
Abstract
Introduction
Loneliness (subjective social isolation), encompasses qualitative and experiential factors that reflect a person’s sense of belonging and quality of relationships (Cacioppo & Hawkley, 2003; Cornwell & Waite, 2009b). In contrast, objective isolation is quantifiable social disconnectedness, and encompasses such factors as the size and structure of social networks, the frequency and duration of social interactions, and the extent of social supports received (Cornwell & Waite, 2009b). Both loneliness and objective isolation are demonstrated risk factors for mortality and a variety of poor health outcomes (Cacioppo & Hawkley, 2003; Holt-Lunstad, Smith, & Layton, 2010; Wilkinson & Weltgesundheitsorganisation, 2003). A growing population of older adults, increasingly living alone, is especially vulnerable to the consequences of social isolation—Surveys suggest 17% of seniors are isolated (Ortiz, 2011) and approximately 20% to 35% report feelings of loneliness (Theeke, 2009; Wilson & Moulton, 2010).
Despite the prevalence of loneliness and objective isolation and their well-established links to poorer health (Holt-Lunstad et al., 2010), their relationship to health care cost and utilization has yet to be comprehensively studied (Valtorta & Hanratty, 2012). Recent work has highlighted the importance of empirically distinguishing between these two forms of social isolation, as the two only loosely correlate (Coyle & Dugan, 2012; Hughes, Waite, Hawkley, & Cacioppo, 2004) and have different impacts on health outcomes (Luo, Hawkley, Waite, & Cacioppo, 2012; Steptoe, Shankar, Demakakos, & Wardle, 2013; Tomaka, Thompson, & Palacios, 2006). It is probable they have distinct impacts on health care spending.
In the current era of cost-containment, clarifying the role loneliness and objective isolation play in health care costs is of renewed importance, and may be relevant to efforts to curb Medicare spending. No studies have yet explored the association between objective isolation, loneliness, and medical expenditures by older adults in the United States. In this study, we aim to expand understanding of this subject by employing a longitudinal sample of Medicare beneficiaries linked to robust social survey and health care spending data.
Background
A wide body of research has demonstrated social isolation in various forms—including loneliness and objective isolation—to be a risk factor for mortality, worse health outcomes, and poorer self-reported health. Research focusing specifically on loneliness suggests its health consequences are most pronounced among vulnerable populations, including older adults (Cacioppo & Hawkley, 2003; Tomaka et al., 2006), while more recent meta-analysis of mortality confirms both loneliness and objective measures of isolation similarly predict upward of 30% increase in mortality risk (Holt-Lunstad, Smith, Baker, Harris, & Stephenson, 2015). In two nationally representative samples (Cornwell & Waite, 2009b; Coyle & Dugan, 2012), both objective isolation and loneliness were shown to be associated with poorer self-reported health, with the added nuance that objective isolation more strongly correlated with poor physical health while loneliness more strongly correlated with poor mental health. The relationship between social isolation and health care use, however, is uncertain and has yet to be comprehensively examined (Valtorta & Hanratty, 2012), especially with explicit attention paid to the distinct parallel constructs of loneliness and objective isolation.
There are multiple mechanisms by which social isolation (objective isolation or loneliness) may affect health care use. It may affect health care use through its influence on various health behaviors (Broman, 1993; Umberson, Crosnoe, & Reczek, 2010). Socially isolated individuals may seek services as a substitute for social relationships (Coulton & Frost, 1982). Social relationships may (a) moderate or “buffer” the impact of stress, thereby enhancing an individual’s health and well-being and precluding the need for health services (Cassel, 1976; Cobb, 1976; Cohen & Wills, 1985; Gourash, 1978); (b) obviate the need for professional health services by providing social support (Gourash, 1978); (c) facilitate the use of health care by serving as “screening and referral agent(s)” for these services (Bass & Noelker, 1987; Gourash, 1978); and (d) transmit norms, attitudes, and values regarding seeking health care (Auslander & Litwin, 1990; Gourash, 1978).
Prior Research Findings on Social Isolation and Health Services Use
In various studies, disparate aspects of social isolation have been shown to influence physician services use, independent of health status; however, the significance and direction of that impact conflict across studies. Contributing to the difficulties in finding consensus among existing studies are variations in study setting (e.g., different nations with differing health care systems), measures of social isolation, measures of health care use (e.g., emergency department visits vs. primary care vs. inpatient admissions), and patient sample group (e.g., seniors, older mental health patients, psychogeriatric patients). Despite these inconsistencies, prior studies are broadly consistent in relying on the Andersen Behavioral Model, which theorizes that a person’s use of health care is influenced by three sets of factors: (a) need for care, (b) predisposing factors (e.g., health beliefs and social structure), and (c) enabling factors (e.g., health insurance, community resources) (Andersen, 1995, 2008). As summarized below, prior research into specific predisposing and enabling factors provides an intriguing but incomplete picture of social isolation’s connection to health care use.
The role of kin and non-kin relationships
Several studies suggest that the impact of social isolation on health care service use depends on the types of relationships involved, be they kin or non-kin. Coe, Wolinsky, Miller, and Prendergast (1985) found that older adults without kin support use hospital emergency rooms 7 to 30 times more often than those with kin in the area, while differences between them for physician visits and other hospital use were not statistically significant. Wolinsky and Johnson (1991) found that both kin and non-kin support are associated with a modest increase in physician visits, while having non-kin support is also associated with fewer hospitalizations and a lower likelihood of nursing home admission; kin relationships were not correlated with any other form of health care use in the study. Some have interpreted this to suggest that there is a stronger substitution effect (whereby informal social supports substitute for formal health care services) present in non-kin relationships (Wolinsky & Johnson, 1991).
