
Abstract
This study examined the prevalence and the impact of fear of falling (FOF) on physical activity (PA), sedentary behavior (PA), and physical function in older adults living in a continuing care retirement community (CCRC). Ninety-three older adults were included and self-reported assessed on PA and SB. Further, participants’ physical function was assessed using a collection of measures of valid objective tests. Independent t test was used to compare the dependent variables between FOF groups, and analysis of covariance (ANCOVA) was used to control for assistive device usage. FOF was prevalent in 47.3% of the sample and PA and SB did not differ between FOF groups (p > .05). ANCOVA revealed that performance on several physical function tests remained significantly better (p < .05) for the no FOF group compared to the yes group. Our findings demonstrated similar levels of PA and SB between FOF groups, but worse physical function for older adults reporting FOF.
• The prevalence of fear of falling in older adults living in a continuing care retirement community is similar to the prevalence observed in older adults from the general population. • Self-report physical activity and sedentary time are not different between groups of older adults living in a continuing care retirement community with and without fear of falling. • Fear of falling negatively impacts physical function in older adults living in a continuing care retirement community.
• Fear of falling should be given as much attention as falls, and not only as its “side-effect”. Thus, our results help inform strategies and interventions that should be, in parts, different from those developed specifically to target falls. • Additional research is needed to demonstrate that reducing fear of falling in this population will lead to increased physical activity participation, reduced sedentary behavior, and improved physical function.What this paper adds
Application of study findings
Introduction
Falls are highly prevalent among older adults, representing a significant public health concern due to their health-related consequences and economic burden (Florence et al., 2018; James et al., 2019; Leilei et al., 2019). This is manifested through substantial medical expenditures required to treat fall-related injuries. Recent data from the United States indicate that 27.5% of individuals aged 65 years and older reported at least one fall in the previous year and approximately 10% reported a fall-related injury (Moreland & Ramakrishna Kakara, 2020). Another significant consequence of falls is the development of fear of falling (FOF). FOF is characterized by a persistent concern about falling and affects a significant portion of the older adult population, particularly those who have previously experienced a fall in the past. Previous studies indicate that FOF is reported by 20–60% of older adults living in the community (Martínez-Arnau et al., 2021; Su et al., 2021; Van Haastregt et al., 2007).
FOF has been identified as an independent risk factor associated with reduced quality of life (Schoene et al., 2019), reduced participation in daily activities (i.e., activity curtailment) (Liu et al., 2021), and an increased risk of falls (Martínez-Arnau et al., 2021). Additional evidence suggests that older adults living in rural areas who report FOF demonstrate lower scores in functional tests compared to their counterparts without FOF (Su et al., 2021). As previously described, FOF is associated with reduced daily activities, potentially leading to a further decline in physical activity participation, an increase sedentary behavior, and an overall reduction in physical function capacity.
Most studies addressing FOF have primarily focused on older adults in the general population, and not much is known about factors associated with FOF in older adults living in community-dwelling facilities such as Continuing Care Retirement Communities (CCRCs). This is important because there is evidence suggesting that older adults living in these facilities may experience a higher prevalence of falls and FOF compared to their counterparts in the general population (Okoye et al., 2021). Both falls and FOF in these settings are believed to be influenced by cultural, environmental, and facility-related factors (e.g., age-related changes in physical capacity, reduced physical activity participation, poor ambulatory surfaces, and unfavorable attitudes towards walking aids) as well as intrinsic factors (e.g., psychological factors, concentration/attention, socio-demographic factors, and morbidity-related factors) (Okoye et al., 2021).
Continuing Care Retirement Communities, a type of facility-based long-term care service, provide different levels of care, including independent housing (houses or apartments), assisted living, and skilled nursing care, all in one location (Krout et al., 2002). Despite falling under the same umbrella category of community-dwelling facility, CCRCs differ from senior housing in the level of care and services offered. CCRCs provide a more comprehensive continuum of care, allowing residents to age in place. On the other hand, senior housing, despite offering several housing levels, generally provides a specific level of care (Carroll & Qualls, 2014).
