
Abstract
The elder abuse field needs high-quality intervention research to assess the best strategies to combat the problem, but few such studies exist. Significant advances have been made in elder abuse research methodology, measurement, justice theory, and other relevant areas, which may remedy this gap. Particular advances include the use of elder abuse severity measures and goal attainment scaling, and the application of restorative justice theory to intervention. Elder abuse research also may benefit from advances in biomedical clinical trial methodology, including characterizing and following up with subjects excluded from trials or those who drop out, estimating numbers needed to treat to assess cost-effectiveness, and a priori stopping rules for when an intervention proves quickly beneficial or harmful. In this article, we argue these advances can and should inform elder abuse intervention research, propose a theoretical framework to guide such efforts, and demonstrate how this framework can inform practice, using elder abuse multidisciplinary teams and nursing home shelters as examples.
“Research seeks to prove; Evaluation seeks to improve.”
Introduction
As researchers and clinicians who have worked in the field of elder abuse for many years, we are profoundly aware of the urgent need for effective interventions. Millions of older adults are abused each year, with an annual prevalence rate of elder abuse in all its forms approaching or exceeding 10% (Pillemer et al., 2016; Yon et al., 2017). The costs of elder mistreatment are enormous, including not only unnecessary human suffering but also strains placed on health and social service systems that work to prevent and treat these complex cases.
Unfortunately, this urgency has led to elder abuse interventions that have been put into practice without rigorous programmatic evaluation. Indeed, a recent systematic review of elder abuse intervention over the last several decades identified 115 elder abuse programs, the majority of which involved interventions; only 2% had a high-quality study design (T. Rosen et al., 2019). An accompanying editorial stated, It is worth spending a moment on barriers to meeting high standards of program evaluation. These include challenges fielding randomized controlled trials with vulnerable older adults served by public programs, the variability of types of abuse that may require different interventions, victims’ variable risk factors, and multiple and divergent settings. Research is also lacking on the perspectives of older adults who have been victimized.
The notion that elder abuse interventions are being developed and deployed in the community without rigorous programmatic evaluation is concerning for several reasons. The most obvious is that they may not work. Alternatively, they may be marginally effective and would benefit from changes informed by high-quality intervention research. Furthermore, an intervention may work, but at excessive cost, and those resources could be more efficiently deployed if also informed by rigorous intervention research. Finally, elder abuse programs almost never consider the unpalatable prospect that interventions might actually be harmful to victims or other stakeholders, which is highly problematic.
Fortunately, many advances have been made in intervention research methods generally, and elder abuse research and theory specifically, which can be brought to bear on determining the effectiveness (or unintended negative consequences) of elder abuse programs. These new trends include improvements in elder abuse measurement, strategies to include a broader array of stakeholders and solicit their perspectives, and general improvements in sampling and study design.
In this article, we discuss recent advances in elder abuse research and theory how they can be brought to bear on improved elder abuse intervention program evaluations. To operationalize how these benefits might be achieved, we focus on two popular and rapidly expanding elder abuse interventions as exemplars: multidisciplinary teams (MDTs) and elder abuse shelters. We would note that our focus is on intervention research in this article. Intervention research tests the effectiveness of programs and policies that reduce risk factors, increase protective factors, reduce harm to individuals, and improve their health and quality of life (Sidani, 2015). Intervention research ideally contributes to both scientific knowledge and human well-being through the application of rigorous methods to determine program effectiveness.
Recent Developments in the Field Relevant to Intervention Research
The field of elder abuse research is in an expanding and dynamic phase, with new advances in methodology and theory. In this section, we suggest how several such advances can inform intervention design and evaluation.
Measuring Elder Abuse Severity
Burnes and colleagues are engaged in innovative research on elder abuse outcome measurement, focusing on developing measures of elder abuse severity. Historically, elder abuse as a dependent or independent variable has been measured dichotomously—absent or present—in virtually all epidemiological studies. This may have been useful in early epidemiologic studies of prevalence, but it clearly does not reflect the experience of most victims and the professionals serving them. Specifically, any type of elder abuse can have a different impact on different victims based on prior history, chronicity, perceived severity, and associated distress.
Consider two older adults who are victims of verbal elder abuse. For one, the abuse takes the form of infrequent verbal insults and taunting. For the other, abuse takes the form of multiple daily threats of institutionalization and abandonment by the abuser, causing severe chronic distress. The designation “Verbal Elder Abuse Victim” does not capture the richness of the differential impact on these two victims, yet they have been treated equivalently in elder abuse research.
