
Abstract
Introduction
Falls are a common health problem among older people and are an important cause of morbidity, mortality, and increased medical costs (Stevens, Corso, Finkelstein, & Miller, 2006; Terroso, Rosa, Marques, & Simoes, 2014). Similar to falls, fear of falling and associated avoidance of activity may lead to adverse consequences, like functional decline, restriction of social participation, impaired quality of life, increased risk of falling again, and institutionalization (Cumming, Salkeld, Thomas, & Szonyi, 2000; Martin, Hart, Spector, Doyle, & Harari, 2005; Pluijm et al., 2006; Scheffer, Schuurmans, van Dijk, van der Hooft, & de Rooij, 2008; Yamashita, Noe, & Bailer, 2012). Reports indicate that 30% to 50% of the population over than the age of 65 years fall at least once and 15% fall more than twice a year (Gillespie et al., 2009). The fall incidence in old people not only increases with age but is also increased in individuals with comorbidities, physical limitations, and psychological conditions, such as depression (Ambrose, Paul, & Hausdorff, 2013; Boelens, Hekman, & Verkerke, 2013; Gill, Taylor, & Pengelly, 2005). Fear of falling rates among older adults range from 20.8% to 85% (Scheffer et al., 2008; Zijlstra et al., 2007) and is shown to be affected by different factors, such as socio-demographic factors, socio-economic status (SES), and health-related factors (Lach, 2005; Scheffer et al., 2008).
One of the challenges Western countries are facing, in addition to an aging population, is the increase of social and ethnic inequalities in health of the population. In the Netherlands, older people from ethnic minority groups are a very heterogeneous group who makes up an increasing share of the total older population. The proportion of older immigrants is expected to increase in the next decades from 13.3% in 2015 to 18.0% in 2040 (Statistics Netherlands, 2016). In the four largest Dutch cities, the proportions are much higher: 26.5% in 2015 and 44.5% in 2040. Older immigrants from Suriname, Turkey, and Morocco, almost all first-generation immigrants, are considered as the largest minority groups in the Netherlands from non-industrialized countries, constituting 0.96%, 0.73%, and 0.72%, respectively, of the Dutch older population (Statistics Netherlands, 2016). Turkish and Moroccan citizens came to the Netherlands as labor migrants in the 1960s and early 1970s, first (mainly) men on a temporary basis. Later, their families were subsequently reunited with them. Surinamese citizens are a very heterogeneous group, with South Asians and Africans as the largest ethnic subgroups, born in the former Dutch colony “Suriname.” A large majority of them came to the Netherlands during the independence of Suriname. Due to the Dutch colonial history, Surinamese are more familiar with the Dutch culture and language than other migrant groups.
Previous Dutch studies have reported substantial differences in health problems and physical limitations for ethnic minority older people compared with their Dutch counterparts in disfavor of older adults from ethnic minorities (Denktaş, Koopmans, Birnie, Foets, & Bonsel, 2009; El Fakiri & Bouwman-Notenboom, 2015; Schellingerhout, 2004). Furthermore, there are indications that some health problems, including type 2 diabetes (Bindraban et al., 2008; Ujcic-Voortman, Schram, Jacobs-van der Bruggen, Verhoeff, & Baan, 2009) and physical limitations, appear at a relatively younger age in ethnic minorities compared with the Dutch population. Nevertheless, there is little evidence concerning the association between belonging to an ethnic minority and an increased fall risk in the Netherlands. As previous research suggests that Dutch ethnic minorities do not present as favorably as Dutch people on a number of health conditions, which may increase the risk of falls, possible differences in fall accidents and fear of falling may partially be a reflection of differences in health status and SES. Previous international studies, mainly conducted in the United States, have reported ethnic differences in fall accidents. However, the results are contradictory. Most American fall-prevalence studies compare Afro-Americans, Hispanic/Latinos, and Whites or non-Hispanic Whites and have shown a lower fall risk for Afro-Americans compared with Caucasian Americans or non-Hispanic Whites (Alamgir, Muazzam, & Nasrullah, 2012; Cauley et al., 2007; Faulkner et al., 2005; J. T. Hanlon, Landerman, Fillenbaum, & Studenski, 2002; Nicklett & Taylor, 2014). The findings of different systematic reviews consistently reveal lower incidence of self-reported falls among Chinese (Kwan, Close, Wong, & Lord, 2011) and Hispanic older adults (Bloch et al., 2010, Landy, Mintzer, Silva, & Schulman, 2011) compared with Caucasian older adults. Some studies, on the contrary, have shown no ethnic differences in risk for falls (E. R. Hanlon, Delgado-Rendón, Lerner, Hargarten, & Farías, 2013; Reyes-Ortiz, Al Snih, Loera, Ray, & Markides, 2004). In Europe, studies are limited and include other ethnic minority groups than those living in the United States or the Netherlands.
