
Abstract
Global positioning system (GPS) technology has been increasingly used in aging research as a tool for reliably capturing the level and patterns of mobility among older adults. This article aims to systematically review the current state of GPS-based mobility research with community-dwelling older adults. Twenty-nine studies from 2008 to 2019 are included. Included studies examined various forms of temporal and spatial mobility measures. This review provides a synthesis of the current evidence on the risk factors or correlates of GPS-driven mobility limitations, such as demographic, cognitive, physical, psychological, and environmental factors. There is variability in types of GPS technology and GPS-derived mobility measures, GPS recording methods, data processing, and correlates of mobility limitation across studies. Future research should focus on identifying meaningful GPS-derived mobility measures and developing standardized protocols for GPS administration and data analytics for comparison across studies.
Introduction
Maintaining mobility is significant for well-being and quality of life among older adults. Mobility limitation has been understood as a functional limitation or disability, such as perceived difficulty carrying out daily activities or inability to perform tasks requiring lower extremity function (Chung et al., 2015). Based on this conceptualization, most research on older adults’ mobility depends largely on a limited set of self-report or performance-based measures. Recently, life-space mobility (LSM), focusing on the size and pattern of the spatial area of movements, has been receiving increasing attention (Peel et al., 2005) because it reflects an individual’s “purposeful movement through the environment from one place to another” (Stalvey et al., 1999, p. 460). These measures, however, are applied sporadically, mostly during clinic visits or in a laboratory context. The infrequent measurements of mobility parameters based on the current practice do not provide a comprehensive view of older adults’ mobility. Given that mobility declines variably over time, there is a need for adopting a new method that can be applied continuously or frequently to measure mobility comprehensively and to potentially detect a change that signals deteriorating health.
Global positioning system (GPS) technologies are increasingly used in aging research to objectively measure the current state of older adults’ mobility. Recent advances in GPS technology and data analytics enable a more precise estimation of changes in mobility performance (e.g., distance, gait speed, and time away from home) and a quantification of geographic range as a measure of mobility (Boissy et al., 2018; Thierry et al., 2013). In addition, the technology has the potential to capture daily movement patterns of older adults interacting with environments (Fillekes, Giannouli, et al., 2019). GPS technology is now incorporated into wearable systems or mobile devices, such as smartphones or GPS watches. Mobility research in older adults will benefit from the use of GPS-based wearable technology that provides the key to reliably capturing the level and pattern of mobility and early detection of mobility changes.
Although GPS technology-based characterization of mobility has been the object of investigation in gerontology, reviews to date included older adults with dementia only (Herrera, 2017), focused on the relationship between physical activity and the environment (Krenn et al., 2011), or selected a small set of studies to develop a conceptual classification of GPS-based mobility indicators (Fillekes, Giannouli, et al., 2019). To our knowledge, there is no systematic review that has examined the current state of GPS-based mobility measures and correlates of GPS-derived mobility limitations among older adults. In an attempt to fill existing gaps in the literature and to provide an update on GPS-based mobility indicators in older adults, we conducted a systematic review of published studies. We focused on community-dwelling older adults because they are likely to be healthier and more active than those in other settings (e.g., nursing home) and thus there is lack of studies using GPS in those environments. The current review aimed to (a) synthesize the types of GPS technologies and approaches for using GPS for measuring mobility among older adults, (b) identify and classify GPS-derived mobility measures and correlates of mobility limitation, and (c) make recommendations for future studies.
Method
Electronic Search
We conducted a systematic search for published English language literature. The databases searched were PubMed, Embase, Cumulated Index to Nursing and Allied Health Literature (CINAHL), Web of Science, IEEE Xplore, and Academic Search Complete (EBSCO). We searched these databases from inception through December 12, 2018. The search utilized a combination of keywords and controlled vocabulary for the concepts, “location tracking” and “older adults,” which was adapted to each database (Online Appendix 1). We included studies if the article (a) used any type of location tracking technology to measure mobility, (b) focused on community-dwelling adults (average age ≥ 60 years), (c) measured mobility in natural environments, (d) quantified GPS-derived mobility measures, and (e) was peer-reviewed. Exclusion criteria included studies that (a) did not have a primary focus on mobility (e.g., usability testing), or (b) included both young and older adults but did not provide separate mobility data for older adults. A total of 4,897 articles were found, with 2,578 left to review after deduplication.