Building upon previous studies that explored FOF in older adults from the general population and the limited scientific literature on those living in community-dwelling facilities such as CCRCs, this study examined the impact of FOF on physical activity, sedentary time, and physical function in older adults living in a CCRC. We hypothesized that older adults reporting FOF would report lower levels of physical activity, spent more time in sedentary behavior, and demonstrate worse physical function compared to their counterparts without FOF.
Methods
Study Design
This cross-sectional study represents a secondary analysis of data from a previous study that explored sedentary behavior, cognition, and physical function in older adults living in a CCRC (Sebastião, 2020; Sebastião et al., 2019). The original study protocol received approval from a university Institution Review Board and was conducted in accordance with the Declaration of Helsinki. Additionally, all participants provided informed consent before data collection.
Participants Recruitment and Setting
Prospective participants were recruited from a single CCRC facility located in the Midwest region of the United States, specifically in the State of Illinois. This facility was selected based on its long-lasting collaboration with the researcher’s institution, and it offers four different types of living options—namely, independent apartments, duplex living, personal care apartments, and licensed healthcare (i.e., assistance needed 24 h). Due to the purpose of the original study, data were exclusively collected from residents in independent apartments, duplex living, and personal care apartments (whether fully or partially independent) who met the eligibility criteria. Residents in the licensed healthcare unit, requiring 24/7 care, were excluded from participation. Inclusion criteria comprised being at least 60 years old, the ability to walk with or without the use of assistive devices (e.g., cane or walkers), absence of conditions exacerbated by physical tests, no significant cognitive impairment (assessed by the ability to engage in a coherent conversation), and residency in the independent living units within the facility. Exclusion criteria included residents in the licensed healthcare unit during data collection. According to CCRC records, excluding those living in the licensed healthcare unit, the facility housed 236 residents aged 60 years and over at the time of data collection. Recruitment and assessment were conducted with a convenience sample of 100 older adults. This final sample represents approximately 42% of the eligible population. However, a data check revealed that seven participants had missing data on key questions related to the present study (e.g., fear of falling), and were therefore excluded from the final analysis.
Assessments
Fear of Falling
Fear of Falling was assessed through the following question: “Are you afraid of falling (yes/no)?” Participants responding “yes” to this question were classified as having FOF. This specific question has been employed in previous studies (Asai et al., 2022; Jaatinen et al., 2022), with researchers reporting a moderate agreement (87.8%, Kappa = 0.57) between this single question and the gold standard questionnaire: fall Efficacy Scale–International (FES-I; specificity 86%; sensitivity 74%, negative predicting value 89%, positive predicting value 69%) (Belloni et al., 2020).
Activity Behavior
Physical activity (PA) and sedentary behavior (SB) were assessed through self-reported. PA was measured using the valid Physical Activity Scale for the Elderly (PASE) (Washburn et al., 1993). The PASE is a ten-item instrument designed to assess PA in large samples of older adults over a 1 week period. This instrument can assess activities performed in different domains, including leisure, yard work, home, and caregiving, with scores expressed as activity counts. SB was measured using a valid questionnaire developed for older adults (Visser & Koster, 2013). The questionnaire consists of ten questions related to screen and non-screen time activities. The total SB was calculated by summing the time reported by participants in each of the ten questions and expressed as minutes per day. This questionnaire has demonstrated acceptable test–retest reliability (0.71), and its scores have been found to be moderately associated (r = .35) with accelerometer-determined sedentary time (Visser & Koster, 2013).
Physical Function
Physical function was assessed using a collection of measures. The Timed Up and Go (TUG) was used as a measure of functional mobility (Podsiadlo & Richardson, 1991), the Timed 25-foot Walk test (T25FW) was used as a measure of walking speed, the Short Physical Performance Battery (SPPB) (Guralnik et al., 1994) was used as an overall measure of lower-extremity function, and the 30 s Chair Stand test (30CST) was used as measure of lower-extremity functional strength (Rikli & Jones, 1999). For the SPPB, the analysis considered each subcomponent (i.e., balance, gait, and lower-extremity muscular strength) along with the summary/total score. High scores across the subcomponents and overall (i.e., summary/total) indicate better physical function.