So far, however, there is limited evidence about an association of fear of falling with ethnicity. Some studies in Eastern countries, including Korea and Taiwan, have found that 53% to 76.6% of older people experience fear of falling (Chang, Chi, Yang, & Chou, 2010; Kim & So, 2013). These rates are higher than the rates found among older subjects in Western countries (40.3%-62.6%; Scheffer et al., 2008; Zijlstra et al., 2007). Kumar, Carpenter, Morris, Iliffe, and Kendrick (2014) showed that being from a Black/minority ethnic group is associated with increased odds of fear of falling (Kumar et al., 2014). The differences in results regarding fear of falling may arise not only from the use of different research tools but also from differences in socio-demographic, cultural, and health characteristics of the older people (Scheffer et al., 2008). Nevertheless, these findings point to the direction of an association between ethnicity and fear of falling.
As falls and related problems, such as fear of falling and mobility restrictions, are a significant cause of morbidity and mortality that can affect society as health care utilization and costs increase, it is relevant to identify those older adults at high risk for falls and fear of falling to tailor prevention strategies.
The aim of this study is twofold: to examine (a) whether the prevalence of falling and fear of falling differs between ethnic minority groups living in the Netherlands, hereby focusing on Moroccan, Turkish, and Surinamese older people, in comparison with the Dutch majority of the population; and (b) whether, in addition to other relevant determinants, ethnicity contributes to the differences in falls and fear of falling. Data from the health questionnaire of the Public Health Services in the Netherlands, a cross-sectional study in a sample of community-living individuals, were used for this study to answer these questions.
Design and Method
Study Population and Setting
The data in this study were collected in 2012 as part of a general health questionnaire by the Public Health Services in the Netherlands (van den Brink, 2012). From the municipal population register of the three largest Dutch cities—Amsterdam, Rotterdam, and The Hague—a random sample was drawn of 35,253 non-institutionalized residents aged 19 years and older. In all three cities, the data collection took place at the same period of time, and combinations of different approaches were used. Eligible respondents were approached at least 3 times to fill out the questionnaire on the Internet or on paper. Individuals with a Turkish background received an additional translated version of the questionnaire. At the fourth and last data collection opportunity, non-respondents from the three major ethnic minority groups (e.g., Moroccan, Turkish, and Surinamese) were re-approached by phone and/or visits to offer them help with filling out the questionnaire or, if needed, to conduct the interview in the respondent’s preferred language. The present study only used data of 8,892 respondents aged 65 years and older. Response rates differed across ethnic groups and cities, and were 57.7% to 60.4% among Dutch, 22.5% to 32.6% among Moroccan, 27.7% to 30.3% among Turkish, and 39.9% to 55.0% among Surinamese older adults. Medical ethics approval was not necessary as particular treatments or interventions were not offered or withheld from respondents. The integrity of respondents was not threatened as a consequence of participating in the study, which is the main criterion in medical-ethical procedures in the Netherlands. Informed consent, in terms of information giving and maintaining confidentially, was respected.
Measurements
The health questionnaire consisted of questions, focusing on socio-demographic characteristics, including age, level of education, and marital status; physical health and limitations; fall accidents and fear of falling; lifestyle risk factors, including alcohol use and physical activity; and psychological health, including depressive symptoms and loneliness.