Study Selection Process
All references were uploaded to reference management software and duplicates were removed. Two researchers (J.C. and L.S.) conducted the title and abstract review independently, applying the inclusion and exclusion criteria. During title and abstract review, 2,516 publications were excluded, thus decreasing the total to 62. We retrieved full-text articles for these 62 publications for further evaluation. After full-text review, 35 articles were further excluded leaving 27 articles for inclusion in the final review. We identified one additional publication from a hand search of reference lists of retrieved articles. One more article just prior to completion of the review was included, for a final total of 29 articles. Our intention was to identify all studies using any type of location tracking technology (e.g., GLONASS), but a final set of articles focused only on GPS technology.
Data Extraction and Study Synthesis
Data extraction was conducted by the first author who reviewed full texts of the relevant articles using a data extraction spreadsheet. We extracted the following information: title, abstract, a parent study if there was any, study design, sample characteristics and size, inclusion/exclusion criteria, GPS technology type, technology use methods, GPS-based mobility measures and mobility status, factors identified as having a significant relationship with GPS-derived mobility level, and attrition rate. The results were summarized in both text and tabular forms. The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) diagram (Moher et al., 2009) fully shows the literature identification and screening process (Figure 1).

PRISMA diagram showing the systematic process of identifying relevant literature.
The quality scoring of each article was conducted using the criteria adapted from Krenn et al. (2011) and Cetateanu and Jones (2016). We included eight indicators deemed important (Online Appendix 2). The possible range of quality scores is from 0 to 8. The quality assessment was conducted by the first author. To ensure reliability of the assessment, the second author independently scored a random subset of articles. Differences in scoring were discussed and reconciled, and another author (D.W.) checked any unresolved discrepancies.
Categorization of GPS-Based Mobility Measures
We classified GPS-derived mobility measures based on the classification framework for mobility indicators (Fillekes, Giannouli, et al., 2019). It is a comprehensive model, based on a concept of daily mobility, defined as “the everyday spatiotemporal patterns of an individual’s movement in their environment” (p. 2), expanding the LSM concept. The model illustrates different aspects of mobility, such as the semantic (actual content of a mobility indicator, including space, time, movement scope, and attribute) and analytical (data processing and analytical properties) characteristics of GPS-based mobility constructs. Specifically, we applied the framework definitions of spatial and temporal mobility indicators and examined the movement mode in each study.
Results
Study Characteristics
Included studies were published between 2008 and 2019 (Table 1). The SenTra Study provided data for 10 publications. Twenty-eight studies used a cross-sectional study design; among them, two studies used mixed-methods study design (Zandieh, Flacke, et al., 2017; Zeitler & Buys, 2015) and one study additionally examined mobility changes over time (Wettstein, Seidl, et al., 2014). Most studies enrolled relatively independent older adults. Exceptions to this were Harada et al. (2017, 2018) and Tung et al. (2014), which included older adults with cognitive impairment only. Eight studies reported an attrition rate or the proportion of invalid GPS data: 28% (Boissy et al., 2018), 25.5% (Kaspar et al., 2015), 19.9% (Zandieh, Flacke, et al., 2017; Zandieh, Martinez, et al., 2017), 17% (Giannouli et al., 2018), 6.7% (Hirsch et al., 2014), 6% (Kerr et al., 2012), and 4% (Theou et al., 2012).
Characteristics of Included Studies, GPS Technology, and Quality Assessment Score.
