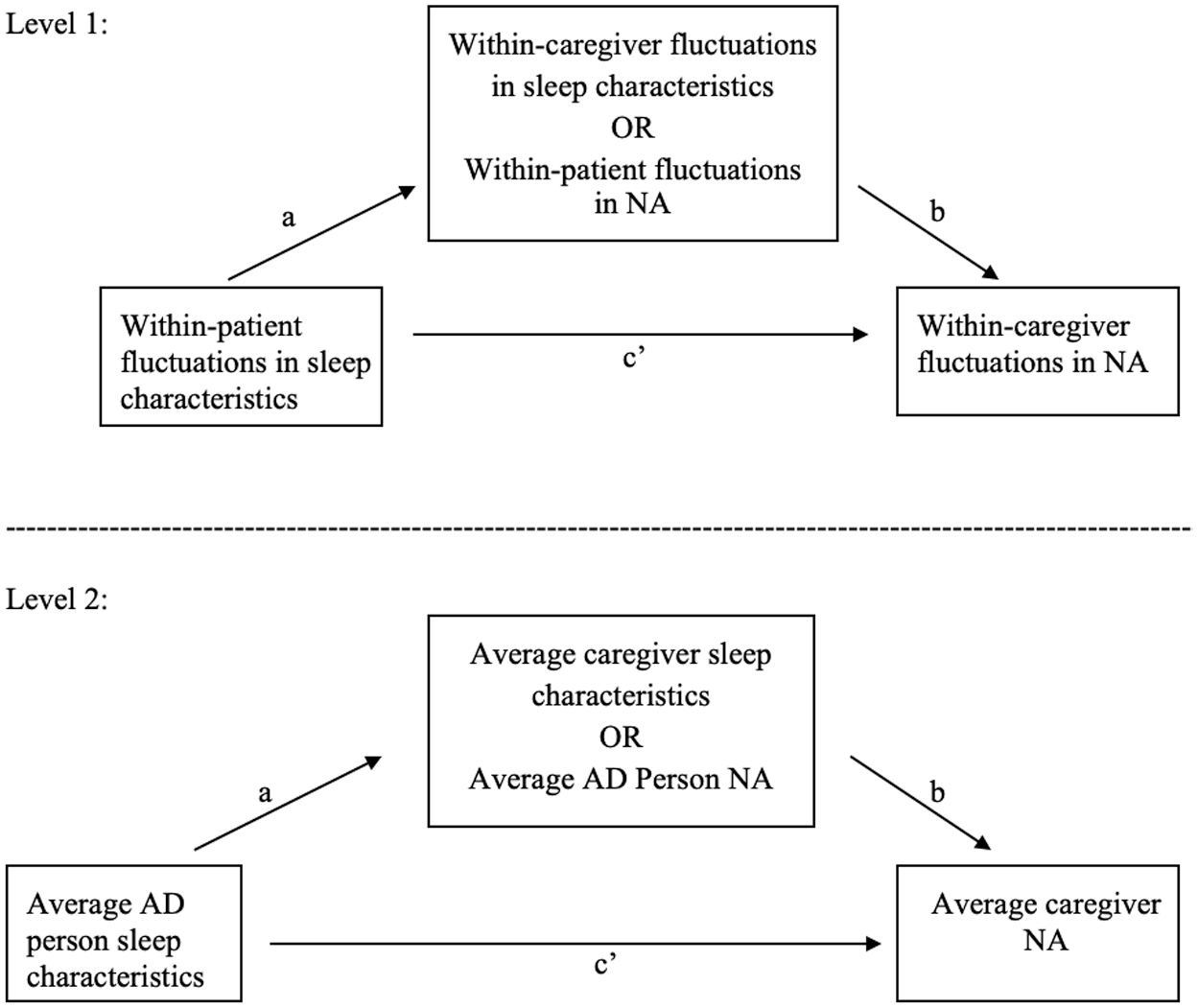
Conceptual model.
