
Abstract
We aimed to examine the longitudinal association between frailty and cognitive impairment in the older Chinese population. This prospective cohort study used data from the Chinese Longitudinal Healthy Longevity Study 2011 wave. We calculated the follow-up duration as 3 years from the baseline year. Frailty was measured using the frailty index, and cognitive function was calculated by Mini-Mental State Examination Scale. Participants who were non-frailty and those with normal cognitive function were included in 2011 and followed up in 2014, respectively. Frailty was an independent risk factor for early-onset cognitive impairment. Age, hearing impairment, and a decreased ability to perform daily activities were the main risk factors for cognitive impairment, while affluent economic status was a protective factor. Cognitive impairment was not found to be an independent risk factor for frailty. We concluded that the frailty index is a significant predictor of cognitive impairment among community-dwelling older adults.
• Physical activity and cognitive function in older adults are interrelated. Frailty is an independent risk factor for early cognitive impairment, and the frailty index can be used to predict early-onset cognitive impairment.
• Since comorbidities are common in older adults, considering a “bio-psychological-social” approach may help prevent frailty and improve efficiency of care for older populations.What this paper adds
Applications of study findings
Introduction
In the older population, health indicators may be improved by effective medications and improvement of socio-economic conditions. The global population is rapidly aging; however, lifespan extension may prolong the decline in physical and cognitive functions as more frail older individuals survive their health problems yet consequently suffer (Chan et al., 2013; Christensen et al., 2013; Jean-Pierre et al., 2021; Verbrugge et al., 2017; Zeng, 2012; Zeng et al., 2017). The rapidly aging population associated with the one-child policy has created a significant challenge and posed serious burdens on the Chinese healthcare system (Zeng & Hesketh, 2016).
Frailty is characterized by a decline in various physiological reserve functions related to aging and an increased vulnerability to stressors. It can be measured in relation to accelerated biological aging using a frailty index (FI), which relates health deficit accumulation to the risk of all-cause and cause-specific mortality in older individuals (Hoogendijk et al., 2019; Mitnitski et al., 2001; Rockwood & Mitnitski, 2007; Searle et al., 2008; Song et al., 2010). The FI includes variables, such as activity of daily living (ADL) and cognitive functions, both of which can predict underlying medical conditions and mortality in older adults (Stenholm et al., 2019; Vermeiren et al., 2016). Early prevention and treatment can reduce frailty in older adults, thereby reducing the risk of disability and minimizing adverse outcomes (Rodriguez-Mañas & Fried, 2015; Stillman et al., 2021). Therefore, it is vital to design interventions based on increased awareness of the factors that pose a high risk for frailty in the aging population (Ofori-Asenso et al., 2019).
Cognitive impairment is an age-related, progressive neurological disease that has significant adverse effects on advanced brain functions, such as orientation, memory, and language. Dementia is the most serious stage of cognitive impairment and is associated with a high mortality rate, and is a heavy societal and economic burden. Mild cognitive impairment (MCI) is a state of cognitive function between normal aging and dementia (Nguyen et al., 2003). MCI has a high risk of progressing to dementia, but this process is considered reversible (Wu et al., 2021). Early identification of high-risk older people with early-onset cognitive impairment can better prevent progression to dementia (Wu et al., 2014). Clinical studies have shown that lifestyle interventions can delay the onset of dementia. Therefore, early screening and prevention of cognitive impairment have received increasing attention recently.
Both frailty and cognitive impairment are risk factors for future adverse health consequences. Recent studies have suggested that physical frailty and cognitive impairment share common etiologies rather than separate constructs (Sargent et al., 2020). However, few studies have shown the impact of the accumulation of health deficits on early-onset cognitive impairment and the influence of cognitive impairment on the progression of debilitating conditions (Brigola et al., 2020; Ma et al., 2019). Our research aimed to examine the longitudinal association between frailty and cognitive impairment in Chinese older adults for potential disease prevention and efficient care.