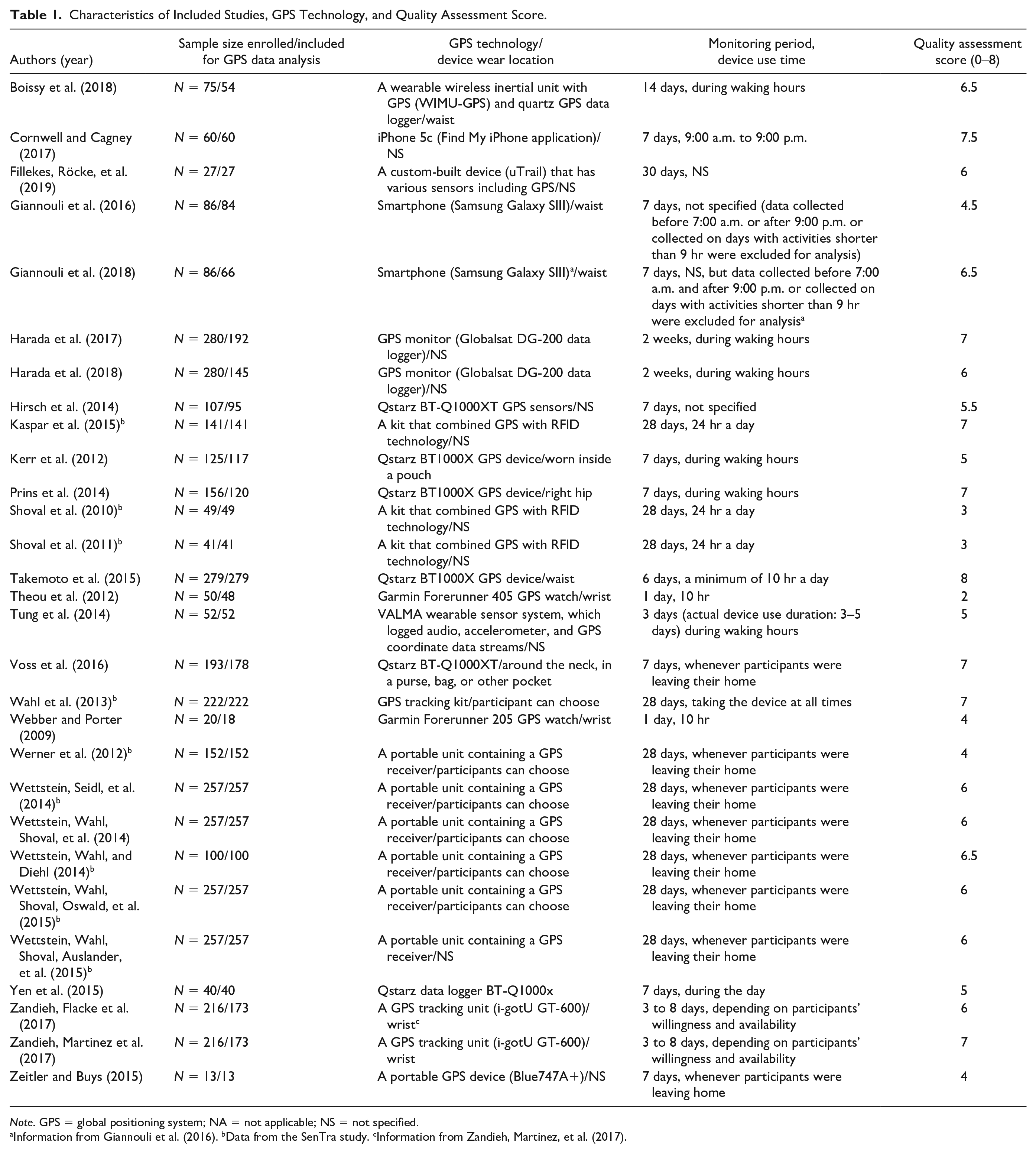
Note. GPS = global positioning system; NA = not applicable; NS = not specified.
Information from Giannouli et al. (2016). bData from the SenTra study. cInformation from Zandieh, Martinez, et al. (2017).
