
Abstract
This study was conducted using the data from 2015 China Health and Retirement Longitudinal Study (CHARLS). Gender-specific association between nighttime sleep duration (NSD) and falls were evaluated through multiple logistic regression by adjusting for confounding variables. Of the 22,899 respondents, 18,446 were eligible and 3,144 (16.99%) had more than a single fall. Short and long NSD were associated with high occurrences of falls in the total and female population, but only a short NSD was associated with a high occurrence of falls in the male population. In conclusion, NSD was strongly and significantly associated with falls, but the association was gender-specific. Accordingly, increasing targeted, evidence-based and gender-specific preventions for NSD and sleep disturbance are necessary among primary care interventions to prevent falls.
What this paper adds
• We conducted a robust analysis in a large sample to add evidence on the association between nighttime sleep duration and falls. • We were the first to investigate the gender-specific association between nighttime sleep duration and falls among community-dwelling middle-aged and older adults in China in this literature. • Similar to the association between nighttime sleep duration and falls in total population, an approximately “U-shaped” dose–response association was observed in female. Notably, the association was a nearly linear in male.
Applications of study findings
• Effective measurements include prolonging nighttime sleep duration should be established in community-dwelling middle-aged and older adults. • Gender differences are noteworthy issues when screening of individuals at high risk of falls in future researches. • Future research should focus on aspects of different sleep problems to falls.
Introduction
Falls have been reported as the second cause of accidental death in humankind, a leading cause of fatal death and nonfatal injury among community-dwelling middle-aged and older adults (World Health Organization, 2021). Traumas and injuries are common after falls, and these factors can lead to fear of falling for individuals, resulting in enhanced dependence and decreased autonomy. Moreover, falls are associated with low life quality, unnecessary hospitalization for individuals, and increased financial burdens for families and societies (Florence et al., 2018; Lohman et al., 2019). One-third of individuals over the age of 65 experience falling at least once during any given year (Siegrist et al., 2016). It is reported that out of every 100 older adults over 65 years old in the United States, approximately 30–40 experience at least one falling each year; the quantity rises to 50 apparently in older adults aged over 80 (Moyer, 2012). In China, annual incidence of falls has been reported among approximately 8.6–37.1% of all middle-aged and older adults, with 60–70% of falls resulting in traumas and injuries (Kang et al., 2017; Zhang et al., 2019; Zhou et al., 2019).
Numerous risk factors have been identified to be associated with falls among middle-aged and older community dwellers, such as demographic characteristics, health conditions, body strength and flexibility, medications categorized as intrinsic factors, and dwelling environment as an extrinsic factor (Pollock et al., 2012; Taylor et al., 2019). Sleep duration is one of the intrinsic factors that primarily influenced falls among middle-aged and older individuals and has been examined regarding the associations with falls in previous studies (Essien et al., 2018; Fu et al., 2019; Wang et al., 2017). However, previous results were inconsistent. For example, Essien et al. (2018) found that a short nighttime sleep duration (NSD) of ≤ 5 hours was independently associated with falls. On the contrary, Wang et al. (2017) revealed that a long NSD of ≥ 10 hours was associated with an increased risk of a single fall compared with the reference duration of 7–8 hours. However, the long NSD lost its significance after controlling for age, sex, and sleep-related variables; meanwhile, the short NSD of ≤ 7 hours was unassociated with falls at all. Interestingly, Fu et al. (2019) examined the relationship between NSD and falls and reported that the occurrences of falls within the < 7-hour group and > 9-hour group were higher than within the 7–8-hour group (Fu et al., 2019).
