
Abstract
In this study, we examined associations of social isolation and loneliness with cognitive impairment among older adults from a Rust Belt region in Southwest Pennsylvania. We used data from the population-based Monongahela-Youghiogheny Healthy Aging Team (MYHAT) study. We found that (a) 11 items combined into two reliable composites of social isolation and loneliness; (b) unique to this study, providing unpaid help to others was an indicator of reduced social isolation; (c) social isolation and loneliness were positively associated with cognitive impairment; and (d) these associations were appreciably attenuated by general health and physical functional status and depressive symptoms, respectively. We concluded that social isolation and loneliness are differentially associated with older adults’ cognitive health, and that their effects might operate through separate pathways. Approaches to address social isolation and loneliness should consider the community context and its implications for older adults’ cognitive health.
• Providing unpaid support to friends, neighbors, and family is an integral component of reduced social isolation among older adults, which has not been included in existing validated scales of social isolation using nationally representative samples. • The link between social isolation and cognitive impairment may be explained by older adults’ general health and physical functional status, whereas the association of loneliness with cognitive impairment may be attributed to depressive symptoms.
• To reduce the risk of cognitive impairment in older adults, comprehensive assessments are needed both of their social life and beneficial social activities, and of their physical and mental health. • Separate interventions are recommended to alleviate the deleterious effects of social isolation and loneliness: Health care that targets older adults’ general health and physical function could mitigate the impact of social isolation on cognition, whereas mental health therapies could reduce the adverse effect of loneliness on cognitive health.What this paper adds
Applications of study findings
Introduction
Social isolation and loneliness affect a substantial proportion of the aging population, among whom one in four experienced social isolation, loneliness, or both, during the last 4 years of their lives (Kotwal et al., 2021) between 2006 and 2016. Previous studies have reported that about a quarter of community-dwelling adults ages 65 and older were socially isolated and 4% were severely socially isolated (Cudjoe et al., 2020; Huang et al., 2023). Regarding loneliness, more than 40% of adults ages 60 and older were found to feel lonely and more than 10% often experienced feelings of loneliness (Perissinotto et al., 2012). Social isolation and loneliness have been shown to have deleterious effects on health outcomes and mortality (Holt-Lunstad et al., 2015). There is increasing evidence that social isolation and loneliness are negatively associated with cognitive outcomes with aging (Evans et al., 2019; Lara et al., 2019) and may do so through different pathways including socio-demographic, lifestyle, psychological and physiological states (e.g., Berkman et al., 2000; Fratiglioni et al., 2004; Hawkley & Cacioppo, 2010).
Conceptualizing Social Isolation and Loneliness
Social isolation is defined as the objective lack of, or limited extent of, social contacts (de Jong Gierveld, 2016). It is an umbrella term that describes different structural and functional aspects of social relationships, including social networks, social engagement, and social support. A wide range of measures have been used to capture various facets of older adults’ social lives indicative of social isolation (Cornwell & Waite, 2009; Cudjoe et al., 2020; Steptoe et al., 2013). For example, the Berkman-Syme Social Network Index (BSNI) includes measures of marital status, number of close ties, church attendance, and social participation to characterize social isolation (Berkman & Syme, 1979). Based on the U.S. National Social Life, Health, and Aging Project, a social disconnectedness scale was created to assess social isolation that included measures of social network size and range, frequency of interaction, number of co-residing individuals who are in the social network, and social activities (Cornwell & Waite, 2009). Steptoe and colleagues (2013) also created a social isolation index that includes variables for living alone, marital status, contacts with friends, family, and children, and organization participation/membership to quantify the level of social isolation among older adults in England.
Loneliness is a subjective perception of the undesirable absence of connections with others (Cacioppo & Hawkley, 2009). Unlike social isolation, loneliness is only recognizable by the individuals themselves. People feel lonely if the objective (i.e., size of social network, frequency of contacts) aspects of their relationships with others do not meet their expectations, or if the level of available social activities or support is misaligned with what they desire (de Long Gierveld, 2016; Cornwell & Waite, 2009). Widely used multi-item loneliness scales (e.g., UCLA loneliness scale and the de Jong Gierveld Loneliness Scale) include indirect measures of loneliness by assessing one’s perceptions toward their social relationships, such as frequency of feeling rejection/isolation from others, whether having confidants/people whom they trust, and frequency of receiving instrumental or emotional support when needed (de Long Gierveld, 2016; Hughes et al., 2004).
