
Abstract
Family caregivers play an essential role in long-term services and supports (LTSS). Despite numerous calls for robust caregiver assessment policies to determine needs and treat them as partners in care planning, there has been limited information about whether or how states assess caregiver needs and strengths, or use caregiver information. Using cross-sectional survey data from the 2015 Process Evaluation of the Older Americans Act National Family Caregiver Support Program (NFCSP), this study analyzes caregiver assessment policies and practices in 54 State Units on Aging, 619 Area Agencies on Aging, and 642 local service providers. It examines whether and for what purposes caregiver assessments are used, what domains are included, and how well current policies conform to recommended practice. It also recommends that policy makers who influence NFCSP and other LTSS programs develop caregiver assessment practices using a multidimensional framework including more caregiver-focused domains and utilizing assessment data to measure program outcomes.
Keywords
Introduction
Family caregiving affects millions of people in the United States. It creates complex challenges that are costly and stressful at the personal level, economically consequential for employers, and important to the public policy agenda at all levels of government (Reinhard, Feinberg, Choula, & Houser, 2015). Family caregivers are unpaid individuals, typically family and friends, who provide assistance to people with personal care and other daily living limitations (Roth, Fredman, & Haley, 2015). There are an estimated 43.5 million family caregivers in the United States, of whom 34.2 million provide unpaid care to an adult age 50 or older (National Alliance for Caregiving & AARP, 2015). There is widespread agreement that they provide significant value to the country’s long-term services and supports (LTSS) system, because they improve quality of care and contribute to reductions in nursing home and inpatient hospital care (Chari, Engberg, Ray, & Mehrotra, 2015; Commission on Long-Term Care, 2013; Lipson, 2015). Although estimates of the economic value of their services can differ based on assumptions, one recent estimate put the value at US$470 billion annually (Reinhard et al., 2015).
The impact of family caregiving has been explored extensively since at least the 1980s (Zarit, Reever, & Bach-Peterson, 1980). Research underscores both the benefits of caregiving and potential negative effects on caregivers’ physical, psychological, and financial health (Bauer & Sousa-Poza, 2015; Leggett, Zarit, Kim, Almeida, & Klein, 2015; Robison, Fortinsky, Kleppinger, Shugrue, & Porter, 2009). Caregiver burden has been described as extreme strain from completing tasks that result in a range of psychological and physical impairments, such as poor nutrition, overeating, lack of exercise, self-medication, alcohol abuse, depression, and anxiety (Brandl & Raymond, 2012; Hoffman & Mitchell, 1998). Burden of care increases with hours of help, and an estimated 40% of caregivers are in high-burden situations, including the 22% who care for a person with dementia (National Alliance for Caregiving & AARP, 2015). Caregivers of persons with dementia are recognized as having some of the highest burdens and unmet needs (Bangerter, Griffin, Zarit, & Havyer, 2017).
Financially, family caregivers may experience the impact of caregiving on work, including lost wages and retirement (Feinberg & Choula, 2012; Reinhard, Levine, & Samis, 2013; Spillman, Wolff, Freedman, & Kasper, 2014). As many as six in 10 report having experienced at least one employment impact including reducing work hours, taking a less demanding job or leave of absence, retiring early, or taking personal or vacation time (Feinberg, Reinhard, Houser, & Choula, 2011; National Alliance for Caregiving & AARP, 2015). From the employer perspective, the economic burden from lost productivity due to caregiver absenteeism has been estimated at US$25 billion annually (Reinhard et al., 2015).
Despite the importance of family caregivers to their care recipients’ well-being and to the country’s system of LTSS, payers and providers of services to care recipients often fail to conduct an assessment of caregivers’ needs and capabilities (Reinhard et al., 2015). When they are assessed, it may be as a by-product of a care recipient assessment, or merely asking the care recipient who is involved in their care and what care they provide (Kelly, Wolfe, Gibson, & Feinberg, 2013). Meaningful caregiver assessment should be a process of gathering information about the entire caregiving situation, to pinpoint both the challenges and strengths of family caregivers, and their ability to contribute to care recipient needs (Feinberg & Levine, 2015). Family caregivers who have been assessed not only feel recognized and better understood by others, but the assessment process effectively identifies the various caregiver roles and the support needed to fulfill each role (Feinberg & Houser, 2012; Montgomery & Kwak, 2008). Targeting the services and supports most needed by family caregivers can protect them from negative aspects of caregiving and may prevent more costly outcomes such as nursing home placement of care recipients (Feinberg & Houser, 2012; Feinberg & Levine, 2015).
A number of federal, state, and other nonprofit programs have been created to address the identified needs of family caregivers. Although state and nonprofit programs vary widely, the primary federal program is the National Family Caregiver Support Program (NFCSP). Established in 2000, the NFCSP was the first comprehensive federal program designed to support the needs of family caregivers who provide care and assistance to aging adults and to grandparents raising grandchildren (Feinberg & Newman, 2004) and as of 2016, to older parents of adult children with a disability (Older Americans Act Reauthorization Act of 2016). The NFCSP provides grants to states, which in turn work in partnership with Area Agencies on Aging (AAAs) and local service providers (LSPs) in the community to offer five core services to family caregivers: information about available services; assistance in accessing supportive services; individual counseling, support groups, and caregiver training; respite care to temporarily relieve caregivers from their responsibilities; and supplemental services to complement the care provided by caregivers (Giunta, 2010). At the discretion of the AAA, additional caregiver programs and services may be offered to meet the local needs of caregivers. Each state and territory receives funding based on the proportion of its population age 70 and older. Since fiscal year (FY) 2008, the program’s annual appropriation has remained relatively constant at approximately US$150 million (Lipson, 2015).