The role of marital status and living alone
Some have examined the relationship between social isolation and health care use through the lens of marital status and living arrangements. In examining the impact of marital status, Cafferata (1987) and Bowling, Farquhar, and Browne (1991) found no significant direct effect between marital status and the use of health services. In contrast, a recent study of health care use patterns among a nationally representative population of older Americans showed married individuals significantly more likely than unmarried individuals to use outpatient services, but no significant difference in their use of hospital care (Manski et al., 2013). Wolinsky and Arnold (1988) and Evashwick, Rowe, Diehr, and Branch (1984) reported contradictory findings with respect to the impact living alone has on the general use of health services. In examining its impact on physician service and hospital use, Wan and Odell (1981) and Cafferata (1987) found that individuals living alone use more physician services; however, their findings conflict with regard to the impact on hospitalization. The use of “living alone” as an indicator of objective isolation has subsequently been called into question by more recent methodologic work by Cornwell and Waite (2009a), which confirmed that living alone (or household size) is not necessarily indicative of broader objective isolation.
The role of social support
Several older studies from diverse nations (the United States, China, Canada) suggest social support, including instrumental (e.g., financial and transportation), informational (e.g., advice, guidance, and referrals), and emotional (e.g., empathy and trust) support, each have unique associations with health services use (Coulton & Frost, 1982; Foreman, Yu, Barley, & Chen, 1998; Penning, 1995). The patterns shown across these studies are complex; the various forms of support may either facilitate or inhibit the use of health care, depending on a number of factors, including the type and level of support provided and the health services in question. Regardless of either a positive or negative relationship between social support and health service use, studies across numerous predictors suggest that social support plays at most a minor role in determining health care use, when compared with medical need (Coulton & Frost, 1982; Wolinsky & Coe, 1984), but this work was limited to frequency of physician visits, and did not include broader measures of intensity of care, such as cost.
Prior Research Findings on Loneliness and Health Services Use
Only recently have a handful of studies looked explicitly at loneliness as a predictor of variation in health care use among older adults. Among the largest is work by Molloy, McGee, O’Neill, and Conroy (2010) in Ireland, which attempted to clarify contradictory findings from smaller studies out of the United Kingdom by separating out emergency versus planned hospitalizations. They found greater loneliness correlated with increased emergency hospitalizations only. In the United States, recent analysis of the Health and Retirement Survey found increased loneliness (and objective isolation) associated with a lower likelihood of receipt of dental care (Burr & Lee, 2013); no such work has yet explored the association of loneliness with overall medical care use in the United States.
The Need for Additional Research
By and large, studies suggest that social isolation does influence the use of health services, including hospitalization and physician visits. However, its exact role is complex and appears to vary based on a number of factors, including the dimension of social isolation or social support evaluated, and the type of outcome in question. The research literature is further complicated by conceptual ambiguity regarding social isolation, variability in measurement approaches, and the use of nonrepresentative population samples (Burr & Lee, 2013). Several decades have passed since a majority of the existing studies were published, and many early studies are limited by variations in how social isolation is defined and measured, a lack of nationally representative samples to draw from, variations in the age profiles of study samples, cross-sectional or limited follow-up, and self-reported use of health services. Thus, the results of studies examining the impact of social isolation on health care use frequently conflict, and both the net effect of social isolation and the specific impacts of loneliness versus objective isolation on service use remain unclear.
Few studies have looked at a representative sample of older adults in the United States, in particular, and none have examined health service use in terms of net medical costs. This is especially salient as evidence is mixed when examining different types of service utilization—robust cost data could both differentiate the patterns of care of socially isolated patients and capture their overall costs—providing a tangible measure of the burden of social isolation.
Medicare as Context to Explore Social Isolation and Health Services Use in Older Adults
Medicare, the United States’s federal health insurance for persons older than 65 (and persons younger than 65 with certain disabilities and end stage renal disease), covers more than 50 million individuals, representing approximately 15% of the U.S. population. Medicare has two main components: (a) Part A Hospital Insurance (“Part A”) which helps cover inpatient acute care, hospice care, and when indicated post-hospitalization “nursing home” care in skilled nursing facilities (SNFs) and (b) Part B Medical Insurance (“Part B”) which helps cover outpatient services and medical providers’ fees including primary care, specialist care, occupational/physical therapies and some home health services. (Part A is provided free of charge to all eligible beneficiaries, while Part B requires a monthly premium paid by the beneficiary, often as a deduction from their social security payments). A third option for Medicare beneficiaries known as Medicare Advantage, created in 1997 as an alternative to traditional Parts A & B, enables beneficiaries to receive their coverage from private health care systems through a system of managed care (e.g., health maintenance organizations [HMOs] and preferred provider organizations [PPOs]) and covers a growing minority (31%) of Medicare beneficiaries (The Henry J. Kaiser Family Foundation, 2016).
Since Medicare’s inception 50 years ago, the proportion of very elderly beneficiaries has grown, and with this, the population has become increasingly complex—two thirds of beneficiaries have multiple chronic conditions (Hamel, Blumenthal, Davis, & Guterman, 2015). This aging population is relevant as the U.S. faces the daunting reality of massive health care spending (approximately 3 trillion dollars annually), which in 2013 surpassed 17% of GDP (gross domestic product), and at 5% to 6% average annual increase, continues to outpace rises in GDP. In the coming decade, the growth of spending on Medicare beneficiaries is expected to rise to 7.9%, as the aging baby-boomer population increases its use of health services (Klees, Wolfe, & Curtis, 2015).
Currently, Medicare is in the early phases of shifting provider payment methodology from fee-for-service toward value-based payment that attempts to incentivize higher quality care and better outcomes, while maintaining (or lowering) costs. With these payment changes underway, there is increased awareness that social risk factors (including social isolation) are important contributors to poor health outcomes. Currently, policymakers are evaluating whether it is necessary to adjust current payment policy to consider social risk factors (National Academies of Sciences, Engineering, and Medicine, 2016).
Objective and Hypotheses
Based on the current literature, we sought to expand understanding of the relationship between social isolation and health care spending among older adults by using data from a nationally representative sample of older adults, a clear distinction between loneliness and objective isolation, and precise measurement of health care use via Medicare expenditures.
