
Abstract
Despite the significant stress of family caregiving, caregivers’ needs and risks are often overlooked in healthcare settings. This study examined the factors associated with primary care physicians’ perceived responsibility to identify and address caregiver needs and risks. Using a national random sample of U.S. primary care physicians (N = 106), multivariable logistic regression analyses were conducted to examine associations of physicians’ perceived responsibility to assess caregivers’ needs with experiential similarity (personal experience with caregiving), structural similarity (being older and female), and secondary exposure variables (time seeing older adults in the outpatient setting). Most (76.5%) physicians felt responsible for identifying caregivers’ needs and risks. In multivariable models, physicians who had personal experience with caregiving were four times more likely than those without it to feel responsible for identifying caregivers’ needs and risks and assessing caregivers’ mental health concerns. Thus, physicians may benefit from educational interventions that immerse them in caregivers’ lived experiences.
• Primary care physicians feel responsible for assessing caregivers’ needs and risks in clinical practice. • Personal experience with caregiving for a family member or friend may help physicians develop empathy for caregivers, better understanding of their challenges, and confidence in interacting with them. • Experiential similarity in caregiving may motivate primary care physicians to assess and address caregivers’ needs.
• Educational interventions designed to provide experiential learning opportunities that immerse physicians in caregivers’ daily lives may help them to be more attuned to caregivers’ needs and alter their counseling practices.What this paper adds
Applications of study findings
Background
Family and other unpaid caregivers are integral to supporting the health and well-being of older adults. These non-professional caregivers provide the majority of assistance to older adults who often have a high prevalence of chronic disease and cognitive impairment. The stress of caregiving puts caregivers at significant risk for burden, defined as the physical, emotional, social, and financial hardships associated with care provision (Adelman et al., 2014). The negative effects of burden can limit caregivers’ ability to manage caregiving tasks, which in turn has adverse consequences for their care recipients, including compromised physical health as well as increased risk of emergency department utilization, hospitalization, nursing home placement, and mortality (Gaugler et al., 2005; Noel et al., 2017). The pervasiveness of caregiving and its negative effects on both the caregiver and the care recipient suggest the relevance and importance of addressing family caregivers’ needs and risks in healthcare settings, where caregivers are often companions at older adults’ routine medical visits (Wolff et al., 2012).
Prior research has demonstrated the lack of routine mental and physical health support that caregivers receive from physicians, as well as physicians’ underutilization of formal procedures to assess caregiver risks (Riffin et al., 2021). Although research within the pediatric literature has demonstrated a link between pediatricians’ perceived responsibility and the action of addressing caregivers’ needs (Venkataramani et al., 2017), limited research has examined the factors that may contribute to physicians’ perceived responsibility to respond to the needs of caregivers who assist older adults.
The present study aims to address this gap in the literature by examining three factors that may influence physicians’ perceived responsibility to identify and address older adults’ caregivers’ needs and risks: experiential similarity (similarity in terms of role status or experience), structural similarity (similarity based on structural characteristics), and secondary exposure characteristics (second-hand experience gained through interactions with individuals with a particular status). This hypothesis and its clinical implications are summarized in Figure 1. In the sections that follow, we describe theoretical and empirical arguments for each of these hypothesized factors. Hypothesized Roles and Clinical Implications of Experiential Similarity, Structural Similarity, and Secondary Exposure in Motivating Physicians to Address Caregivers’ Needs.
Experiential Similarity
Theory and research suggest the critical role of experiential similarity in developing empathic understanding toward individuals who have undergone an analogous experience. Homophily theorists contend that individuals of the same status (i.e., caregivers) are likely to share similar perspectives and engage in mutual support (Pillemer et al., 2003). In support of this hypothesis, empirical work has shown that among adult child caregivers of parents with dementia caregiver status similarity is highly correlated with the provision of emotional support to other caregivers over the long-term (Suitor et al., 1995). In addition, a study of Canadian physicians found that personal caregiving experience helped them be sensitive to caregivers (Yaffe & Klvana, 2002). Prior research has also shown that physicians’ personal experiences may influence their recommendations to patients. Physicians who have personally experienced the benefits of an activity, such as exercising and other health habits, are more likely to counsel patients to achieve similar habits (Lewis et al., 1991). Extending this logic to the context of caregiving, experiential similarity may equip physicians with first-hand knowledge of the caregiving experience, and consequently the belief in the benefits of attending to caregivers’ needs and concerns. Thus, we hypothesize that physicians who have caregiving experience may be more likely to feel responsible for addressing caregivers’ struggles.