The possible explanation for the inconsistent results in previous studies is that NSD may be broad and do not portray a single entity. Other intrinsic factors, such as physical activity (PA), cognitive function, body pain, and depressive symptom, can be associated with falls and should be considered. Lower body weaknesses, resulting from lack of PA, cognitive impairment, and body pain, are potent fall risk factors and frequently associated with gait abnormalities (Cai et al., 2020; Carrasco et al., 2020; Morris & Lewis, 2020). Among previous studies that investigated falls among postmenopausal women, depression was reported to be associated with poor postural stability, which could result in additional falls (Hita-Contreras et al., 2018; Zhou et al., 2021). In addition, gender-specific differences in NSD could not be ignored. Kuo et al. (2010) conducted a study targeting gender-specific association between self-reported sleep duration and falls in older adults of ≥ 65 years old, and reported that sleep deprivation was independently associated with falls in women but not in men. To the best of our knowledge, gender-specific association between NSD and falls among middle-aged and older adults in China is yet to be investigated. Therefore, we hypothesized that middle-aged and older adults with a short NSD (≤5 hours per day) would have a high occurrence of falls, and the association would be different between male and female.
Material and Methods
Participants
This research was conducted using the data from 2015 China Health and Retirement Longitudinal Study (CHARLS), a nationally longitudinal survey aiming at investigating and evaluating the aging issue in China, which was conducted by Institute of Social Science Survey of Peking University. Data are publicly available and can be downloaded directly from the official website: http://charls.pku.edu.cn/en. China Health and Retirement Longitudinal Study started in 2011 and is updated every 2 years, thus covering 150 country-level units distributed in 28 provinces of China, which include assessments of social, economic, and health conditions of community populations. Ethical approval was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015) (Zhao et al., 2014). Participants were fully informed of the purpose of the study and signed written informed consent to participate. Currently, the CHARLS survey has released data from waves 1 to 4. CHARLS wave 4, which was released in 2018, had only released partial data, excluding anthropometric measurements, such as body mass index (BMI). Therefore, we conducted a survey using data from 2015 CHARLS survey (wave 3), which involved 22,899 respondents. To investigate the potential association between NSD and falls among community-dwelling middle-aged and older adults, the exclusion criteria were as follows: (a) participants aged under 45 years old (n = 1,018); (b) participants without fallen down records (n = 1,977); (c) participants with missing nighttime sleep data (n = 1,458). Finally, a total of 18,446 individuals were included in this study.
Measurements
Falls were collected as “yes” or “no” by asking the question “Have you fallen down?” for a new participant and “Have you experienced falls since the last interview date?” for a reinterview respondent. Individuals were classified as “fall” and “no fall” on the basis of their responses.
Nighttime sleep duration was assessed by asking the question “During the past month, how many hours of actual sleep did you get at night (average hours for one night)?” It was recorded as an integer. Nap was defined as “yes” if respondents took a nap after lunch for more than 30 minutes. Sleep disturbance was evaluated by asking the respondent to rate the following question “My sleep was restless.” Answers had four categories included < 1 day, 1–2 days, 3–4 days, and 5–7 days.
Confounding variables, including demographic characteristics, lifestyle items, functional statuses, and health statuses were collected and analyzed in this study. BMI was calculated as current weight in kilograms divided by the square of height in meters. Cognitive function was calculated using the Telephone Interview of Cognitive Status (TICS), which included word recall test and the ability to redraw a picture (Bai et al., 2021). The sum of correct answers and completing pictures ranged from 0 to 21, and a high score indicated good cognitive function. PA contained the amount of time a person spent on vigorous activities, moderate activities, and walking in a usual week. According to the responses, we indexed the amount of PA per day as 1 (<0.5 h), 2 (0.5–2 h), 3 (2–4 h), and 4 (>4 h). The weekly PA duration score was calculated by multiplying the number of days and the daily PA duration index for each activity. Finally, we generated the variable of PA score using metabolic equivalent (MET) multipliers as follows: PA score = 8.0*total vigorous activity weekly duration score + 4.0*total moderate activity weekly duration score + 3.3*total walking weekly duration score (Deng & Paul, 2018). Depressive symptoms were assessed by the Center for Epidemiologic Studies Depression (CES-D-10) Scale, which comprised 10 items. Each of the four-option response to the item was scored ranging from 0 to 3, and the total score was the sum of points for all 10 items. A total score of 10 or higher indicated the presence of clinical depression (Lin et al., 2021). Other variables and detailed information are present in Supplementary Table 1.