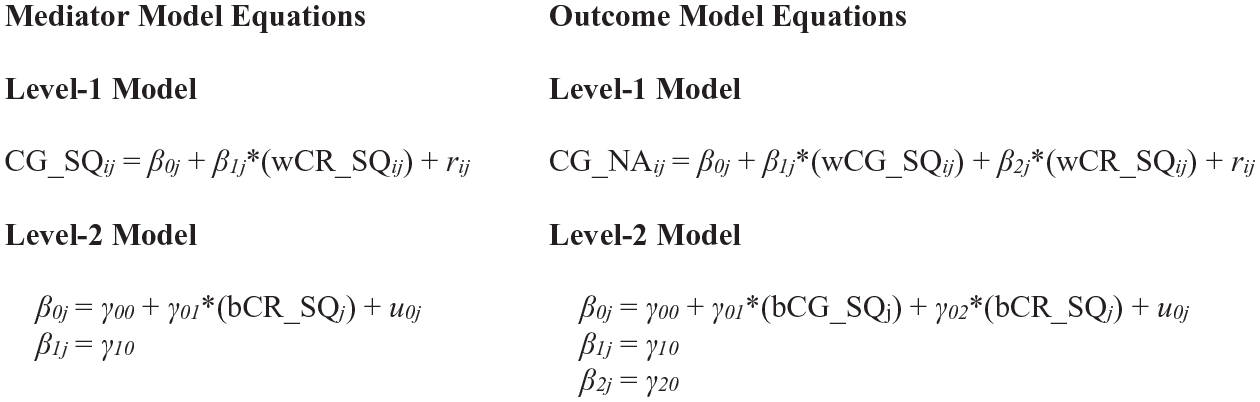
Sample model equations for multilevel mediation analyses.
Results
Descriptive Statistics
Data were aggregated at the between-subject level to provide descriptive statistics for sleep and mood variables (Table 2). There was a trend for caregivers to report better sleep quality in persons with AD than themselves, t(33) = 1.79, p = .082. Caregivers reported greater PA in themselves than in persons with AD, t(33) = 6.93, p < .001; there was not a significant difference in NA for the caregiver and NA in the person with AD, t(33) = −1.52, p = .138. Log-transformed scores for NA in both caregivers and persons with AD were used in Mplus analyses due to substantial positive skew (i.e., skewness >1). Awakenings due to the person with AD were reported by caregivers about half the time, and this variable was dichotomized (i.e., 0 vs ≥1 awakenings).
Descriptive Statistics and Correlations Between Study Variables at the Between-Person Level.
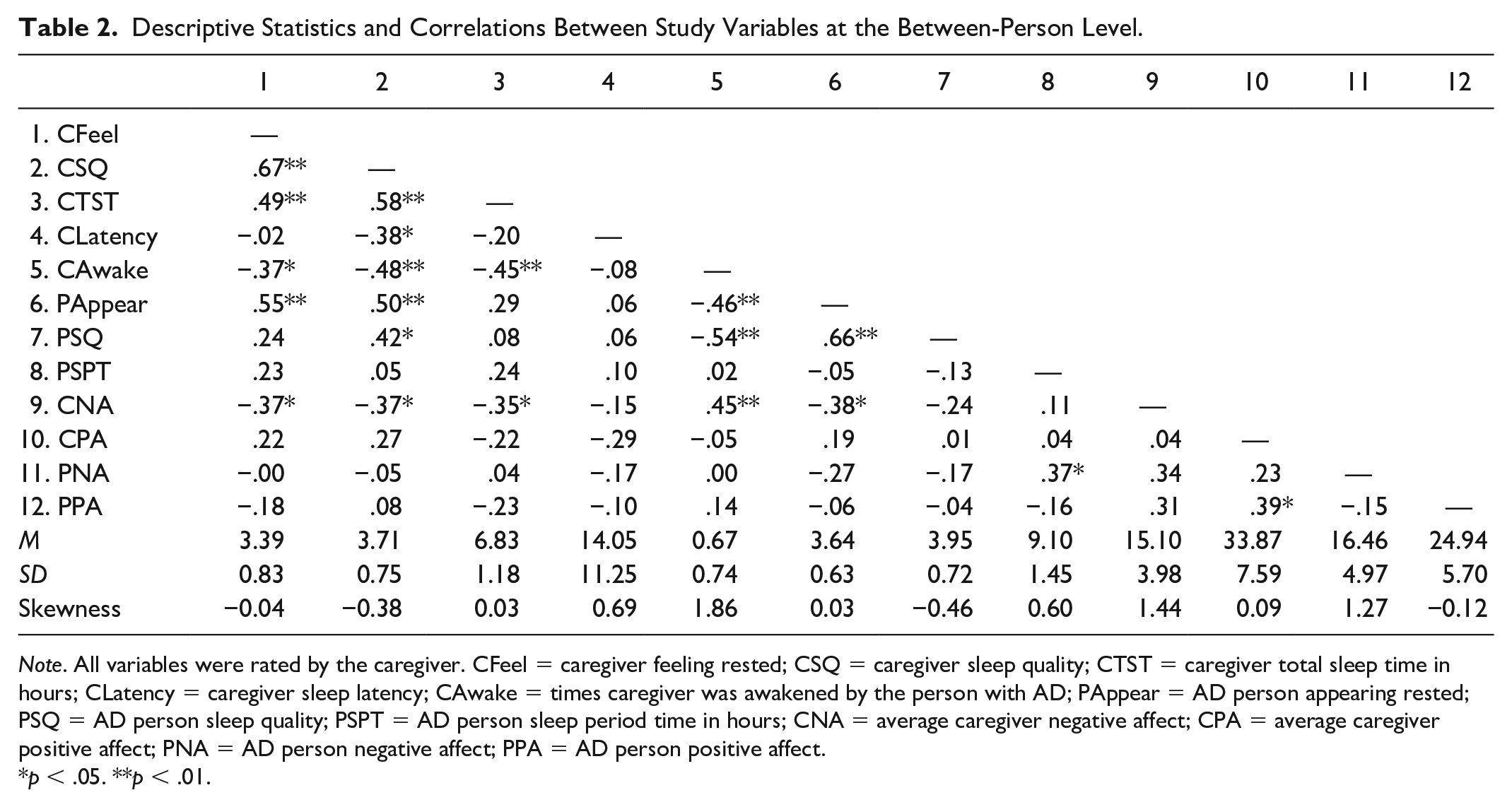
Note. All variables were rated by the caregiver. CFeel = caregiver feeling rested; CSQ = caregiver sleep quality; CTST = caregiver total sleep time in hours; CLatency = caregiver sleep latency; CAwake = times caregiver was awakened by the person with AD; PAppear = AD person appearing rested; PSQ = AD person sleep quality; PSPT = AD person sleep period time in hours; CNA = average caregiver negative affect; CPA = average caregiver positive affect; PNA = AD person negative affect; PPA = AD person positive affect.
p < .05. **p < .01.
Mediational Analysis Results: Impact of AD Person Sleep Variables on Caregiver NA
Due to a high bivariate correlation (r = .66, p < .001) between the person with AD appearing rested and sleep quality in the person with AD, these variables were used as indicators to estimate a latent variable of subjective sleep quality in persons with AD. Similarly, caregiver feeling rested and caregiver sleep quality (r = .67, p < .001) were used to estimate a latent variable of subjective caregiver sleep quality.
Separate mediation models were conducted for each combination of two predictor variables (i.e., latent sleep quality and sleep period time in persons with AD) and five mediator variables (i.e., caregiver sleep quality, caregiver total sleep time, number of times caregiver was awakened by the person with AD, and affect in the person with AD), resulting in 10 models predicting caregiver NA (Table 3).