In doing so, we expected to confirm that both forms of social isolation correlate with chronic illness and thus—prior to adjustment for health—would predict greater health care use. Second, we expected that—once adjusted for health and other sociodemographic factors—the two forms of social isolation would have distinct independent associations with health care use, though we remained agnostic as to whether net effect for each would show them to be barriers or accelerators of total health care use. Third, we believed examination of the types of care used (inpatient, outpatient, SNF) would reveal distinct signals for loneliness and objective isolation. Specifically we anticipated those who were objectively isolated would have higher need and use of SNF care given lack of social supports that might facilitate return to home after inpatient admissions; and we anticipated outpatient care, as a potentially more optional type of care, might show more variation for both objective isolation and loneliness, but remained agnostic regarding the direction of effect, recognizing they could both act as hindrances to use (e.g., via deficiencies in transportation and mood/motivation, respectively) and precipitants of use (e.g., via outpatient care substituting for inadequate informal health assistance and social contacts, respectively).
Method
Data Source and Study Population
We analyzed data from 2006, 2008, and 2010 waves of the University of Michigan Health and Retirement Study (HRS; N = 25,904), a nationally representative panel survey of adults age 50+, linked to Medicare beneficiary summary files for 2006-2012. In 2006, HRS introduced a Psychosocial & Lifestyle Questionnaire (response rate 90%) with questions on social relationships, activities, and perceptions (Smith et al., 2013). The questionnaire is administered to alternating halves of the HRS panel; as a new group of respondents age into Medicare each wave, we combined unique respondents from three waves and linked them to subsequent Medicare spending data through 2012, to create a longitudinal cohort of 9,438 respondents, aged 65 or older at the time of survey.
We limited our analytic sample to beneficiaries continuously enrolled in Original Medicare Parts A or B (n = 5,938), because spending data are unavailable for those who instead enroll in the newer, managed care Medicare Advantage. Our exclusion criteria (Online Appendix Figure 1) removed those who died within 1 year after initial interview (n = 171), based on the rationale that psychosocial survey responses and spending captured only in the final months of life would not be representative. Our final sample was 5,270 beneficiaries, linked to all available Medicare data following their baseline interview. Follow-up time for each respondent varied, with start determined by timing of initial psychosocial interview, and end reached with completion of the 2012 HRS survey wave or, if sooner, death. Median follow-up was 4.5 years (range = 1-7).
Measures
Subjective isolation: Loneliness
Loneliness was captured by a three-item scale contained in the HRS Psychosocial and Lifestyle Questionnaire. The scale is validated, and shown to capture information distinct from measures of social network (Hughes et al., 2004). It asks how often respondents (a) feel left out, (b) feel lack of companionship, or (c) feel isolated from others. For each question, there are three possible responses: “never or hardly ever,” “some of the time,” or “often.” Our analysis defines as “lonely” those who answered “some of the time” or “often” to any of the three items. This dichotomous approach to defining loneliness is identical to methods applied to HRS data by Perissinotto, Stijacic Cenzer, and Covinsky (2012) in their work demonstrating loneliness predicts increased mortality and functional decline. (It assumes that each of the three loneliness scale items can be taken to reflect “different ways a person might express loneliness rather than additive components of loneliness” (Perissinotto et al., 2012, p. 1079). In preparatory work, we considered a three-level approach, but found no suggestion of stronger effect for those responding “often” (vs. “some of the time”), and it instead found it only increased standard error for the few (9%) in the highest category of loneliness. We also considered treating loneliness as a continuous measure, but with only six levels of response and marked leftward skew, decided this was less appropriate; notably, prior work by Perissinotto et al. (2012) examined four different ways to treat the same loneliness scale in a similar HRS population (examining its association with mortality and functional decline) and demonstrated the dichotomous approach was as predictive and informative as the alternatives.
Objective isolation
To identify objective isolation, we created a scaled measure of social connectedness, based on normalized values of several survey questions capturing social network and interaction, and applied two thresholds to define three categories of objective isolation status: those with social connectedness score <1 standard deviation below the mean were defined as objectively “isolated,” those with scores within 1 standard deviation of the mean were defined as “not isolated,” and those with scores >1 standard deviation above the mean were defined as objectively “well-connected.” In preparatory work, we explored using the scale as a continuous or binary predictor, but confirmed the relationship was nonlinear and it was more appropriate to look at the extremes; once this was decided, 1 standard deviation was chosen a priori for cutoffs.
We derived our measure by applying the methodology developed by Cornwell and Waite (2009a; see Online Appendix Methods for full details), and arrived at an internally consistent scale (Cronbach’s α coefficient = .72) based on responses to HRS questions capturing (a) social network size; (b) network range (number of types of relationships in respondents social network); (c) the number of close friends; (d) how often respondents are in contact (write, talk, or meet) with children, other family, and friends; and how often respondents meet in person with (e) children, (f) family, and (g) friends.
Outcomes
For each respondent, we derived mean monthly spending, dividing total Medicare reimbursement by number of months of follow-up claims data for that individual. Medicare spending was obtained from HRS-specific Medicare Beneficiary Interview Summary Files which, instead of summarizing yearly data, summarize total spending on each beneficiary from one wave of biennial survey to the next (MedRIC Documentation for HRS Data Requestors, n.d.). Given varying entry and follow-up times, we normalized costs as monthly averages per beneficiary, with inflation adjustment to 2012 using the consumer price index. Our primary outcome was average Medicare spending per beneficiary per month, with regressions estimating marginal differences in monthly spending; we also present estimates of annual spending (monthly average × 12).
Secondary outcomes include Medicare reimbursement examined by type of care. Specifically, we looked at inpatient, outpatient, and SNF care, to clarify if loneliness and isolation predicted distinct patterns. As many beneficiaries did not receive any SNF or inpatient care, we also examined utilization as binary outcomes (for SNF) and frequency counts (for inpatient and outpatient care). Finally, to broadly capture health outcomes, we examined the likelihood and time to death during follow-up—that is, specifically exploring if spending differences by social isolation status accompanied better or worse outcomes.
Covariates
We adjusted for covariates that capture a wide array of factors known to influence access and use of health care (Andersen & Newman, 1973), and thus health care spending. Time-varying covariates were from the same HRS wave as respondent’s social isolation measures.
Demographic characteristics collected in HRS include age, sex, self-reported race, and education level; all of these were treated as categorical variables, with age represented by five groups (65-69, 70-74, 75-79, 80-84, 85+). Marital status was characterized as currently married/partnered or unmarried in the main analysis (with more granular treatment of past marital status explored in secondary analysis). Socioeconomic status was captured using HRS reported household-level income and net worth (converted to five income levels and six net worth categories for the purpose of analysis), and respondent’s working status. Urban or rural status was based on Beale Rural-Urban Continuum Codes.