Requests for NFCSP and other caregiver services have increased over time, but government agencies and nonprofits are less likely to meet the demand (Feinberg et al., 2011). Calls for assessment of caregivers’ needs for purposes of prioritizing and allocating scarce program dollars have also grown over the last decade. For example, the 2005 National Consensus Development Conference for Caregiver Assessment acknowledged that supporting family caregivers, including assessing their needs, is one of the key elements in an effective state LTSS system (Feinberg & Levine, 2015; Kelly et al., 2013). However, caregivers are often omitted as a significant component of home and community-based services (HCBS) because Medicaid policy views the care recipient as the legal beneficiary of services and not the family (Kelly et al., 2013). The degree to which caregiver needs are formally assessed and taken into account in care planning is one manifestation of the extent to which their essential role is acknowledged.
Since 2005, when the Family Caregiver Alliance detailed the recommendations of the National Consensus Development Conference for a national caregiver assessment policy (Family Caregiver Alliance, 2006a, 2006b), there have been many additional calls for more robust caregiver assessments. The AARP Public Policy Institute has addressed the subject often, and in 2013 made a strong case for including caregiver assessment in all Medicaid HCBS programs, including a discussion of the most useful assessment domains (Kelly et al., 2013). Also in 2013, the Federal Commission on Long-Term Care, among other extensive recommendations concerning family caregivers, recommended that the Centers for Medicare and Medicaid Services (CMS) include a family caregiver needs assessment in any care plan or discharge plan that relies on their services (Commission on Long-Term Care, 2013). A recent CMS rule on community living does include a brief though nonspecific requirement that caregivers be assessed when they are part of a service plan (State Plan Home and Community-Based Services for the Elderly and Individuals with Disabilities, 2014). For the first time in 2017, CMS also allows clinicians to bill Medicare for assessing the knowledge, needs, social support, and willingness to provide care of caregivers of persons with cognitive impairment (Alzheimer’s Association, 2017).
Other researchers suggest that the interRAI Minimum Data Set Home Care, an assessment commonly used for Medicaid HCBS waivers, should include questions about family caregivers and their support needs (Kelly et al., 2013). The National Quality Forum (NQF) in its 2016 final report on performance measurement gaps in HCBS recommended that caregivers’ support needs be assessed, not merely their ability to provide care, and that benchmarks be developed for measuring caregiver well-being outcomes (NQF, 2016). Most recently, the National Academies of Sciences, Engineering, and Medicine (2016), as part of its comprehensive review of caregiving, recommended that Medicare, Medicaid, and the Department of Veterans Affairs routinely identify family caregivers and assess and support their needs in the delivery of health care and LTSS.
Despite these growing appeals for more robust caregiver assessment policies, there is currently only limited information about whether or how states actually assess caregivers in various programs. In their Medicaid programs each state develops its own criteria, and there is no universal requirement to assess family caregivers in their role of providing HCBS (Kelly et al., 2013). A 2012 AARP Public Policy Institute survey of caregiver assessment practices in Medicaid HCBS programs found that only 15 states assess informal caregivers as part of the client assessment process (Kelly et al., 2013). The 2017 State LTSS Scorecard looked more broadly at assessment of family caregivers in a variety of state programs, not just Medicaid. It found that as of 2016, the number of states conducting mandatory or optional assessments of family caregivers in at least one of 10 programs had grown to 33, but that most of these assessments are conducted in smaller caregiver support programs rather than in Medicaid (Reinhard et al., 2017).
For states that wish to develop caregiver assessment policies, or to strengthen current practices, there are no national standards and few models or best practices for determining the content of effective assessments. Bangerter et al. (2017) recently reviewed the wide variation of methodological rigor in measuring the needs of caregivers of people with dementia and recommended more theoretical attention to developing reliable and valid assessment tools for that population. In the absence of any national or comprehensive standards for caregiver assessment in Medicaid or other programs, some researchers have suggested models for developing the content of caregiver assessments. Zarit (2006) suggested using Pearlin’s Stress Process Model of caregiving as a conceptual foundation for the creation of a comprehensive, multidimensional caregiver assessment and its component domains (Pearlin, Mullan, Semple, & Skaff, 1990). The Stress Process Model analyzes caregiver stress from the theoretical orientation of the stress process and its mediation and examines the stressors experienced by caregivers, the resulting adverse consequences, and the resources that buffer the effects of those stressors (Aneshensel, Pearlin, Mullan, Zarit, & Whitlatch, 1995; Pearlin et al., 1990). Using the Stress Process Model as a conceptual framework, Zarit suggests five areas of exploration for caregiver assessments: the caregiving context (sociodemographic factors, history of care, caregiving arrangements); primary stressors, both objective (cognitive status, behavioral issues, dependence in daily living activities) and subjective (overload, stress); secondary stressors (family and job conflict, economic problems); mediating psychological and social resources (coping, social support); and outcomes (health, well-being, service utilization, facility placement) (Zarit, 2006).
In this article, we provide an in-depth description of caregiver assessment policies and practices at all levels of the NFCSP, using data from the 2015 process evaluation of that program. We describe the extent to which caregiver assessments are used in the NFCSP and for what purposes. We also explore the content of assessments and domains included, comparing them to Zarit’s (2006) conceptual framework based on Pearlin’s Stress Process Model. We conclude by exploring how well these practices meet growing expectations for a focus on caregivers as key players in HCBS and highlight opportunities to improve assessment practices and measurement of caregiver program outcomes.