This makes it difficult to interpret and utilize research results. This is best illustrated by invoking the paradigm of the clinical trial in biomedical research, wherein the diseases of subjects are not adjusted for baseline severity. Imagine a chemotherapy trial for lung cancer in which patients with minor and widely metastatic disease are pooled together at the study’s beginning and that the only measured outcome of the study is cure versus death. Positive or negative effects may thus erroneously be ascribed to the intervention when, in reality, they arose from baseline differences. Furthermore, patients who are not “cured” of their malignancies would be deemed as “treatment failures” even if the treatment afforded enormous improvement in quality of life and perceived well-being.
Using data from the New York State Elder Abuse Prevalence Study, Burnes and colleagues not only looked at whether elder abuse was absent or present in the sample for the purpose of determining prevalence; he also determined (a) how frequently the abuse occurred in the previous year, and (b) what the perceived distress was for the victim (Burnes et al., 2018). The result show that different forms of abuse had differential impact based on frequency and perceived distress.
The implications for intervention studies are clear: (a) prior to enrollment, victims should be stratified based on severity, and (b) frequency and severity should be included in outcome measures because older adults can have different experiences after an intervention, even if the abuse is not completely stopped. Insofar as elder abuse victims are rarely extricated from their environments completely, this approach is a more useful measure of outcome.
In modern biomedical research, separate trials and/or subgroup analyses are typically conducted taking into account the severity of initial disease. Because cure is rarely the outcome of chronic disease therapy in medicine, more salient and proximate measures are invariably and requisitely considered, ranging from functional status to quality of life. The equivalent should be done for elder abuse.
Involving More Stakeholders: Restorative Justice Theory
To those with little or no familiarity with the complexity of elder abuse, serious cases typically and understandably evoke outrage and the belief that perpetrators should be arrested and prosecuted to assure justice for the victim. This posture stems from the concept of retributive justice, a theory of punishment that punishes the criminal in proportion to their crime. Also referred to as retaliatory justice or “lex talionis” (from the Latin, law of retribution), it is derived from the code of Hammurabi, best exemplified by the aphorism “an eye for an eye.”
However, the retributive justice paradigm is often inapplicable to elder abuse cases and can cause additional undue harm to victims, society, and even abusers. For example, should we incarcerate an adult child with schizophrenia whose neglect of his father stems from medical nonadherence? Do we ignore the pleas of a competent victim not to arrest a grandchild who is drug addicted and neglectful because it would cause emotional distress and nursing home placement for that older adult? Should we prosecute stressed caregivers who briefly respond to a spouse’s dementia-related agitation in the midst of morning caregiving with a push or slap? There are countless examples, and no stakeholder is served well by this inflexible posture.
Accordingly, there is an increasing interest in the concept of restorative justice as it relates to elder abuse cases (Brown & McNeal, 2018). Restorative justice is a response to crime wherein all stakeholders (beyond just the victim and perpetrator) are identified. Their experiences and perspectives about what happened are shared, including who was harmed and how, with the goal of building a consensus about how the harm can be repaired by the perpetrator in a way that prevents revictimization of the victim as well as the community.
This paradigm aligns with the goals of elder abuse intervention and the perspectives of many stakeholders. A police officer arresting an abuser who is developmentally disabled may insist on criminal prosecution, but such a perpetrator will be at grave risk if incarcerated, and the affected victim may be permanently placed in a nursing home if that abuser is the sole caregiver. Politicians may have strong feelings about tax dollars directed to incarceration versus relevant community mental health services for such an abuser. Community members may feel differently depending on the danger a perpetrator poses to them should he or she be permitted to return home with other remedies. The discussion and consensus process initiated by restorative justice is in and of itself an intervention that can honor all perspectives and may heal many of those affected.
Discerning Stakeholder Values: Goal Attainment Scaling (GAS)
Identifying all stakeholders is an important first step, but how may these diverse perspectives be solicited and measured in a way suitable for research? The use of GAS as applied to elder abuse is another promising new development in this regard (Burnes & Lachs, 2017). In this methodology, each victim or other stakeholder designates his or her own desirable outcomes from an intervention before it is proffered. These outcomes or “goals” are highly specific, individualized, and speak to activities that have been negatively affected by a victim’s elder abuse and what they would like remedied.
