
Abstract
Negative social evaluations about aged-care work continue to discredit those who perform this type of work. Drawing on ‘dirty work’ literature from the field of management and stigma theory from the field of psychology, this study examines occupational stigma in the context of aged-care work and its relationship with negative outcomes for people who work in aged care. Findings from a path analysis revealed that aged-care workers (n = 185) who ascribe occupational taints and poor occupational conditions with aged-care work perceive aged-care work as being stigmatized, and in turn, are more likely to internalize this stigma. Through this process of perceiving and internalizing occupational stigma, aged-care workers experience greater psychological distress, job dissatisfaction, and turnover intentions. This research fills a void within the gerontology literature regarding the psychological processes underlying how occupational stigma may come to negatively impact this workforce. Findings offer practical implications for policy reform and managerial training.
Keywords
• This study is the first to find quantitative support for the relationship between occupational taints/occupational conditions in aged-care work and aged-care worker outcomes. • Aged-care workers who perceive heightened stigma associated with aged-care work may internalize these negative evaluations. • People who work in aged care experience adverse psychological and job outcomes when they perceive and internalize the stigma surrounding aged-care work.
• Policy reforms for improving aged-care work require a targeted approach to address poor occupational conditions and practices associated with occupational taint. • The aged-care workforce may benefit from training for ongoing stigma management.What this paper adds
Applications of study findings
People who work in aged care may ascribe occupational stigma surrounding their work to themselves (Ostaszkiewicz et al., 2016). In line with the ‘dirty work’ literature (Ashforth & Kreiner, 1999) from the field of management, we define occupational stigma as negative social evaluations that discredit people who engage in ‘dirty work’—occupations perceived to be tainted because they involve working with human waste, death, and socially marginalized groups. We argue that aged-care work can be perceived by some as ‘dirty work’ (see Manchha et al., 2022). Subsequently, the aged-care workforce is at risk of experiencing negative consequences associated with occupational stigma (Ashforth & Kreiner, 2014). Accordingly, previous work shows that aged-care workers report that they are perceived and treated more negatively by others because of their work (Manchha et al., 2021). However, little quantitative research has examined the nature and psychological processes through which occupational stigma surrounding aged-care work may predict detrimental worker outcomes.
This study examines occupational stigma in the aged-care work context. Specifically, we test whether perceiving occupational stigma is associated with the internalization of this stigma, and whether internalized stigma can predict worker outcomes of psychological distress, job dissatisfaction, and turnover intention. With the findings from this study, we strive to fill a void within the gerontology literature and help inform strategies to support aged-care workers with managing the stigma of working in aged care.
Antecedents of Stigma Associated with Aged-Care Work
‘Dirty work’ researchers have traditionally examined antecedents of occupational stigma in terms of occupational taint. Occupational taint refers to characteristics that may blemish people working in a particular occupation in the eyes of others (Ashforth & Kreiner, 2014). The literature proposes that there are three types of occupational taint—physical taint refers to the idea that the occupation involves tasks dealing with dirt, bodily functions, or death, social taint refers to the idea that the occupation involves affiliating with or working with entities who may belong to marginalized social groups, thereby reducing a worker’s social standing, and moral taint refers to the idea that the occupation involves tasks deemed as morally questionable (Ashforth & Kreiner, 2014). Researchers have theorized that when an occupation is perceived as tainted in any of the above ways, society will come to view both the occupation, and those working in the occupation, in a stigmatized way.
Aged-care work has been linked to occupational taint in existing qualitative studies (Banks, 2018). First, aged-care workers often perceive physical taint in their work because it requires contact with bodily functions and handling human waste (e.g., incontinence care; Ostaszkiewicz et al., 2016). They also may perceive social taint, given that aged-care work involves working with people (e.g., residents and co-workers) who may belong to social groups that experience discrimination based on negative age and race-based stereotypes (Clarke & Ravenswood, 2019). Finally, the aged-care industry is frequently and publicly reported to engage in unethical practices (e.g., elder abuse, unregulated institutions that may infringe on the rights of older adults; Hodroj et al., 2022). The existing composition of aged care, with its poorly regulated governance, may systemically foster inadequate care and neglected residents (Hart et al., 2021). Thus, some aged-care workers may also perceive their work is associated with moral taint. The more aged-care workers feel that their work is associated with physical, social, or moral taint, the more they may perceive that their occupation is stigmatized by society.