Method
This study draws on data collected as part of the 2015 Process Evaluation of the Older Americans Act (OAA) Title III-E NFCSP (Lewin Group, 2016), which was part one of a two-phase approach that constitutes the first full-scale evaluation of the NFCSP since its establishment in 2000. The Administration for Community Living (ACL) commissioned the comprehensive evaluation to gauge the impact of the federal investment in NFCSP, and to provide guidance for improving program efficiency, client outcomes, and effective targeting of vulnerable elders and their caregivers. ACL is separately completing an outcomes evaluation to examine the program’s impact on caregivers receiving services and the care recipients that they serve. ACL directed that both the process and outcome evaluations focus only on caregivers of older adults age 60 and above, and data were therefore collected only for those caregivers.
Because three types of organizations perform different functions relative to the NFCSP, the Process Evaluation gathered data separately from each group. State Units on Aging (SUAs) are the state governmental units responsible for state-level coordination of planning, fund-distribution, and monitoring of OAA programs, including the NFCSP. SUAs grant NFCSP funds to their state’s AAAs, which are community-level organizations established under the OAA to be locally responsive to the changing needs of the older adults in their communities. In a few states, SUAs also function as the only AAA in their state. AAAs often do not directly provide NFCSP services, but contract with LSPs to deliver services. LSPs are for-profit or not-for-profit businesses that adhere to contractual standards set by the AAAs and/or the SUA for delivery of NFCSP services, but have freedom as to how their businesses are run.
The methods described are for the 2015 Process Evaluation. This study did not collect any additional data, but used a subset of data specific to caregiver assessments collected in the course of the Process Evaluation.
Participants
The primary method of data collection for the Process Evaluation was a series of three online surveys directed to all 54 SUAs that operate an NFCSP (the SUA survey), all 619 AAAs active at the time of the survey (the AAA survey), and a sample of 642 LSPs (the LSP survey). The LSP sample was drawn from LSP contacts provided by the 457 AAAs that responded to the AAA survey. Because 10 of the 54 SUAs have a single planning and service area, they also function as AAAs and are included in both the SUA and AAA surveys.
Recruitment
All SUAs, AAAs, and LSPs received an email message with a unique survey link to the appropriate survey. SUAs also received an attached PDF version of the SUA survey and were given the option of completing it in either format. Emails were sent to all SUA directors and AAA directors, who identified the most appropriate person to respond to the survey. LSP contacts were provided by the AAA to which they provide NFCSP services. As most SUAs have close working relationships with ACL’s federal and regional offices, a member of ACL’s Office of Performance and Evaluation conducted reminder phone calls to each SUA, answered questions, and addressed any concerns. ACL also requested that SUAs encourage their AAAs to respond to the voluntary survey. AAAs also received automated reminders every 2 weeks while the survey was in the field. LSPs received follow-up emails and telephone calls from the research team reminding them to respond, answering questions, and offering to assist them to complete the survey over the telephone.
Survey Instruments
SUAs, AAAs, and LSPs each completed a survey specific to their role in the NFCSP. Survey questions for the three organizational types were identical when appropriate; otherwise, questions were tailored to the function of each entity type. The three surveys were pilot tested by the research team prior to finalization. Two SUAs, nine AAAs, and five LSPs, chosen to ensure variety in NFCSP program size and geographic location, provided feedback on clarity of survey language, time burden, question wording, and question ordering. Researchers made the necessary changes before survey dissemination to the larger sample. Although some questions varied among the three surveys, all focused on services available for caregivers and ways in which caregivers could access these services. Common topics (e.g., funding sources, wait lists, prioritization of services, assessment policies) were included across the three surveys. 1
Most questions specific to caregiver assessments in the AAA and SUA surveys were similar or identical. These included questions about who is assessed (caregiver, care recipient, or both), whether a standardized assessment tool is used, what domains are included in the assessment, policies on the frequency of assessment, whether training is provided to staff or volunteers on caregiver assessment, how assessments are used, and what outcomes, if any, are measured. SUAs were asked about state-level policy and regulation on individual-level caregiver assessments, how they define caregiver assessment (open-ended response), and whether there has been an effort at the state level to use the same caregiver assessment tools across all HCBS programs. AAAs were asked whether they were involved in developing a uniform caregiver assessment, and whether the establishment of the NFCSP prompted the creation or enhancement of a caregiver component in assessments for a Medicaid waiver program for older adults.
The LSP survey asked whether the organization ever conducted a comprehensive assessment of need for caregiver clients. If so, the LSP was asked the question identical to one in the AAA and SUA surveys regarding what domains are included in the assessment. In addition, LSPs indicated how often they conduct the caregiver assessment and share the findings with the AAA versus receive assessment results from the AAA, which entity develops the individual caregiver service plan, and whether the assessment form is statewide, comes from the AAA, or is created by the LSP.
Response Rate
Surveys were completed by all 54 SUAs (100% response rate), and by 457 of 619 AAAs (78% response rate). Of the 642 LSPs recruited, 63 were determined to be ineligible because they no longer provided NFCSP services or did not provide support for caregivers of older adults at the time the survey was fielded. Of the remaining sample, 393 responded, for a response rate of 68%.
Results
Results are presented first to highlight statewide, SUA-level definitions of caregiver assessments as well as policies on how they are conducted and who is assessed. Next, we compare responses to questions asked of both SUAs and AAAs on their caregiver assessment policies, and questions asked of all three organization types on the content of their assessments and domains covered. Finally, we present results from survey questions that were asked only of AAAs, or only of LSPs, to delve more deeply into policies at those levels.
SUA Policy on Caregiver Assessments
SUA responses to the only open-ended question, asking how they define caregiver assessment, revealed wide variation among SUAs in their approach to caregiver policy. A handful of SUAs stated they have no such definition, or that each caregiver program in the state defines its own assessment process. Several others described a highly decentralized process with no significant SUA-level direction:
[Our] caregiver assessment involves a series of questions on our intake tool that looks at caregiver eligibility and the needs of their care recipient. It is very basic and would be viewed more as an intake process than a true assessment form. Some of our contracted providers are doing more of a true assessment of caregiver and care recipient need, but this is not mandated at the SUA or AAA level.