Functional and health status data include self-reported measures of comorbid disease, functional ability (activities of daily living, or ADLs), substance use history, depressive symptoms, and body mass index (BMI). Comorbidity is measured by asking respondents which, if any, of the seven chronic conditions a doctor has ever told them they have: high blood pressure, diabetes, lung disease, heart problems, cancer, stroke, or arthritis/rheumatism. We coded ADL impairment by summing the activities in which respondents reported limitations, among walking, bathing, dressing, transferring, and eating. Tobacco use was based on self-report of ever having smoked; alcohol use was based on self-reported current use. Depression was measured using the Center for Epidemiological Studies Depression (CES-D) Eight-Item Scale (Steffick, 2000). BMI was calculated based on self-reported height and weight, at time of response to the Psychosocial and Lifestyle Questionnaire, and converted to a five-level categorical variable using standard cutoffs. (See Online Appendix Table 1 for the full set of covariates and the definitions of levels within categorical variables.)
Statistical Analysis
We first calculated descriptive statistics to compare Medicare spending and covariate distribution across each of our two measures of social isolation. We examined correlation coefficients between loneliness and objective isolation, and between loneliness and depression to answer concerns they might represent overlapping conditions.
To determine how loneliness and isolation predicted Medicare costs, we performed multivariable regression using generalized linear modeling (GLM) to estimate the marginal difference in per-person per-month health care spending. In our GLM models, we assumed a Gamma distribution of the errors with a log link function, as an appropriate estimator for nonnormally distributed health care spending data. All models adjust for HRS’s complex sampling design, using population weights to obtain nationally representative estimates, and adjusting estimates of standard error using clustering at the geographic region.
We ran three regression models, each one controlling for additional sets of covariates, to clarify the influence of covariate-adjustment on the effect size of loneliness and objective isolation on spending. Our first model controls for basic demographic information (age, gender, marital status) only. Our second model controls for the full set of sociodemographic variables (adding race, education, BMI, and geographic and economic covariates). And finally, our third model adjusts for all collected covariates, adding adjustment for functional and health status.
To demonstrate how loneliness and objective isolation are distinct, we explicitly include both together in our models. Given, however, the potential that the two measures were collinear, we also modeled each alone; we found their individual effects to be consistent regardless of whether we adjusted for the other. We further ruled out multicollinearity by calculating variance inflation factors (VIFs) for our full model—All were within acceptable range at <4, and near 1 for our primary predictors.