Associations of Social Isolation and Loneliness with Cognition
Ample evidence now shows that social isolation and loneliness are adversely associated with cognitive outcomes among older adults. Cognitive change with aging falls along a continuum from normal to dementia. With normal aging, declines can occur in information processing, working memory capacity, and executive function (Harada, et al., 2013). When decline in cognitive function affects daily life, a person is considered cognitively impaired. In longitudinal studies, social isolation and loneliness have each been found to be associated with long-term age-related cognitive decline (Evans et al., 2019) as well as elevated risk for mild cognitive impairment (MCI) and dementia (Lara et al., 2019). Our research group has previously shown that a rich social network with more and diverse ties and participation in social activities, the opposite of social isolation, is protective against cognitive impairment (Hughes et al., 2013). Loneliness is associated with more severe cognitive impairment (Cacioppo & Hawkley, 2009) and higher risk of dementia (Sutin et al., 2020), which in most studies is observed after accounting for the confounding effect of social isolation on cognitive outcomes (Shankar et al., 2013; Sutin et al., 2020; Yang et al., 2020). Recently, social isolation and loneliness resulting from restrictions and sudden disruption of social life due to the COVID-19 pandemic have shown to have deleterious effects on older adults’ cognitive functioning, especially among older adults already with dementia (Ismail et al., 2021).
Pathways Linking Social Isolation and Loneliness with Cognitive Impairment
Social isolation and loneliness have been proposed to influence cognitive outcomes through different pathways. One pathway is through health-related behaviors (lifestyle). According to Berkman and colleagues (2000), social networks provide access to social support which through social influence or supportive functions affect health-promoting or health damaging behaviors, such as smoking, alcohol consumption, diet, adherence to medical treatments, help-seeking behaviors, and physical activities.
Another pathway is one in which social isolation and loneliness trigger implicit hypervigilance and feelings of vulnerability to stressful situations, which have been linked to cardiovascular and cerebrovascular disease (Valtorta et al., 2016) that are known risk factors for cognitive impairment (Fratiglioni et al., 2004; Livingston et al., 2020). Other vascular risk factors including hypertension, diabetes, and obesity are also associated with loneliness as well as increased risk of dementia (Sutin et al., 2020).
A third potential pathway is where social isolation and loneliness affect sleep. Each are associated with augmented stress reactivity (e.g., irritability and inability to rest, relax, or let down), which can lead to sleep deprivation and lower sleep quality and affect older adults’ cognitive function and increase risk for cognitive impairment (Cacioppo & Cacioppo, 2014; Hawkley & Cacioppo, 2010).
A fourth pathway is through depression, particularly for loneliness (Hawkley & Cacioppo, 2010). Loneliness and depression are conceptually associated because feeling lonely can be a symptom or consequence of depression (Jylhä & Saarenheimo, 2010; Radloff, 1977). Loneliness may lead to depressive symptoms by reducing positive expectations of social encounters and avoiding unfavorable social outcomes, which in turn increases the risk of dementia (Cacioppo et al., 2010).
Finally, general health and physical functional status may link social relationships and cognition among older adults (Leigh-Hunt et al., 2017; Livingston et al., 2020; Kim et al., 2020). Loneliness may lower older adults’ self-rated health (Nummela et al., 2011), likely due to decreased social activities and related augmented stress, which can lead to reduced cognitive functioning (Tomaszewski Farias et al., 2018). As an objective measure of general health, a greater number of prescribed medications is associated with higher odds of mild cognitive impairment and dementia among older adults (Cheng et al., 2018). Increased number of prescribed medications raises the risk of unexpected adverse drug reactions and interactions, leading to impaired cognition (Oyarzun-Gonzalez et al., 2015). Lack of social support and loneliness could discourage older adults from engaging in instrumental daily activities (Guo et al., 2020). For example, socially isolated older adults may not have friends or family members to drive them to shop for groceries or attend medical appointments and become less capable of maintaining a healthy lifestyle. Severe IADL restriction with more activities requiring assistance can be a long-term predictor of future diagnosis of mild cognitive impairment and dementia (Altieri et al., 2021).
This study aimed to understand how social isolation and loneliness are associated with cognitive impairment among older adults from small-town Rust Belt communities in Southwestern Pennsylvania, whose once-vibrant economy heavily relied on the steel industry until it collapsed in the 1970s and has not fully recovered (Ganguli et al., 2010). This study is among the first to investigate how social isolation and loneliness were associated with cognition among older adults from this region that experienced a downward-trending economy and population decline since the 1970s. The population is not highly educated, and no other industry has moved into the area to replace the coal and steel industries. Most older adults have “aged in place” and have lifelong friends and neighbors in the same area, possibly providing a buffer against isolation and loneliness. Meanwhile, the once-vibrant social life of these towns has been depressed by the out-migration of the younger family and community members for better economic opportunities, which could lead to higher levels of isolation and loneliness. Shrinking social networks and low socioeconomic status provide a unique context to study how social isolation and loneliness are associated with cognitive impairment.