At the other end of the spectrum are a small number of SUAs that tightly define and prescribe the caregiver assessment process. For example,
Assessment means the process of determining eligibility for a program, and may be used to measure the changes in a client due to participation in a program . . . The assessment shall include, but not be limited to: 1. A caregiver profile, including demographic information on the caregiver and the care recipient; 2. An evaluation of the informal support systems available to, and used by, the caregiver; 3. A care receiver profile and evaluation of the strengths and needs of the older adult; and, 4. Determination of the formal support services and resources available to the caregiver within the community.
SUA-level assessment tools also varied widely, from homegrown tools of differing levels of comprehensiveness developed for one SUA, to standardized and/or evidence-based tools such as TCARE® (Tailored Caregiver Assessment and Referral), the American Medical Association Caregiver Health Self-Assessment Questionnaire, and the Harmony SAMS (Social Assistance Management Systems) assessment. Although method of administration was often described as “face to face,” “in-home,” or “in person,” some also described a telephone interview process.
SUA policies on individual-level caregiver assessments most often include who is to be assessed (82%) and the content of the assessments (66%). SUAs less frequently regulate how often assessments are conducted (58%) or who can perform them (52%). Only about a third of SUAs (31%) reported that there had been an effort at the state level to use the same caregiver and care recipient assessment tools across all HCBS programs. Of the 16 SUAs reporting such efforts at program integration, 12 integrate their assessment tools across Medicaid HCBS for older adults and for adults with disabilities, and 11 do so for state-funded caregiver services.
Comparison of SUA and AAA Caregiver Assessment Policies
There are a number of notable differences between, and commonalities among, SUAs and AAAs in their responses to a common set of caregiver survey questions, summarized in Table 1. Only 57% of SUAs have a standardized caregiver assessment, compared with nearly three quarters (71%) of responding AAAs. About half of each organization type (45% of SUAs and 52% of AAAs) had conducted caregiver assessment training for staff and volunteers in the most recent FY. Although a significant majority of SUAs (81%) report that they assess both care recipient and caregiver, the practice of assessing both is less common at the AAA level (70%). Fifteen percent of AAAs assess only the care recipient and 12% assess only the caregiver. Only a small percentage of SUAs and AAAs conduct no assessments.
Comparison of State Unit on Aging and Area Agency on Aging Responses to Assessment Questions.

SUA state-level policy on frequency of conducting reassessments under a variety of circumstances is similar to reassessment policies reported by AAAs, with half of each group reporting a policy of annual reassessment. Fewer than half of each group has a policy to conduct reassessments upon change in status, with a slightly smaller proportion of AAAs than SUAs conducting reassessments upon change in caregiver status (38% vs. 44%), or care recipient status (36% vs. 42%). One fifth of SUAs and 13% of AAAs have no policy on frequency of reassessment. SUA policy on how assessments and reassessments are used tracks closely with how AAAs actually use them. The most frequent use of assessment data, by SUA policy (63%) and in AAA practice (79%), is to develop care plans for the caregiver. About half of both entities use assessments to prioritize who receives services. However, other potentially beneficial uses of assessment data, including strategic planning, program development, and measurement of caregiver program outcomes, are employed by less than a quarter of SUAs and AAAs and represent significant opportunities for improvement.
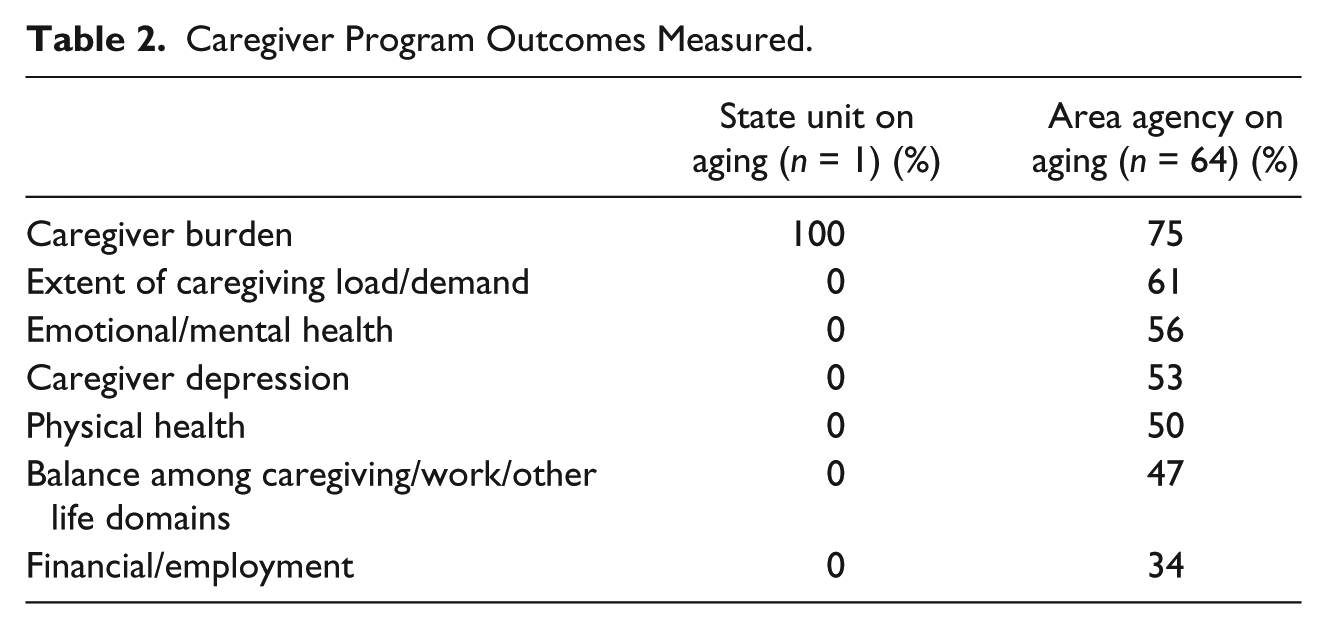
The small percentage of SUAs (18%) and AAAs (15%) who indicated that they use assessment data for measuring caregiver program outcomes were queried further about which outcomes are measured (Table 2). Only one SUA responded, indicating possible confusion about defining caregiver outcomes, and leading to the question whether those SUAs know details on how assessments are used. Approximately half to three quarters of the 64 responding AAAs measure outcomes such as caregiver burden or depression, emotional/mental and physical health, extent of caregiving demands, and balance among caregiving and other life domains. A third (34%) measure financial or employment outcomes.