Quality of Studies
The total quality score ranged from 2 to 8 (Table 1). Eighteen studies were situated in the upper third of the scale (6–8), 10 studies were in the middle third (3–5.5), and one study was in the lower third (0–2.5). Overall, most studies can be regarded as being of moderate to high quality from the perspective of this review.
GPS Tracking Method for Measuring Mobility
Three types of GPS devices were identified as a mobility measurement tool: GPS data loggers, smartphones, and GPS watches. We found a trend that smartphone has been adopted in recent publications. The GPS recording period ranged from 1 to 30 days. The daily GPS device use time varied greatly from 10 to 24 hr a day.
GPS-Derived Mobility Measures
Online Appendix 3 shows the classification of identified GPS-derived mobility measures and movement modes. The spatial aspect of mobility is based on the spatial distribution of the GPS data, such as the size of the movement, or frequency of mobility-related events, whereas the temporal aspect of mobility reflects the time or duration of mobility behaviors, or movement speed (Fillekes, Giannouli, et al., 2019).
Spatial mobility measures
The spatial aspect of mobility was examined in 25 studies. Spatial measures are grouped into four categories. The most frequently used indicator was the distance moved. Various forms of distances were examined, including maximum or average distance from home, distance in vehicles, distance walked, total distance moved, maximum action-range defined as the largest straight-line distance away from home, ellipse maximum distance, and trip length for grocery shopping. The number of mobility-related behaviors was examined using different indicators, including the number of walking tracts, number of total trips, number of trips walked or cycled to get groceries, or number of vehicle trips. Similarly, the number of visited places was calculated in eight studies. The spatial size of the mobility-related events was computed using different indicators, such as ellipse area, perimeter based on a convex hull, daily path area calculated by buffering all of an individual’s trips by 200 m, area based on minimum convex polygon, and life space ranging from Level 1 (home/garden) to Level 6 (area beyond German-speaking municipalities of Switzerland). Three studies used a spatial measure indexed by time, including distances from home by hour of the day (Shoval et al., 2011), number of walking tracks by hour of the day and by day of the week (Shoval et al., 2010), and walking distance during the weekends and weekdays (Kaspar et al., 2015).
Temporal mobility measures
Temporal indicators of mobility were assessed in 24 studies. The most commonly measured parameter was the duration of mobility-related events (e.g., walking duration, time at home, and outdoor time). Interestingly, one study examined a duration for trips made for grocery shopping as it reflects daily mobility behaviors in older adults (Prins et al., 2014). In addition, movement or gait speed was measured in eight studies.
Travel modes
Thirteen studies examined different travel modes. Three studies examined a walking mode only (Kerr et al., 2012; Zandieh, Flacke, et al., 2017; Zandieh, Martinez, et al., 2017), whereas Zeitler and Buys (2015) quantified two different types of motorized modes (car and public transportations).
GPS-Based Mobility Status
The majority of the studies reported GPS-derived mobility status data of study participants (Online Appendix 3). There was variation in the temporal aggregation of the GPS data (e.g., daily average or an average for the whole monitoring duration) and the level of mobility.
Factors Associated With GPS-Based Mobility Levels
The majority of the studies identified factors that are associated with older adults’ mobility levels captured by GPS technology (Online Appendix 3).
Demographic factors
Eight studies reported the relationship between age and the level of GPS-measured mobility. People in the older age group spent most of their time closer to home and used the morning hours for out-of-home trips compared with people in the younger group (Shoval et al., 2011). Age was significantly, negatively correlated with outdoor time (Harada et al., 2017), numbers of trips during the winter but not the summer (Yen et al., 2015), the number of places visited and outdoor time (Wahl et al., 2013; Wettstein, Wahl, & Diehl, 2014), and life spaces (Hirsch et al., 2014). The mobility-restricted group was significantly older than the outdoor-oriented cluster and the walkers cluster (Wettstein, Wahl, Shoval, Auslander, et al., 2015). On the contrary, the relationship between age and mobility levels differed by travel mode: the trips cycled by those aged 75 years and older were shorter than for those aged 65 to 74 years, whereas the relationship was reversed for walking distances (Prins et al., 2014).