Falls and fear of falling
Two dependent variables were considered: the prevalence of falls and fear of falling. For assessing fall prevalence, participants were asked the following question: “How many times did you fall in the past 12 months?” with four answer categories: “never,” “once,” “twice,” and “3 or more times.” “Fallers” were identified as individuals with ≥1 fall in the past 12 months, and “recurrent fallers” were defined as individuals with a fall history, that is, ≥2 falls in the past 12 months. Fear of falling was measured by the question “Are you afraid of falling?” with five answer possibilities: “ never,” “almost never,” “sometimes,” “often,” or “very often” (Amsterdam and Rotterdam), or a dichotomous answer “yes” or “no” (The Hague). The answer options “never,” “almost never,” and “no” were denoted as “no fear of falling,” and the answer options “sometimes,” “often,” “very often,” and “ yes” were denoted as “having fear of falling.” Fear of falling was analyzed by using a dichotomized variable dividing the subjects into two groups according to their responses to the question: (a) no fear of falling and (b) having a fear of falling.
Determinants of falling and fear of falling
The independent variable was ethnicity, Dutch, Moroccan, Turkish, or Surinamese, which was determined by the country of birth of the respondents and/or his or her parents (Statistics Netherlands, 2016). Respondents with a Dutch ethnicity were used as reference group.
Variables that have been identified by earlier studies as risk factors or determinants for falls or fear of falling were grouped into the following categories: socio-demographic variables, physical health, lifestyle indicators, and psychological factors.
Socio-demographic variables included gender, age, education, income, and marital status. Educational level was measured by asking the respondent the highest achieved educational level and was divided into three categories: The highest educational level was used as reference category. Annual income concerned the household income (5 quintiles) adapted for the number of persons who depended on it (one or more). Statistics Netherlands (www.cbs.nl) enriched the data set with information on household income which was provided by the Dutch tax authorities. For the analyses, the 5 quintiles were recoded to 4 quintiles, with the highest quintile as the reference category. In marital status, the categories “single/never married,” “divorced or separated,” and “widowed” were denoted as “living alone,” with married/co-habituated as the reference category. For neighborhood, data of the municipal personal record database were used to determine whether or not respondents live in a deprived neighborhood. Neighborhoods were considered as deprived according to an accumulation of some indicators and problems, such as urbanization index, and unemployment.
Physical health was assessed by using different variables: perceived health, multimorbidity, and functional limitations. Perceived health was measured by the following question: “How well is your health in general?” Respondents were asked to rate their health as excellent, very good, good, fair, or poor and the answers were recoded as a dichotomous measure: perceived health is fair or poor versus good, very good, or excellent. Multimorbidity was indicated by the presence of two or more chronic conditions from a selection of 19 self-reported chronic conditions for which the subject was under control or treatment of a general practitioner (GP) or a medical specialist. Functional limitations were assessed by means of the Organisation for Economic Cooperation and Development (OECD) long-term disability questionnaire (McWhinnie, 1981), which identifies individuals having one or more limitations in mobility, hearing, or sight. Individuals with no limitations were used as reference category.
Lifestyle indicators that were examined included being overweight, measured by using the body mass index (BMI); alcohol consumption, defined as consuming alcohol or not; and physical activity, which was based on whether or not participants fulfilled the norm for healthy physical activity representing half an hour a day of physical activity for at least 5 days a week.
Psychological factors that were assessed included psychological distress and loneliness. Psychological distress/depression was measured by means of the Kessler Psychological Distress Scale (K10; Kessler et al., 2002), consisting of five items about anxiety and five items about depression, with answer categories ranging from never (0) to always (4). Loneliness was determined by the 11-item De Jong Gierveld Loneliness Scale (De Jong Gierveld & Kamphuis, 1985); response categories were no (0), more or less (1), and yes (2). For both conditions, dichotomized variables were used: depressed/anxious versus not depressed/not anxious (as the reference category), and lonely versus not lonely (as the reference category).
Analysis
Descriptive statistics are presented using data which were weighted by age, gender, ethnicity, and geographical area to reflect the total population that resides in the three cities. Ethnic groups were compared with respect to socio-demographic information, health characteristics, lifestyle, and falls and fear of falling.
Multiple regression analyses were conducted to examine whether ethnicity contributed to the variance in falls and/or fear of falling, when other variables of interest were taken into account. The analyses were conducted stepwise by entering the different types of variables mentioned above into the multiple regressions. First, a regression analysis was conducted with ethnicity exclusively (Model 0). Second, age and gender were added to the model to adjust for the differences in age and gender among the Dutch, Moroccan, Turkish, and Surinamese older adults (Model 1). In the following step, other background characteristics were added to the model, including SES indicators, including the items of educational level and income; whether or not living in a deprived neighborhood; and living conditions (Model 2). Finally, all health determinants, including perceived health, functional limitations and loneliness, and lifestyle factors, including physical activity and alcohol use, were entered into the regression model (Model 3). A comparable regression analysis was performed with fear of falling as the dependent variable. In addition, “experiencing a fall in the previous year” was entered to the model, as this determinant was identified as a risk factor for fear of falling in previous studies.