Caregiver Program Outcomes Measured.
Caregiver Assessment Domains
One question common to all three surveys asked organizations to indicate which domains were included in their caregiver assessment. This question was asked of all AAAs, but was only asked of SUAs that indicated their state has a standardized assessment (57%), and LSPs that reported they conduct initial needs assessments for NFCSP clients (52%). Results from all three were similar (Table 3). Interestingly, the top two domains on SUA assessments, and the most frequent domain included in AAA assessments (care recipient demographics and financial status and care recipient’s health and well-being), focus on the care recipient, not the caregiver. The top two domains in LSP assessments (caregiver’s health and well-being and caregiver background and the caregiving situation) more directly recognize the caregiver as a distinct consumer.
Domains Included in Caregiver Needs Assessment.
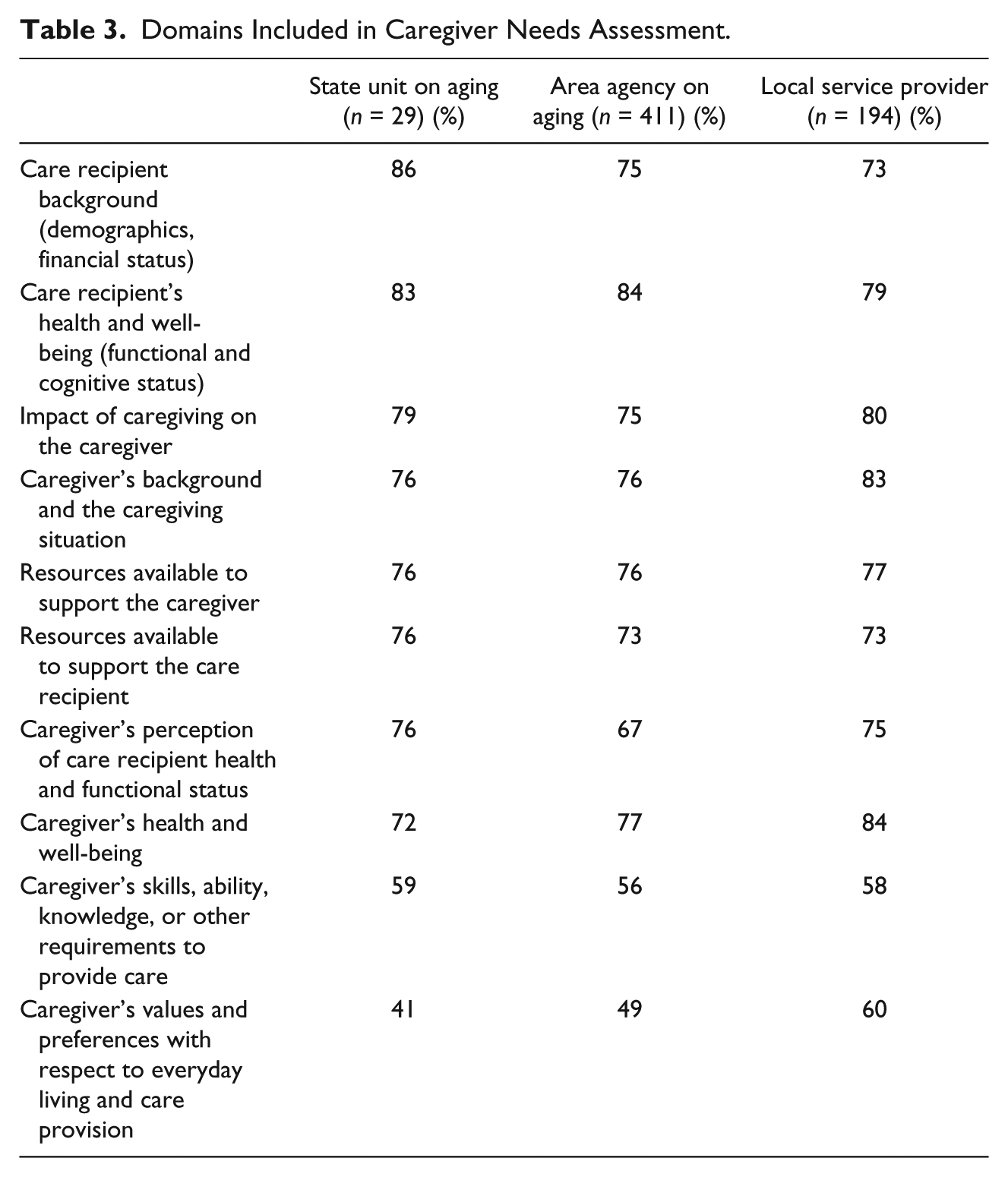
Other caregiver-specific domains were also well-represented in the assessments, with three quarters or more of all three organization types including impact of caregiving on the caregiver and resources available to support the caregiver. The domains least frequently included in all three assessments were caregiver’s skills, ability, or knowledge to provide care and caregiver’s values and preferences with respect to care provision.