Females had reduced levels of mobility in terms of outdoor time (Shoval et al., 2011; Wahl et al., 2013), number of visited places (Wahl et al., 2013), and mean distances from home (Shoval et al., 2011; Wettstein, Wahl, & Diehl, 2014). More women than men tended to belong to the mobility-restricted group rather than the outdoor-oriented or walkers groups (Wettstein, Wahl, Shoval, Auslander, et al., 2015). In Shoval et al.’s (2010) study, males were likely to be more active outside during the first half of the day, whereas females were likely to be more active outside their homes during the second part of the day. In contrast, females showed higher levels of area and perimeter based on a convex hull than males (Tung et al., 2014).
Living situation is also associated with GPS-based mobility levels. Those living alone made significantly fewer trips, traveled shorter distances in vehicles, and spent less time in vehicles (Boissy et al., 2018). Individuals living alone, divorced, or widowed were likely to belong to the mobility-restricted group (Wettstein, Wahl, Shoval, Auslander, et al., 2015). Older adults who were single were more likely to take shorter walking trips (Zandieh, Martinez, et al., 2017). However, having more household members had a significant, negative association with outdoor time and the number of visited nodes (Wahl et al., 2013).
Other demographic factors identified include driver’s license and vehicle access, retirement, education, race/ethnicity, and income. Older adults with valid driver’s license and vehicle access had larger activity spaces (Hirsch et al., 2014). Older adults without vehicle access showed significantly fewer trips, traveled shorter distances in vehicles, and spent less time in vehicles, and retired individuals moved shorter distances in vehicles, spent less time in vehicles, and had a smaller ellipse area and shorter ellipse maximum distance (Boissy et al., 2018). Wettstein, Wahl, and Diehl (2014) reported that fewer years of education were related to longer outdoor time, while educational attainment was independently related to outdoor walking durations (Zandieh, Martinez, et al., 2017). Cornwell and Cagney (2017) found a difference in mobility levels by race/ethnicity, where Hispanic participants visited fewer tracts (including both residential and nonresidential tracts) than non-Hispanic White respondents (p < .10). Low-income older adults had a significantly greater proportion of in-home time, traveled a shorter distance, spent less time in vehicles, and had smaller ellipse areas and ellipse maximum distance compared with those with higher income (Boissy et al., 2018).
Cognitive function
Nine studies found that cognitive function is related to mobility outcomes. Cognitively impaired older adults spent less time on foot (Boissy et al., 2018) or out of home (Wettstein, Seidl, et al., 2014), traveled shorter distances (Shoval et al., 2010, 2011), and visited fewer places (Wettstein, Seidl, et al., 2014; Wettstein, Wahl, Shoval, Oswald, et al., 2015) than those without cognitive decline. Dementia patients demonstrated smaller life spaces (area, perimeter, and mean distance) compared with those without cognitive impairment (Tung et al., 2014). In a cluster-analysis study (Wettstein, Wahl, Shoval, Auslander, et al., 2015), older adults with cognitive impairment were likely to belong to the mobility-restricted group rather than the outdoor-oriented or walkers groups. Significant relationships were found between two mobility indicators (time out of home and the number of visited places) and cognitive function (Wahl et al., 2013). Two studies quantified the relationship between specific cognitive function indicators and mobility outcomes. A composite mobility measure, consisting of three GPS-based parameters and one motion sensor-based parameter (active and gait time), was correlated with two planning ability measures and two visuospatial attention measures, but not with spatial working memory measures (Giannouli et al., 2018). Episodic memory was significantly, positively related to outdoor time, the number of visited nodes, mean distance from home, and maximal distance from home, while mean distances from home were greater for persons with worse executive function (Wettstein, Wahl, & Diehl, 2014).