Structural Similarity
Theories of role structure and reference groups suggest that structural similarity may influence physicians’ perceived responsibility toward caregivers. Such theories assert that individuals with similar social statuses not only hold similar values, but also greater empathy toward others in a similar life stage (Merton, 1968). For example, physicians who are older may be more supportive of similar-age individuals caring for older relatives, and physicians who are women may feel greater responsibility for addressing caregiver needs due to their increased likelihood of becoming a caregiver and experiencing caregiving burden when they assume this role (Gallicchio et al., 2002). Moreover, prior research shows that women tend to be more empathetic and attuned to nonverbal cues than men (Doherty et al., 1995), and therefore may be more likely to identify psychosocial health concerns and offer education or counseling to address them (Maheux et al., 1990). In sum, the extant literature suggests that older physicians and physicians who are women may be more attuned to caregivers’ concerns.
Secondary Exposure
Secondary exposure refers to the second-hand experience gained through frequent contact with individuals in the target group (e.g., older adults or caregivers). Physicians with more frequent contact with older adults may be more likely to have greater exposure to caregivers due to the higher prevalence of caregiving among older adults, who are often accompanied by caregivers to their medical visits (Wolff et al., 2012). Physicians who have greater exposure to older patients through more frequent interactions may have greater empathy toward caregivers, and thus feel more motivated and responsible to address their needs.
Prior research has shown that experiential similarity plays a larger role than status similarity in forming support networks (Suitor et al., 1995). In addition, we suspect that personal experience with caregiving inherently leads to a deeper understanding and empathy for caregivers than indirect, secondary exposure. We therefore expect that experiential similarity may be more important than structural similarity or secondary exposure in determining physicians’ perceived responsibility toward family caregivers.
In sum, guided by theories of homophily and reference groups, we expect that experiential similarity may be more important than structural similarity or secondary exposure in determining physicians’ perceived responsibility toward family caregivers. The identification of factors related to physicians’ perceived responsibility to identify and address caregiver needs will help guide future interventions to increase physicians’ attention to caregiver concerns in the geriatric setting.
Methods
Participants
The American Medical Association (AMA) Masterfile was used as the sampling roster to identify five hundred U.S. based primary care physicians. The database records the education, specialty, and board certification status of all physicians in the U.S. regardless of their membership to the AMA and represents the largest association of physicians in the U.S. For this study, 250 physicians each were randomly selected from two pools: (1) physicians with Internal Medicine as the primary specialty and with board certification status in Geriatrics and (2) physicians with Internal Medicine as the primary specialty without board certification in Geriatrics. The sample was limited to primary care providers because this specialty emphasizes general health promotion and disease prevention (including evaluation of social determinants of health) and long-term relationships with patients and their families (Parmar et al., 2020).
Physicians were eligible if they treated older adults (age 65+) and had been working in a primary care practice for at least 1 year beyond training. They were ineligible if they worked outside of the United States or worked for the Veterans Affairs (VA) or the armed forces. VA physicians were excluded from the present study due to the VA’s integrated model of health care delivery that includes extensive services and supports for caregivers (e.g., Program of Comprehensive Assistance for Family Caregivers; Program of General Caregiver Support Services) that are not available to caregivers in the broader civilian community. These services may influence VA physicians’ attitudes and practices towards caregivers in a way that is not generalizable to U.S. primary care providers outside the VA (Bruening et al., 2020). Further details about the survey development and design are described in Riffin et al. (2021).
Survey Design and Distribution
The survey instrument was designed and reviewed by a multidisciplinary team composed of researchers with expertise in gerontology, health services, and psychometrics. It was then reviewed iteratively by local primary care physicians. The survey contents, language, and organization were refined and condensed based on physicians’ feedback over multiple iterations. The revised, final version of the survey was pilot tested via an online survey of one hundred physicians prior to administration to the target population. Minor revisions were made after pilot testing and prior to survey distribution.