AAA-Specific Results
Additional survey results specific to AAAs paint a broader picture of caregiver assessment policy and practices at the AAA level. In determining the type and amount of caregiver services only 59% of AAAs report that they use the caregiver needs assessment, whereas “availability of program resources” is the most important factor, cited by 74%. Whereas the establishment of the NFCSP in 2000 enabled the incorporation of some positive changes for caregivers in Medicaid waiver programs for older adults, only 8% of AAAs reported that the NFCSP prompted the enhancement or creation of a caregiver component in the waiver assessment.
On a positive note, over half (52%) of AAAs are currently developing a uniform caregiver assessment, and nearly two thirds of that group are doing so with partners, the rest without the involvement of partners. The small number of AAAs (n = 14) that do not conduct any caregiver assessments gave a variety of reasons for not doing so. Most report that they do not directly provide caregiver programs or that assessments are done through others, including LSPs or state-level agencies. Others report that they gather at least some information on caregivers through the intake or screening process, but do not conduct formal assessment due to lack of funds.
LSP-Specific Results
The LSP survey probed more deeply into LSP assessment practices and their relationships with AAAs in serving caregivers. Responses reveal a wide range of practices in who conducts assessments, how they are shared between organizations, the origins of the assessment forms, and which entity develops the service plan (Table 4). A little over half (52%) of LSPs report that their organization conducts initial comprehensive assessments of caregiver needs, and 81% of that group conducts the assessment all or most of the time, with the rest only some of the time. Although nearly two thirds of LSPs that conduct assessments share them with AAAs all or most of the time, 16% hardly ever or never do so. Of LSPs that ever conduct assessments, 39% use their own form, a third use a statewide assessment, and a quarter use assessments that come from the AAA.
Local Service Provider Assessment Practices.
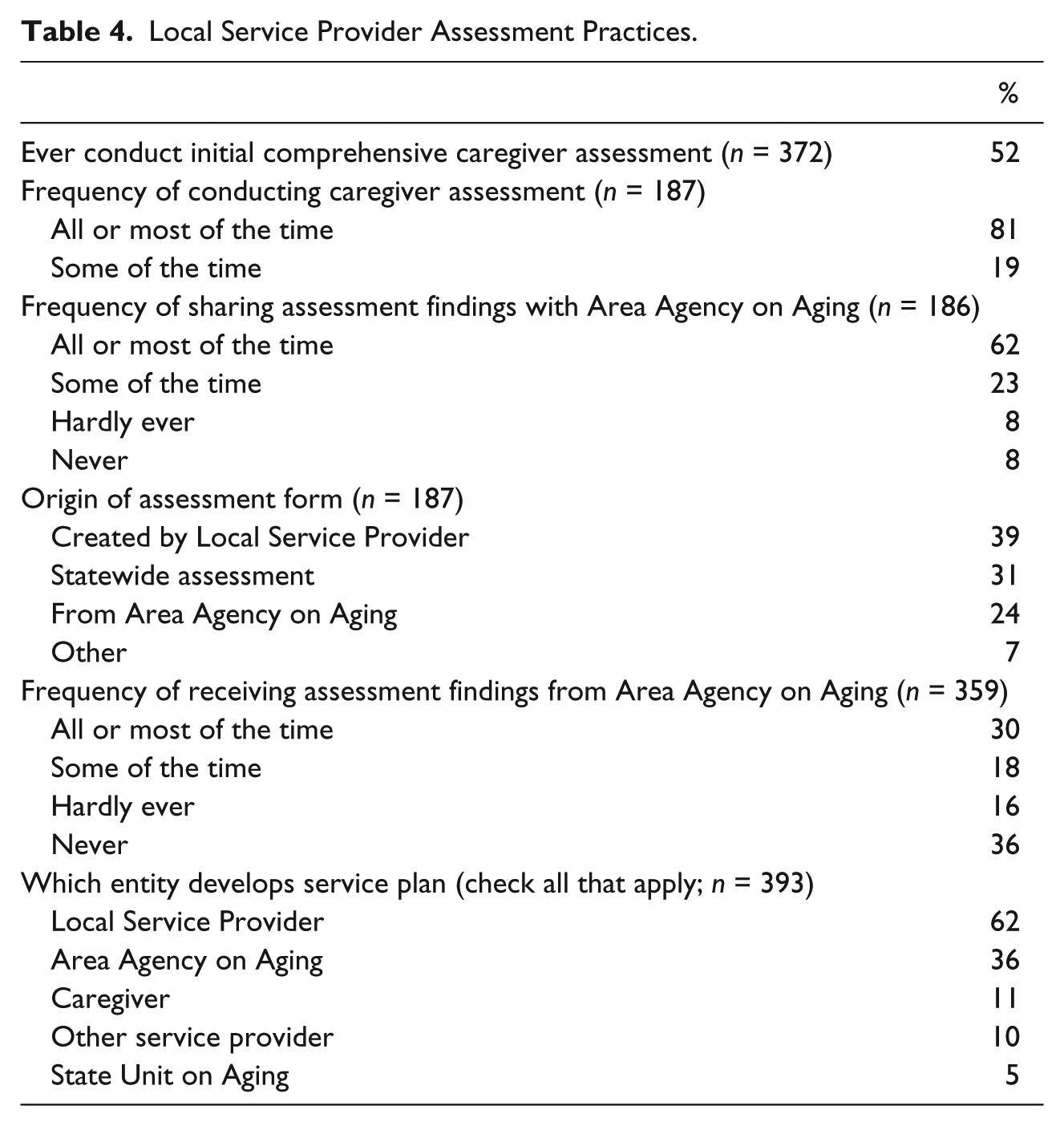
A third of all LSPs receive assessment findings from AAAs all or most of the time whereas over half (52%) hardly ever or never do. Development of caregiver service plans is often a joint endeavor, but LSPs are involved most often, with AAAs involved a third of the time, and other entities including SUAs and other service organizations involved occasionally.