Fallers, who had at least one fall in the past 12 months, were compared with non-fallers. Recurrent fallers, who experienced at least two falls, were compared with participants who experienced no or one fall in the past 12 months. Individuals experiencing fear of falling were compared with those with no fear of falling. Differences were reported as odds ratios (ORs) with 95% confidence intervals (CIs) for all outcome measures.
All analyses were performed in SPSS 20.0 for Windows by using Complex Samples. Statistical significance level was set at .05.
Results
Background and Health-Related Characteristics
Table 1 shows the background characteristics and health condition of the study sample. Of the 8,892 participants, 7,952 (89.8%) were of Dutch, 165 (1.9%) of Moroccan, 188 (2.1%) of Turkish, and 587 (6.6%) of Surinamese origin. The study included more women than men, but their proportions were not equally distributed according to ethnicity. All ethnic minority groups were, on average, younger, less educated, more frequently living in a deprived neighborhood, and had a lower income than the Dutch older adults. In addition, ethnic minorities tended to have worse health and lifestyle outcomes than the Dutch, except for alcohol use.
Characteristics of the Study Population According to Ethnicity (n, Unweighted; %, Weighted).
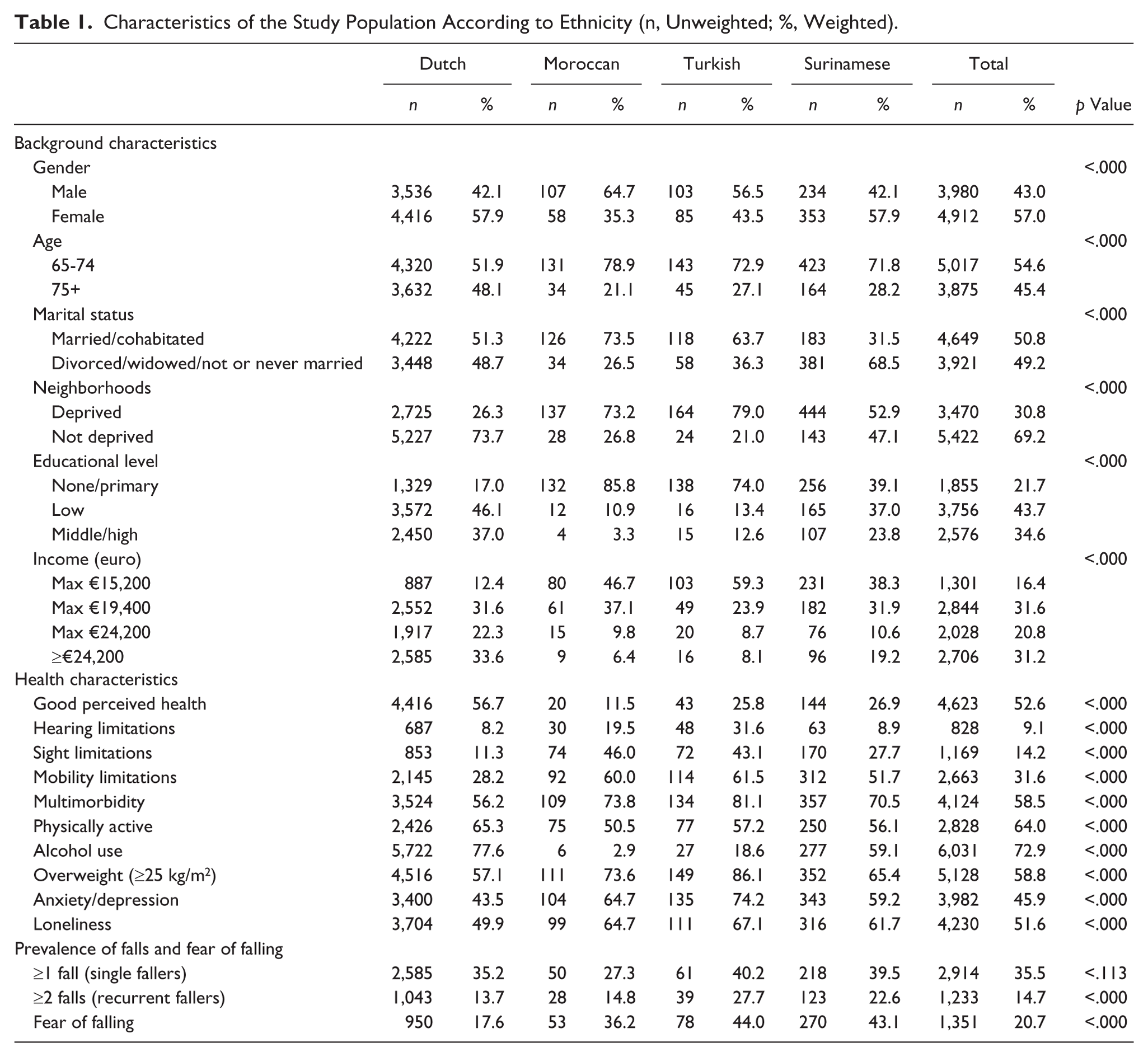
Regarding the prevalence of falls in the previous 12 months, Surinamese and Turkish older adults had the highest scores (40%), followed by the Dutch (35%), whereas the Moroccans had the lowest score (27%; Table 1). There were also differences in the prevalence of recurrent falls—14% in Dutch, followed by Moroccan (15%), Surinamese (23%), and Turkish people (28%). All three older ethnic minority groups experienced more fear of falling (44% Turkish, 43% Surinamese, and 36% Moroccan) than the Dutch (18%).