Other Variables
A sociodemographic and health questionnaire was used in the study for the purpose of sample characterization. Collected information included: sex (male/female), age (years), race/ethnicity (American Indian, Asian, Black/African American, Native Hawaiian/Pacific Islander, Latino(a), White), number of falls in the past 12 months (latter categorized as zero falls or one or more falls), number of medications, diagnosed chronic diseases, and use of assistive device (yes/no).
Analysis
Data were analyzed using SPSS 26.0 statistical software (IBM Corp IBM SPSS. Armonk, NY), with significance set at p < .05. Descriptive statistics were employed for sample characterization. The sample proportion (prevalence) of FOF, along with a 95% confidence interval (95% CI), was calculated using the Clopper-Pearson interval or exact interval method. Differences between FOF groups (no FOF vs. yes FOF) on the main outcomes—physical activity, sedentary time, and physical function—were assessed using t test for independent samples. Effect sizes were computed based on Cohen’s d and interpreted as small (0.1), moderate (0.3), and large (0.5) according to standard criteria (Cohen, 2013). Given the significant difference in the number of individuals using assistive devices to walk between FOF groups, we conducted an analysis of covariance (ANCOVA). The ANOVA was controlled for the use of assistive device in the outcomes that were found to be significant in the univariate analysis.
Results
Participant Characteristics
General Demographic and Health Characteristics of the Sample Overall and Separated by Fear of Falling Status.
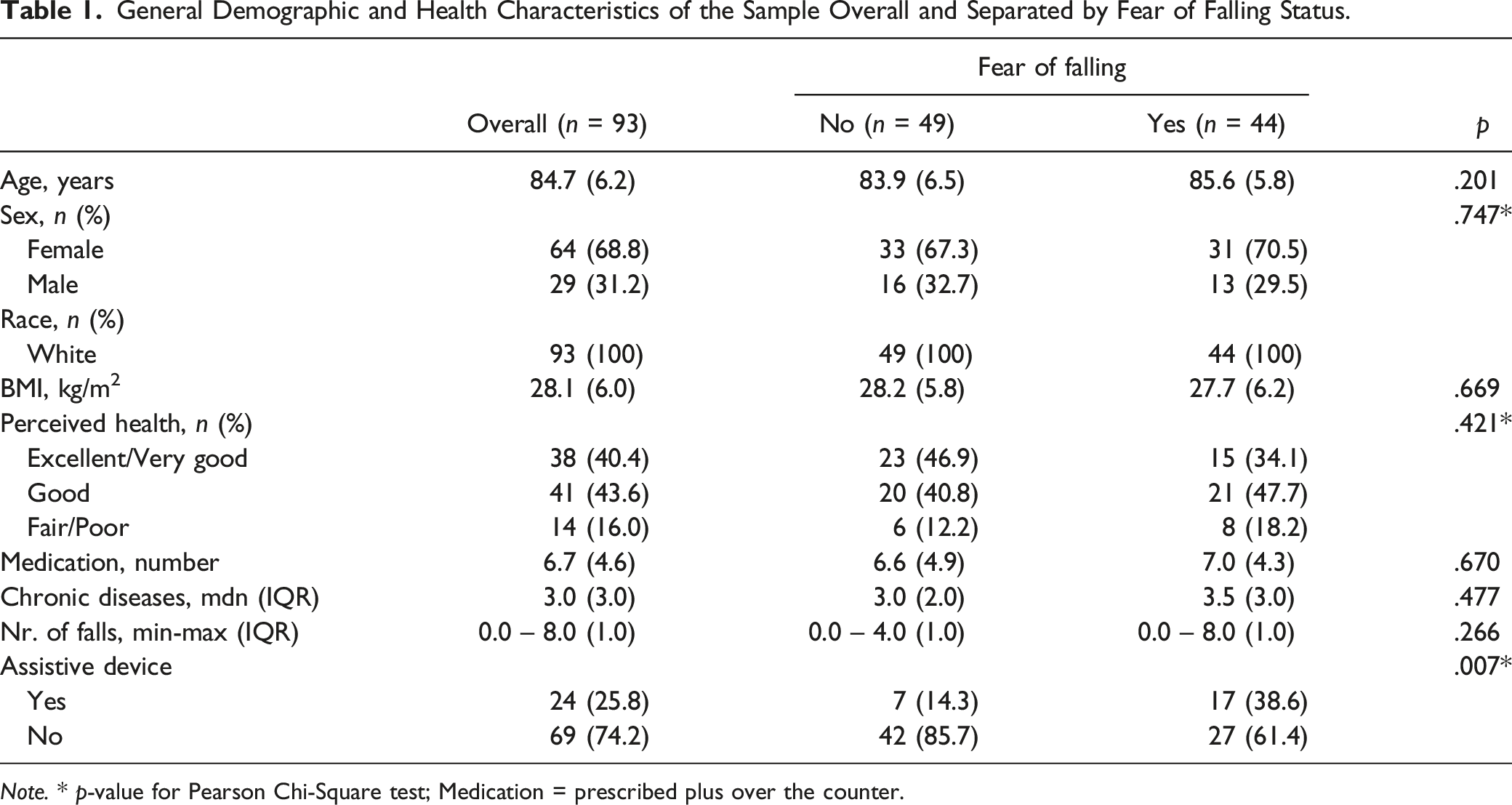
Note. * p-value for Pearson Chi-Square test; Medication = prescribed plus over the counter.
Prevalence of Fear of Falling
A total of 93 older adults were included in the study. The overall prevalence of FOF in our sample was found to be 47.3% (95% CI [36.9%–57.9%]). Of those reporting having FOF, 38.6% reported using an assistive device for walking. Further analysis stratified by sex revealed an FOF prevalence of 48.4% (95% CI [35.8%–61.3%]) among older women and 44.8% (95% CI [26.4%–64.3%]) among older men. No significant difference in FOF prevalence was observed based on sex, χ2 (1, N = 93) = 0.104, p = .747. Additionally, among older adults reporting zero falls in the past 12 months, the prevalence of FOF was 43.9% (95%CI [30.7%–57.6%]), while those reporting one or more falls in the past 12 months had a prevalence of 52.8% (95%CI [35.5%–69.6%]). There was no significant difference in FOF prevalence based on fall history, χ2 (1, N = 93) = 0.704, p = .401.
Physical Activity, Sedentary Behavior, and Physical Function
Mean and Standard Deviation Values of Physical Activity, Sedentary Behavior, and Physical Function Overall and Separated by Fear of Falling Groups.
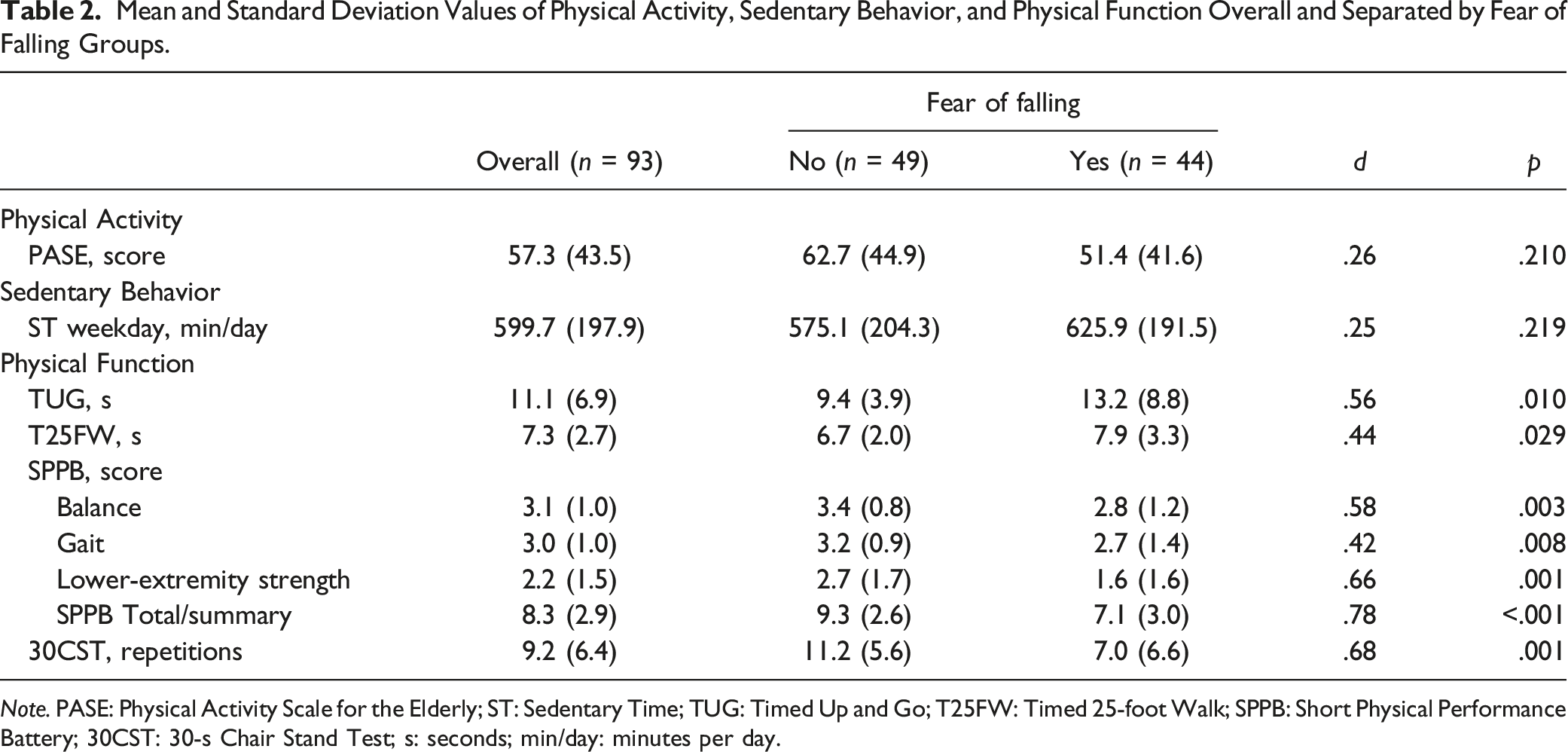