The mail-based survey was distributed to a national random sample of primary care physicians in the United States from March 2019 to November 2020. Three methods were employed to enhance survey response rates, following the modified Dillman survey method (Dillman et al., 2014). First, both postal mail and electronic, online modalities of participation were offered to make the survey more accessible. Second, a $25 unconditional gift card was included with every survey. Lastly, the research team reviewed each recipient’s completion status 2 weeks after the mailing date and placed reminder phone calls to non-responders. The Institutional Review Board of Riffin et al. (2021) approved this protocol as an exempt study.
Measures
The survey instrument (as previously described in Riffin et al. (2021)) was designed to characterize primary care physicians’ approaches to identifying and addressing the needs of family caregivers of older adults. The survey collected information in four domains: (1) physicians’ self-reported practices regarding formal and informal assessment of caregivers’ needs and risks, (2) the barriers and facilitators to conducting these assessments, (3) physicians’ feelings of responsibility towards assessing and addressing caregivers’ needs and risks, and (4) characteristics of the respondents and their practice. The first two domains were examined in Riffin et al. (2021); the present study focuses on the last two domains (i.e., characteristics of physicians and their associations with physicians’ perceived responsibility to address caregiver needs and risks).
Dependent Variables
To measure respondents’ perceived responsibility to assess and address caregivers’ needs and risks, the respondents indicated on a 5-point Likert scale how strongly they agreed or disagreed that primary care providers should be responsible for each of the following tasks: (1) identifying caregivers’ needs and risks, (2) providing medical referrals to caregivers, (3) addressing caregivers’ need for services or supports, (4) assessing caregivers’ physical health concerns, and (5) assessing caregivers’ mental health concerns. For each outcome variable, the responses were collapsed into two contrasting categories (0 = strongly disagree, disagree, or neutral; 1 = agree or strongly agree) so that the two categories had approximately evenly distributed response rates.
Independent Variables
Variables for experiential similarity, structural similarity, and secondary exposure were reported in the survey. Experiential similarity was measured by asking respondents to indicate whether he or she is currently providing or has ever provided caregiving assistance to a family member or friend (0 = no; 1 = yes). The two structural similarity variables were age and gender. Participants were asked for their age in years and to self-report their gender (0 = male; 1 = female; 2 = other). Lastly, secondary exposure was accounted for by two variables. Physicians were asked to indicate how many hours per week they spent seeing older adults in the outpatient setting and to self-report the proportion of older adults (age 65+) in their patient panel.
Demographic and Practice Characteristics
The survey collected self-reported demographic information of the respondents, including their race and ethnicity. The responses for race and ethnicity were recategorized into White versus other (0 = White; 1 = Asian, Black or African American, Hispanic or Latino, or other), given the small sample sizes in the other categories. Respondents were also asked for information about their patient panel, including the proportion of older adults with and without dementia who attend appointments with a caregiver. For exploratory purposes, the present study included these variables in supplementary analyses (Supplementary Tables 1, 2 and 3).
The survey also collected information about physicians’ patient panel, clinical background, and practice structure, which were not included in the present analysis.
Statistical Analysis
Descriptive statistics were computed to characterize physicians’ demographics, self-reported patient panel characteristics, and perceived responsibility to address caregiver needs and risks. Unadjusted logistic regression analyses were used to analyze bivariate associations of experiential similarity (i.e., first-hand experience with caregiving), structural similarity (i.e., gender, age), and secondary exposure characteristics (i.e., hours per week spent seeing patients in the outpatient setting, proportion of older adults in the patient panel) with each of the five outcome variables related to physicians’ perceived responsibility to assess and address caregivers’ needs. The primary outcome variable of interest was physicians’ perceived responsibility to identify caregivers’ needs and risks. Four additional outcome variables were physicians’ perceived responsibility to: (1) provide medical referrals to caregivers, (2) address caregivers’ need for services or supports, (3) assess caregivers’ physical health concerns, and (4) assess caregivers’ mental health concerns.