Physical function
Nine studies identified physical factors in relation to mobility limitations. Changes in outdoor time from baseline to follow-up were significantly associated with changes in the total distance walked in 6 min and times spent for chair stand test in cognitively impaired older adults (Harada et al., 2018). Outdoor time was significantly correlated with steps-per-day and cardiorespiratory fitness (Harada et al., 2017). Older adults who spent 30 min or more outdoors reported higher physical functioning (Kerr et al., 2012). Older adults reporting functional limitations walked and cycled shorter distances than those without limitations (Prins et al., 2014). Slower gait speed and dependency in activities of daily living were significantly associated with restricted convex hull area and perimeter (Tung et al., 2014). Takemoto et al. (2015) reported that the daily number of distances traveled and minutes of pedestrian trips had a significant relationship with the ability to perform the Short Physical Performance Battery and 400-m walk test. Better physical functioning, measured by the 36-item Short Form, was associated with greater walking distances and longer walking durations (Wettstein, Wahl, & Diehl, 2014). Being physically active was associated with being a member of the walkers group rather than the mobility-restricted group (Wettstein, Wahl, Shoval, Auslander, et al., 2015). In regression analysis to evaluate the predictive ability of three physical performance measures for each of the real-life mobility measures (life-space size, mean action-range, and maximum action-range), stride length was the only significant predictor of all real-life measures, whereas stride velocity and cadence were not predictive (Giannouli et al., 2016).
Other physical correlates of mobility limitations include pain, self-reported health, and frailty. Pain interference had a significant negative relationship with the daily number of distances traveled and minutes of pedestrian trips (Takemoto et al., 2015). The walkers group reported better subjective health than the mobility-restricted group (Wettstein, Wahl, Shoval, Auslander, et al., 2015). In Theou et al.’s (2012) study, GPS-based movement speed was correlated with frailty. They also reported that GPS-based outdoor activity minutes, distance, and speed were not significantly different across three frailty categories, but that a trend was found that older adults with lower levels of frailty spent more time in outdoor activities, had greater distances traveled, and had a faster movement speed compared with older adults with intermediate or high levels of frailty.
Psychological factors
Older adults spending more than 30 min outdoors (not including vehicle time) reported fewer depressive symptoms and less fear of falling than those who do not (Kerr et al., 2012). Outdoor time was significantly, negatively correlated with depression (Harada et al., 2017) and bad mood (Kaspar et al., 2015). The daily number of and daily distances traveled in pedestrian trips had a significant negative relationship with fear of falling and depression, and that the daily pedestrian trip time and the daily number of vehicle trips were significantly, negatively related to fear of falling (Takemoto et al., 2015). Apathy and depression were negatively correlated with the life-space area and perimeter (Tung et al., 2014). Depression had significant correlations with outdoor time in cognitively healthy older adults and all older adults including those with no cognitive impairment and mild cognitive impairment (MCI; Wahl et al., 2013). Life satisfaction was significantly associated with outdoor time. More depressed people spent less time out of home (Wettstein, Wahl, & Diehl, 2014). The outdoor-oriented group reported significantly higher outdoor motivation than the mobility-restricted or walkers group (Wettstein, Wahl, Shoval, Auslander, et al., 2015). In a study with three groups of older adults (no cognitive impairment, MCI, and dementia), a composite measure of out-of-home walking (distance, speed, and duration) was positively related to environmental mastery, and a global mobility measure (outdoor time and number of visited places) was a significant positive factor of positive affect in persons with dementia (Wettstein, Wahl, Shoval, et al., 2014).
Social and built environmental factors
People who had physical support to go outside of their homes showed larger activity spaces (Hirsch et al., 2014). There were negative correlations between caregiving burden and three mobility indicators of dementia patients (time spent walking per day, the number of visited places, and number of walking tracks per day; Werner et al., 2012). Three studies found that neighborhood characteristics are related to mobility. Older adults living in less walkable neighborhoods had larger activity spaces measured as standard deviation ellipse (p = .02), minimum convex polygon (p = .01), and daily path area (p = .01; Hirsch et al., 2014). Older adults living in high-deprivation areas spent significantly fewer hours walking outside the home than those in low-deprivation areas (Zandieh, Flacke, et al., 2017; Zandieh, Martinez, et al., 2017). Older adults living in neighborhoods with more green space and recreation centers or areas dedicated less to schools and industries had higher outdoor walking levels (Zandieh, Flacke, et al., 2017).