Results of Mediation Analyses Predicting Caregiver Negative Affect.
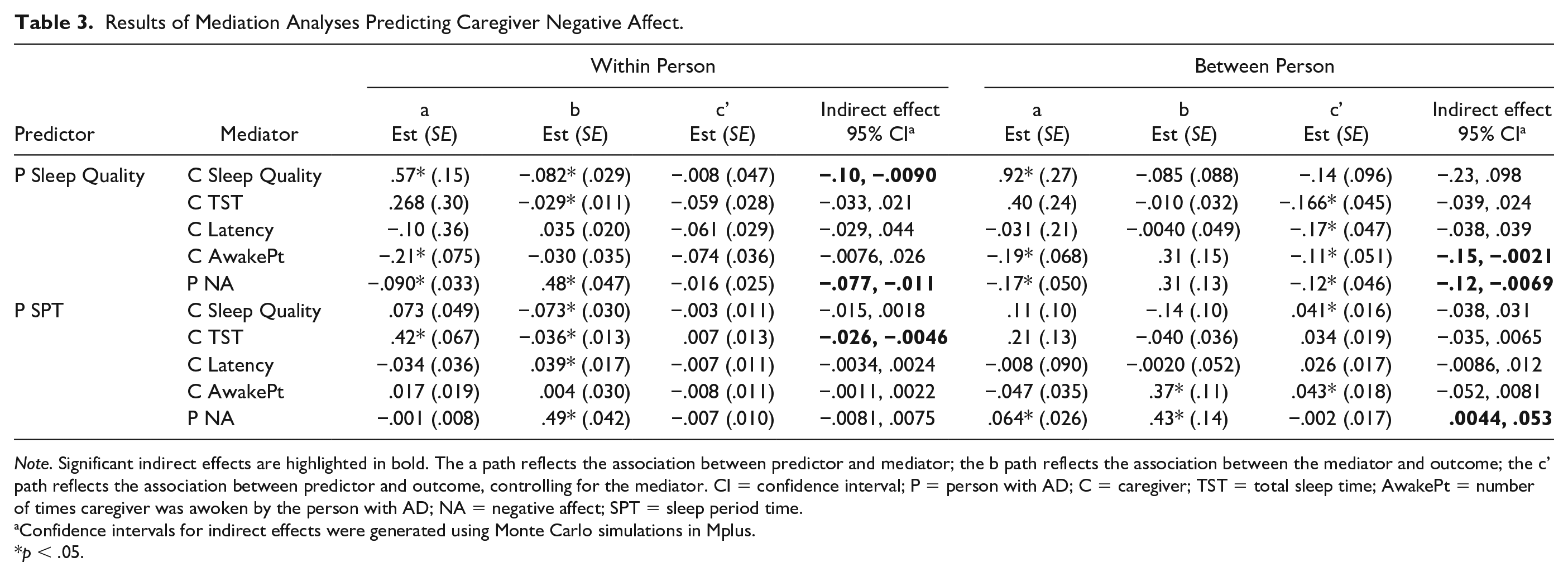
Note. Significant indirect effects are highlighted in bold. The a path reflects the association between predictor and mediator; the b path reflects the association between the mediator and outcome; the c’ path reflects the association between predictor and outcome, controlling for the mediator. CI = confidence interval; P = person with AD; C = caregiver; TST = total sleep time; AwakePt = number of times caregiver was awoken by the person with AD; NA = negative affect; SPT = sleep period time.
Confidence intervals for indirect effects were generated using Monte Carlo simulations in Mplus.
p < .05.