Beyond occupational taint, we further argue that poor occupational conditions in aged care, such as pay and resource disparity (e.g, registered nurses in aged care earned 10% less than registered nurses in the acute sector in Australia; Tune, 2017), may contribute to the stigmatized image of aged-care work (Choi et al., 2020). We argue that these poor occupational conditions may signal to aged-care workers that their work is socially devalued (Manchha et al., 2021). Based on the literature above, we propose that greater perceptions of physical taint, social taint, moral taint, and poor occupational conditions will be associated with greater perceived occupational stigma.
Aged-care workers’ perceptions of physical taint (H1a), social taint (H1b), moral taint (H1c), and poor occupational conditions (H1d) in aged-care work are positively associated with occupational stigma of working in aged care.
Direct effects of perceived occupational stigma on internalization of stigma
Drawing on the Four Types of Stigma Model (Pryor & Reeder, 2011), we posit that, when people who work in aged care perceive their occupation is stigmatized, they may internalize these negative societal beliefs and feelings, and reproduce this stigma themselves. Stigma scholars refer to this process as internalizing stigma, which occurs when an individual consciously or unconsciously accepts devaluation and status loss is a part of their own identity (Major et al., 2018). From this perspective, we theorize that aged-care workers may ascribe the stigmatizing negative evaluations associated with aged-care work to themselves. This can explain previous findings where people who perceived that aged-care work was devalued may feel ashamed to perform aged-care work (Hebditch et al., 2020).
Aged-care workers’ perceived occupational stigma of working in aged care is positively associated with internalized stigma of working in aged care.
Direct effects of internalized stigma on aged-care workers outcomes
Stigma literature has documented adverse consequences of stigma, including poor psychological wellbeing (Major et al., 2018), and we anticipate that people who work in aged care may experience poor psychological and job outcomes when they engage in stigma internalization—projecting the negative evaluations associated with their occupation onto themselves. For instance, workers may experience psychological distress (i.e., anxiety and depressive symptoms, Kessler et al., 2002) when they internalize ostracization and/or shame for working in aged care (Mantzorou et al., 2020). Likewise, aged-care workers may feel greater job dissatisfaction when they accept negative perceptions about their job (Manchha et al., 2021). This psychological distress and job dissatisfaction may also be reflected in greater turnover intention (i.e., intentions to leave their job; Booi et al., 2021). Gao and colleagues (2015) found nursing assistants were more determined to leave aged care when they felt “less than.” Thus, we predict that workers who have internalized the stigma of their work may experience greater psychological distress, job dissatisfaction, and turnover intentions.
Internalized stigma is positively associated with aged-care workers’ psychological distress (H3a), job dissatisfaction (H3b), and turnover intention (H3c).
The mediating role of perceived occupational stigma and internalized stigma
No study has directly examined how occupational stigma comes to negatively impact the aged-care workforce. Building on the previous sections, we argue that people who work in aged care may experience poor psychological and job outcomes because of the occupational taints, poor occupational conditions, and resultant stigma associated with their job (which they have internalized). Specifically, workers may experience greater psychological distress, job dissatisfaction, and turnover intention as a result of perceiving and internalizing the stigma attributed to aged-care work. Thus, we hypothesize that perceived occupational stigma and internalized stigma are serial mechanisms through which perceived occupational taints and poor occupational conditions predict psychological distress, job dissatisfaction, and turnover intention.
Perceptions of taints and poor occupational conditions indirectly predicts workers’ psychological distress (H4a), job dissatisfaction (H4b), and turnover intention (H4c), through perceived occupational stigma and internalized stigma.
Our conceptual model is presented in Figure 1.