Note. PASE: Physical Activity Scale for the Elderly; ST: Sedentary Time; TUG: Timed Up and Go; T25FW: Timed 25-foot Walk; SPPB: Short Physical Performance Battery; 30CST: 30-s Chair Stand Test; s: seconds; min/day: minutes per day.
Analysis of Covariance
The use of assistive device was found to be significantly different between FOF groups (no FOF vs. yes FOF; Table 1). Further analysis using ANCOVA controlling for the use of assistive device demonstrated that subcomponents of the SPPB, including balance (mean [SE]: no FOF, 3.3 [0.1] vs. yes FOF, 2.9 [0.01]; p = .041), lower-extremity strength (mean [SE]: no FOF, 2.5 [0.2] vs. yes FOF, 1.9 [0.2]; p = .031), and the SBBP summary/total (mean [SE]: no FOF, 8.8 [0.3] vs. yes FOF, 7.7 [0.3]; p = .015), remained significantly different between FOF groups, favoring the no FOF group. In addition, even after accounting for assistive device use, performance in the 30 s Chair Stand Test (30CST), indicating muscular endurance, remained significantly different between FOF groups, favoring the no FOF group (mean [SE]: no FOF, 10.2 [0.7] vs. yes FOF, 8.1 [0.7]; p = .045). No significant differences were observed in Timed Up and Go (TUG) performance (mean [SE]: no FOF, 10.4 [0.8] vs. yes FOF, 12.1 [0.8]; p = .158), Timed 25-Foot Walk (T25FW) performance (mean [SE]: no FOF, 7.0 [0.3] vs. yes FOF, 7.5 [0.4]; p = .326), and SPPB subcomponent gait (mean [SE]: no FOF, 3.0 [0.1] vs. yes FOF, 2.9 [0.1]; p = .226).