Methods
Study Design and Participants
The Chinese Longitudinal Healthy Longevity Survey (CLHLS), which provides information on health status and quality of life of older persons, is conducted nationwide in randomly selected counties and cities in 22 provinces in China (Sargent et al., 2020). We used data from the 2011 and 2014 CLHLS waves. All participants provided written informed consent. Further details regarding the CLHLS have been published elsewhere (Brigola et al., 2020). We excluded individuals who had missing information on cognitive function and on more than 30% of the variables used to calculate the FI. The number of participants included in the 2011 datasets followed up in 2014 was 1657. Consequently, we included 1545 participants with normal cognitive function in 2011, excluded those with cognitive impairment, and conducted a follow-up survey in 2014. We calculated the follow-up duration from the baseline year to analyze whether frailty is a risk factor for cognitive impairment. We then performed logistics regression analysis to further explore which dimension of the FI majorly contributed to cognitive impairment. On the other hand, 1477 participants in the non-frail group in 2011 were enrolled to investigate the contribution of cognitive impairment to frailty progression after baseline enrollment.
Measures
Health deficits were calculated using the FI. We selected 40 items related to functional, psychological, comorbidity, and social deficits. Binary variables were encoded as 0 or 1. The encoding of ordered and continuous variables was based on their distribution (Zeng et al., 2008; Chen et al., 2020). A score of 2 was assigned if the respondent had suffered more than one serious disease over the past 2 years (W. B. et al., 2005; Chen et al., 2020). The FI score was calculated as the sum of health deficits divided by the total number of deficits and was measured continuously between 0 and 1 (Supplementary Table S1). A score <0.25 indicated non-frailty, while a score ≥0.25 indicated frailty (Fan et al., 2020; Goggins et al., 2005).