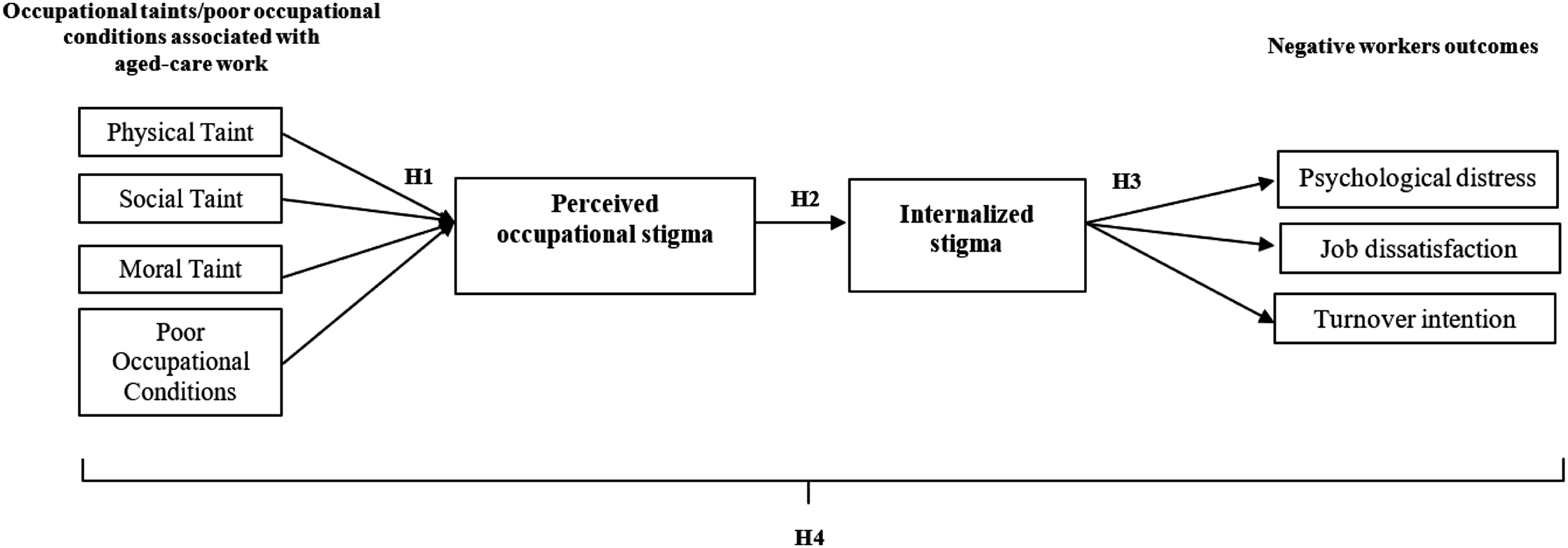
Conceptual model.
Methods
Participants and Procedure
A sample of adults who work in aged care were recruited via Prolific, an online participant recruitment platform widely used in psychological research. For the purposes of this study, we refer to the aged-care workforce as people employed to provide services to older adults in an institutional, home, or/and community context. These services may include a range of roles including personal care workers, nurses, allied health, management/administration, and auxiliary positions.
We used inbuilt Work-Industry filters on the Prolific platform to firstly identify participants who currently worked in the broader fields of “Medical,” “Health Care,” or “Social Assistance.” Targeting only these participants, we then launched a custom pre-screening survey on Prolific which enabled us to separate these participants further and identify people from this pool who currently worked in aged care (i.e., within the last 4 weeks). Participants who qualified for the study from this pre-screening process were invited to participate in the main two-part survey.
Out of the 199 participants who completed the Time 1 survey, 185 participants who completed both time points (146 females and 39 males aged 19–69, Mage=37.51, SD=10.74 years) were retained for analysis (attrition rate of 7%). Participants worked in a variety of aged-care contexts including institutional (69%), home (21%), community (7%), or other settings (i.e., retirement village, 3%); in roles involving personal care work (36%), allied health (29%), nursing (23%), management and administration (11%), and auxiliary duties (1%). Participants were from the United Kingdom (68%), United States (30%), and Australia (2%). The mean tenure and hours worked per week was 7.34 years and 33.68 hours, respectively.
Data was collected in July 2021. At Time 1, we measured participants’ perceptions of physical taint, social taint, moral taint, and poor occupational conditions, their perceived occupational stigma, internalized stigma of working in aged care, and demographic details. In order to reduce common method bias, participants were asked to report their psychological distress, job dissatisfaction, and turnover intention at Time 2, one week later. This study was granted ethics approval by the Human Research Ethics Committee of The University of Queensland. Participants gave written consent to engage in this study.
Measures
Aged-Care Work-Related Questions
Before completing the main measures, participants were presented with a brief definition that aged-care work referred to work where one “provides services to older people (aged 65 and older).” Participants were asked to respond to several questions about their role in aged care and context where they worked, the results of which were presented above: “What is your current role in aged care?” (From a range of options including allied health professional, doctor, nurse, personal care worker/nursing aid/nursing assistant, management and administrative staff, auxiliary worker), “Where do you currently work?” (From a range of options including institutional, home, community, retirement village), “How long have you worked in aged care?” “How many hours do you work in aged care in an average week?”