To fulfill our study aim, we first used procedures of scale construction to combine multiple indicators of social relationships and create composites that represent social isolation and loneliness. We then examined the associations of these composites with cognitive impairment. Finally, we explored five pathways—lifestyle, vascular health, sleep complaints, depressive symptoms, and general health and physical functional status, which might explain any associations found between social isolation and loneliness and cognitive impairment.
Methods
Sample
We used data from the Monongahela-Youghiogheny Healthy Aging Team (MYHAT), a prospective population-based cohort study investigating the epidemiology of mild cognitive impairment in the community. Participants aged 65 years or older were randomly drawn from voter registration lists of selected towns in a geographically defined region of Southwestern Pennsylvania between 2006 and 2008. The sample included 1,982 participants from the baseline cycle of MYHAT (collected between 2006 and 2008) with an average age of 77.65 years old. Participants were assessed on a range of objective and subjective measures of social relationships, cognition, and health that could explain the associations of social isolation and loneliness with cognitive impairment.
Measures
Social Isolation and Loneliness
Summary Statistics for Items and Composites of Social Isolation and Loneliness.
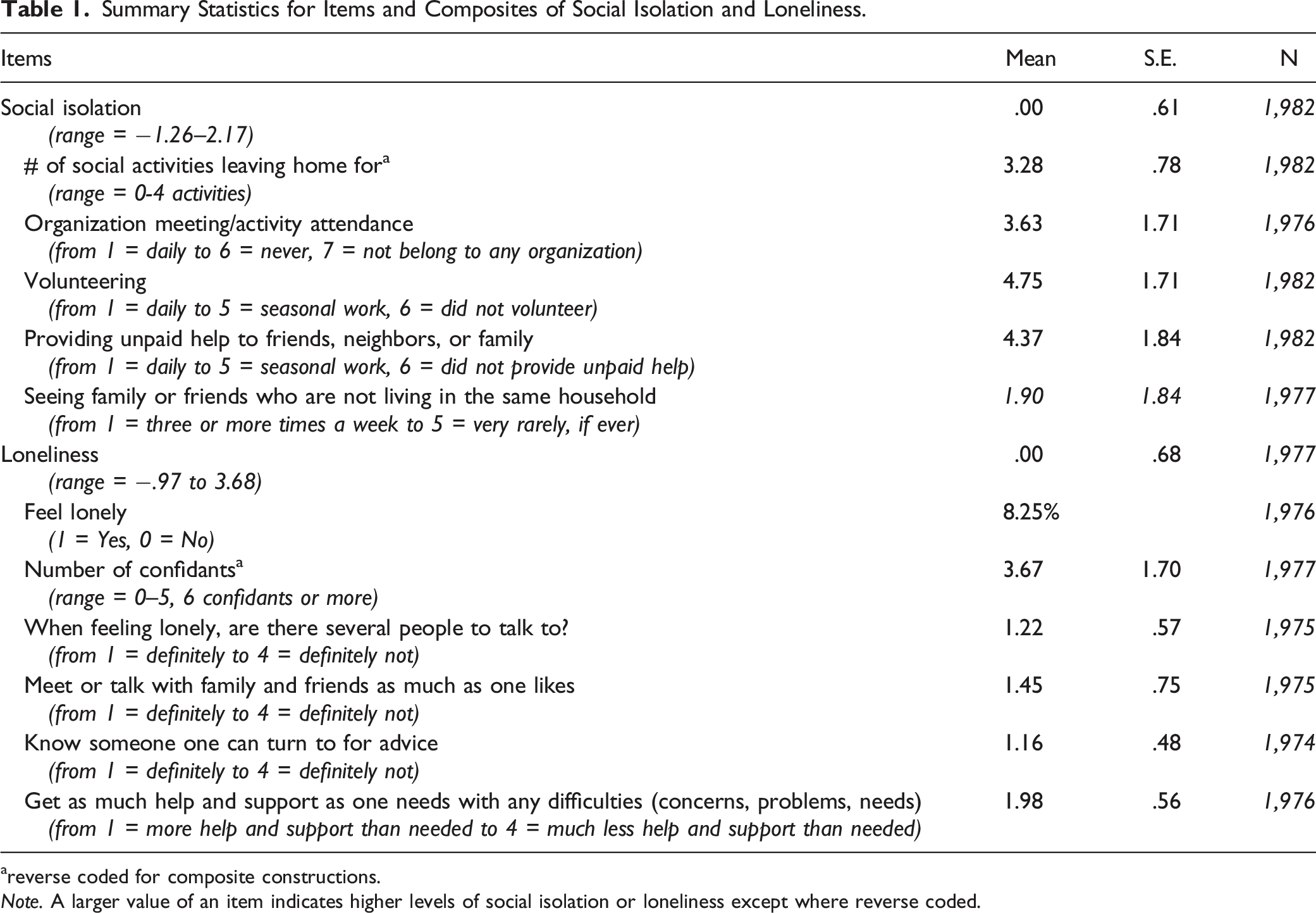
areverse coded for composite constructions.