Discussion
The present study investigated differences in activity behavior (i.e., PA and sedentary time) and physical function among older adults living in a CCRC facility in the Midwest region of the United States, based on the presence of FOF. Our main findings include: (1) a relatively high prevalence of FOF independent of sex or fall history, (2) no significant difference in PA or SB between FOF groups, and (3) reduced physical function among older adults reporting FOF, even after controlling for assistive device use. Our findings partially support our hypothesis that FOF would be associated with low levels of PA, high amounts of sedentary time, and reduced physical function among older adults living in a CCRC.
The prevalence of FOF in older adults of the general population has varied considerably (20%–60%) (Dhar et al., 2022; Martínez-Arnau et al., 2021; Su et al., 2021; Van Haastregt et al., 2007). This variation is also notable in older adults with history of severe fall-related injuries, ranging from 21% to 95% (Jørstad et al., 2005; Scheffer et al., 2008). A study focusing on individuals aged 60 years and older, attending an outpatient hospital department, reported a prevalence of FOF at 42% (Dhar et al., 2022). Another study involving older Canadians residing in public housing in Ontario observed a prevalence of 39% among residents. The authors further demonstrated that males had a significantly lower odds of experiencing FOF compared to females, while alcohol consumption was associated with increased odds of FOF (Pirrie et al., 2020). In a recent large-scale study utilizing the National Health and Aging Trend Study, which the evaluation methods were the same as our study, researchers observed a prevalence of 48.8% for FOF in older adults who experienced a fall in the previous year, and 46.8% in those who experienced a fall in the previous month (Chen et al., 2021). Our results corroborate somehow with those observed in older adults from the general population. Despite not observing a significant different FOF prevalence based on fall history (presence x absence), we observed higher absolute values in those reporting previous falls compared to the National Health and Aging Trend Study. Moreover, our finding on FOF prevalence was higher compared to those observed in the Canadian study. However, unlike the Canadian study, we did not observe a significant difference in FOF prevalence based on sex. Variations in FOF prevalence across studies may be partly attributed to differences in assessment methods and the characteristics of the population under investigation.
Our findings demonstrated differences in the subcomponents of the SPPB, namely, balance, lower-extremity strength, and the overall summary/total score, as well as in the 30 Second Chair Stand Test between groups experiencing FOF and those not reporting FOF. Importantly, the differences remained significant even after accounting for the use of assistive device to walk, with the group reporting no FOF presenting with better performance in the physical function tests compared to their counterparts with FOF. Our findings corroborate results from previous studies on FOF and physical function in older adults from the general population (Huang et al., 2022; Su et al., 2021). For example, Huang et al. conducted a study involving 105 older adults, investigating the association between FOF and seven common physical function measures. Their results, after controlling for age, suggested that participants reporting FOF performed significantly worse in physical performance tests assessing balance (i.e., Berg Balance Scale), lower-extremity function (i.e., SPPB), walking speed, function mobility (i.e., TUG), and lower-extremity strength (i.e., Five Times Sit to Stand Test) (Huang et al., 2022). Similarly, Su et al. investigated the prevalence of FOF and its association with physical function and fall history among older adults (≥75 years old) living in rural areas of China (Su et al., 2021). The findings demonstrated that FOF was independently associated with functional mobility (i.e., TUG), balance (i.e., 4-Stage Balance Test), and fall history in the participants. In addition, previous studies have suggested a direct effect of FOF on physical function performance in older adults (Lee & MoonKi Choi, 2017; Park et al., 2014), including associations with leg muscle strength (Deshpande et al., 2008). Collectively, our findings coupled with results from previous work and suggest a potential association between FOF and reduced physical function in older adults, both in the general population and those living in CCRC. This is a concern because researchers suggest that older adults may limit their daily activities due to FOF (da Costa et al., 2012). Such activity curtailment may contribute to a subsequent decline in muscular strength, creating a detrimental cycle and ultimately affecting their ability and confidence to perform activities of daily living without falling (Liu et al., 2021).