Main Measures
Given that little extant work had quantitatively examined the stigma of aged care and job outcomes in the aged-care context, there were no existing measures of these variables that were already applied to the aged-care context. It was therefore necessary to develop purpose-built items to measure these constructs through careful consideration of the literature in this space. Where possible, items from existing measures of the broader construct were adapted and expanded for the purposes of assessing these constructs in the aged-care context (see supplementary material).
For all measures below, item responses were averaged to form an index of the construct the measure was used to capture. As can be seen from the Cronbach αs, all measures demonstrated good internal consistency. Apart from the measure of Psychological Distress, all items in each measure were responded to on seven-point Likert scales anchored from 1 “strongly disagree” to 7 “strongly agree.”
Physical Taint
A five-item scale was used to measure perceptions of physical taint in aged-care work. We adapted three items from Bickmeier (2018)’s measure of physical taint in the context of animal euthanasia to the aged-care context and added two purpose-built items to expand the scale and assess physical taint in a way that was more industry-specific to aged care (e.g., “Most people in society tend to think aged-care work is unclean”; α = .89).
Social Taint
A five-item scale was used to measure perceptions of social taint in aged-care work. We used Banks (2018) theory piece exploring the concept of social taint in aged care to develop a purpose-built scale assessing social taint in aged care (e.g., “Most people in society tend to think aged-care work involves caring for people who are less important”; α = .81).
Moral Taint
A four-item scale was used to measure perceptions of moral taint in aged-care work. We expanded on Valtorta et al. (2019)’s general measure of moral taint to develop a purpose-built scale assessing moral taint specific to aged care (e.g., “Most people in society tend to think aged-care work is unethical”; α = .92).
Poor Occupational Conditions
A six-item scale was used to measure perceptions of poor occupational conditions in aged care. These items were adapted from Chou et al. (2002) and assessed perceived occupational conditions including factors such as pay, opportunities for training, opportunities for career development, and working conditions (e.g., “I tend to think aged-care work involves unsatisfactory pay and remuneration”; α = .86).
Perceived Occupational Stigma
A twelve-item scale was used to measure perceptions of occupational stigma attached to working in aged care. These items were adapted from Boyes et al. (2013), Neville (2016), and Williams et al. (1997) and were applied to the aged-care context (e.g., “I often feel that most people treat aged-care workers with less respect”; α = .94).
Internalized Stigma
A twelve-item scale was used to measure participants’ internalization of the stigma of working in aged care. These items were adapted from Neville (2016) and Ritsher et al. (2003) and were applied to the aged care context (e.g., “I often feel embarrassed about working in aged care”; α = .88).
Psychological Distress
A six-item scale from the Kessler Psychological Distress scale (K6, Kessler et al., 2002) was used to measure participants’ psychological distress (e.g., “Over the last 30 days, I have felt so depressed that nothing could cheer me up”; α = .92). Responses ranged from 1 “None of the time” to 5 “All of the time.”
Job Dissatisfaction
A two-item scale adapted from Bowling and Hammond (2008) was used to measure participants’ job dissatisfaction (e.g., “I am satisfied with my job.” [reversed scored]; α = .81).
Turnover Intention
A three-item scale was used to measure participants’ intentions to leave their job in the aged-care sector. We adapted these items from Fried et al. (1996)’s measure of turnover intentions to make them specific to the aged-care context (e.g., “I have seriously thought about leaving the aged-care sector”; α = .87).
Analysis
We conducted a series of path analyses using AMOS to examine the effects between hypothesized predictors and outcomes as proposed in the conceptual model (Figure 1). Model fit was considered acceptable if the chi-square (χ2) test was non-significant, and if the χ2/df-ratio was below 2, the Comparative Fit Index (CFI) was above 0.95, the Root Mean Square Error of Approximation (RMSEA) was below 0.06, and the Standardized Root Mean-square Residual (SRMR) was below 0.08 (Hu & Bentler, 1999). The initial model tested only the paths depicted in the conceptual model. Modification indices were used to determine whether other theoretically-viable paths could be freed to improve model fit. We employed the bias-corrected bootstrapping method (Fritz & MacKinnon, 2007) to test indirect effects of perceived occupational taints/poor occupational conditions on workers outcomes through perceived occupational stigma and internalized stigma.
Results
Means, Standard Deviations, and Zero-Order Correlations Among the Hypothesized Predictors and Outcomes.