Discussion
There is criticism that traditional mobility measures focus on perceived ability or capacity to make movements rather than actual mobility performance (Giannouli et al., 2016; Taylor et al., 2019). We found that GPS technology provides a capability of assessing mobility performance rather than mobility capacity. Also, GPS-based mobility studies focus on an individual’s spatiotemporal movement in their environment, but do not cover functional terms (e.g., physical ability to move around). Some of these measures are underrepresented in traditional mobility research, such as spatial size of mobility-related behaviors (e.g., ellipse area, minimum convex polygon) or straight-line distance. Therefore, mobility limitation defined and measured by GPS may not be the same as the mobility status determined by a traditional method that is mostly focused on functional abilities or biomechanical and physiological aspects of mobility. Given that declining mobility signals functional deterioration, accurate evaluation of mobility in older adults should be a critical component of geriatric care. This suggests that for older adults facing functional declines, longitudinal GPS-enabled mobility monitoring can be a reliable and objective tool for early detection of changes before they impact the quality of life as documented in a previous report (Manley et al., 2020).
This review shows that the breadth of aspects can be derived from GPS data for characterizing older adults’ mobility, such as spatiotemporal movement, travel modes, or weekday–weekend patterns of mobility. Although the differentiation of spatial and temporal mobility measures reflects the multidimensional aspects of mobility, it could only represent a partial understanding of mobility. It is necessary to identify a comprehensive and meaningful mobility pattern and understand mobility in the broader social and built environmental context not just as a collection of single mobility indicators or as physical movement (Franke et al., 2019). For example, if combined with data visualization techniques, GPS data can show where an individual spends most of their time over a specific period (Chung & Myers, 2019) or provide a picture of the varied development of mobility limitation over time or within-day fluctuation (Shoval et al., 2010, 2011). This type of granular information will be helpful to identify the reason for variability—whether it is caused by health impact, individual preferences, or unavailability of support for mobility behaviors. In addition, by combining GPS technology and other types of mobility assessment (e.g., diary), we can identify mobility behaviors that give a meaning and allow social connectedness.
There was considerable variation in the type of GPS devices, device use methods, and GPS-derived mobility measures across studies. For instance, some studies applied GPS technology only for 12 to 14 hr, whereas others measured mobility over the 24-hr span of the day. Although the same indicator of mobility was used in studies (e.g., outdoor time), different methods of defining the indicator were observed (e.g., outdoor durations for a specific travel mode, or outdoor time regardless of travel modes). This inconsistency may indicate that GPS-based mobility research is not mature yet and there is a need for a further discussion of definitions and operationalized constructs of meaningful mobility patterns for older adults.
Among all types of tracking technologies, GPS data loggers (especially Qstarz BT-1000XT) are frequently used in reviewed studies. Previous studies suggest that the Qstarz devices are acceptable for larger population studies due to its long battery life and spatial accuracy (Duncan et al., 2013; Schipperijn et al., 2014). GPS devices with extended battery duration might be particularly useful in aging studies to reduce the burden on older adults (e.g., charging). This capability also lowers the chance of missing data due to forgetfulness. On the contrary, technological advances in the past 10 years have made possible the development of miniaturized body-worn sensors with improved accuracy and longer battery life. The advantage of these devices is that older adults can wear it all the time with less interruption in daily lives. We found only two GPS watch-based and three smartphone-based studies. Given that a growing number of older adults are adopting wristband sensors or smartwatches to track their fitness and health (Vogels, 2020), these types of technologies may offer future potential for collecting location-based mobility data, as seen in more recent studies included in this review.