Examples include the wish to remain at home despite the presence of an abusing family member, to be able to visit regularly with grandchildren, or to attend church on a daily basis. Once these goals are articulated, anchored outcomes are created for each goal (such as visiting church daily, weekly, infrequently, or not at all) which are recorded pre- and postintervention. Failure or success of the intervention is judged on whether these personally articulated goals are achieved. Statistical methods are used to normalize the scales across participants so that outcome scores are comparable.
Two aspects of GAS are especially compelling. First, it is how clinicians think and work to serve victims. They are typically confronted with complex cases causing multiple kinds of distress and must creatively problem-solve to optimize multiple outcomes, many of which may not be reflected or even considered on a standardized instrument. Second, GAS aligns well with the clinical concept of “person-centered care” in modern medicine. Outcomes that researchers value highly (like incarcerating a perpetrator) may be of no interest to a victim (or other stakeholders) and even be harmful.
New GAS smartphone apps are now being piloted for Adult Protective Service (APS) workers in the field in which victims can not only choose from several prepopulated outcomes but also add their own. GAS is clearly a promising methodology for discerning victim and other stakeholder preferences in elder abuse.
Monitoring and Measuring for Stakeholder Adverse Events in Elder Abuse Interventions
The history of interventions for social and medical conditions research is rife with examples of well-intentioned programs deployed without evidence in which subsequent programmatic evaluations revealed ineffectiveness or even danger to the target audience or stakeholders that were not initially considered. In elder abuse, for example, hundreds of millions of dollars have been spent on mandatory reporting laws since they were incepted in the 1970s; there is still no consensus on their value (U.S. General Accounting Office, 1991) and many observers believe they have done nothing to help victims.
In medicine, we once routinely performed cholecystectomy for asymptomatic gallstones until we found it did not help, and we administered thalidomide to prevent miscarriages until we discovered it led to birth defects. Drug prevention programs for adolescents have been found in some cases to increase the risk of substance abuse (Werch & Owen, 2002). Mandatory incarceration programs for perpetrators of domestic violence programs can fracture families and paradoxically escalate violence. There are countless examples of unintended perverse negative outcomes of interventions.
It is remarkable, then, that elder abuse studies have rarely included an examination of adverse events and negative consequences, although clinicians are well aware of this possibility, which have been discussed in the literature. In primary care, for example, identification of elder abuse may escalate an already incendiary domestic violence situation when abusers are confronted (Lachs, 2004). Identification of elder abuse has also been shown to be a strong risk factor for nursing home placement (Lachs et al., 2002), a traumatic and generally undesirable event that permanently removes the older adult from the community.
When well-meaning interventions are proffered without a rigorous, evidence-based outcome study and safeguards, stakeholders may be harmed.
Other General Advances in Research Methodology Relevant to Programmatic Evaluation
In addition to specific advances in elder abuse research methodology, elder abuse programmatic evaluation may also benefit from advances in biomedical clinical trial methodology, including statistical and sampling techniques such as propensity matching, characterization and following up with subjects excluded from trials or those who drop out, estimating number needed to treat to assess cost-effectiveness, and a priori stopping rules for when an intervention proves quickly beneficial or harmful.
Programmatic Evaluation: Real-World Examples
Applying this paradigm will require an a priori stipulation of positive and negative outcomes, articulation of the measures to be used, and rigorous evaluation strategies. To illustrate how such aims might be achieved, we apply these evaluation methods to two elder abuse interventions that are gaining traction despite a relative paucity of effectiveness data: Elder Abuse Multidisciplinary Teams and the Use of Nursing Home Beds as Shelters for victims of Elder Abuse.
Elder Abuse MDTs
Elder abuse MDTs are spreading rapidly across the United States (Twomey et al., 2010). MDTs consist of physicians, social workers, law enforcement, attorneys, and other community participants working together in a coordinated fashion. Led by an MDT Coordinator (typically a social worker), teams convene on a regular basis to discuss difficult elder abuse cases in their community and coordinate a rational response with each team member providing expertise. A discrete plan of action is developed with individual team members assigned to specific tasks; a follow-up time frame is specified. Advocates for MDTs argue that they improve efficiency, coordination, and professional support experienced by members (Lachs & Pillemer, 2015). MDTs may help victims, families, and the professionals who serve them in many ways, but both the potential positive and negative consequences to all stakeholders must be considered, and this should drive the development of metrics for their evaluation (Table 1).