Statistical Analysis
Continuous and categorical variables were analyzed through descriptive analyses to explore participants’ characteristics. In our empirical study, fall incidence was 17.0%, thus odds ratios may overestimate relative risks (Andrade, 2015), so we used a generalized linear model to analyze associations between NSD and falls. One-factor logistic regression models were then used to estimate odds ratios and 95% confidence intervals (CI) for the study association. Restricted cubic spline (RCS) was used to investigate and display the possible dependency of associations between NSD and falls by setting five knots. We assumed data were missed at random. The multiple imputation by chained equations (MICE) of missing values was used, and results before and after imputation were compared (White et al., 2011). Outliers were tail-reduced to preserve sample features to the greatest extent. Thereafter, several models, including a crude model that used data before multiple imputation, and five other models were established to assess associations between NSD and falls. Finally, nomogram was employed to display the contribution degree of each factor in the model to the outcome variable. It made prediction model results more readable than before. Date management and analysis were carried out using R 4.1.0 statistical package for the social sciences for Windows. All tests were performed two-tailed with a significant level of p < .05.
Results
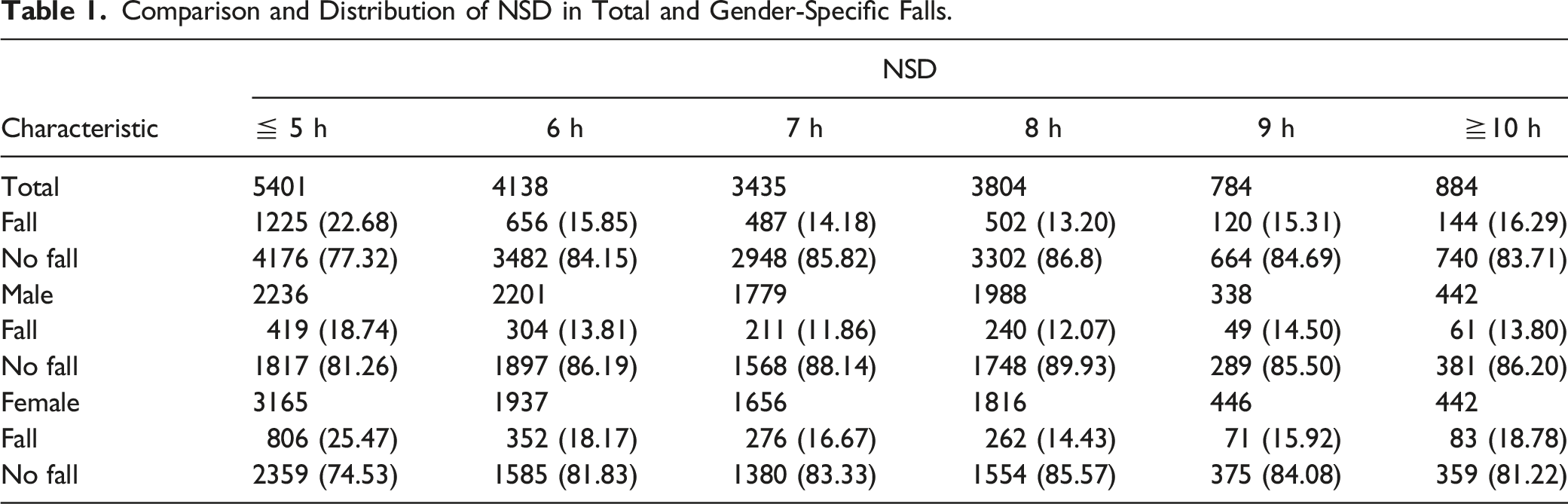
Of the 22,899 respondents in 2015 CHARLS, 18,446 were eligible and 8,984 (48.70%) were male. Among the total population, 3,144 (16.99%) had more than a single fall. Descriptive data are displayed in Supplementary Table 2. The mean NSD in the fall group was (5.96 ± 2.11) hours per 24-hour period and significantly different from that in the no fall group (p < .001), which was (6.46 ± 1.89) hours. Other parameters were all significantly different between the fall group and no fall group (p < .05), except for BMI and nap time.