To acquire a comprehensive understanding of the relationships of physician characteristics with their perceived responsibility to assess caregivers’ needs, additional exploratory analyses examined bivariate associations of the outcome variables with three additional variables: (a) physician’s race, (b) proportion of older adults with dementia in the respondent’s patient panel who attended appointments with a caregiver, and (c) proportion of older adults without dementia in the respondent’s panel who attended appointments with caregivers (Supplementary Tables 2 and 3). There were no significant associations between these variables and any of the outcome variables at the p < .05 level. Due to the lack of significance and lack of theoretical support from the current literature regarding their influence on physicians’ perceived responsibility to assess and address caregivers’ needs and risks, the three variables were excluded from the final multivariate analyses to create the most parsimonious model. The exclusion of these variables did not change the number and types of significant relationships identified in the final models (see Supplemental Tables 2 and 3).
Multicollinearity among the experiential similarity, structural similarity, and secondary exposure variables was examined using variance inflation factors (VIF) (<5). Based on the assessment of multicollinearity, none of these variables was excluded from the multivariate analyses. All variables were entered simultaneously into separate multivariable models for each of the five outcome variables related to physicians’ perceived responsibility to assess and address caregivers’ needs. All data analyses were conducted using IBM SPSS Version 26.0.
Results
Sample Characteristics
The overall response rate was 22% with 106 responses received from 474 eligible physicians. Twenty-six physicians from the 500 in the survey sample were excluded because they did not meet the eligibility criteria; they did not treat older adults (age 65+), had not been working in a primary care practice for at least 1 year beyond training, worked outside of the United States, or worked for the Veterans’ Affairs or the armed forces. Physicians with and without geriatrics certification did not differ significantly with respect to demographic or practice characteristics (see Riffin et al. (2021) for details). Therefore, data from both groups are presented in aggregate.