Discussion
Policy makers and caregiver advocates have increasingly recognized that meaningful assessment of family caregivers is a key component of a robust LTSS system (Family Caregiver Alliance, 2006a; Feinberg & Levine, 2015). Determination of caregiver needs facilitates the targeting of resources to caregiver supports, which enable them to continue in their caregiving roles and in turn may prevent premature and costly institutionalization of care recipients. In-depth knowledge about actual assessment policies and practices at all levels of the LTSS system, however, has been lacking. The most pertinent data come from the 2012 AARP Public Policy Institute survey of informal caregiver practices in state Medicaid HCBS programs, which found that only 15 states had a family caregiver assessment (Kelly et al., 2013), and the 2017 State LTSS Scorecard, which found that in 2016, 33 states conduct optional or mandatory caregiver assessments in at least one program (Reinhard et al., 2017). Data from the recent NFCSP Process Evaluation supplement those earlier findings and provide broader insights into current policy and practices concerning caregiver assessment at the SUA, AAA, and LSP levels in the NFCSP. Although this study was somewhat limited (it included only NFCSP programs for caregivers of older adults that provide a minimum of respite or training/education services, and did not include Medicaid waiver or other state or local caregiver programs), it does provide a robust and representative picture of caregiver assessment practices within a national program.
Study findings illustrate wide variations in caregiver assessment policies and practices across all levels of the NFCSP, from whether assessments are conducted at all, to what purposes they are used for and what domains are included. In many organizations that provide caregiver services, caregiver needs are not assessed at all or in any standard way, or are assessed only as a by-product of a care recipient’s condition. Although care recipient condition can be an important source of stress for caregivers, numerous other factors play important roles and merit consideration. Assessment content at all levels of the NFCSP ranges from cursory to detailed. Where assessments do exist, organizations are missing opportunities to use them to accomplish the broader strategic goal of program development or measuring program outcomes.
At the state level, SUAs reported widely varying definitions of what constitutes a caregiver assessment, making it difficult to compare the effectiveness of state-level caregiver support programs. Even within a state, the comparison is challenging as standardized assessment tools appear less common at the SUA level (57%) 2 than at the AAA level (71%). More troubling, although most SUAs believe that both caregivers and care recipients are being assessed, a significant minority of AAAs (30%) report assessing only the caregiver or care recipient, or neither. More standardized assessment tools for all publicly funded programs, which have been recommended by advocates for over a decade (Family Caregiver Alliance, 2006a), would address this discrepancy.
SUA and AAA reported practices on frequency of reassessment, and use of assessment data suggest areas for improvement in program operations. Fewer than half of both SUAs and AAAs conduct reassessments upon a status change of either caregiver or care recipient, missing an opportunity to address changes in a dynamic caregiving situation that can threaten caregivers’ well-being. As expected, use of assessment data to develop care plans for caregivers is common at both levels. However, it is a less important factor for AAAs in determining the type and amount of caregiver services, which are more likely to be determined by availability of program resources. Fewer than half of AAAs and SUAs use assessment data to prioritize who receives services, leading to the question of how priorities for service are determined and whether caregivers with higher needs are being well served. There is also considerable room for expansion in the use of assessment data for strategic planning and program development, which happens less than a quarter of the time. As there is variable size distribution of AAAs across states, ranging from one to more than 50, some differences in SUA and AAA responses may not necessarily point to inconsistency between SUA-level policy and local practice, but may be affected by more AAA responses from high-AAA density states.
The content of caregiver assessment instruments can usefully be analyzed through the lens of the Pearlin Stress Process Model. Study data (Table 3) revealed that most assessment domains recommended by Zarit’s development of the Stress Process Model are explored, although in differing degrees, in current assessment practice at all three NFCSP levels. Although actual wording of individual assessment questions is unknown, the similarity of domain names indicates movement toward a similar result. Caregiving context, for example, can be gleaned from items comprising the “caregiver’s background and the caregiving situation.” Likewise, primary objective stressors are measured in the “care recipient’s health and well-being, functional and cognitive status” domain, and some subjective stressors through “impact of caregiving on the caregiver.” It is unclear from the data whether secondary stressors such as family/job conflicts and economic problems fall under that rubric, but they can and should be included. The presence of mediating psychological and social resources can be determined in the domains of “resources available to support the caregiver” and “caregiver’s skills, ability, knowledge.”
Some domains included, particularly by SUAs and AAA, are weighted more toward the care recipient’s background, health, and well-being, indicating that even in a program designed explicitly to benefit caregivers, the care recipient remains the primary focus. Although the LSPs that conduct assessments (only 52% of those surveyed) are somewhat less likely to include care recipient domains and somewhat more likely to explore caregiver background, impact of caregiving on the caregiver, and caregiver health and well-being, there is room for improvement at all levels in exploring caregiver skills, abilities, values, and preferences. To give a complete picture of the caregiving situation and resources needed to maintain or improve it, a comprehensive assessment should include an exploration of multiple caregiver domains that consider caregiver strengths as well as needs.
One of the most striking study findings is that more than 80% of SUAs and AAAs do not use assessment data to measure caregiver program outcomes, representing missed opportunities to ascertain the program’s impact on its consumers. In the Stress Process Model, the most salient outcomes of stressors experienced by caregivers are declines in their physical or mental health, and relinquishment of caregiver activities, either by transfer to others or institutional placement of the care recipient (Pearlin et al., 1990). These are exactly the outcomes that the NFCSP and other caregiver support programs seek to mediate through the provision of services.