With regard to gender-specific falls, 1,284 (16.99%) in men and 1,850 (19.55%) in women had more than a single fall. Nighttime sleep duration, frequency of restless sleep, and other parameters, including age, education status, living area, cognition function, instrumental activities of daily living scale (IADLS) difficulty, PA, memory, eyesight, hearing, depression, body pain, self-reported health (SRH), and chronic disease, were all significantly different between the fall group and no fall group in both male and female populations (p < .05). However, BMI was only significantly different between the fall group and no fall group in the male population (p < .001), whereas marital status, alcohol use, and nap time were solely significantly different between the fall group and no fall group in the female population (p < .001).
Comparison and Distribution of NSD in Total and Gender-Specific Falls.
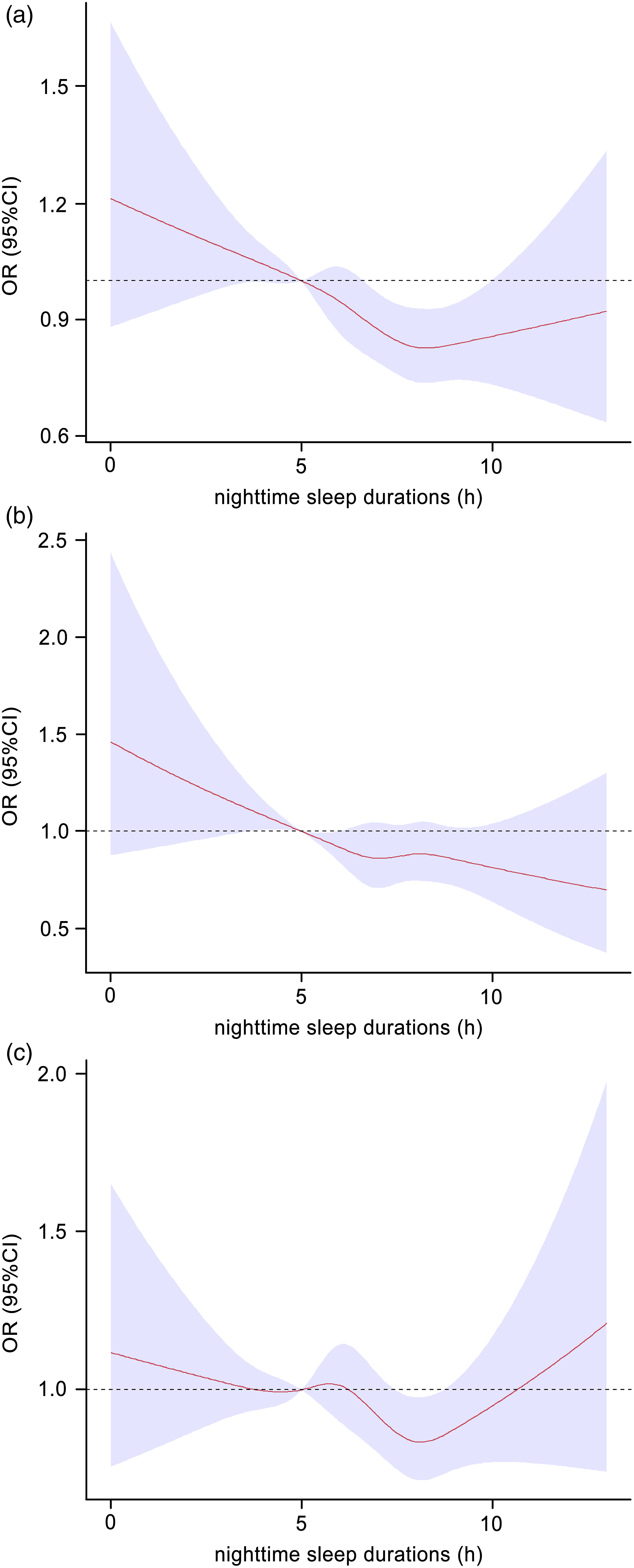
Associations between NSD and falls among the total (1a. n = 18,446), male (1b. n = 8984), and female (1c. n = 9462) populations.