Note. A larger value of an item indicates higher levels of social isolation or loneliness except where reverse coded.
Clinical Dementia Rating
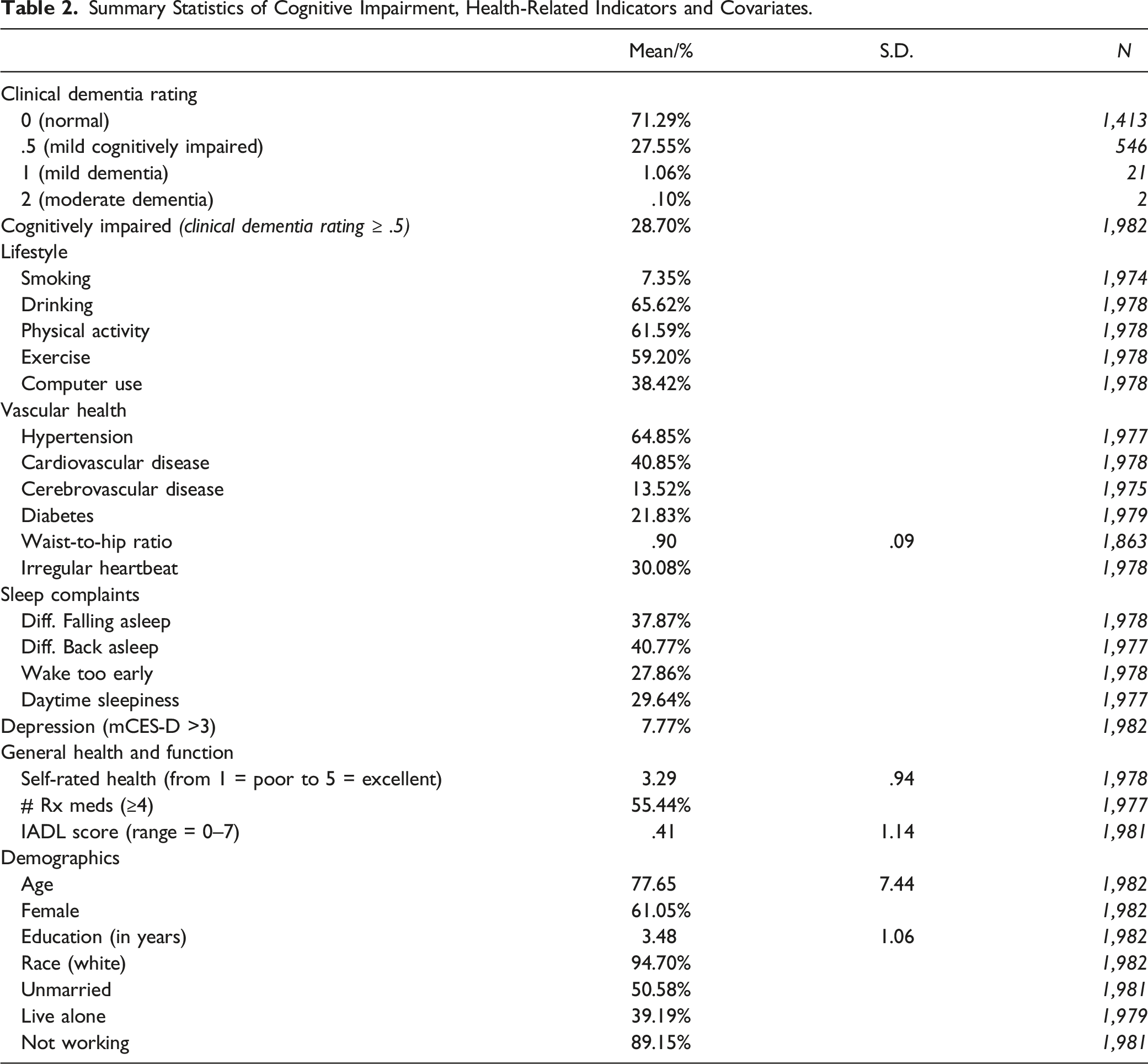
The Clinical Dementia Rating (CDR®) Staging Instrument (Morris, 1993), as previously detailed (Ganguli et al., 2010), was used to measure cognitively driven independence in everyday activities. There are five stages in the original rating of global CDR, ranging from normal (CDR = 0); mild cognitive impairment/very mild dementia (.5); mild dementia (1), moderate dementia (2), to severe dementia (3). We recoded CDR as a binary variable, with 0 indicating cognitively normal (CDR = 0) and 1 indicating cognitively impaired (CDR ≥ .5, mild cognitive impairment to severe dementia were grouped together).