Descriptive Characteristics of Survey Respondents.
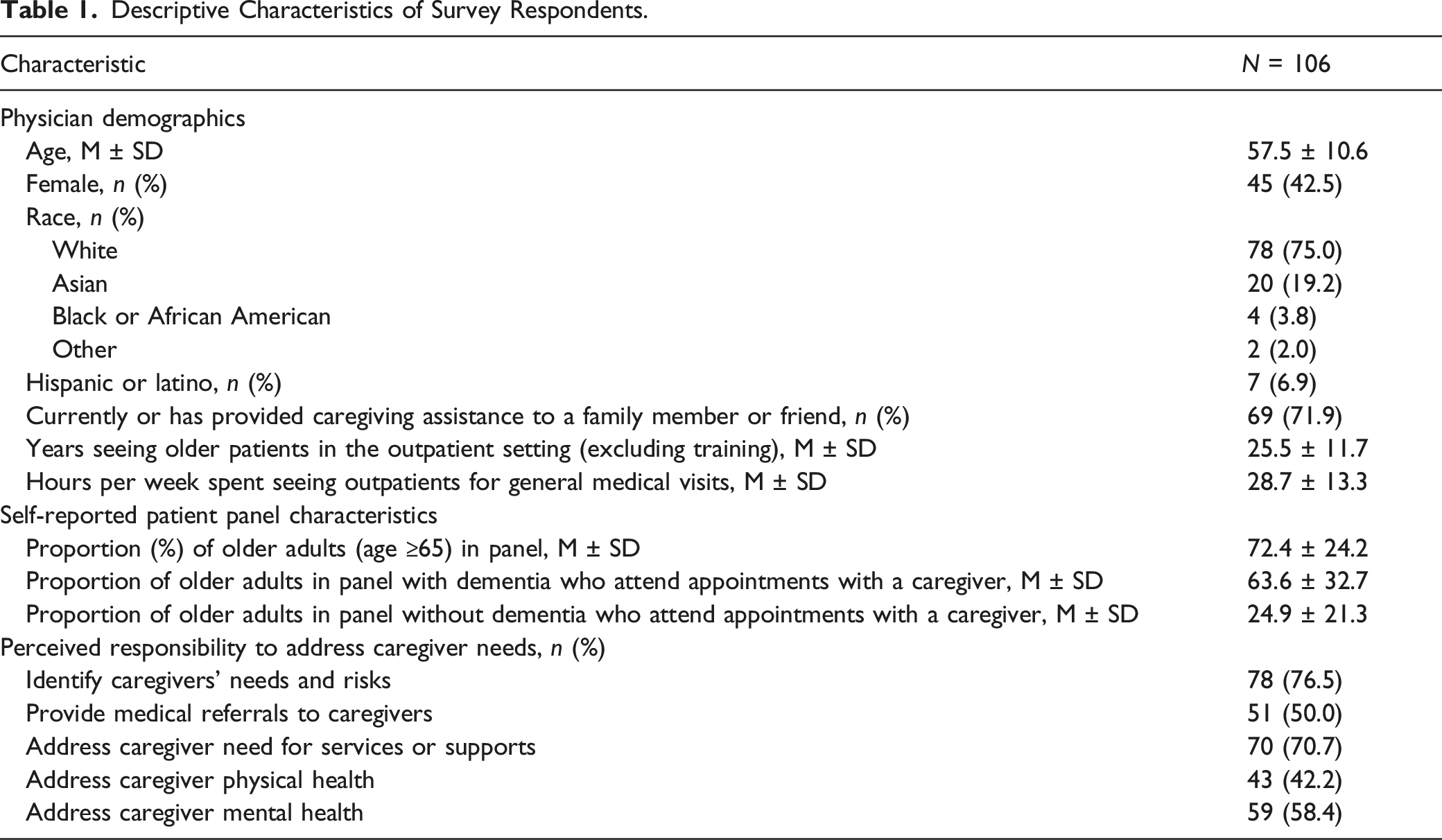
Overall, the attitudes of physicians reflected a feeling of responsibility to assess and address caregivers’ needs and risks. Most (76.5%) physicians agreed or strongly agreed that primary care providers are responsible for identifying caregivers’ needs and risks. Half of the physicians in our sample agreed or strongly agreed that primary care providers should provide medical referrals to caregivers (50.0%) as well as to address caregivers’ physical health concerns (42.2%) and mental health concerns (58.4%). Most (70.7%) of the primary care providers concurred that primary care physicians have a responsibility to address caregivers’ need for services or supports.
Bivariate Analysis
Bivariate Logistic Regression Analysis Examining Associations of Experiential Similarity, Secondary Exposure, and Structural Variables with Physicians’ Perceived Responsibility to Identify Caregiver Needs.

Significant associations (p < .05) are bolded, and borderline significant associations (p < .10) are underlined.
Physicians’ age and gender, the two variables representing structural similarity, were not significantly associated with any outcome variables (Table 2). The secondary exposure variable, number of hours per week spent seeing older adults in the outpatient setting, had a marginally significant association with physicians’ perceived responsibility to address caregivers’ physical health concerns (uOR 1.03; 95% CI 1.00–1.07) but was not associated with the other four outcome variables (physicians’ perceived responsibility to identify caregivers’ needs and risks, provide medical referrals to caregivers, address caregivers’ need for services or supports, and address caregivers’ mental health concerns). The proportion of older adults in the patient panel was not significantly associated with any of the outcome variables (Table 2).
Multivariate Analysis
Multivariate Logistic Regression Analysis Examining Associations of Experiential Similarity, Secondary Exposure, and Structural Variables with Physicians’ Perceived Responsibility to Identify Caregiver Needs.