Within-person mediation
Consistent with expectations, there was evidence of several significant within-person mediational processes predicting caregiver NA from patient sleep variables. Poorer sleep quality in persons with AD relative to their person-specific average was associated with poorer sleep quality in caregivers relative to their person-specific average, which was in turn associated with greater caregiver NA. Caregiver sleep quality mediated the relationship between sleep quality in persons with AD and caregiver affect at Level 1 (indirect effect = −0.047, SE = 0.024, 95% CI = −0.10, −0.009). Similarly, poorer sleep quality than usual in persons with AD was associated with greater than usual NA in persons with AD, which was in turn associated with greater caregiver NA. NA in persons with AD mediated the relationship between sleep quality in persons with AD and caregiver NA (indirect effect = −0.043, SE = 0.016, 95% CI = −0.077, −0.011). Caregiver total sleep time mediated the association between sleep period time in persons with AD and caregiver NA at the within-person level (indirect effect = −0.015, SE = 0.005, 95% CI = −0.026, −0.0046). That is, greater sleep period time in persons with AD relative to their person-specific average predicted greater total sleep time in caregivers relative to their person-specific average, which in turn predicted lower NA in caregivers.
Between-person mediation
There were several significant between-person mediational processes predicting caregiver NA from sleep variables in persons with AD. Whether caregivers were awoken during the night by the person with AD mediated the association between patient sleep quality and caregiver NA (indirect effect = −0.059, SE = 0.038, 95% CI = −0.15, −0.0021). That is, greater sleep quality on average in persons with AD was associated with lower likelihood of persons with AD awakening caregivers during the night, which in turn was associated with lower caregiver NA on average. Persons with AD that had greater than average sleep quality tended to have lower than average NA, which was associated with lower than average caregiver NA; average NA in persons with AD mediated the relationship between sleep quality in persons with AD and caregiver NA (indirect effect = −0.053, SE = 0.025, 95% CI = −0.12, −0.0069). NA in persons with AD significantly mediated the association between sleep period time in persons with AD and caregiver NA (indirect effect = 0.027, SE = 0.012, 95% CI = 0.0044, 0.053); counter to expectations, persons with AD that had higher than average sleep period time also tended to have higher NA, which was in turn associated with greater caregiver NA. No other mediational processes were found to be statistically significant.
Mediational Analysis Results: Impact of AD Person Sleep Variables on Caregiver PA
As above, mediation models were conducted for each combination of two predictor and five mediator variables, resulting in 10 models predicting caregiver PA (Table 4). At the within-person level, as expected, poorer subjective sleep quality than usual in the persons with AD predicted poorer subjective sleep quality than usual in the caregiver, which in turn predicted lower caregiver PA; caregiver sleep quality mediated the association between sleep quality in persons with AD and caregiver PA (indirect effect = 0.097, SE = 0.043, 95% CI = 0.025, 0.20). Greater sleep period time than usual in persons with AD predicted greater caregiver total sleep time than usual, which in turn predicted greater caregiver PA. Greater sleep time in persons with AD was associated with greater caregiver PA via greater caregiver sleep time (indirect effect = 0.027, SE = 0.012, 95% CI = 0.0032, 0.053). There were no statistically significant mediational processes at the between-person level.
Results of Mediation Analyses Predicting Caregiver Positive Affect.