Stakeholders Likely to Benefit From Elder Abuse Multidisciplinary Teams: Relevant Domains for Evaluation and Potential Concerns.
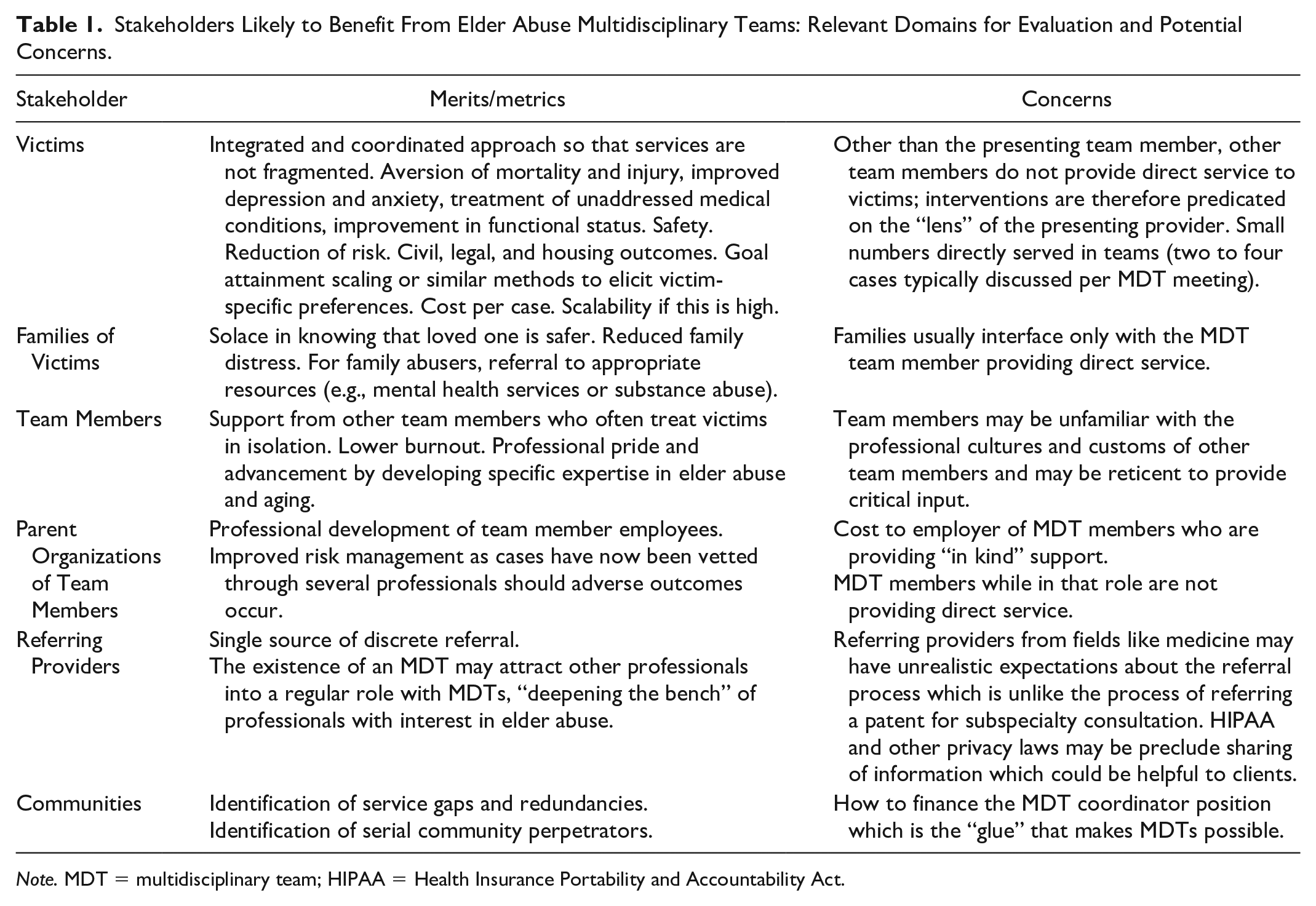
Note. MDT = multidisciplinary team; HIPAA = Health Insurance Portability and Accountability Act.