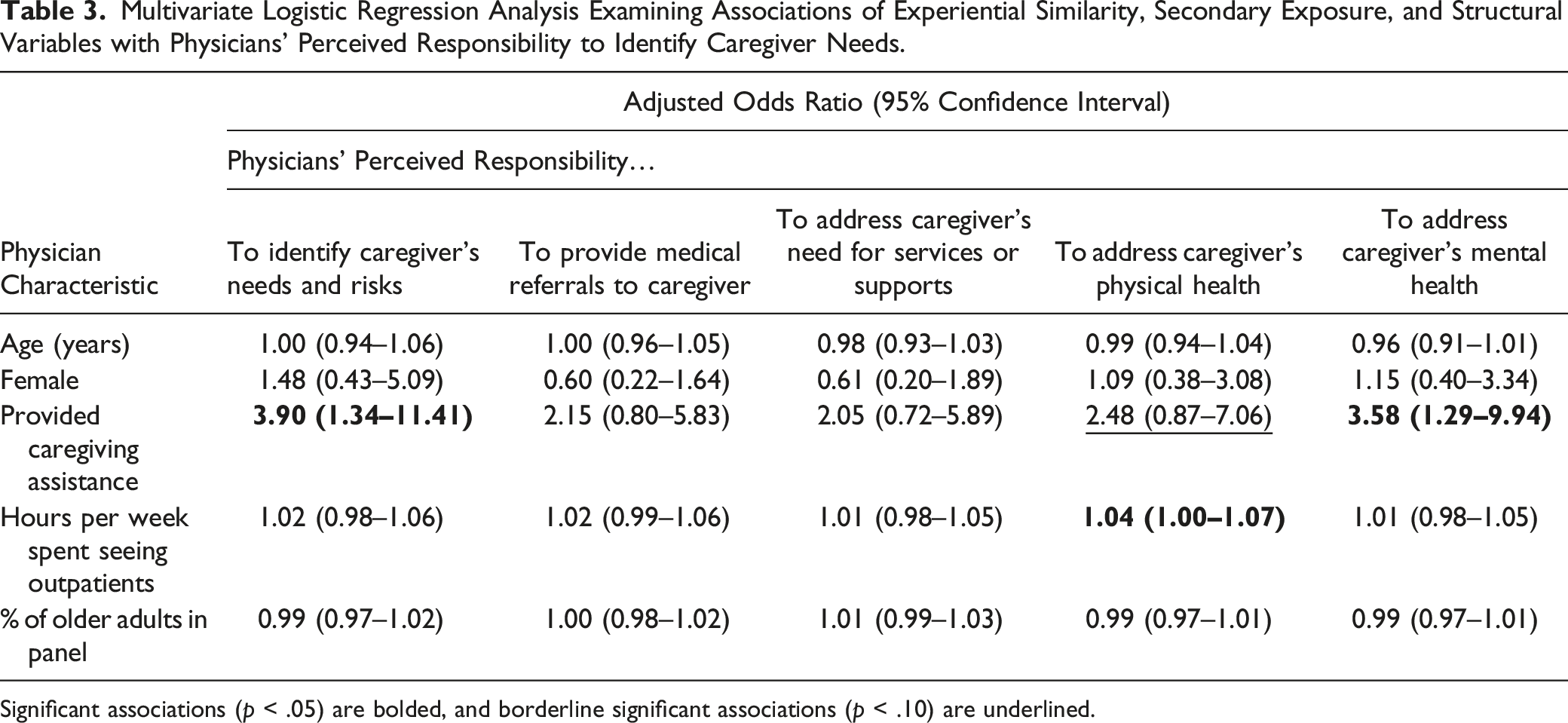
Significant associations (p < .05) are bolded, and borderline significant associations (p < .10) are underlined.
Discussion
In the present study, three-quarters (76.5%) of a national sample of primary care physicians agreed or strongly agreed that primary care providers are responsible for identifying caregivers’ needs and risks. This high prevalence likely reflects recent trends in healthcare delivery toward person- and family-centered care (Clay & Parsh, 2016). Furthermore, multivariable analyses revealed significant associations of experiential similarity with physicians’ perceived responsibility to identify caregivers’ needs and risks and to address caregivers’ mental health concerns. Physicians’ perceived responsibility in each of these areas was four times greater in those who had provided caregiving assistance to a family member or friend compared to those without personal experience.
Secondary exposure, measured by the number of hours per week spent seeing outpatients and the proportion of older adults in their patient panel, had only a marginally significant association with the physicians’ perceived responsibility to address caregiver’s physical health. Likewise, structural similarities in age or gender were not associated with any of the outcome variables.
Our findings are consistent with research demonstrating that experiential similarity plays a larger role than status similarity (i.e., age similarity, gender similarity) in forming and maintaining support networks among people with similar status (Suitor et al., 1995), and with studies showing that prior caregiving experience is positively associated with providing emotional support to other caregivers (Suitor & Pillemer, 1993). Caregivers experience significant emotional and physical burdens associated with their caregiving responsibilities, and primary care physicians with caregiving experience may have a shared appreciation of these burdens and demands (Suitor & Pillemer, 1993). In other words, experiential similarity in caregiving for a family member or a friend may make physicians more likely to recognize the negative consequences of caregivers’ burden, motivating them to identify and address caregiver needs in the healthcare setting. This finding is consistent with empirical research demonstrating that prior experience with caregiving for an older adult with dementia is positively associated with providing emotional support to other caregivers and negatively associated with causing interpersonal stress for other caregivers (Suitor & Pillemer, 1993).