The adapted Mini-Mental State Examination Scale was used to evaluate cognitive functions, and the scores were as follows: illiteracy >17 points, primary school education level >20 points, and middle school education for normal cognitive function >24 points (Cui et al., 2011; Folstein et al., 1975; Su et al., 2021).
The Activity of Daily Living Scale comprises two parts: the Physical Self-Maintenance Scale (PSMS) and the Instrumental Activities of Daily Living Scale (IADL) (Folstein et al., 1975; Fan et al., 2020). PSMS and IADL comprise six and eight items, respectively (Lawton & Brody, 1969). The lowest total score is 14 points, which indicates normal function; a score >14 indicates varying degrees of functional decline, with 56 as the highest, indicating dysfunction. A single item is classified as 1 being the normal and 2–4 as a functional decline. Moreover, two or more items having a score of ≥3 points or a total score of ≥22 points are considered significant functional impairment (Wiener et al., 1990).
Statistical Methods
Binary logistic regression was used to estimate the association between cognitive impairment and frailty, with age, sex, marital status, economic status, education, smoking history, alcohol consumption, diet, exercise, social activities, sleeping hours, and body mass index (BMI) as potential confounders. Results were reported with adjusted odds ratio (OR) and 95% confidence interval (CI). All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and IBM SPSS Statistics version 20 (SPSS Inc., Chicago, IL, USA), and graphs were plotted by R (vesion 4.0.2).
Results
Participant characteristics at baseline.
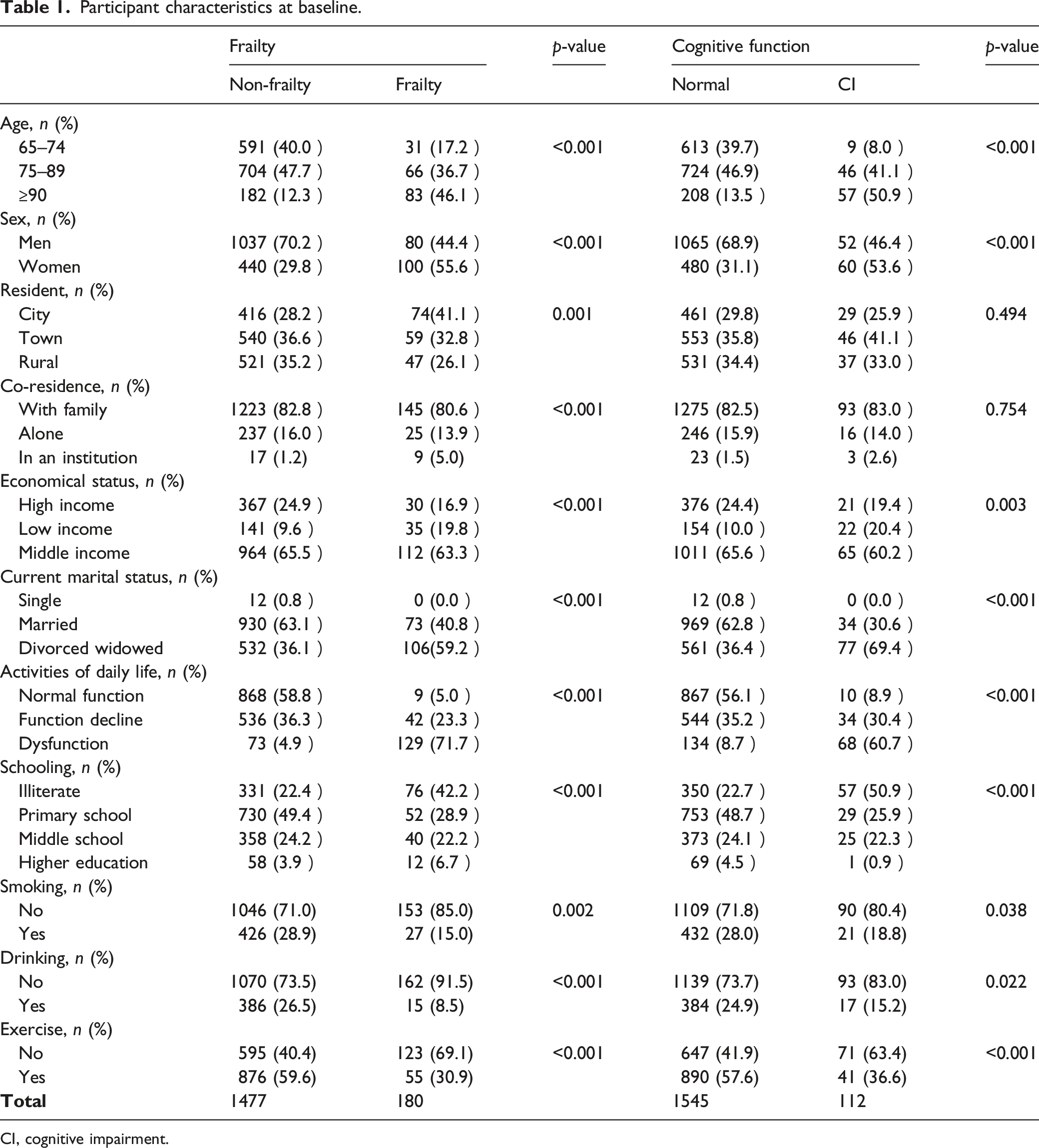
CI, cognitive impairment.
Logistic regression model analysis of the effect of frailty on cognitive function.
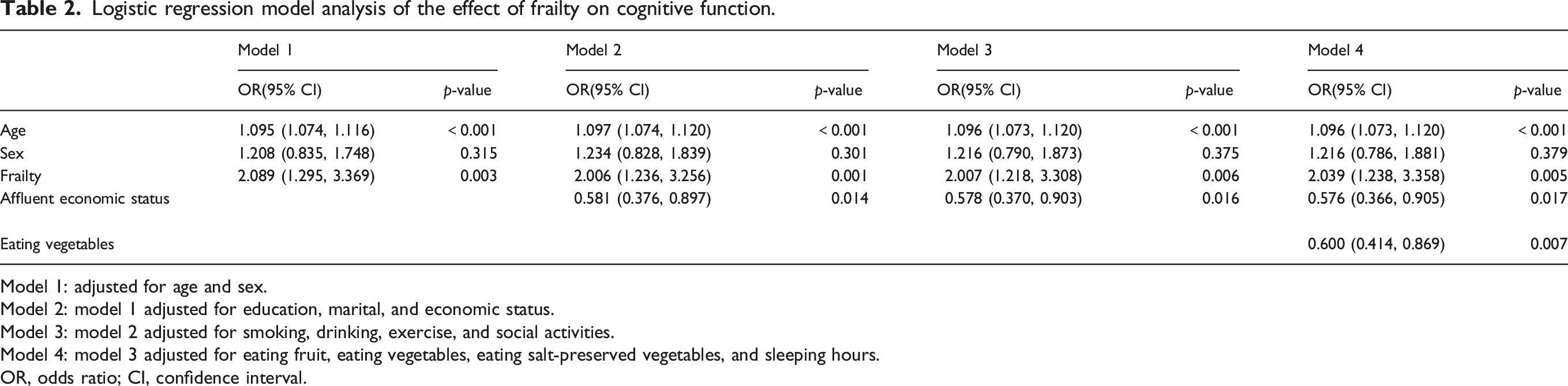
Model 1: adjusted for age and sex.