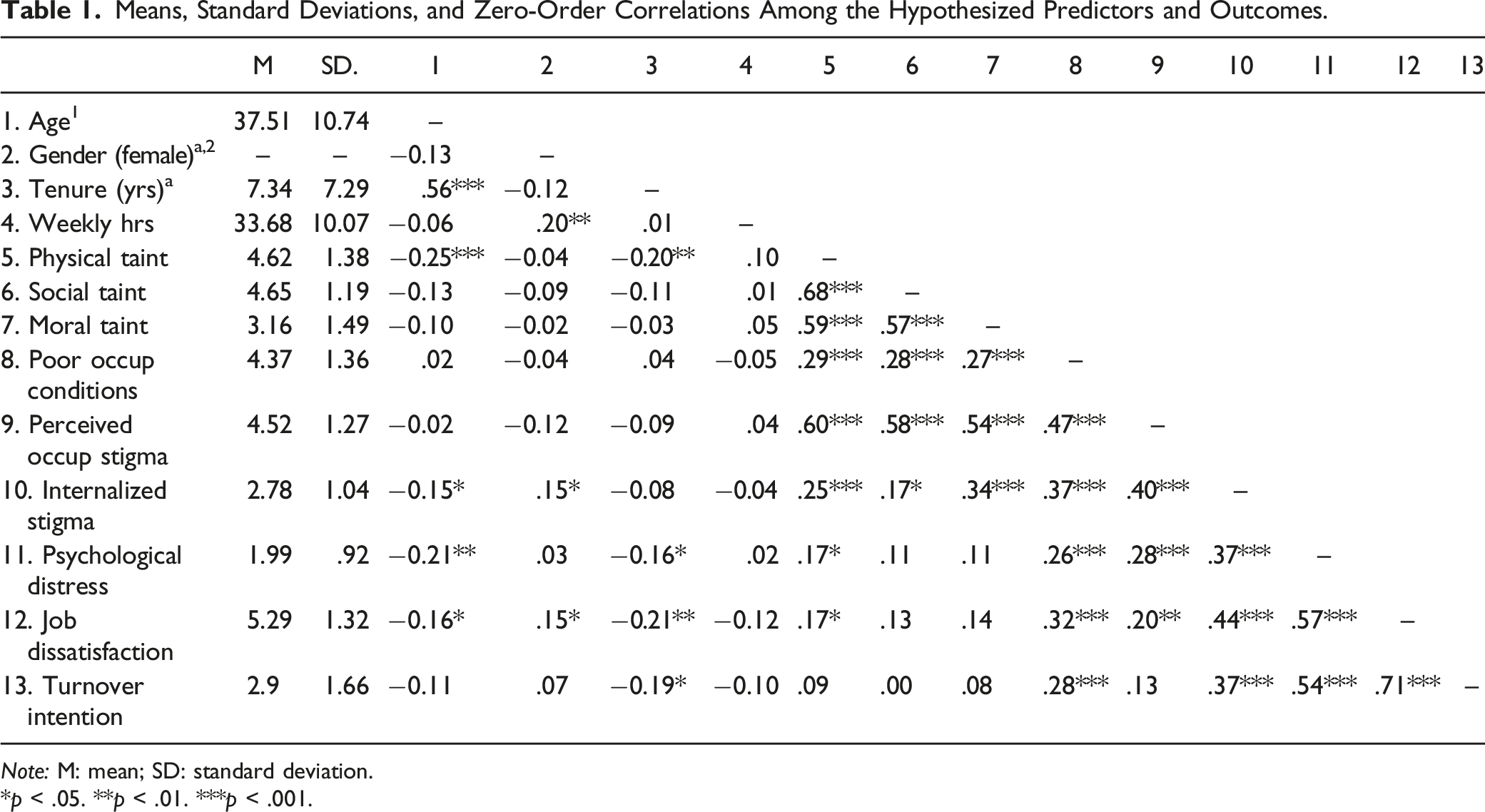
Note: M: mean; SD: standard deviation.
*p < .05. **p < .01. ***p < .001.