Potential benefits
For elder abuse victims, who typically traverse many systems—health care, law enforcement, housing, criminal justice, and social welfare to name a few—an integrated team approach has many attractive features that should serve as metrics. These include coordination of care, integrated health care and legal representation, avoidance of redundant services, and a discrete follow-up plan with “ownership” for follow-up assigned to designated individuals on the team. Thus, measures like client safety, a reduction in harm, and attention to untreated medical problems that were previously unaddressed because of isolation are all benefits. Similarly, when mistreatment is the product of untreated medical or psychiatric problems in the abuser such as addiction or mental illness, there may be an opportunity to comprehensively address the direct causes of abuse with the integrated interventions MDTs can offer.
Members of MDTs also may benefit directly; serving elder abuse victims is hard work that is often conducted in isolation. Worries about burnout among APS professionals and others are a real concern. Having the emotional support of a large team of professional colleagues who can offer advice and feedback is invaluable; most MDT members report that this is a major attraction to membership (Navarro et al., 2010). For members who do not work primarily in the field of aging or elder abuse (such as police officers), participation in an MDT afford the opportunity for “specialization” within their profession and an opportunity for professional advancement and recognition.
Communities can benefit in many ways as well. In addition to improving the general safety of their environments and instilling a source of pride as advocates for older people, the presence of a team can alert communities to both gaps and redundancies in programs that serve older adults generally and elder abuse victims specifically, allowing for the more strategic deployment. MDTs also may lead to the identification of community abusers who prey on older people serially, when multiple cases are presented to the team with similar patterns. The coordinated approach may permit a swift integrated response to apprehend such an offender and prevent the victimization of others.
Potential concerns
Although promising, there are several concerns raised by the popularity and spread of MDT movements.
MDTs do not provide direct services to victims; rather, those direct service providers present cases of concern to them to the larger team, one of whom will typically interact with a victim directly unless a cross referral is made. How data are presented to the team about a victim has enormous bearing on the nature of discussions on individual cases. Team members may speak different “languages,” and the siloed nature of different professions with different policies, practices, and administrative structures may actually impede help for victims. For example, professionals wishing to present a difficult case to the team may be restricted by their institutions’ privacy policies and Health Insurance Portability and Accountability Act (HIPAA). In certain jurisdictions, law enforcement officers may be precluded from presenting or participating in team discussions when criminal proceedings are pending.
Data collection methods and quality in MDTs have not been standardized. In a recent review of MDTs across the country, data collection methods ranged from physical hard copies, to simple excel spreadsheets, to more sophisticated data collection systems. In addition, the number and types of variables collected were also wide-ranging. Yet, another data problem is where MDT data should reside. Hospitals with physicians participating in MDTs will not want their HIPAA-protected health data on external servers. Although these many problems in data quality, access, and standardization may seem insurmountable, the upside for research progress in elder abuse is enormous, and several researchers are working toward creating a standardized data set for MDTs.
“Live” elder abuse cases often create the need to make swift decisions in the field with limited information to assure client safety; team members subsequently presenting their decisions to an MDT may feel second-guessed. Cultural concerns between different team members may lead to resentment or a “blame game.” APS professionals, for example, may feel intimidated about presenting their cases and action plans to highly trained geriatricians and psychiatrists, and that their work is being scrutinized. Similarly, physicians may have little appreciation for the difficult work APS perform in the field with limited support. Insofar as each team member reports to a different organizational hierarchy, accountability to team members may take a back seat to their own institutional table of organization. Relatedly, different levels of engagement by team members may develop based on “buy in” by their home institutions.
When their true costs are calculated, MDTs may turn out to be expensive. Typically, team members participate by providing “in kind” support (their salaries are paid by their employers), and the combined hourly cost of 10 or 20 professionals meeting weekly for 2 hr is substantial. In addition, these are hours that are not spent in direct clinical service. Although typically only the salary of the MDT coordinator is a “new” expense, how do communities replace the time of this critical full-time equivalent (FTE) in austere budgetary environments?
Finally, MDTs may not be able to serve a large number of victims relative to the overall need. Complex cases require much time and discussion; in a typical MDT meeting, two to four cases are presented, raising issues of scalability and cost-effectiveness.
Nursing Home Shelters for Elder Abuse Victims
Widely used for younger victims of domestic violence, the shelter concept is designed to allow a victim to escape a dangerous home situation to a place of safety. Shelters have primarily targeted victims of intimate partner violence, allowing them respite from the violent situation while they can make plans for an alternative living arrangement. Typically, shelters address a range of problems victims experience, helping them access legal advice, financial aid, and employment (Wilkes, 2019).