Despite the low level of PA and high amount of sedentary time observed in the participants of our study, we did not observe a significant difference in any of these behaviors between groups of FOF (no FOF vs. yes FOF). This unexpected finding contrasts with previous research suggesting an association between FOF and activity restrictions in older adults (da Costa et al., 2012), which technically result in reduced PA and increased sedentary time. A recent systematic review, exploring the association between objectively measured PA and SB with falls, FOF, and fractures, reported that FOF is associated with lower engagement in PA and increased sedentary time (Ramsey et al., 2022). The inconsistency between our study and the available scientific literature may, in part, be attributed to our chosen method for assessing these behaviors. In our study, both PA and sedentary time were assessed using self-report questionnaires. While these questionnaires have been validated for use among older adults, it is important to acknowledge the challenges associated with self-report assessment of PA and SB, particularly in the older adult population (Ogonowska-Slodownik et al., 2022).
This study comes with limitations. First, the cross-sectional study design employed greatly limits our ability to establish-and-effect, which should be explored by longitudinal studies. Second, the use of a single question to assess FOF, while demonstrating a good level of agreement with established measures such as FES-I, prevents us to identify potential levels of FOF (e.g., moderate and high). This is important because certain outcomes may be influenced by the severity/level of FOF. Additionally, previous research suggests differences in FOF as a function falls (presence or absence) and FOF that may or may not alter activity (e.g., activity restrictions/curtailment). Although we were able to address FOF in the context of the presence or absence of falls in our sample, data on potential activity restriction/curtailment associated with FOF were not collected in the original study. Third, PA and sedentary time were assessed using self-report measures, and self-report assessment of both PA and SB can be challenging among older adults. Future studies should attempt to replicate the present findings but adopting an objective measure of PA and SB such as accelerometer. Lastly, data were collected in a convenience sample of older adults living in a wealthy CCRC located in the Midwest region of the United States, with 100% the participants self-reported as White and nearly 70% were female. Consequently, the generalizability of our findings is limited to this demographic; therefore, caution is need in extrapolating the results to a more diverse population.
Despite the limitations, this study adds to the scarce literature on FOF in older adults living community dwelling facilities such as CCRC and provides valuable information regarding the association between FOF and physical function in this population. Given that FOF is associated with nearly three-fold increase in the risk of falls among older adults (Deandrea et al., 2010), even after adjusting for factors such as age and chronic disease (Chen et al., 2021), it warrants special attention. In addition, FOF appears to be independently associated with the occurrence of falls. For example, an old individual may be afraid of falling, without necessarily having previously fallen in the last year, yet this fear increases the likelihood of falls, particularly for older women (Lavedán et al., 2018; Schoene et al., 2019). Thus, our findings underscore the need for targeted interventions aimed at mitigating risk factors associated with falls, specifically focusing on addressing FOF within CCRC populations.
Our findings suggested similar levels of self-reported PA and sedentary time between groups categorized by FOF (no FOF vs. yes FOF). However, the group reporting FOF presented with significant worse physical function, as demonstrated by the lower scores in the SPPB and its subcomponents (except gait, and 30CST), compared to their counterparts reporting on FOF. Considering the wide range of negative health implications, including physical functional decline, it is important that FOF be given as much attention as falls, rather than addressing as its “side-effect.” Thus, it is important to develop strategies and interventions that should be, in parts, different from those developed specific to target falls. This is because studies need to demonstrate that reducing FOF will lead to increased participation in PA, decreased sedentary time and improved physical function in this population. To this end, the implementation of targeted FOF prevention programs is key to improving health behaviors and physical function of older adults living in CCRC and older adults in the general population, considering the high prevalence of FOF in both groups. In doing so, strategies and interventions of this nature have the ultimate potential to lead to fall prevention, improved overall health, and consequently improved quality of life among this population.
Footnotes
Acknowledgments
The authors would like to thank Oak Crest Senior Housing Community for allowing us to conduct the present work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Protocol/Human Subject
Northern Illinois University Institutional Review Board (Approval Reference Number: HS18-0011).