Determinants of Recurrent Falls and Fear of Falling
The results of the univariate analysis show that almost all socio-demographic and health-related factors were significantly associated with recurrent falls and fear of falling, with the exception of alcohol use, and having a low educational level in the case of falls (Table 2). The characteristics older age, a female gender, living alone, living in a deprived neighborhood, income <€19,400, greater functional limitations, greater multimorbidity, poor perceived health, depressive symptoms, and loneliness were associated with a higher OR of a recurrent fall or fear of falling. With regard to educational level, having none/primary education significantly increased the ORs for both falls and fear of falling, and a low educational level increased only the OR for fear of falling.
Results of the Univariate Logistic Regression Analysis for the Dependent Variables (Falls and Fear of Falling) and Socio-Demographic and Health-Related Variables (OR and 95% CI).
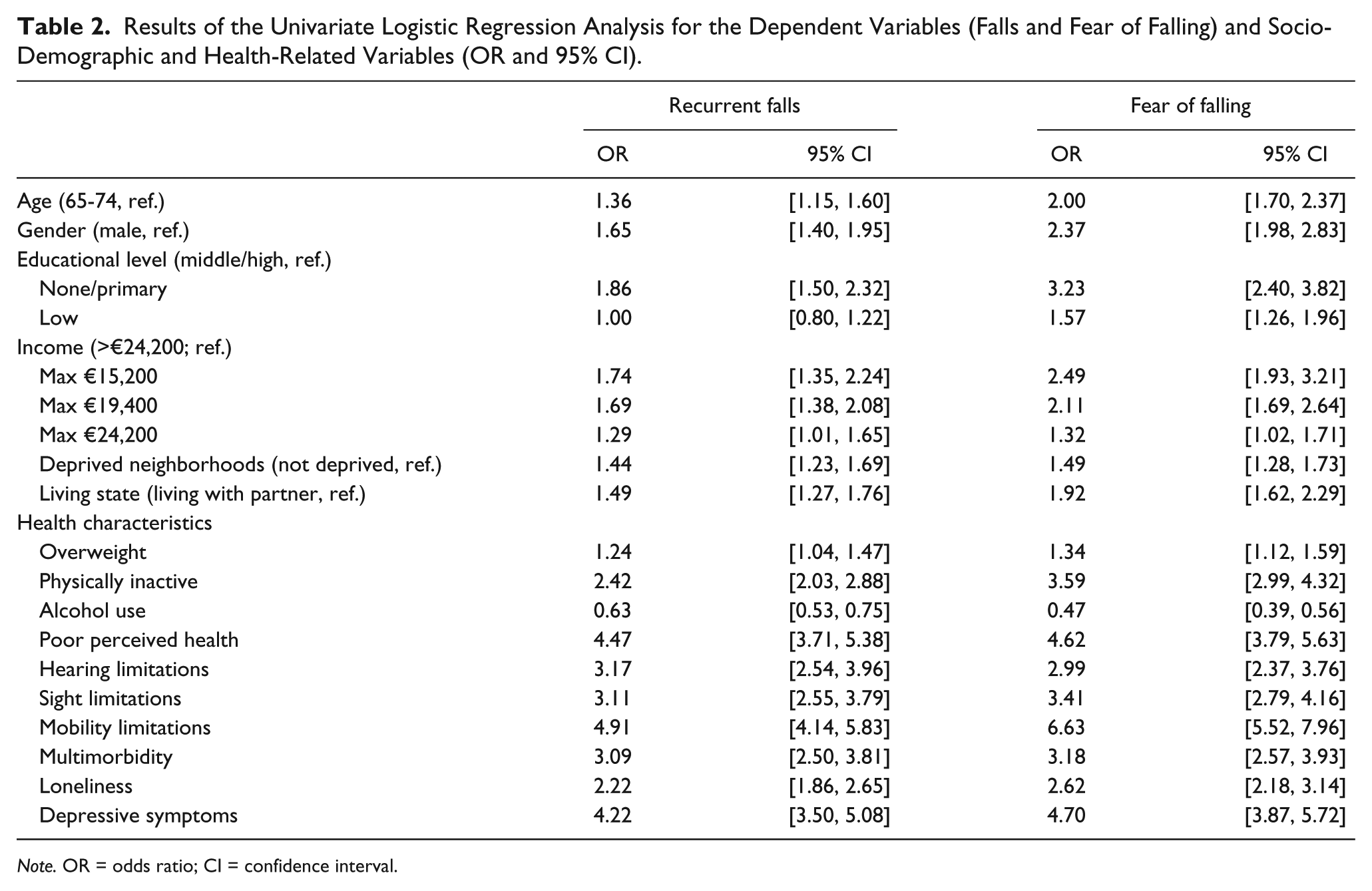
Note. OR = odds ratio; CI = confidence interval.
Among lifestyle factors, physical inactivity and overweight were associated with a higher OR, whereas alcohol use with a lower OR of falling and fear of falling.
Ethnic Differences in Fall Accidents and Fear of Falling
The results of the regression models for falling and ethnicity are shown in Table 3. Turkish and Surinamese ethnic backgrounds were associated with a higher rate of falls compared with a Dutch ethnic background (OR = 2.41, 95% CI = [1.48, 3.94] for the Turkish; and OR = 1.84, 