Multiple Logistic Regression of Factors Influencing Falls among Community-Dwelling Middle-Aged and Older Adults.
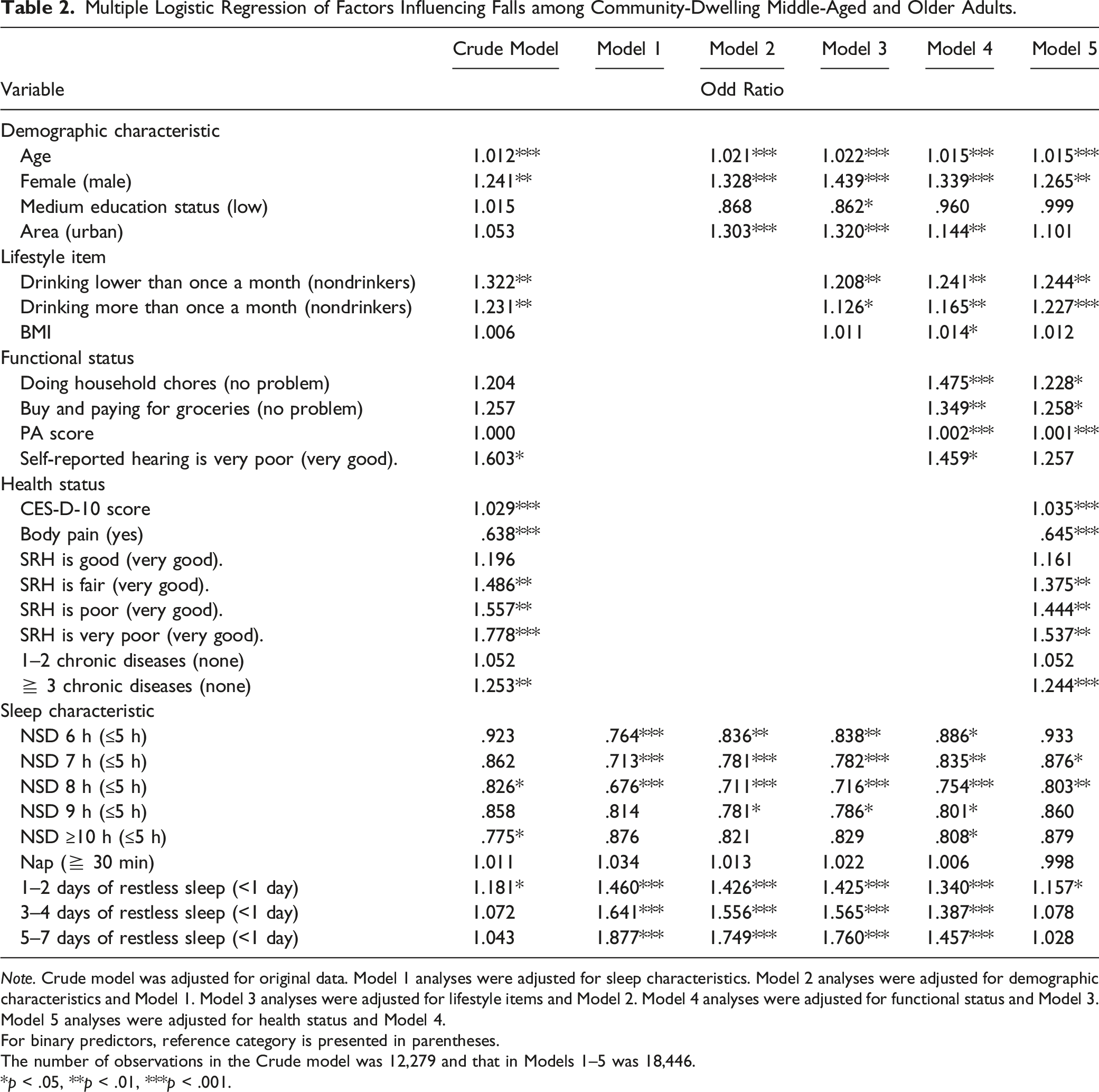
Note. Crude model was adjusted for original data. Model 1 analyses were adjusted for sleep characteristics. Model 2 analyses were adjusted for demographic characteristics and Model 1. Model 3 analyses were adjusted for lifestyle items and Model 2. Model 4 analyses were adjusted for functional status and Model 3. Model 5 analyses were adjusted for health status and Model 4.