In sensitivity analyses (see Online Appendix Sensitivity Analysis), we explored the robustness of our findings to alternative definitions of function, depression, and health status. Last, we examined potential subpopulation effects, applying our main model to three subcohorts defined by marital status (married, widowed, or unmarried); we were specifically interested because older studies treat marital status as a proxy for social connectedness (Bowling et al., 1991; Cafferata, 1987; Evashwick et al., 1984; Wolinsky & Arnold, 1988) and recent work suggests marriage increases some health care use (Manski et al., 2013).
For our secondary outcomes, inpatient, outpatient, and SNF spending, we estimated separate GLM models, using the same covariate sets. We then used Poisson regression to estimate how counts of inpatient and outpatient visits differed by loneliness and objective isolation status, and used logistic regression to analyze the likelihood of any SNF use during follow-up. Finally, we estimated the effect of loneliness and objective isolation on mortality with a Cox proportional hazards model.
Results
Our cohort of beneficiaries had an average age of 74 years, with mean and median monthly Medicare spending of US$1,024 and US$489, respectively. Of the 5,270 participants, 55.3% reported being lonely, while 13.7% were objectively isolated by our social connectedness scale. Baseline characteristics (Table 1, Online Appendix Table 1) and Medicare spending (Table 2) varied across both measures of social isolation. For example, both lonely and isolated participants were significantly more likely to have lower economic means, be more depressed, and report chronic illness and impaired ADLs. The lonely were disproportionately very elderly (≥80 years) and unmarried, whereas objective isolation varied less across age and marital status. The lonely were more likely to be female, the isolated more likely to be male.
Sample Description: Characteristics by Social Isolation Status, Among Medicare Beneficiaries in the Health and Retirement Study 2006 to 2010.
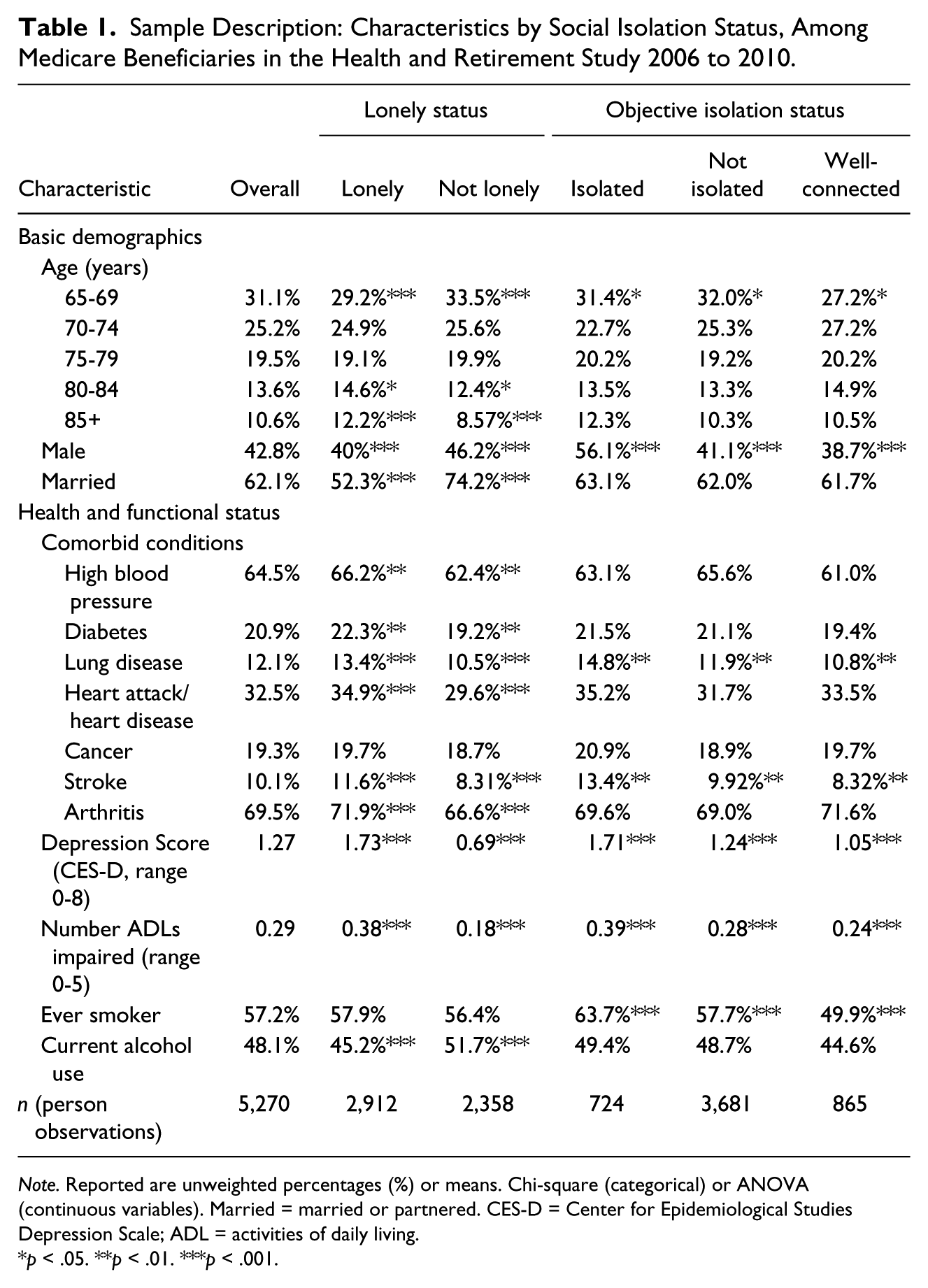
Note. Reported are unweighted percentages (%) or means. Chi-square (categorical) or ANOVA (continuous variables). Married = married or partnered. CES-D = Center for Epidemiological Studies Depression Scale; ADL = activities of daily living.
p < .05. **p < .01. ***p < .001.
Unadjusted Monthly Medicare Spending and Mortality, by Social Isolation Status.
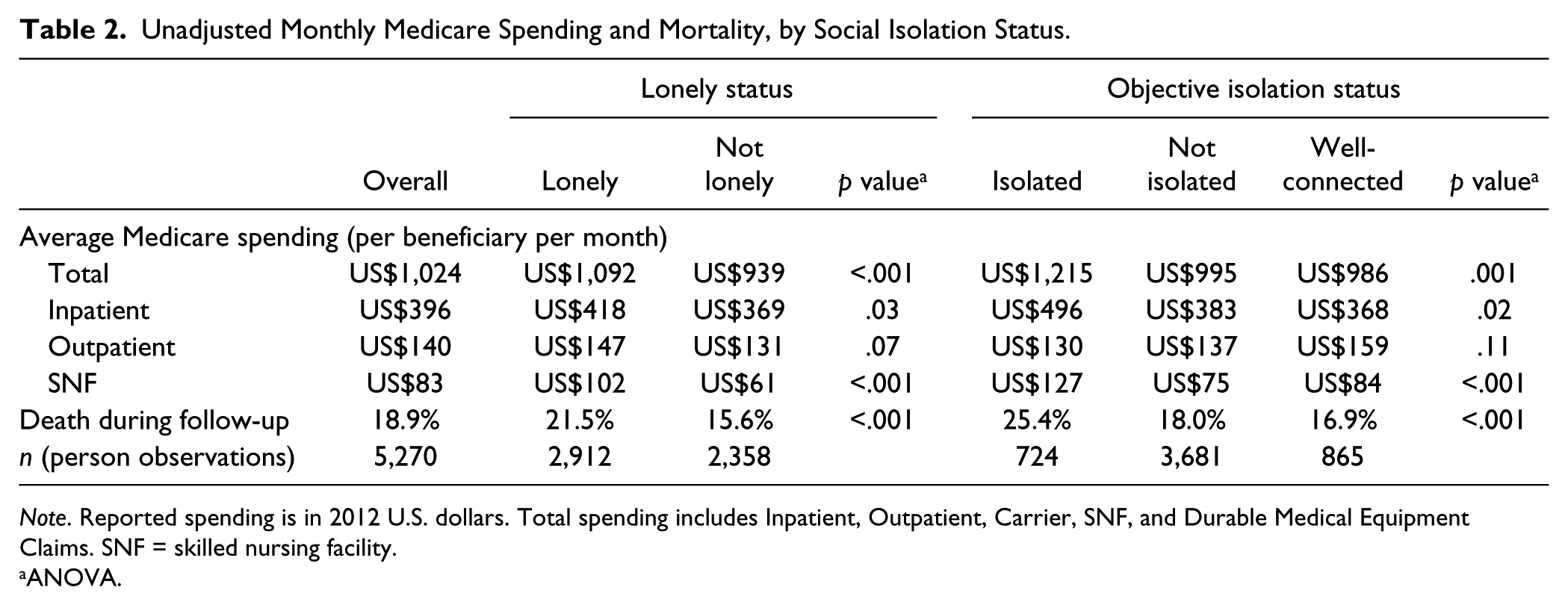
Note. Reported spending is in 2012 U.S. dollars. Total spending includes Inpatient, Outpatient, Carrier, SNF, and Durable Medical Equipment Claims. SNF = skilled nursing facility.
ANOVA.
Both the lonely and the isolated had higher Medicare spending: lonely beneficiaries spent US$153 more per month than nonlonely counterparts; the isolated spent US$220 more than their nonisolated counterparts. Despite similar patterns overall, the correlation between loneliness and objective isolation was limited, with 68% of those identified as objectively isolated also being lonely (Pearson correlation coefficient r = .20). Loneliness was also distinct from, and only weakly correlated with, depression (r = .25).