Model 2: model 1 adjusted for education, marital, and economic status.
Model 3: model 2 adjusted for smoking, drinking, exercise, and social activities.
Model 4: model 3 adjusted for eating fruit, eating vegetables, eating salt-preserved vegetables, and sleeping hours.
OR, odds ratio; CI, confidence interval.
Logistic regression model analysis of the effect of cognitive function on frailty.
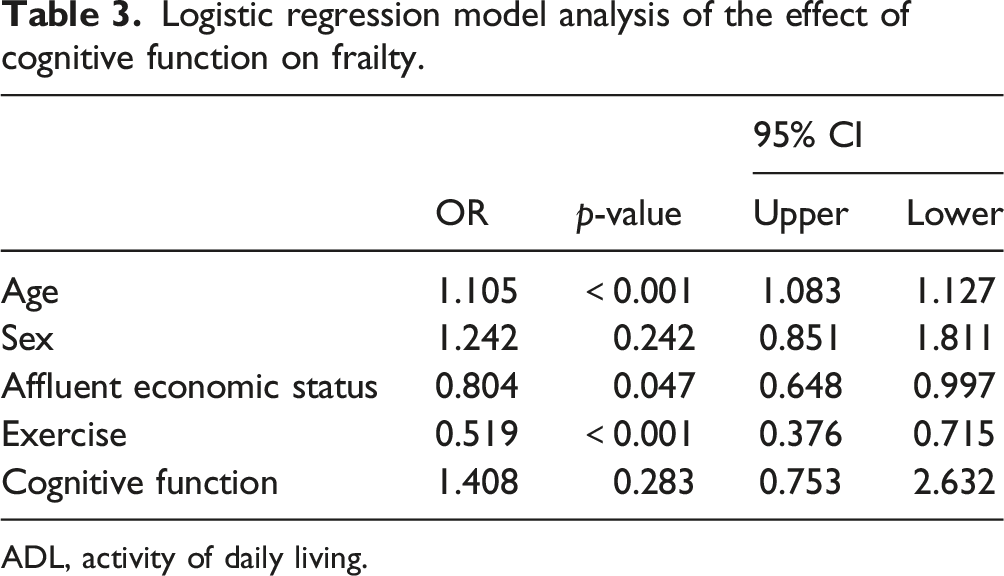
ADL, activity of daily living.
Based on the preliminary analysis, we performed univariate regression analysis of self-rated health, personality characteristics, daily activities, hearing impairment, visual impairment, and chronic comorbidities. Visual impairment, hearing impairment, and ADL dysfunction were all significant risk factors for cognitive impairment. The results of the multivariate regression analysis are shown in Figure 1. Affluent economic conditions reduced the risk of cognitive impairment by 40.1% (95% CI: 0.387, 0.927, p = 0.022). Hearing impairment was also a risk factor for cognitive function (OR 1.909, 95% CI: 1.049–3.472, p = 0.034). The risks of ADL decline and dysfunction increased by 1.903 (95% CI: 1.262, 2.869, p = 0.002) and 5.78 (95% CI: 3.455, 9.668, p < 0.001), respectively. Logistic regression of frailty components on cognitive function.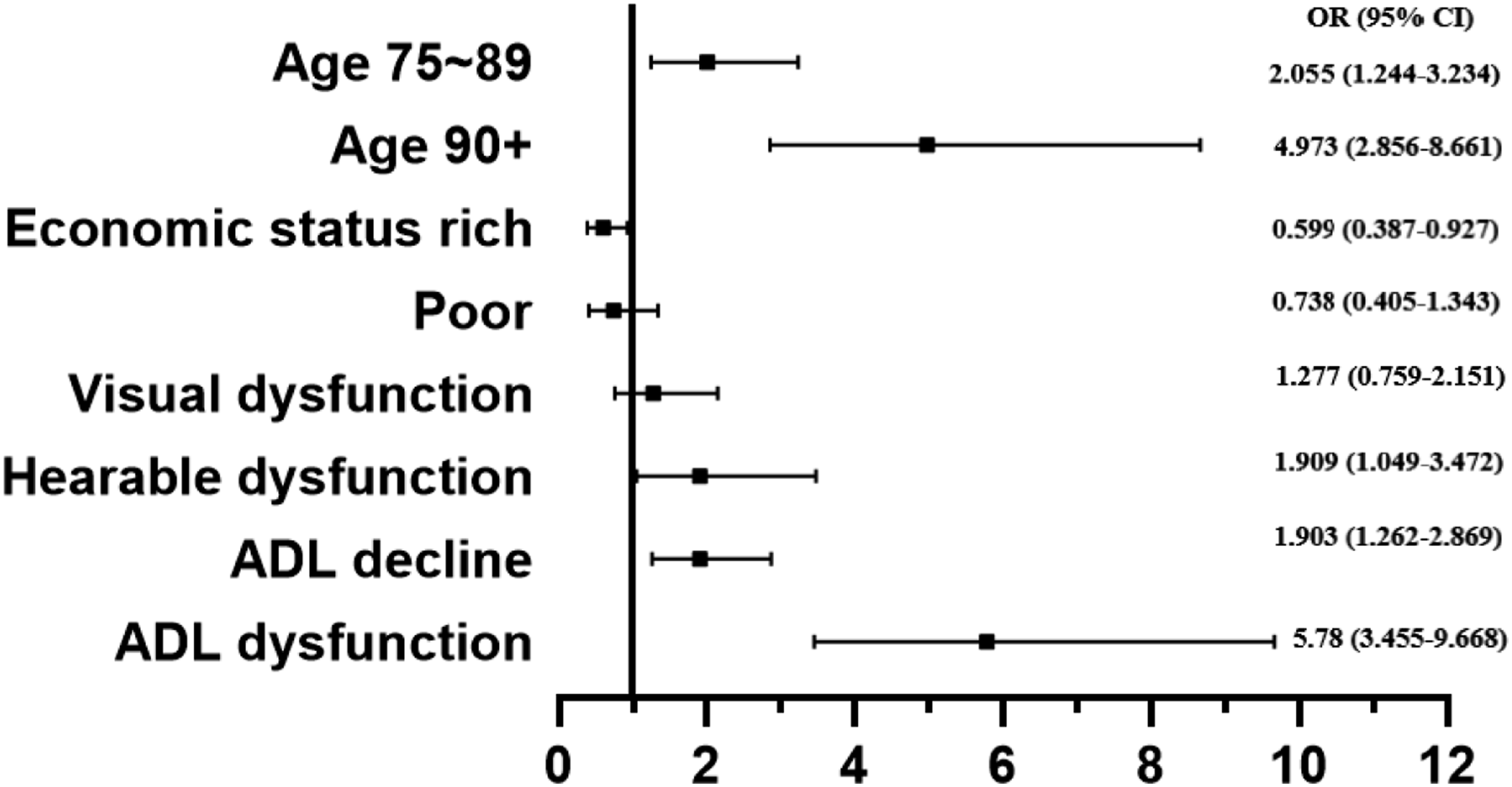
Discussion
The incidence rates of cognitive impairment and frailty are increasing in an aging population. (Davies et al., 2021; Zhang et al., 2021). Our study revealed the impact of health deficit accumulation on early-onset cognitive impairment, including the influence of cognitive impairment on the progression of debilitating conditions. To date, there are few cohort studies that have shown these results.
Some studies have suggested that overlapping risk factors and shared biological pathways may be involved in both cognitive impairment and frailty (Robertson et al., 2013; Sargent et al., 2018). Cognitive impairment and frailty may also be associated with certain risk factors. Socio-demographic factors, including old age, sex, economic status, current marital status, and education, were statistically significant at the baseline in our study. Frail older adults were at a higher risk for cognitive impairment than non-frail ones. Frailty was strongly associated with cognitive impairment, consistent with its role as a significant predictor of dementia among community-dwelling older people (Kojima et al., 2016).