For binary predictors, reference category is presented in parentheses.
The number of observations in the Crude model was 12,279 and that in Models 1–5 was 18,446.
*p < .05, **p < .01, ***p < .001.
Discussion
To our knowledge, this study is the first to comprehensively explore gender-specific association between NSD and falls among middle-aged and older adults in China. We demonstrated that Short and long NSD were associated with high occurrences of falls in the total and female population, an approximately “U-shaped” dose-response association in RCS analysis; however, only short NSD was associated with a high occurrence of falls in the male population, which was a nearly linear association in RCS analysis. These associations remained significant in multiple analysis after controlling for demographic characteristics, lifestyle items, functional statuses, and health statuses. Furthermore, parameters such as age, education status, living area, drinking status, BMI, IADLS, PA, hearing, depressive symptom, SRH, chronic disease, and restless sleep were significantly associated with falls in different models using multiple logistic regression.
Sleep duration has been found to be associated with falls; however, evidence in literature is mixed with some agreeing an association between short sleep duration (<7 h) and falls exists (Essien et al., 2018; Lee et al., 2021; Ma et al., 2017), some suggesting an association between long sleep duration (≥9 h) and falls exists (Kim et al., 2016; Wang et al., 2017), and others demonstrating that short and long sleep durations are associated with falls (Fu et al., 2019; Helbig et al., 2013). Our study showed that Short and long NSD were positively associated with falls in the total population, which confirmed the results of Fu et al. (2019) and Helbig et al.’s (2013) studies. Although the mechanisms have not been thoroughly elucidated, plausible reasons were proposed in prior studies. Han et al. (2021) demonstrated that probable rapid eye movement sleep behavior disorder can interact antagonistically with sleep insufficiency in additive and multiplicative scales to influence fall risk. Racial diversity is another worth noting risk factor for association with falls. Asian populations have an increased likelihood of short sleep duration, whereas other populations likely have long sleep duration; hence, the association of long sleep duration and falls are more pronounced among other populations than Asian populations (Wu & Sun, 2017).
Our study also found that gender was an independent factor, and its impact on falls differed from male to female. Short and long NSD were associated with high occurrences of falls in the female population, but only short NSD was associated with high fall risk in the male population. Kuo et al. (2010) conducted a gender-specific analysis to assess the association between sleep duration and falls and found that short sleep duration was an independent fall risk factor in women but not in men. Note that a significant number of women, with the percentage of 40–60%, would suffer from poor sleep quality or insomnia during their menopausal transition (Shaver & Woods, 2015), which may be caused by the decrease in estrogen level and sclerostin loss (Serrano-Checa et al., 2020). One explanation for the gender-specific differences can be that some behaviors and lifestyle factors may affect muscle strength performance differently in men and women (Zhang et al., 2022). For example, sleep quality is positively correlated with grip strength in men, but not in women (Zhang et al., 2021). Another explanation is that women in this age are in menopausal transition or postmenopausal period and may suffer from poor sleep quality, depression, insomnia or osteoporosis (Shaver & Woods, 2015; Zhou et al., 2021).