Most SUAs, AAAs, and LSPs already gather some data on caregiver health and well-being, at least at initial assessment or intake. As most SUAs and AAAs also perform reassessments, they should have some longitudinal data that would allow them to compare caregiver status on these domains over time. Data from the limited number of AAAs (n = 64) that use assessment data to measure caregiver program outcomes present a roadmap for others aiming to gauge program impact. Greater use of assessment data to measure outcomes such as caregiver burden, extent of caregiver demand, emotional/mental and physical health of caregivers, depression, balance among life domains, and financial/employment considerations would allow SUAs and AAAs to adjust services that have poor outcomes and advocate for increased funding for proven successful outcomes. Outcomes already measured by this small number of AAAs are similar to measurement concepts related to family caregiver well-being recently recommended for further development by the NQF (2016) to improve quality measurement in HCBS.
The caregiver-specific assessment domains included in the NFCSP Process Evaluation surveys were derived from a list offered by the AARP Public Policy Institute for discussion and for inclusion in Medicaid HCBS waiver programs throughout the country (Kelly et al., 2013). That same report noted that as the NFCSP is the main source of funding for family caregivers, it should develop a uniform caregiver assessment for use across the states that would include the recommended domains. Some of the building blocks of a comprehensive caregiver assessment already exist in pockets of the NFCSP program, and could be used in a joint effort to create a uniform assessment across programs. A uniform assessment used both by NFCSP programs and state Medicaid HCBS programs could facilitate seamless referrals of caregivers between programs when appropriate without the need for burdensome duplicate assessments (Kelly et al., 2013).
At the LSP level, which is often closest to the consumer, caregiver assessment practices vary significantly, perhaps reflecting the broad range of LSP services provided and variability within states and AAAs. Many LSPs may view their client to be the care recipient rather than the caregiver. For example, home health, homemaker, or companion agencies may provide direct services to a care recipient although from an NFCSP perspective, they are viewed as providing respite to the caregiver and paid from caregiver support funds. Only about half of LSPs ever conduct an initial caregiver assessment and half receive assessment findings from an AAA at least some of the time. For those that do conduct caregiver assessments, the assessment form is almost equally likely to be their own creation, come from an AAA, or be a statewide assessment. Although LSPs report that they are involved in service plan development more often than AAAs (62% to 36%), they may be referring only to the services provided by their own agency and not to a comprehensive caregiver service plan in which the AAA may have contracted with multiple agencies to provide multiple services to the same caregiver.
Overall, data from the NFCSP Process Evaluation reveals substantial progress since the program’s inception in 2000 in elevating family caregivers, with their strengths as well as their needs, to an important focus of the HCBS system. Some SUAs and AAAs have robust policies and practices on caregiver assessment and reassessment and comprehensive tools that evaluate important aspects of the caregiving situation. A few use assessment data not only to prioritize service recipients and develop care plans, but also for strategic planning, program development, and measurement of caregiver program outcomes. Many domains assessed and outcomes measured are consistent with Pearlin’s Stress Process Model as expanded by Zarit in the context of the caregiver assessment process.
There are many opportunities, however, for improvement in caregiver assessment policies and practices. The lack of standardization at all levels and across levels makes it difficult to evaluate any program’s impact on caregivers or compare results across organizations. In keeping with the chorus of recommendations from many quarters for more rigorous caregiver assessment policies, ACL should collaborate with SUAs and AAAs to create more standardization in NFCSP-recommended assessment tools, based on the most important domains of caregiver well-being and measuring strengths as well as needs. SUA and AAA input will ensure that states’ desire for program flexibility as well as guidance is accounted for. It is encouraging that over half of AAAs are currently involved in the development of a uniform caregiver assessment. Building upon and learning from these efforts will create a stronger result.
Assessment results should also be used more widely to measure program outcomes. Although ACL’s planned caregiver outcomes evaluation will give useful guidance on the overall effectiveness of the national program, it is important to be able to continually evaluate outcomes at the state and local levels. More standardization in assessment process and tools will aid in this effort.
Standardization and outcomes measurement should not be limited to the NFCSP in isolation. Caregiver support in state Medicaid and other HCBS programs should be coordinated and referrals between programs made more seamless, ideally using the same or similar assessment tools. Indeed, through the NFCSP, ACL envisioned that each service component would eventually become available to caregivers nationwide by stimulating development of a multifaceted system that integrates NFCSP services, other OAA services, and other HCBS programs across the U.S. Department of Health and Human Services and other federal, state, and local entities. Greater standardization of assessment policies and tools across programs, coupled with robust and continual measurement of outcomes will help to fulfill that vision.
This in-depth examination of one key aspect of caregiver program operations across multiple levels of NFCSP program administration provides an important starting point for understanding more about the current state of, and future possibilities for, the assessment of caregivers in the NFCSP and beyond. Future research efforts could benefit from an examination of assessment practices for caregivers of younger adults and children with disabilities and for young caregivers in general, as well as caregiver assessment practices in other countries. Framing further development of assessment content through the Stress Process Model will lead to better person-centered and dyad-centered planning, and ultimately to more effective measurement of caregiver interventions and program outcomes. Mounting calls for such a focus from diverse quarters, including AARP, the NQF, and the National Academies of Science, among others, greatly enhance the chances for success.
Footnotes
Acknowledgements
The authors thank the many employees of the Administration for Community Living who contributed valuable suggestions and guidance during the study.
Authors’ Note
The opinions and conclusions expressed herein are those of the authors and do not necessarily reflect those of the Administration for Community Living.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Administration for Community Living.