The initial fit of the path model containing only the paths depicted in the conceptual model (Figure 1) was poor, χ2 (22) = 86.41, p < .001, χ2/df-ratio = 3.93, CFI = 0.52, RMSEA = 0.13 [0.10, 0.16], SRMR = 0.14. Given that all predictor variables (i.e., physical taint, social taint, moral taint, occupational conditions) were theoretically related (Ashforth & Kreiner, 2014), covariances were freed between them. Likewise, covariances were freed between the outcome variables (i.e., psychological distress, job dissatisfaction, turnover intentions; Nelson et al., 2021). Inspection of the modification indices revealed direct paths between (a) poor occupational conditions and internalized stigma, and (b) perceived occupational stigma and psychological distress, which could be freed to improve model fit. These paths were theoretically justifiable, given that (a) recognition of one’s poor occupational conditions could directly lead to the internalization of negative sentiment about one’s job, and (b) perceiving a societal stigma surrounding one’s occupation could directly induce psychological distress. Thus, both paths were freed. Our final model (Figure 2) demonstrated good fit, χ2 (17) = 22.53, p = .165, χ2/df = 1.33, CFI=0.96, RMSEA=0.04, and SRMR=0.04. Direct and indirect effects observed in the path model. Note *p < .05, **p < .001.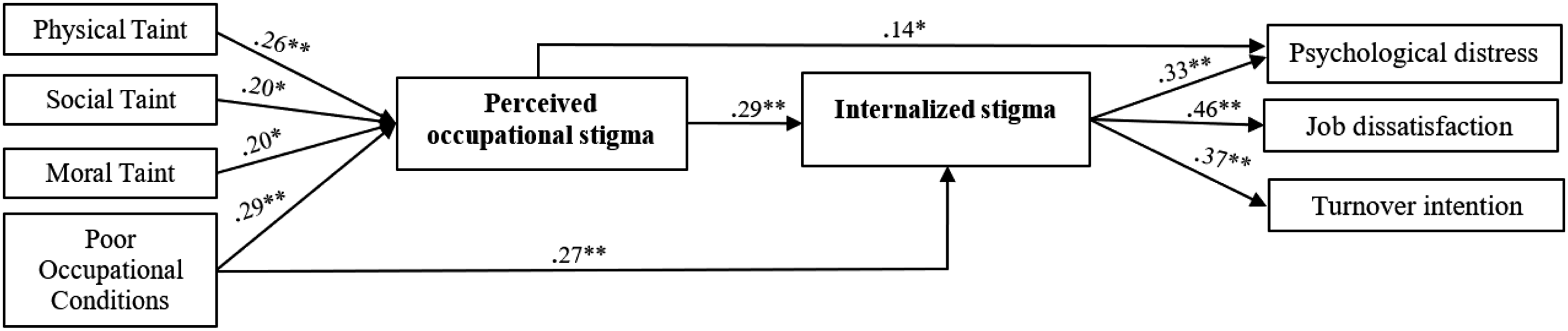
Direct Effects
We found support for Hypothesis 1(a)–(d). Higher perceived physical taint (β = .26, p = .001), social taint (β = .20, p = .006), moral taint (β = .20, p = .003), and poor occupational conditions (β = .29, p < .001) significantly predicted greater perceived occupational stigma of working in aged care. Hypothesis 2 was also supported, as greater perceived occupational stigma significantly predicted greater internalized stigma (β = .29, p < .001). Supporting Hypothesis 3(a)–(c), greater internalized stigma significantly predicted greater psychological distress (β = .33, p < .001), job dissatisfaction (β = .46, p < .001), and turnover intention (β = .37, p < .001). As aforementioned, two unpredicted direct paths also emerged. First, poorer perceived occupational conditions directly predicted greater internalized stigma (β = .27, p = .002). Second, greater perceived occupational stigma directly predicted greater psychological distress (β = .15, p = .018).
Indirect Effects
Indirect Effects of Perceived Taints/Occupational Conditions on Workers Outcomes.

Standard Errors (SE) are listed in parentheses and Confidence Intervals (CI) in square brackets. All coefficients are bootstrapped 95% CI. Significant effects appear in bold type.
Discussion
This study examines occupational stigma in the aged-care context. Drawing on the “dirty work” literature (Ashforth & Kreiner, 2014) we investigate occupational taints as part of a robust theoretical framework for understanding the nature of occupational stigma associated with aged-care work. Findings from this study uncovered relationships between occupational taints (e.g., physical taint, social taint, moral taint) and the stigma of aged care, which have previously only been reported in qualitative literature (Clarke & Ravenswood, 2019; Ostaszkiewicz et al., 2016). The more workers perceived that aged-care work was physically tainted (e.g., construed as ‘unclean,’ ‘foul,’ and ‘disgusting’; Ostaszkiewicz et al., 2016), socially tainted (e.g., involved for people who are less capable, or frail; Clarke & Ravenswood, 2019), and morally tainted (e.g., associated with unethical behaviors; Manchha et al., 2022), the more they perceived the occupation to be stigmatized. This study found empirical support for moral taint as a basis for perceptions of occupational stigma surrounding aged-care work. Findings suggest that workers are cognizant of the stereotypes related to unethical behaviors in aged care (Manchha et al., 2021), and suspect that these evaluations may ascribe moral taint to aged-care work.