Adjusting only for basic demographics, both loneliness and isolation were predictive of increased Medicare spending: +US$68/month and +US$202/month, respectively (p < .001 for both). However, further, adjusting for socioeconomic and health status, the association with spending changed markedly for loneliness and reversed (Online Appendix Table 2). In our fully adjusted model, loneliness predicted a US$64/month reduction (an estimated −US$764 annually) in Medicare spending, while isolation predicted a US$137/month increase (+US$1,643 annually) in Medicare spending (p < .001 for both; Table 3).
Estimates of Effect of Loneliness and Objective Isolation, by Type of Health Care Use.
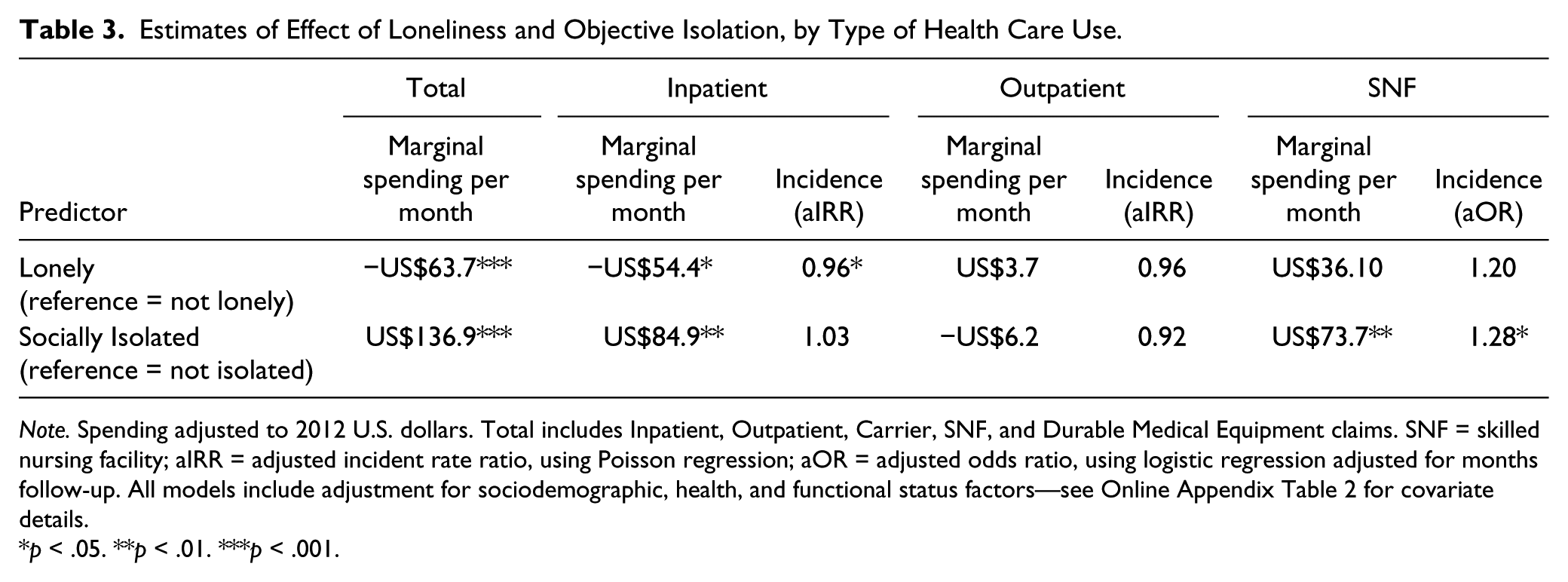
Note. Spending adjusted to 2012 U.S. dollars. Total includes Inpatient, Outpatient, Carrier, SNF, and Durable Medical Equipment claims. SNF = skilled nursing facility; aIRR = adjusted incident rate ratio, using Poisson regression; aOR = adjusted odds ratio, using logistic regression adjusted for months follow-up. All models include adjustment for sociodemographic, health, and functional status factors—see Online Appendix Table 2 for covariate details.
p < .05. **p < .01. ***p < .001.
In subanalysis by type of care (Table 3), we found similar patterns for inpatient spending, with isolation predicting higher (+US$85/month) and loneliness predicting lower inpatient spending (−US$54/month) after full adjustment. There was, however, no statistically significant difference in outpatient spending predicted by loneliness, or by isolation. Poisson regression of frequency of inpatient and outpatient use showed loneliness predicted less frequent use of both types of services (incidence rate ratio of 0.96 for each); however this was only statistically significant for inpatient care. Isolation, but not loneliness, predicted increased spending on SNF care (+US$74/month, p < .001); both predicted increased likelihood of receiving any SNF care, but only reached statistical significance for isolation (adjusted odds ratio = 1.28, p = .04) not loneliness (1.20, p = .05).
Unadjusted analysis suggested both loneliness and isolation were associated with approximately 40% higher annual mortality during follow-up (Table 2; Online Appendix Figures 2 and 3). After fully adjusting for sociodemographic and health factors with Cox hazard regression (Table 4) isolation, but not loneliness, significantly predicted higher mortality with a 31% (p < .001) increase in the risk of death.
Loneliness and Objective Isolation as Predictors of Death in Medicare Beneficiaries, HRS 2006-2010, Cox Hazard Regression.