Health-Related Indicators
Five groups of health-related indicators were included to explore potential pathways linking social isolation and loneliness with cognitive impairment. Lifestyle included five binary variables: smoked, consumed alcohol, and exercised in the past year, and physical activity and computer use at the time of the survey. Vascular health comprised five binary variables: whether participants reported having been diagnosed with hypertension, cardiovascular disease, cerebrovascular disease, diabetes, or irregular heartbeat, and one continuous variable: waist-to-hip ratio reflecting central (abdominal) obesity as the ratio of waist to hip in inches. Sleep complaints were measured using four binary variables: difficulty falling asleep, difficulty falling back sleep during the night, early morning awakening, excessive daytime sleepiness. Depressive Symptoms were measured by the modified Center for Epidemiologic Studies-Depression (mCES-D) scale (Radloff, 1977). In our cohort, this scale had a highly skewed distribution (Ganguli et al., 1995), where 3 symptoms or less represent the 90th percentile or the 10% most depressed members of the sample. Therefore, we used 3 symptoms as the cut-off value to recode the depressive symptoms variable as a binary variable, >3 symptoms as 1 and ≤3 symptoms as 0. Note the mCES-D item “I felt lonely” was omitted in the calculation to avoid direct overlap with the loneliness composite measure. General health and physical functional status had three variables: self-rated health was measured by participant’s evaluation of their own health compared to that of other people their age, values ranging from 1 = poor to 5 = excellent; number of prescription medications refers to the total number of prescribed medications a participant was taking regularly. Each medication was either verified from medication bottle labels by interviewers or described extensively by the participant. The variable was dichotomized with four or more medications coded as 1, otherwise as 0, with 4 medications representing 50% of participants in this sample. IADL scores ranged from 0 to 7 with one point given (1 = with some help or completely unable; 0 = without help) for every activity where help was needed (Fillenbaum, 1985).
Covariates
Covariates included the following demographic variables known to influence the prevalence of mild cognitive impairment and dementia, and social isolation and loneliness: age (in years), gender (1 = woman, 0 = man), education (1 = less than 8th grade, 2 = 8th—11th grade, 3 = High school graduate or GED, 4 = some college, 5 = college graduate, 6 = graduate school graduate), race (1 = white, 0 = others), unmarried (1 = yes, 0 = no), live alone (1 = yes, 0 = no), working status (1 = not working; 0 = working). For example, more advanced age and less education were associated with higher risk of mild cognitive impairment and dementia among older adults in the United States (Manly et al., 2022), as well as social isolation and loneliness (e.g., Cudjoe et al., 2020; Sutin et al., 2020).
Analytical Approach
Composite Construction
We selected items for each social isolation and loneliness composite based on their content validity, determined by literature (de Long Gierveld, 2016; Cornwell & Waite, 2009; Hughes et al., 2004; Steptoe et al., 2013), suggesting that these items may be indicative of objective or subjective assessment of social relationships. Details about the statistical methods of creating the composites can be found in the Supplementary section. We then tested the association between social isolation and loneliness using Pearson’s correlation test.
Associations Between Composites and Cognition
We used simple logistic regression and simple linear regression to test the bivariate associations of the likelihood of being cognitively impaired and social isolation and loneliness with the five groups of health-related indicators and demographic covariates, respectively. Finally, we used multivariable logistic regression to test the associations of social isolation and loneliness with cognitive impairment independent of each other and then independent of each group of health-related indicators adjusting for demographic covariates.