Additionally, we introduced poor occupational conditions into our model based on existing literature in gerontology (see Choi et al., 2020) which argue that working conditions surrounding the provision of aged care continue to devalue this work and those who perform aged-care work. In line with this body of literature, we found that workers perceived poor occupational conditions (e.g., limited financial rewards) reinforced status loss associated with aged care (Hebditch et al., 2020). Thus, poor occupational conditions can also be construed as a driver of perceived occupational stigma in the aged-care context.
It should be noted that this data was collected during COVID-19. We recognize that COVID-19 has highlighted poor working conditions in the aged-care industry. Throughout the pandemic, aged-care workers have experienced chronic understaffing, heavy workloads, and inadequate remuneration (McGilton et al., 2020). This calls attention to systemic issues that may reinforce the undesirable qualities of aged-care work.
Another novel finding from our study was that aged-care workers applied the occupational stigma surrounding their work to themselves. This process, known as internalizing stigma, involves a person experiencing diminished self-worth as a result of perceiving that they are stigmatized by society (Pryor & Reeder, 2011). As predicted, we found that aged-care workers who perceived that working in aged care is a shortcoming also projected negative evaluations about aged-care work onto themselves. Internalized stigma was, in turn, a predictor of psychological distress and adverse job consequences (e.g., job dissatisfaction, turnover intentions). The heightened psychological distress, job dissatisfaction, and turnover intentions may have negative implications for broader workforce challenges in the aged-care industry (e.g., attracting and retaining workers). For example, high turnover rates are linked to shortages in the provision of aged care as well as greater job stressors and decreased morale (Nelson et al., 2021).
In addition to the effects hypothesized, we found that occupational stigma may reduce workers’ psychological wellbeing without necessarily requiring internalization of the stigma. For instance, people may suffer psychological distress as a result of simply being aware of the social devaluation related to aged-care work and worrying others will devalue them (Mantzorou et al., 2020). This direct relationship did not emerge for job dissatisfaction or turnover intentions, suggesting that aged-care workers may only develop dislike for their work and desire to leave if they have internalized the stigma.
Findings also revealed a significant direct relationship between poor occupational conditions and internalized stigma. This is evident in how poor occupational conditions make social inequalities surrounding aged-care work more salient; for instance, people employed in aged care were required to work without access to personal protective equipment even 2 months into COVID-19 (Manchha et al., 2022). Consequently, workers may feel disempowered when they recognize their working conditions are subpar (Ostaszkiewicz et al., 2016), leading them to internalize the stigma of aged-care work. The present work unearthed quantitative evidence for these relationships.
Implications
This study employed a multi-disciplinary approach through integrating research from the field of management (Ashforth & Kreiner, 2014) with stigma research from the field of psychology (Pryor & Reeder, 2011) to introduce a novel framework for examining the nature of occupational stigma in the aged-care work context. This perspective enabled us to fill a void in the gerontology literature in two ways. First, we drew on the “dirty work” literature as a principled approach to conceptualize multiple occupational taints, which allowed us to test a breadth of distinct drivers of stigma associated with aged-care work. Second, we employed mechanisms from stigma research to explain how psychological processes underlying stigma can negatively impact workers’ outcomes.
This study offers practical implications for managing this stigma in terms of policy reform and managerial training. From a structural level, findings suggest that effective policy reforms should target addressable problems, such as those to do with occupational conditions and moral taint. For example, policies could focus on enhancing client quality and safety care standards, through ensuring adequate remuneration, training, and opportunities for career advancement, as these factors are prototypical of poor occupational conditions (Manchha et al., 2022). We also note that, although moral taint is sometimes unjustified when applied to workers who do not engage in immoral or unethical practices (Hodroj et al., 2022), the attribution of moral taint to aged-care work may sometimes be a legitimate reflection of the existence of such practices. Thus, policies focusing on mitigating these practices (e.g., elder abuse) may help reframe negative societal perceptions about aged-care workers’ ethics and hence, moral taint associated with aged-care work.
Managerial training may also establish and sustain ongoing stigma management, given that certain bases of the stigma of working in aged care, such as physical taint, may be more difficult to change due to the nature of the work. Training could provide access to resources and coaching to leaders about effective ways to propagate messages that champion the positive qualities of aged-care work. In turn, this may help assist workers with reframing negative stereotypes that are typically internalized. Collectively, the strategies above may help address the ongoing attraction and retention issues in the field of aged care (Manchha et al., 2022).