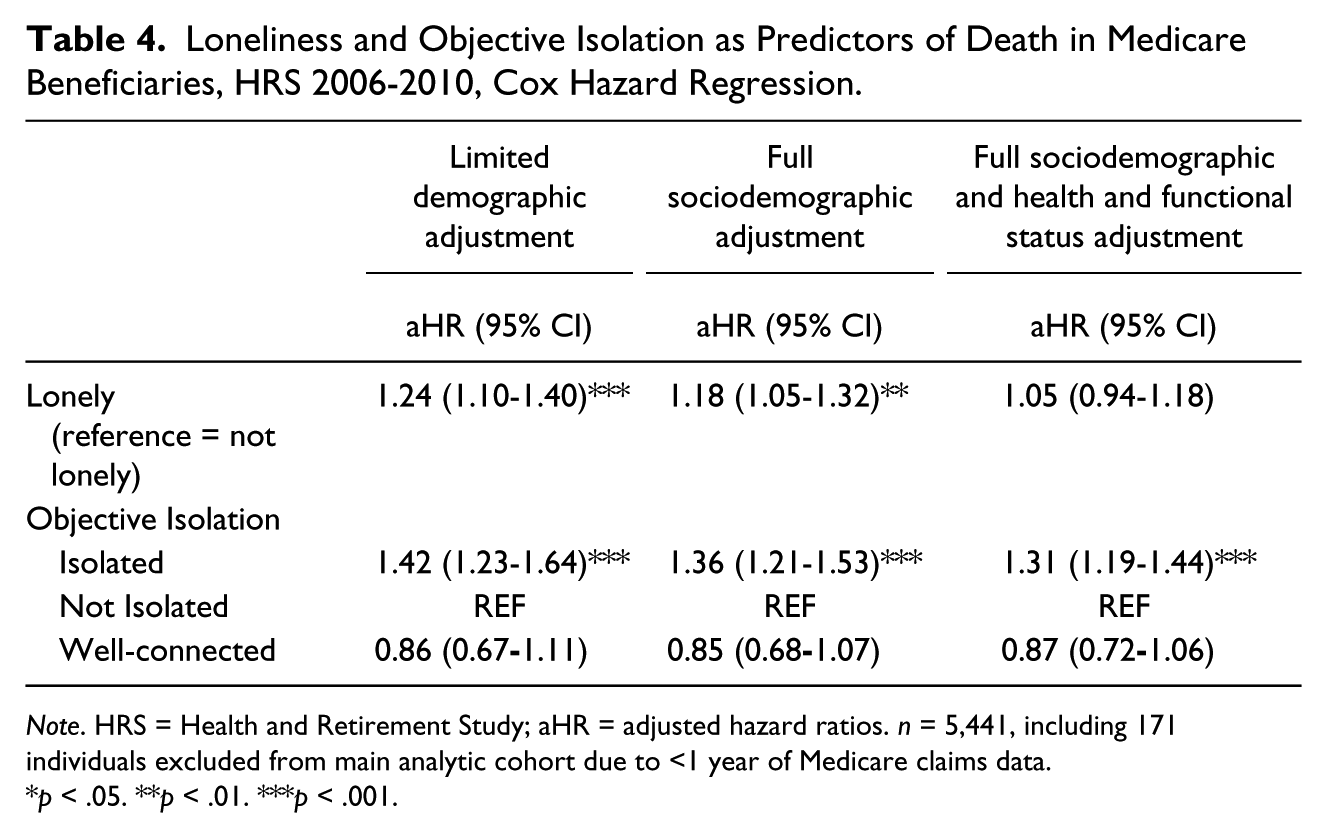
Note. HRS = Health and Retirement Study; aHR = adjusted hazard ratios. n = 5,441, including 171 individuals excluded from main analytic cohort due to <1 year of Medicare claims data.
p < .05. **p < .01. ***p < .001.
Last, in our sensitivity analyses exploring the robustness of our results, alternative measures and modeling assumptions had little effect on the overall findings (see Online Appendix Sensitivity Analysis). Notably, depression consistently demonstrated an opposite effect on spending compared with loneliness. Subpopulation analysis by marital status (married, widowed, unmarried) reduced our power to detect significance, but suggested objective isolation was most prominently a predictor of increased spending (+US$273/month, or US$3,276 annually, p < .05) in the 27% of our cohort that was widowed; loneliness was most markedly associated with reduced spending (−US$489/month, or US$5,868 annually, p < .01) in the 11% of our cohort that was unmarried (see Online Appendix Table 3).
Discussion
This study is the first to measure the association between loneliness, objective isolation, and health expenditures in the Medicare population. We find that objective isolation is associated with increased Medicare spending, while loneliness’s association appears opposite. In general, Medicare spends an estimated US$1,643 more annually on objectively isolated beneficiaries than on similar individuals with greater social connections. The increased spending is more pronounced for widowed seniors: Medicare spends US$3,276 more per year on beneficiaries who are dually widowed and isolated, than on their widowed peers who are not isolated. We did not find that increased spending on isolated beneficiaries produced better outcomes (i.e., reduced hospitalization or mortality). Instead, adjusting for differences in initial health status, we found that objectively isolated individuals used more skilled nursing services and had over 30% higher annual risk of death.
Conversely, we find that Medicare spends US$768 less per year on lonely beneficiaries than it does for similar beneficiaries (i.e., after adjusting for health status) who do not report being lonely. This latter finding suggests that loneliness might be a barrier to accessing health care, while the former suggests that providing objective social support to older adults (especially the widowed) has potential to reduce health care spending.
While several prior works have explored psychosocial contributors to accessing health services (Babitsch, Gohl, & von Lengerke, 2012), most have not explicitly measured health care spending or focused on the ever-growing Medicare population. Our study adds a contemporary perspective particularly relevant in the era of cost-containment and, together with studies such as Unützer et al. (2009) showing depression predicts higher Medicare costs (incidentally reconfirmed in our models), forms a nascent body of work exploring psychosocial influences on Medicare spending.
As we hypothesized, we confirm that loneliness and objective isolation are more prevalent in those with poor health status and poorer socioeconomic indicators, and (once adjusting for those factors) the two forms of social isolation are distinct with regard to health care use patterns. Among the various hypothesized pathways by which social isolation might influence quantity of health care used—including potentially increased use (e.g., due to lack of social support’s “buffering” effect against stress and illness) and decreased use (e.g., via less presentation to care due to lack of facilitating social agents; Gourash, 1978)—we demonstrate that objective isolation’s net impact is an increase in total health care use. As we expected, we found that SNF use is higher among objectively isolated. The degree to which increased SNF care spending appears to contribute to the total increased spending for objectively isolated is impressive and, we propose, also intuitive as it likely reflects those with less robust social supports are more likely to be directed to “nursing home” care post-hospitalization, rather than home with assistance from their social supports. We did not confirm our hypothesis that outpatient spending would be more influenced by social isolation, despite its potentially more elective nature. This may in part reflect a lack of statistical power, as outpatient care is cheaper and a small fraction of total health care costs in our cohort. The trend toward less frequent outpatient care we observed (incident rate ratio [IRR] = 0.92, p = .1) for beneficiaries who were objectively isolated suggests such isolation may present a barrier to accessing outpatient care, which remains compatible with a possible substitution effect of higher cost inpatient and SNF care for lower cost outpatient care.