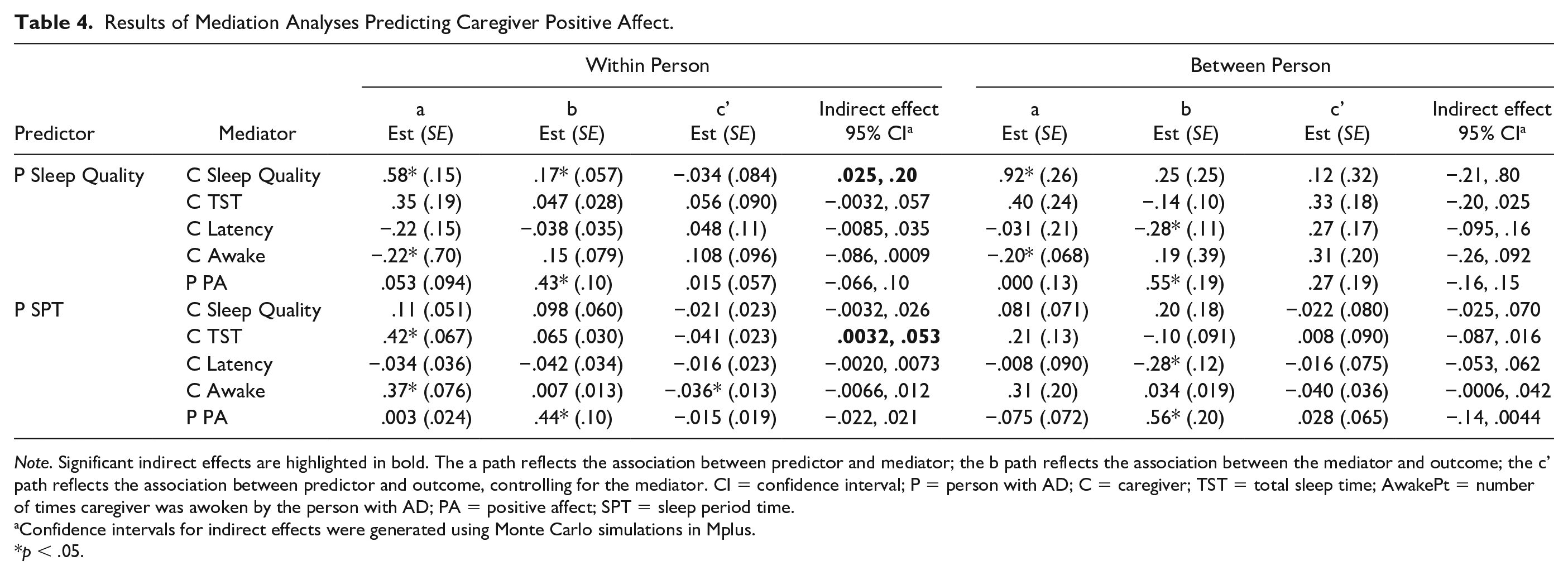
Note. Significant indirect effects are highlighted in bold. The a path reflects the association between predictor and mediator; the b path reflects the association between the mediator and outcome; the c’ path reflects the association between predictor and outcome, controlling for the mediator. CI = confidence interval; P = person with AD; C = caregiver; TST = total sleep time; AwakePt = number of times caregiver was awoken by the person with AD; PA = positive affect; SPT = sleep period time.
Confidence intervals for indirect effects were generated using Monte Carlo simulations in Mplus.
p < .05.
Discussion
Family members provide the majority of care for persons with AD (Friedman et al., 2015). Improving sleep and affect in caregivers would benefit the caregiver, improve the caregiving process, and may prolong the time that a person with AD can live at home (Ooms & Ju, 2016). This study demonstrated several mechanisms by which daily sleep characteristics of persons with AD affect caregiver sleep and affect.
As hypothesized, daily sleep characteristics of the person with AD influenced daily caregiver affect, and this association was partially due to caregiver sleep behaviors. On days that caregivers reported poorer sleep quality in persons with AD, they self-reported poorer sleep quality, greater NA, and lower PA. Similarly, on days that persons with AD were in bed for longer, caregivers reported getting more sleep, and self-reported less NA and greater PA. These results are consistent with findings of retrospective associations between sleep in persons with AD and NA outcomes in caregivers (Arthur et al., 2018; Mausbach et al., 2013; Mohamed et al., 2010). Although previous studies have outlined associations between daily fluctuation in caregiver sleep and mood (Liu et al., 2015; McCrae et al., 2016), the current results further detail the associations between sleep characteristics of the person with AD and caregiver outcomes. That is, results provide evidence for an indirect pathway linking fluctuations in sleep disturbance in caregivers and care recipients to fluctuations in caregiver mood.
Our data are unique in including assessment of PA in the person with AD and caregiver. Lower caregiver PA was associated with poorer sleep on the preceding night for the person with AD. PA supports recovery from negative emotions (Fredrickson et al., 2000) and can serve as a protective factor in times of stress (Ong et al., 2006). Thus, it is important to bolster, protect, and sustain PA in family caregivers.