Results
Composites of Social Isolation and Loneliness
Table 1 shows the summary statistics for eleven individual items measuring social isolation and loneliness and the results of the factor analysis to create composites measures for social isolation and loneliness (results shown in Supplemental Tables 2 and 3). The social isolation composite included items related to objective evaluations of the participants’ social relationships: the number of social activities for which participants left home, frequencies of attendance at organizational meetings or activities, of volunteering, of providing unpaid help to family and friends, and of seeing family and friends not living in the same household. A novel finding in our study was that (infrequently) providing unpaid help to friends and family, not typically measured as part of social isolation, was highly correlated with other common social isolation components. Our finding suggests that helping members of the immediate social network with, for example, childcare, might counter social isolation in older adults.
The loneliness composite included items reflecting the participants’ subjective appraisal of their social contacts and support: feeling lonely, feeling they have several people to talk to when feeling lonely, number of individuals that they regard as confidants, meeting or talking as often as they would like with family and friends, getting as much help and support as they need with any difficulties, and knowing someone to whom they can turn for advice.
The composite score for social isolation ranged from −1.26 to 2.17, and the composite score for loneliness ranged from −.97 to 3.68. The two composite measures were moderately correlated (Pearson’s r = .26, p < .001) with each other, as shown in Table 3, which is consistent with previous reports (Cornwell & Waite, 2009; Steptoe et al., 2013).
Associations of Social Isolation and Loneliness with Cognitive Impairment
Summary Statistics of Cognitive Impairment, Health-Related Indicators and Covariates.
Bivariate Associations of Cognitive Impairment, Social Isolation and Loneliness With Health-Related Indicators and Covariates.