Limitations
We acknowledge several limitations of this study. First, we included aged-care workers in a variety of different roles to test our proposed model. This was necessary, given that our convenience sampling method produced low numbers of aged-care workers in each of the roles. This was also strength, allowing us to test our model using aged-care workers from many occupations. The underrepresentation of people working in each type of role, however, precluded analyses testing for differences across them. It is possible that the effects observed in this study may be stronger or weaker for aged-care workers as a function of their specific occupation or context. Future research should recruit higher numbers of aged-care workers in these different roles to examine whether type of aged-care work or work environment influences the stigma processes observed in this paper.
For example, those who work in areas like allied health or in management roles may not perceive that their specific jobs are associated with physical taint (e.g., human waste, death), or may recognize that their occupations are afforded higher status than those working in other aged-care roles. This may protect them, somewhat, from the negative consequences of stigma relative to those in other aged-care roles. We note, however, that participants who carry out their allied health or management tasks in an aged-care environment or for clients in aged care may still feel as though they are performing less valued work as a function of other processes, including social taint (which can not only be derived from working with the stigmatized population of older adults, but also from working with the stigmatized population of other aged-care workers). Indeed, previous research shows that even allied health professionals outside the aged-care workforce recognize the stigma that comes from working in institutional aged care and are therefore motivated to avoid it (Manchha et al., 2022).
Also, several variables in this study were measured with purpose-built scales due to the lack of existing scales fit for the purpose of examining stigma in the aged-care context. It should be noted, however, that the items used were high in face validity and tests of internal consistency (i.e., Cronbach’s α) showed that all scales were highly reliable. Furthermore, the findings derived using these scales were consistent with our theorizing and align with recent work examining the stigma of aged care that has used similar approaches to constructing scales to measure stigma processes in aged care (e.g., Manchha et al., 2022). Nevertheless, future research should focus on developing and validating a new measure to capture these variables (e.g., occupational taints) as they play out in the aged-care context.
Agenda for Future Research
Researchers can extend this study’s findings through exploring factors that could protect workers from experiencing the negative consequences of stigma. For example, stigma management strategies such as normalizing stigma, shifting attention to non-stigmatized aspects of aged-care work, developing occupational pride or a positive sense of occupational identity to improve a sense of self (Ashforth & Kreiner, 2014) could be explored. Further investigations may involve understanding the conditions under which these strategies strengthen/weaken the relationship between occupational stigma and workers outcomes. Future studies may employ an experimental study design to test occupational pride or identity variables.
Also, the present study conceptualized turnover intention as a negative and undesirable outcome for aged-care workers due to its traditional associations with job dissatisfaction and poor psychological wellbeing (Bowling et al., 2010; Harrison et al., 2006; Woznyj et al., 2022). We acknowledge that although turnover intention is often traditionally framed as a negative outcome in the literature, changing jobs and/or industries, particularly away from one that is heavily stigmatized, may offer benefits to workers (e.g., personal development, career progression). Future studies should therefore explore both the negative and positive implications of leaving a stigmatized occupation, perhaps in a longitudinal design. This would allow us to better understand the ways in which workers may benefit psychologically when they are able to escape the stigma of their work.
Conclusions
This present study is the first to empirically test relationships between occupational stigma pertaining to aged-care work and worker outcomes. Findings revealed that perceptions of physical taint, social taint, moral taint, and poor occupational conditions predicted perceived occupational stigma. Perceived occupational stigma then predicted greater internalized stigma, which was, in turn, associated with greater psychological distress, job dissatisfaction, and turnover intentions. Thus, aged-care workers who view their work as stigmatized can apply negative evaluations about aged-care work to themselves, which in turn may lead to adverse psychological and job outcomes. Further research is required to understand ways in which our existing and emerging aged-care workforce can address this occupational stigma.
Supplemental Material
Supplemental Material - “The Stigma is what you do”: Examining the Relationship Between Occupational Stigma and Worker Outcomes in the Aged Care Context
Supplemental Material for “The Stigma is what you do”: Examining the Relationship Between Occupational Stigma and Worker Outcomes in the Aged Care Context by Asmita V. Manchha, Kïrsten A. Way, Michael Thai and Ken Tann in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study has been approved by The University of Queensland Human Research Ethics Committee [Approval No. 2020/HE002847].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.