Loneliness is extremely common among older adults (Theeke, 2009; Wilson & Moulton, 2010). A majority (55%) of Medicare beneficiaries in this nationally representative sample met our criteria for being lonely. Though objective isolation is not as common (14% within our cohort), it nevertheless affects a substantial proportion of the American older adult population—17% of seniors live alone, putting them at high risk of isolation (Ortiz, 2011). Given the scope of the problem, as well as the differential effect of objective isolation and loneliness on Medicare spending, our findings suggest two distinct responses.
The first, in response to objective isolation, is clear and involves efforts to promote concrete assistance for those who are isolated. At the level of the health care delivery, innovative care models that incorporate social assessment and linkage to social support services hold promise for significant cost savings. Already several such programs (largely arising from new incentives and initiatives of the Affordable Care Act, such as the Healthcare Innovation Challenge Awards) have shown some early promise to reduce costs (Shier, Ginsburg, Howell, Volland, & Golden, 2013). Our study findings lend additional optimism that cost savings (in addition to improved well-being) can be found via care models that assess and address objective social support gaps.
Clinicians and policy makers alike have a role in responding to increasing evidence of social isolation’s influence. Clinicians can help identify social isolated patients by asking about social network and support structures. The Center for Medicare and Medicaid Services (CMS) can play an important role by reimbursing interventions that address social isolation. Encouragingly, CMS leadership has demonstrated exploratory steps in this direction as, in their own words, “CMS is testing various approaches for medical practices, including methods for linking practices and patients to social support services” through their Innovation Center (Kassler, Tomoyasu, & Conway, 2015, p. 109).
The second call to action, for loneliness, is more nuanced, but begins with increased recognition of its prevalence, its co-occurrence with poor health, and its potential role as a barrier to seeking care. In light of our findings, this effort need be justified, rightly, more on the basis of reducing suffering than on potential cost savings. Our finding of loneliness’s inverse association with spending (after adjusting for health status) may be less important than our re-demonstration of its strong correlation and co-occurrence with poorer socioeconomic, mental and physical well-being—that is, reported loneliness might provide a simple and useful marker of high risk older adults in need of intervention. This idea is supported by Pitkala, Routasalo, Kautiainen, and Tilvis’s (2009) randomized control trial of psychosocial group rehabilitation targeted explicitly at lonely older adults which intriguingly showed, despite no effect on reported feelings of loneliness (Routasalo, Tilvis, Kautiainen, & Pitkala, 2009), significantly improved self-reported health and reduced mortality and health care spending.
We demonstrate loneliness is a more prevalent form of psychological distress than depression, suggesting clinicians can play an important role in identifying and addressing loneliness (similarly as they do for depression), for example, with a simple questionnaire such as the three-question loneliness scale (Hughes et al., 2004). Once identified, they can offer referral to appropriate social and behavioral health resources. While the most effective management of loneliness per se remains uncertain, a recent meta-analysis of interventions to reduce loneliness showed consistent support for approaches that addressed maladaptive social cognition, such as cognitive-behavioral therapy (CBT; Masi, Chen, Hawkley, & Cacioppo, 2011). Whether the reductions in reported loneliness seen with CBT alter subsequent health and health care use warrants future investigation.
As with any study, ours has limitations. We focus on community dwelling, fee-for-service (Medicare Parts A and B) beneficiaries. Social isolation’s relationship to spending may be different within Medicare Advantage, which historically attracts a healthier population (McWilliams, Hsu, & Newhouse, 2012). However, examining the >3,000 excluded HRS respondents aged 65+ with Medicare Advantage, we found no difference in rates of loneliness and objective isolation, and only minimal skew toward a younger healthier population compared with our analytic cohort (M age 72 vs. 73, and M count of chronic conditions 2.2 vs. 2.3). Regardless, future study of social isolation in managed care and nursing home populations is warranted. Another concern is that our definition of loneliness is overly sensitive, with half of beneficiaries meeting our criteria; however, our cohort’s prevalence of loneliness only somewhat exceeds that reported (43%) in a slightly younger HRS sample, of adults age 60 and above, in work by Perissinotto et al. (2012), which demonstrated the same definition of loneliness reliably predicted increased risk of functional decline (twofold) and mortality (45% increase). Furthermore, as described in our methods, when we explored the option of using an additional threshold to discriminate “very lonely” respondents, we found this small fraction of respondents were not distinct in their health care spending compared with the plurality of “mildly lonely.”
As with all observational studies, unobserved differences, including residual differences in baseline medical complexity, could bias the observed findings. However, the fact that loneliness and objective isolation switch from having parallel associations (without adjustment) to having opposite associations once we adjust for best available health measures makes it unlikely that more complete adjustment for health would reverse this overall finding. Conversely, given the reversal of loneliness’s effect once adjusting for health status, it is possible our health covariates include yet unrecognized pathways (rather than confounders) by which loneliness influences health care patterns—for example, if loneliness were to directly cause increased substance use, hypertension, or other such conditions, adjusting for these health factor might attenuate loneliness’s true impact on health care spending by excluding these mechanisms from the effect estimate. Last, analysis of two closely related constructs raises concern for collinearity and interactions that could bias results; however, in addition to our reassuring findings of limited correlation and lack of multicollinearity, we tested modeling each construct alone and found the effects of objective isolation and loneliness were consistent regardless of whether we adjusted for the other.
These findings highlight the importance of accounting for both forms of social isolation and approaching them distinctly in future research and when devising policy solutions. Novel health care initiatives that focus on maximizing objective social supports and connectedness merit further funding and evaluation, as reducing objective isolation is not only inherently valuable to affected individuals but also holds promise for reducing health care spending.
Footnotes
Acknowledgements
Sincere thanks to Lena Schoemaker of Stanford University for analytic support. Data use was by permission of the Health & Retirement Study, University of Michigan, and the Centers for Medicare and Medicaid.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging at the National Institutes of Health (AG017253 to J.G.S. and J.B.) and the AARP Public Policy Institute.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.