The use of nursing home beds to shelter community elder abuse is an idea that is gaining attention (Sewell, 2013). Advocates argue that nursing homes are logical places where victims can be protected and evaluated while their situations are sorted out. Facility resources can be used to carry out such evaluation, typically including an interdisciplinary team of clinicians, lawyers, social workers, and others so that a safety plan may be created.
An example is the shelter created by the Hebrew Home in the Riverdale in New York City. Known as the Harry and Jeanette Weinberg Center for Elder Justice (Reingold, 2006); attempts at national and even international dissemination and replication are already underway (Solomon & Reingold, 2012). In addition to its shelter activities, the Weinberg Center also conducts community and professional education programs and collaborates with many other elder abuse programs. Recently, the John A. Hartford Foundation funded an evaluation of the program by the Rand Corporation, which we believe to be the largest such investment in an elder abuse evaluation ever, in anticipation of potential dissemination (The John A. Hartford Foundation, 2019).
Potential benefits
For individual elder abuse victims and their concerned nonabusing family members, the potential benefits of the shelter would seem obvious (Table 2). Elder abuse cases in the community are extraordinarily complex and chronic, often with ongoing abuse continuing to occur while community evaluations and interventions take place. Shelters may provide a desperately needed “time out” and a place for safety while a litany of problems—legal, psychological, financial, and housing related, to name a few—are addressed.
Stakeholders Likely to Benefit From Nursing Home Elder Abuse Shelters: Relevant Domains for Evaluation and Potential Concerns.
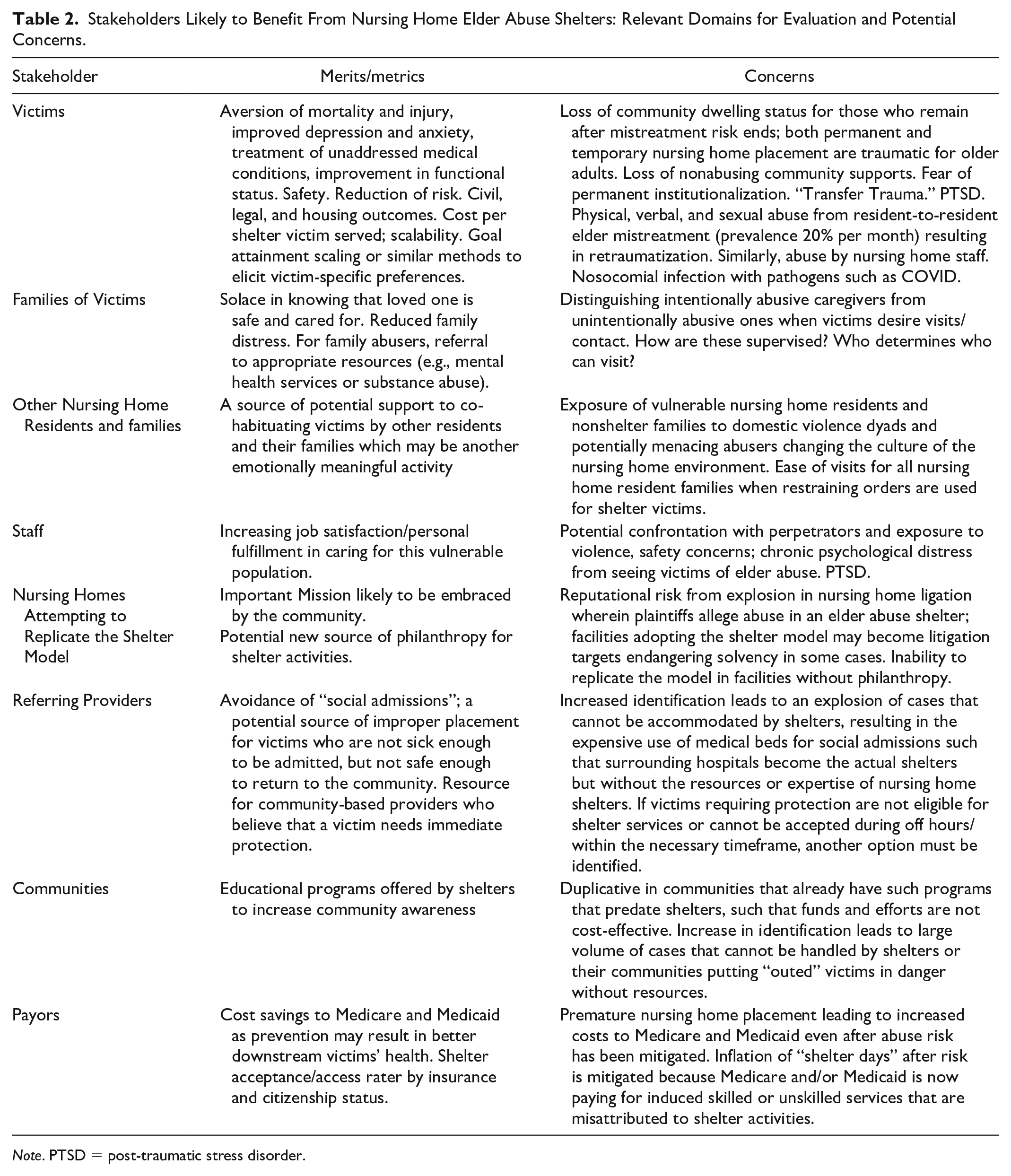
Note. PTSD = post-traumatic stress disorder.