Furthermore, at the between-person level, whether caregivers experience PA on a given day is more strongly associated with whether they and their care recipient slept well the night before than with whether they and their care recipient sleep well in general. This pattern is consistent with prior studies that have highlighted the importance of irregularity in sleep in persons with AD and their caregivers as a predictor of poor caregiver mood (e.g., Liu et al., 2015).
Also at the between-person level, there were two findings relevant to daily NA in caregivers. First, persons with AD with greater than average sleep quality were less likely to wake the caregiver during the night, which was associated with lower average caregiver NA. Second, persons with AD who were perceived by caregivers to have better sleep quality and who spent more time in bed displayed lower levels of NA on average, which was in turn associated with lower average caregiver NA. Thus, there are several pathways from patient sleep disturbance to caregiver NA. Our findings are consistent with retrospective associations between poorer sleep and worse mood in healthy adult populations (Alcántara et al., 2016; Cho et al., 2008; Lee et al., 2013) but illustrate the importance of prospective daily diary data to identify which aspects of patient sleep—notably sleep quality and sleep quantity—might be most important for caregiver outcomes.
Limitations
All ratings of sleep and affect were provided by the caregiver. Findings reflect associations between caregiver perceptions of AD person sleep and affect and caregiver outcomes, and it is possible that caregiver mood on any giving day influenced ratings of care recipient mood. In addition, there is common method variance in predictor and outcome variables. These limitations are mitigated somewhat by the fact that the influence of common method variance is reduced in repeated-measures designs (Podsakoff et al., 2003) and that caregivers reported sleep in the morning and affect in the evening which reduces shared rater bias.
Our assessment of disturbed sleep is based on subjective information (American Academy of Sleep Medicine, 2005), which is common in clinical studies (Edinger et al., 2004). Subjective and objective sleep measures are typically not correlated (Rosa & Bonnet, 2000) and provide unique data about sleep quality and other variables. Thus, these results may not generalize to objective measures of sleep, such as polysomnography and actigraphy.
The study included a sample of convenience, comprised of caregivers who were willing and able to participate in an 8-day diary study. The majority of the caregivers were recruited through caregiver support groups (Mittelman et al., 2006). The current sample may be higher functioning and better supported than other samples of caregivers of persons with AD with regard to sleep and mood.
NPS are common in AD and may contribute to caregiver mood and sleep difficulties (e.g., Shin et al., 2005). We did not control for potential associations between NPS and caregiver ratings of mood and sleep and thus cannot exclude NPS as an alternate explanation for the association between sleep difficulties in persons with AD and caregiver mood.
Finally, the study sample size was small, which may affect the reliability of parameter estimates (McNeish, 2017). However, the use of Monte Carlo simulations to generate confidence intervals for estimates of indirect effects improves the reliability of the outcomes of interest (i.e., indirect effects). The small sample size also limited our ability to investigate moderator variables (e.g., age, sex, room sharing) in the current analyses.
Treatment Implications
Interventions to improve sleep quality and quantity in persons with AD might have stronger effects on NA than PA for the person with AD but beneficial effects on NA and PA for the caregivers. At medical visits, practitioners might learn more valuable information about sleep and mood in the patient–caregiver dyad by focusing on daily fluctuations in sleep, rather than on global judgments of sleep quality or behaviors. For some patient–caregiver dyads, interventions might be implemented to improve patient sleep, such as implementing daily exercise and increasing sleep hygiene (Irish et al., 2015). For other dyads, aspects of disturbed sleep may be unavoidable (e.g., being frequently awakened by the person with AD). In these cases, respite care might be needed to provide the caregiver opportunities for periodic uninterrupted sleep.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
This study was approved by the University of Massachusetts Amherst Institutional Review Board (Protocol #2009-0237).