Frailty transitions are independent of progression in cognitive status in the earliest stages of cognitive impairment (Chong et al., 2015; Ma et al., 2019). Frailty is related to an increased risk for Alzheimer's disease and dementia (Suo et al., 2016). Future studies should be conducted to assess how frailty is associated with cognitive changes over time. Since FI indicates the accumulation of health deficits to determine the specific influencing factors of frailty on cognitive impairment, we analyzed the various dimensions of frailty. We found that limitations in daily behavioral ability had a significant effect on cognitive function. This finding is similar to the results of previous studies (Wang et al., 2021; Wu et al., 2021). Decreased ADL ability is a risk factor for cognitive function and frailty, indicating that physical and mental activities are interrelated (Wu et al., 2021). Hearing impairment was also a significant risk factor for cognitive impairment and a decreased ability to perform ADL, which can be treated using interventions and rehabilitation equipment. Frailty contributed to early-onset cognitive impairment in this cohort and may constitute a novel modifiable target for early-onset cognitive impairment (Borges et al., 2019). Limited or impaired social functioning is associated with the development of frailty, possibly due to decreased mobility, which adversely affects social functioning (Davies et al., 2021). We assessed the impact of loneliness and emotional status on cognitive function but could not draw a causal conclusion. Research on loneliness and social isolation across large time spans should provide a better understanding of their relationships.
Cognitive impairment and physical frailty interact; as such, cognitive problems and dementia are more prevalent in physically frail individuals, and those with cognitive impairment are more prone to becoming frail (Halil et al., 2015). The therapeutic efficacy of physical and cognitive interventions depends on discrete neuronal mechanisms (Wallace et al., 2019). However, our longitudinal survey did not show any effect of cognitive impairment on frailty. This might have occurred due to several reasons. FI indicates the accumulation of overall health deficits, the burden of cognitive impairment is not that obvious, and dementia is a clear risk factor for debilitating conditions. It is also possible that the follow-up period was too short for any outcome events to be observed.
Given the rapid urbanization and upward job mobility in China, many older adults are now living alone and are thus prone to healthcare problems, in addition to having specific healthcare needs (Zeng et al., 2014). Therefore, the earlier health deficits and cognitive functioning problems are detected, the sooner suitable intervention is provided. As a limitation, this study did not include the analysis of molecular and biological markers, as well as other related factors. It is not sufficient to explore the mechanism of the influencing factors. Three years of follow-up was relatively short for some outcome events to occur and subsequently determine causality. Causal relationships should be investigated with long-term follow-up, and common-sense or telemedicine interventions can be used to evaluate the effectiveness of relevant interventions in further studies (Esfandiari et al., 2021). Chinese older adults have a long and deep-rooted tradition of filial piety, and the different way of elderly care from the West may also have a distinct impact on cognitive function and frailty (Laidlaw et al., 2010).
In conclusion, frailty is an independent risk factor for early cognitive impairment, and the FI can predict early-onset cognitive impairment. The association between mobility and cognitive function should be considered when evaluating the overall health of the older population. As the comorbidity of several diseases is common in older adults, comprehensive consideration should be given to daily behavior, psychology, and social participation to support the process of healthy aging in diverse orientations. Considering a biological, psychological, and social approach may help prevent frailty and improve efficiency of care for older populations (de Haan, 2021).
Supplemental Material
Supplementary Material - Longitudinal Relationship Between Frailty and Cognitive Impairment in Chinese Older Adults: A Prospective Study
Supplemental Material for Longitudinal Relationship Between Frailty and Cognitive Impairment in Chinese Older Adults: A Prospective Study by Xinxin Zhao, Qi Chen, Liang Zheng, Longbing. Ren, Yinghong Zhai, Jue Li, and Jia He in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Key R&D Program of China (No. 2017YFC0908005), and The Outstanding Clinical Discipline Project of Shanghai Pudong (Grant No. PWYgy2021-02)
Ethical approval
The Medical Ethics Committee of Tongji University, Shanghai, People’s Republic of China approved the present study (2021tjdx070).
Informed Consent
Written informed consent was obtained from all participants prior to the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.