There should be considerations for factors leading to GPS data quality and precision issues, such as signal loss, battery issues, lack of participants’ protocol adherence to wearing the device, and device misuse (Krenn et al., 2011). We found that two thirds of the studies included a discussion of whether there were satellite- or battery-related errors or how data or signal loss was handled or linked to mobility outcomes. However, inconsistent computational algorithms or definitions of unusable data across studies indicate a need for developing standardized GPS measurement and data analytics protocol. In addition, most studies did not provide specific information regarding training of participants. A thorough training of older adults on how to use the GPS device is critical to ensuring appropriate technology use and GPS data quality. Moreover, positional accuracy was reported only in one third of the studies. Because of the limitations in reporting, it was impossible to explain factors associated with the precision of GPS data. Given the potential usefulness of using GPS devices in geriatric care (e.g., detecting locations of dementia patients to prevent wandering or functional losses), there should be a focus of future efforts on identifying the nature of the signal loss or missing data (Cetateanu & Jones, 2016; Krenn et al., 2011) and determining the specifics of the signal processing steps to extract exact locations.
Many studies provided empirical support for an association between GPS-driven mobility status and breadth of multiple factors. Among them, cognitive function was one of the most frequently examined factors. This may reflect the current challenges in mobility assessment among older adults with cognitive impairment because of their limited ability to communicate or remember their mobility behaviors or locations (Shoval et al., 2011). In addition, we found that significant associations between some aspects of social-environmental factors and GPS-based mobility levels were identified in only two studies (Hirsch et al., 2014; Werner et al., 2012). It is necessary to consider the important role of the social environment in determining one’s decision to go outside, such as social connection, identity, or social resources (Caspi et al., 2013), and to interpret mobility as “ongoing experiences, practices, and processes” (Franke et al., 2019, p. 2) that interact with neighborhood social capital.
Among the limitations of this review, the first is that it may not provide an exhaustive list of GPS-derived mobility measures because of the inclusion criteria. Second, great variability in the type and measurement of factors identified as having an association with GPS-based mobility status made it impossible to compare the effect size across studies. Third, the quality scoring indicators were developed based on the previously published work and adapted to the current review context, but the indicators could have limitations.
Recommendations for future research include (a) considering the use context (e.g., cognitive status), user preferences, GPS recording periods, and the characteristics of the environment where the location tracking takes place (e.g., dense locations) before selecting GPS tracking technology; such approaches could promote adherence to GPS monitoring protocols, which is critical to the quality of location data; (b) performing a minimum of 7-day GPS monitoring to include data from multiple days and find weekday and weekend mobility variations; (c) developing and implementing rigorous training instructions to ensure older adults’ adherence to the study protocol based on multiple educational strategies (e.g., printed materials, teach-back use, and ongoing technology support); and (d) developing algorithms to identify early warnings for a target adverse health outcome (e.g., cognitive impairment or social isolation).
Conclusion
GPS technology has the potential to examine highly detailed geographic and temporal scope of mobility in older adults, thus providing a “holistic view” of mobility in real time and enabling prompt interventions to prevent adverse health events resulting from mobility limitations. Potential future research should identify meaningful GPS-derived mobility patterns and develop standardized guidelines for GPS use and data analytics (e.g., wear time, recording period, and definition of usable data). In addition, future examination needs to focus on social and built environmental factors, such as availability of neighborhood organizations, facility accessibility, transit access, or the diversity of cityscapes that have not received much attention, but potentially influence the level of GPS-derived mobility status.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820979801 – Supplemental material for GPS Tracking Technologies to Measure Mobility-Related Behaviors in Community-Dwelling Older Adults: A Systematic Review
Supplemental material, sj-pdf-1-jag-10.1177_0733464820979801 for GPS Tracking Technologies to Measure Mobility-Related Behaviors in Community-Dwelling Older Adults: A Systematic Review by Jane Chung, Lana Sargent, Roy Brown, Tracey Gendron and David Wheeler in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.