In addition, nursing homes are places where a range of medical and psychiatric resources may be brought to bear on a victim’s situation in a coordinated fashion. Thus, there are many relevant metrics of nursing home-based emergency shelters to be measured, including mortality and/or further injury, reducing depression and anxiety, improving functional status, stabilizing chronic medical conditions, and anxiety. For victims who return to the community after shelter, what are rates of readmission, revictimization, and relative safety by removing or mitigating risk? And what happens to perpetrators after community return? These outcomes must be measured in the context of the cost per shelter victim served to understand the actual return on investment (ROI). Even if the shelter is clinically successful, if “cost per case” is high, many more victims could be served at lower cost by bringing the same services to the victim in subsidized community housing with careful case management, avoiding the trauma of nursing home placement.
Victims may not be the only beneficiaries. Families are likely to be relieved that a relative is at least temporarily safe. Nursing home employees may find additional meaning in their difficult work by helping these victims. Facilities themselves can garner community stature and support through this additional noble mission that may attract philanthropy. Ripple effects may occur in local communities, especially if shelters provide elder abuse education.
Potential adverse events to stakeholders
For any medical or social condition, nursing home placement, either temporary or permanent, is perhaps the most draconian solution and an intervention of last resort. Patients, families, and public fear it for many reasons, including the understandable stigma that it signals the end of community living and independence (Loebel et al., 1991; H. Rosén et al., 2019). Elder abuse victims are among the most medically, emotionally, and socially frail older members of society. Thus, the potential negative effects of removing an elder abuse victim from their environment to shelter them in a nursing home, however dangerous and/or well intentioned this may be, must be considered if we are to avoid unintended consequences for all stakeholders.
For example, evidence is emerging that even the best nursing homes can be violent places for all dyads (residents, staff, and families); recent studies have shown that rates of resident-to-resident elder abuse in nursing homes are 20% per month (Lachs et al., 2016). Placing an elder abuse victim in a shelter only to experience a different kind of abuse is a pyrrhic victory. Furthermore, studies over three decades show the possibility of elder abuse victimization by staff (Yon et al., 2019).
It is therefore critical in evaluating elder abuse shelters to ascertain whether additional victimization occurs during shelter. In addition, moving out of one’s home to a nursing home has been shown to result in “transfer trauma” with extremely elevated rates of adverse events such as health instability, hospitalization, and death, especially within the first 90 days of admission (Hirdes et al., 2019). Implementers of such programs need to measure outcomes related to possibly iatrogenic consequences of the nursing home environment ranging from the high rates of depression to exposures to resistant bacterial pathogens not present at home. The recent pandemic of Coronavirus in nursing homes underscores this.
There are further concerns about using nursing homes as emergency elder abuse shelters that emerge from the social context of long-term care that could negatively affect nursing home culture. There is a literature that underpaid frontline staff themselves may come from disadvantaged environments and be victims of domestic violence at a higher rate than in the general population (Tellis-Nayak & Tellis-Nayak, 1989). What is the impact of both seeing older domestic violence victims and having to interact with their abusers who may be menacing when you are a domestic violence victim at home? And what about other families who may have to interact with visitors, some of whom are elder abuse perpetrators? How does the need for heightened security and restraining or protective orders affect other family members’ ability to visit?