An important aspect of experiential similarity is that it may equip individuals with the necessary first-hand knowledge and understanding to offer tailored recommendations and coping strategies to others undergoing a similar experience. Prior research has found that physicians draw upon their prior experiences to navigate difficult conversations during patient visits, and the same approach may be used when talking to caregivers about their mental and physical health or need for resources (Lamiani et al., 2012). In a similar vein, physicians’ counseling practices are commonly predicted by their personal health behaviors (e.g., exercise routines, smoking status) whereby doctors who implement healthier habits are more likely to counsel their patients about their benefits (Lewis et al., 1991). Applied to our study, physicians who have managed caregiver burden themselves may feel more comfortable or even compelled to recommend their own strategies to other caregivers.
Overall, our research, combined with prior literature, suggests that experiential similarity may operate through several mechanisms of action, including empathy towards caregivers, understanding and knowledge of their experiences, and confidence in communicating with them. Future investigation will be necessary to clarify the direct and indirect pathways by which experiential similarity may influence physician’s motivation to address caregivers’ needs, specifically by evaluating factors such as empathy and knowledge as potential mediators of this association.
The marginally significant relationship between the number of hours per week physicians spent seeing older adults in the outpatient setting and their perceived responsibility to address caregiver needs suggests that secondary exposure alone may not be sufficient to motivate physicians to attend to caregiver issues. Despite interacting on a regular basis with caregivers that accompany older adult patients to healthcare visits, clinicians who lack personal experience with caregiving may not be able to empathize as strongly with caregivers about the responsibilities of caregiving and their negative effects as those physicians with personal experience with caregiving (Wolff et al., 2012).
Implications for Medical Education
A key difference between experiential similarity and secondary exposure to caregiving is that secondary exposure is limited to interactions with caregivers in the healthcare setting when the physician is providing care to a patient accompanied by his or her caregiver. Experiential similarity goes beyond the clinical setting to encompass the broader lived experiences of caregivers, including their daily challenges and struggles. Medical education targeting experiential similarity should therefore emphasize immersive learning opportunities that engage physicians in understanding caregivers’ day-to-day activities and experiences outside of healthcare settings.
For instance, a study has found that increased personal interactions of undergraduates and nursing students with persons with dementia and their families in the community setting can help to improve knowledge and dispel negative attitudes about dementia and family caregivers (Daley et al., 2020). Similarly, research has shown that forming personal relationships with people with dementia and their caregivers in non-medical settings can help medical students to be more sensitive to caregivers’ burden (Jefferson et al., 2012). Lastly, the three-year Building Care Partnerships through Interprofessional Education project implemented a curriculum that consisted of films of caregivers’ stories, structured discussions on caregiving, and practice in effective communication with caregivers through simulations, learning exercises, case studies, and real clinical encounters, succeeded in helping medical students and residents to better understand caregivers’ perspectives and communicate with them (Blackie et al., 2019). The results of these interventions suggest that an intimate view into the caregivers’ lives, such as by watching in-depth interviews with caregivers, may help future physicians develop empathy towards caregivers and feel more committed to serving their needs.
Implications for Clinical Practice
Training primary care physicians to work with caregivers will be increasingly important in the coming decades as greater numbers of older adults seek medical care. Recent research using the same dataset as this study found that only a tenth of U.S. primary care physicians have a standard procedure for conducting caregiver assessments and that only one fifth routinely address caregiver physical and mental health issues (Riffin et al., 2021). In contrast, our study indicates that the majority (76.5%) of physicians feel responsible to identify caregiver needs, with 43% and 59% feeling responsible to address caregiver physical and mental health issues, respectively. Future research will need to address this disconnect between current and ideal practices.