As healthy older adults go through aging, they exhibit a temporally advanced sleep phase (falling asleep early and waking up early) (Patel et al., 2018). Sleep complaints are common in older adults. Sleep problems primarily refer to nighttime sleep problems, which contain various symptoms, such as trouble in falling asleep, trouble in waking during the night, daytime sleepiness, and poor sleep quality. Our results revealed that 1–2 days of restless sleep per week compared with < 1 day was positively correlated with falls. We thought it might be due to the prevalence of widespread sub-health state and interactions with other covariates, which we did not analyze. Further understanding of the relationship between sleep duration and disturbance and falls sheds light on designing evidence-based preventions and interventions targeting at this vulnerable population. Depression was also accounted for the associations between sleep duration and falls in this study. Insomnia is one of the symptoms of depression. Previous investigation demonstrated that the presence of depressive symptom can mediate association between self-reported sleep quality and falls among older adults (Liu et al., 2021), for which taking antidepressants may be a possible explanation. Antidepressants may affect orthostatic hypotension, sedation, and cognitive functioning, which have effects on postural control and consequently lead to falls in the older adults (Jung et al., 2022). Body pain and SRH also strongly increased occurrences of falls in this study. Various sleep problems are significantly associated with pain in patients suffering from chronic pain (Keilani et al., 2018). Association between self-reported sleep duration and poor health may be due principally to confounding or reverse causality whereby sicker people spend more time in bed or need more sleep precisely due to their sickness (Cauley et al., 2019). According to Kim et al. (2020), older adults may fail to complete physical assessment tests due to weak muscle strength, joint pain, and cognitive emotional comorbidities. Thus, the SRH assessment or questionnaire can be an alternative tool for older individuals who cannot perform physical test that assess fall risks. Based on the investigation by Cepeda et al. (2016), subjects with poor health statuses reported having 46 min per day (95% CI from −56.85 to −35.67) less than those with excellent health statuses in sleep duration. A difference of 30 minutes of sleep is associated with a substantive change in clinical well-being. Chronic disease can directly increase fall risks because of themselves; meanwhile, they can contribute to frailty and prolong bedridden time to increase fall risks in middle-aged and older adults additionally. Kao et al. (2012) reported that the presence of symptoms combined with chronic disease results in a four- to nine-fold increase in fall risks. Taking liquors likely causes falls. In addition, alcohol-related falls can require more management and treatment than nonalcohol-related falls due to intoxication; the resulting decrease in psychomotor functioning and the behavior of intoxicated patients are often present (Woods et al., 2019).
The study has several limitations that should be acknowledged. First, it was cross-sectional, and drawing conclusions about causality was difficult. Notwithstanding, we adjusted for important fall risk factors, including mental status, chronic disease, and PA. Second, NSD and falls were reported by participants themselves, which may suggest interviewee recall bias inevitably. However, self-reporting to obtain sleep duration may be the only viable way when a large number of subjects are included, which has been used to analyze associations between sleep durations and falls in prior studies. With respect to falls, Ganz et al. (2005) found that retrospective recall falls have similarly high sensitivity and specificity compared with criterion-standard prospective assessments using some form of ongoing fall monitoring. Third, we were unable to use the latest data due to the latency of the CHARLS data release. However, we will continue to track the results of newly released data and report back in due course.
Conclusions
In summary, our study showed that NSD was strongly and significantly associated with the occurrence of falls. Approximately “U-shaped” dose–response associations in the total and female population were observed, but only a nearly linear association was found in the male population. Also, a robust procedure adjusting for a complex survey design in a large sample was used. Exploring the mechanisms of gender differences in association between NSD and falls and furtherly increasing targeted, evidence-based and gender-specific preventions for NSD and sleep disturbance among primary care interventions are necessary to prevent falls among community-dwelling middle-aged and older adults in China.
Supplemental Material
Supplemental Material - Gender-Specific Association Between Nighttime Sleep Duration and Falls Among Community-Dwelling Middle-Aged and Older Adults in China
Supplementary Material for Gender-Specific Association Between Nighttime Sleep Duration and Falls Among Community-Dwelling Middle-Aged and Older Adults in China by Nan Zhang, Cui Wang, Yuli Li, Mei Yang, Jing Yang, Fenghui Chen, and Ping Yan in Journal of Applied Gerontology
Footnotes
Acknowledgments
All authors thank the CHARLS for providing data. We are grateful to those who designed, conducted, and participated in this study. We thank Professor Jia Guo from Xiang Ya School of Nursing, Central South University, for providing guidance in the manuscript writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Xinjiang Medical University doctoral research start-up grant.
Ethical Approval
This work was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015).
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.