An additional implementation concern is that nursing homes attempting to adopt the shelter model may assume reputational risk. There is an explosion of civil litigation against nursing homes in the United States, both meritorious and frivolous, in which families allege elder abuse; in some cases, this has led to insolvency and closure (Zinn et al., 2009). However, irrespective of a lawsuit’s merit, families may be especially aware of mistreatment that occurs in a facility’s elder abuse shelter. If this is the case, facilities attempting to replicate the shelter model may be unfairly rewarded by becoming bigger targets for civil litigation, negative publicity, and public scrutiny.
While examining outcomes is the most important method for evaluating interventions, much may also be learned using relevant process measures, and there are many important variables to be measured here: Exactly what types of interventions are being proffered for both elder abuse and other neglected medical problems? Elder abuse victims may be in immediate grave danger; how long from the referral does it take for a person to enter? Are patients accepted during nights and weekends? A “shelter” by its very name and designation connotes a place of safety for people in danger that people can access without regard to time of the day, financial means, or clinical complexity.
No proposed modern medical intervention is evaluated without an economic analysis. How many victims are served by shelters and what is the cost per case to philanthropies who want to fund shelters? Insofar as Medicaid, Medicare, and other payers contribute to nursing home remuneration, how does this financial synergy work? Relatedly, for victims who transition to live in these facilities as the best alternative to community return once elder abuse risk is eliminated, how are bed days (an important ROI metric) allocated between “shelter days” and “custodial skilled nursing days” that have nothing to do with shelter services?
We also need to hear from referring stakeholders such as primary care physicians, hospitals, APS, and other community-based organizations. How are nursing home shelter programs filling gaps in services needed for victims? What are their strengths and key limitations? Also, the community elder abuse education programs offered by shelters or others invariably lead to heightened awareness and greater detection, with a nearby nursing home shelter being an obvious and ideal disposition for these victims. Can shelters accommodate the increase in referrals they have generated through their educational efforts and respond quickly? And, if they cannot, what is the blowback from hospital administrators who may be saddled with additional emergency department visits and dreaded “social admissions”; this backlog makes hospitals de facto and expensive elder abuse shelters in and of themselves but without portfolio. It also blocks access to acute care hospital beds that may be desperately needed in some communities for seriously ill patients and offers lower reimbursement to hospitals struggling with solvency.
Finally, an often-cited adage in medical research very much applies here: What happens to patients enrolled in clinical studies is certainly interesting, but knowing about what happened to those who are excluded is absolutely critical (Tierney & Stewart, 2005). An elder abuse shelter must likely employ selection criteria; for example, it may only admit individuals who are deemed able to return to their own homes after entry. Again, this is at odds with models of domestic violence shelters for other populations that are generally considered to be immediately accessible safe places with few exclusion criteria for victims in imminent danger.
Therefore, we need to know what were the victims like who were not accepted? How many were denied relative to those who were accepted? What happened to them? What was the basis for their lack of eligibility? What are rates of access and denial sorted by measures like clinical complexity, psychiatric co-morbidity, insurance status, and immigration status? Similarly, while we must know about nursing homes that successfully adopted the shelter model, we must also know about those who could not and determine precisely what the barriers were.
Conclusion
The urgent need for elder abuse interventions has led to the creation and dissemination of programs that have not undergone rigorous evaluation. We may be allocating expensive resources to programs that do not work or that may actually be harmful. It is urgent that we remedy these gaps in our knowledge as victims are suffering.
Many recent advances in elder abuse measurement and theory, as well as clinical trial methods widely used in biomedical and social science research, can and should be brought to bear on elder abuse intervention evaluation in the future. MDTs and nursing home shelters are two such cases that are ripe for rigorous testing and can be evaluated with regard to a diverse array of stakeholders beyond just victims. Such a paradigm can illuminate the benefits of elder abuse interventions, identify unintended consequences, and inform funders of their ROI both quantitatively and qualitatively.
Many new elder abuse interventions are being conceptualized and created in addition to MDTs and elder abuse shelters. These include the creation of Vulnerable Elder Protection Teams in hospitals (T. Rosen et al. 2018) and Emergency Department elder abuse screening programs. Insofar as the history of medicine generally and the field of domestic violence are filled with well-intended treatments that proved to be ineffective or even harmful, these must be rigorously evaluated. And although the well-intentioned impulse to create interventions to combat elder abuse is understandable, a cautionary adage from the business world would seem to apply here: “Bad decisions made with good intentions are still bad decisions” (Collins, 2009).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anthony Rosen’s participation was supported by a Paul B. Beeson Emerging Leaders Career Development Award in Aging (K76 AG054866) from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.