As older adults transition into geriatric care, there is often a shift from dyadic patient–physician encounters to triadic encounters that also include a caregiver. Although prior research shows that physicians value caregivers’ involvement and input about the patient, they face an ethical and practical conflict in balancing patient autonomy with caregivers’ opinions. Geriatric patients report discomfort in sharing personal details, especially about mental or sexual health, in front of caregivers, and physicians have noticed a decrease in patient participation when the caregiver is present (Barone et al., 1999). Despite these challenges, clinical practice guidelines and transformations in medical ethics have prompted a shift within healthcare delivery toward meaningful engagement of caregivers and recognition of their needs for support (Gitlin & Hodgson, 2016).
Recent studies and ethical commentaries have considered ways to engage caregivers and address their needs without compromising patient autonomy (Griffin et al., 2020). For example, Gitlin and Hodgson (2016) have asserted that physicians have an ethical responsibility to (1) address caregivers’ health issues and capacity to provide care, (2) provide resources to caregivers, and (3) communicate to the patients about the caregiver’s role. These activities ensure that physicians act in accordance with the bioethical principles of beneficence, which governs that physicians act in the best interest of the patient, and nonmaleficence, which ensures that physicians minimize harm towards the patient. Medical students may benefit from additional training in how the Health Insurance Portability and Accountability Act (HIPAA) applies to triadic encounters as well as the limitations of HIPAA with respect to sharing patients’ information with caregivers (Carter & Bourque, 2018).
Beyond medical training, broader changes within healthcare delivery will be necessary to close the gap between research and clinical practice. Despite the availability of numerous empirically validated caregiver assessment tools, including those funded by the Health Resources and Service Administration (HRSA), they are underutilized in healthcare settings (Carter & Bourque, 2018; Guthrie et al., 2021). To incentivize physicians to utilize these tools, research has also pointed out a need to incorporate caregivers’ satisfaction into practice quality indicators, require hospitals to train family caregivers, and establish reimbursement codes for caregiver assessment since physicians commonly report lack of time and inadequate compensation as barriers to addressing caregivers’ needs (Gitlin & Hodgson, 2016; Riffin et al., 2021). In sum, clinical practice should address a multitude of factors including medical training and continuing education, practice quality measures, and the physician reimbursement system to incentivize physicians to support caregivers.
Limitations
The present research has several limitations and is subject to several biases among study participants. Self-report bias, retrospection bias, nonresponse bias, and social desirability bias may have skewed participants’ responses and inflated the percentage of physicians who reported that they felt responsible for identifying caregiver needs and risks (i.e., the dependent variable). As a secondary data analysis, analyses were limited to the questions included in the original survey, and as a cross-sectional study, causality cannot be inferred. Despite including an unconditional financial incentive with the survey, placing follow-up phone calls to survey participants, and providing the option to complete the survey by mail or online—strategies that have been shown to improve physician participation in postal surveys—the response rate was low (22%) (Sebo et al., 2017; Young et al., 2020). Nevertheless, this response rate is consistent with other surveys of healthcare providers (Cook et al., 2016).
Conclusion
Most physicians in this study felt that primary care providers are responsible for identifying caregivers’ needs and risks. Furthermore, physicians who had first-hand experience with caregiving were four times more likely than those without caregiving experience to feel responsible for identifying caregivers’ needs and risks and to assess caregivers’ mental health concerns. Overall, a multi-pronged approach involving the development of novel evidence-based interventions, changes to medical curricula and training, and transformations in healthcare delivery will be necessary for ensuring that future generations of physicians are adequately equipped to support and engage effectively with family caregivers.
Supplemental Material
Supplemental Material - What Motivates Physicians to Address Caregiver Needs? The Role of Experiential Similarity
Supplemental Material for What Motivates Physicians to Address Caregiver Needs? The Role of Experiential Similarity by Taeyoung Park, Karl Pillemer, Corinna Loeckenhoff, J. Jill Suitor3, and Catherine Riffin in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors would like to thank Drs. Julia Felice and John Michael for reviewing earlier drafts of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Institute on Aging [K01AG061275, 2019-2023]; the Cornell Human Ecology Alumni Association; and Cornell University. Corinna Loeckenhoff and Karl Pillemer acknowledge support from a National Institute on Aging funded Edward R. Roybal Center [P30AG022845, 2019-2024]. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
IRB Protocol
The Weill Cornell Medicine Institutional Review Board approved the protocol used for the survey as an exempt study (protocol #1709018564).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.