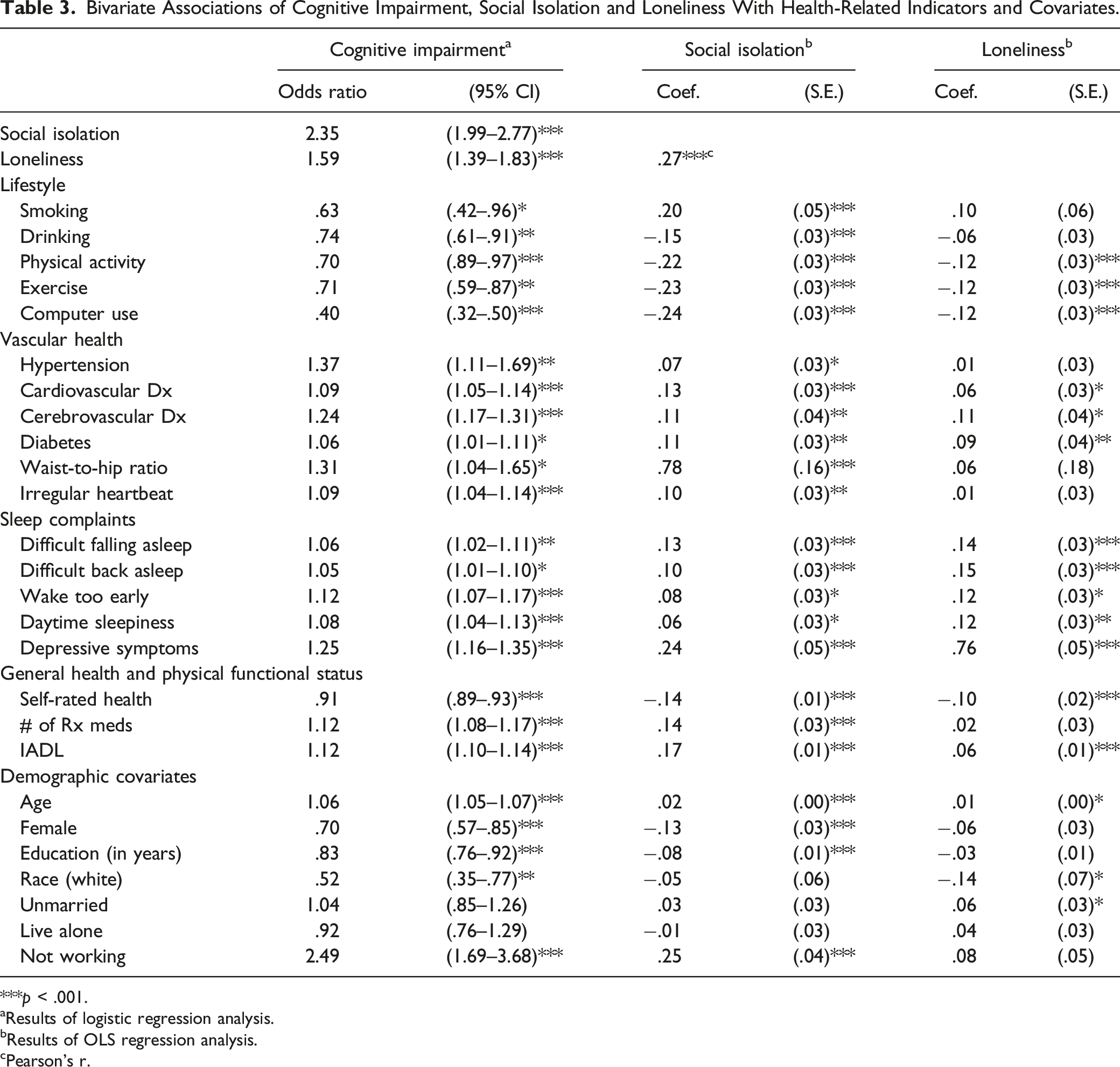
***p < .001.
aResults of logistic regression analysis.
bResults of OLS regression analysis.
cPearson’s r.
Associations (Odds Ratios) Between Social Isolation and Loneliness and Cognitive Impairment Adjusting for Health-related Indicators.

Note. Results of logistic regression analysis on cognitive impairment.
All odds ratios are significant with p-values less than .001, except for the association between social isolation and general health in Model 3 with p-value less than .01.
aAdjusted for demographic covariates.
bCompared to the odds ratio of social isolation in the model only adjusted for demographic covariates.
cCompared to the odds ratio of loneliness in the model only adjusted for demographic covariates.
dBoth social isolation and loneliness are included in the model.
Discussion
In this study, we investigated social isolation and loneliness and their associations with cognitive impairment measured by the Clinical Dementia Rating Staging Instrument® in MYHAT, a population-based sample of older adults from a Rust Belt region with relatively low socioeconomic status.
We first developed two composites measuring social isolation and loneliness in this cohort of older adults by utilizing variables available related to social relationships. In the MYHAT cohort, providing unpaid help to friends, neighbors, or family was an integral component of social isolation and associated with lower level of social isolation. This measure has not been incorporated in existing validated social isolation scales, as evidenced by reports from nationally representative surveys of older adults (Cudjoe et al., 2020; Cornwell & Waite, 2009; Steptoe et al., 2013). Being productive within their immediate social network could provide a buffer against social isolation among older adults within a relatively small community. Older adults’ experience of social isolation is varied by individual characteristics (Cornwell & Waite, 2009; Cudjoe et al., 2020). Findings from this study imply that geographic locations and community characteristics could be important contextual factors to understand older adults’ social life. Future research is needed to assess the validity of these composites and refine measures of social isolation and loneliness based on community-level factors.
Social isolation and loneliness were independently associated with cognitive impairment, and they attenuated each other’s associations with cognitive impairment, which is consistent with the literature. Theoretical mechanisms (Cacioppo & Hawkley, 2009; Fratiglioni et al., 2004) and empirical research (Holwerda et al., 2014; Kim et al., 2020; Sutin et al., 2020) suggest a mediating effect of social isolation on the association between loneliness and cognition. A recent study (Yang et al., 2020) also found that loneliness partially mediates the negative association of social isolation on older adults’ cognitive functioning. These findings further support their unique, yet related, links with cognition among older adults.
The five groups of health-related indicators attenuated the positive associations of social isolation and loneliness with cognitive impairment to varying degrees. The positive association between social isolation and cognitive impairment was reduced the most by general health and physical functional status. This attenuation may be explained by social isolation challenging older adults’ perceptions about their health. Lack of social activities and infrequent provision of help to others could lead to fewer opportunities for physical activity of adequate intensity to prevent or slow decline in physical function. The perceived health decline, diminishing daily function capabilities, and heightened adverse side effects or drug interactions due to increased prescribed medication use together could contribute to worse cognitive outcomes. The reduction of the positive association of loneliness with cognitive impairment was greatest after including depressive symptoms in the model, which is consistent with previous studies (Holwerda et al., 2014; Kim et al., 2020; Sutin et al., 2020), and may be explained by the inherent correlation between loneliness and depression (Jylhä & Saarenheimo, 2010; Radloff, 1977). Lonely older adults’ negative emotional responses, such as the fear about social rejection and failure and feeling irritable and intolerant of others in social settings, are closely related to depressive symptomology. Taken together, the state of older adults’ general health and physical functional status may be the more important factor to explain how social isolation contributes to cognitive impairment, whereas mental conditions may be more relevant to disentangle the association between loneliness and cognitive impairment. The significant, yet weak, association between social isolation and loneliness, the differences in pathways linking them with cognitive impairment, as well as their independent associations with cognitive impairment, suggest that these two attributes require distinct interventions to alleviate their potential deleterious effects on cognition among older adults (Kotwal et al., 2021).
Lifestyle, vascular health, and sleep complaints did not show strong influences on the associations of social isolation and loneliness with cognitive impairment in multivariate analysis, although their bivariate associations were significant. Contrary to existing literature (Lee et al., 2010; Sutin et al., 2020), we found that older smokers were less likely to be cognitively impaired in bivariate and multivariate analysis. The potential protective effect of smoking against cognitive impairment is likely due to survival bias and/or competing risks commonly found in studies of smoking and AD among older adults, especially for those 75 years and older (Chang et al., 2012). Given participants’ average age of 77.65 years in this study, the negative association between smoking and cognitive impairment can also be explained by this phenomenon.
Limitations of this study include the cross-sectional design, requiring caution in drawing inferences from the observed associations and potential mechanisms. The issues of reverse causality and bidirectionality between social isolation, loneliness and cognitive impairment can be addressed in longitudinal analyses (Evans et al., 2019). One possibility is that social isolation and loneliness are consequences of cognitive impairment, as behavioral reactions to diminished cognitive functioning or as a direct result of the pathology underlying cognitive impairment. The possibility of bidirectionality is that while social isolation and loneliness are leading to cognitive decline, cognitive change simultaneously is leading to higher levels of social isolation and loneliness. In addition, the lack of temporal order between social isolation/loneliness and health-related indicators does not allow us to claim they are indeed mechanisms in this study. For example, while we conclude that general health and physical functional status could link social isolation with cognitive impairment, it is also possible that older adults who are in poor physical health and functional status are more likely to become isolated and cognitively impaired. The lack of attenuative effects of lifestyle and vascular health is likely also due to the cross-sectional design with which we could not examine their delayed and long-term mediating associations found in longitudinal studies (Fratigolioni et al., 2004; Kim et al., 2020). In addition, the cross-sectional design does not allow us to statistically test and compare the strengths of each group of indicators. Future longitudinal research could validate the observed factor structure, determine the direction of the associations we observed, confirm the five potential pathways through mediation analysis, and explore more mechanisms through which social isolation and loneliness are associated with increased risk for cognitive impairment.
Conclusion
Providing unpaid help to members in the immediate social network was an essential component in understanding social isolation and associated with a lower level of social isolation among older adults from communities in the U.S. Rust Belt. This item is not included in existing scales of social isolation used in nationally representative samples. This novel finding could inform future research on interventions to reduce social isolation, which should take into consideration the influences of community characteristics on older adults’ needs for beneficial social lives. This study also highlighted the differences between the associations of social isolation and loneliness with cognitive impairment. Interventions to reduce the potential detrimental effects of social isolation and loneliness on cognition need targeted approaches. Understanding that social isolation and loneliness are correlated, yet unique, types of experience for older adults is the first step, followed by the acknowledgement that these aspects of social relationships may associated with older adults’ cognitive health through different pathways. For example, medical care and other interventions that target older adults’ general health and physical function could help to alleviate the impact of lack of social contacts on cognition. Cognitive behavioral therapy for depression focused on interpersonal interactions (Donovan & Blazer, 2020) and interventions on emotional self-regulation and social cognition (Hawkley & Cacioppo, 2010) could further reduce the adverse effect of loneliness on older adult’s cognition. Our findings also suggest that a comprehensive assessment of an older adult’s social life along with and interprofessional collaborations when treating older adult’s physical and mental health may help reduce the risk of cognitive impairment related to social isolation and loneliness.
Supplemental Material
Supplemental Material - Social Isolation and Loneliness in a Population Study of Cognitive Impairment: The MYHAT Study
Supplemental Material for Social Isolation and Loneliness in a Population Study of Cognitive Impairment: The MYHAT Study by Fang Fang, Tiffany F. Hughes, Andrea Weinstein, Hiroko Dodge, Erin Jacobsen, Chung-Chou Chang, Beth E. Snitz, and Mary Ganguli in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant #R37AG023651 from the National Institute on Aging.
IRB Approval
Monongahela-Youghiogheny Healthy Aging Team (MYHAT), whose data was used in this manuscript, has been approved by University of Pittsburgh Institutional Review Board. The IRB approval number is STUDY19040058.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.