95% CI = [1.38, 2.46] for the Surinamese older adults). Being from a Moroccan ethnic group was not significantly associated with a raised OR compared with the Dutch. Adjusting for age and gender increased the ORs for all three ethnic minority groups, but the association between falls and ethnicity was only significant in Turkish and Surinamese older people (OR = 2.90, 95% CI = [1.77, 4.75]; and OR = 2.08, 95% CI = [1.55, 2.80], respectively). When adding the SES indicators, the OR decreased but the ethnic differences, mentioned earlier, persisted. After entering the lifestyle and health-related variables to the model, ethnicity was no longer significantly associated with an increased OR for falls. Variables significantly associated with falls in the final model (Model 3) included poor perceived health, depressive symptoms, loneliness, having two or more chronic conditions, and functional limitations (hearing, sight, and mobility limitations).
Multivariate Association of Different Background and Health Characteristics With Recurrent Falls (OR and 95% CI).

Note. OR = odds ratio; CI = confidence interval.
Table 4 displays the regression models for fear of falling, with ethnicity being the independent variable, before and after adding socio-demographic characteristics followed by health and lifestyle indicators. Compared with the Dutch, being from an ethnic minority group was associated with increased OR for experiencing fear of falling (OR = 2.66, 95% CI = [1.66, 4.26] for the Moroccan; OR = 3.67, 95% CI = [2.33, 5.78] for the Turkish; and OR = 3.54, 95% CI = [2.72, 4.60] for the Surinamese older individuals).
Multivariate Association of Different Background and Health Characteristics With Fear of Falling (OR and 95% CI).
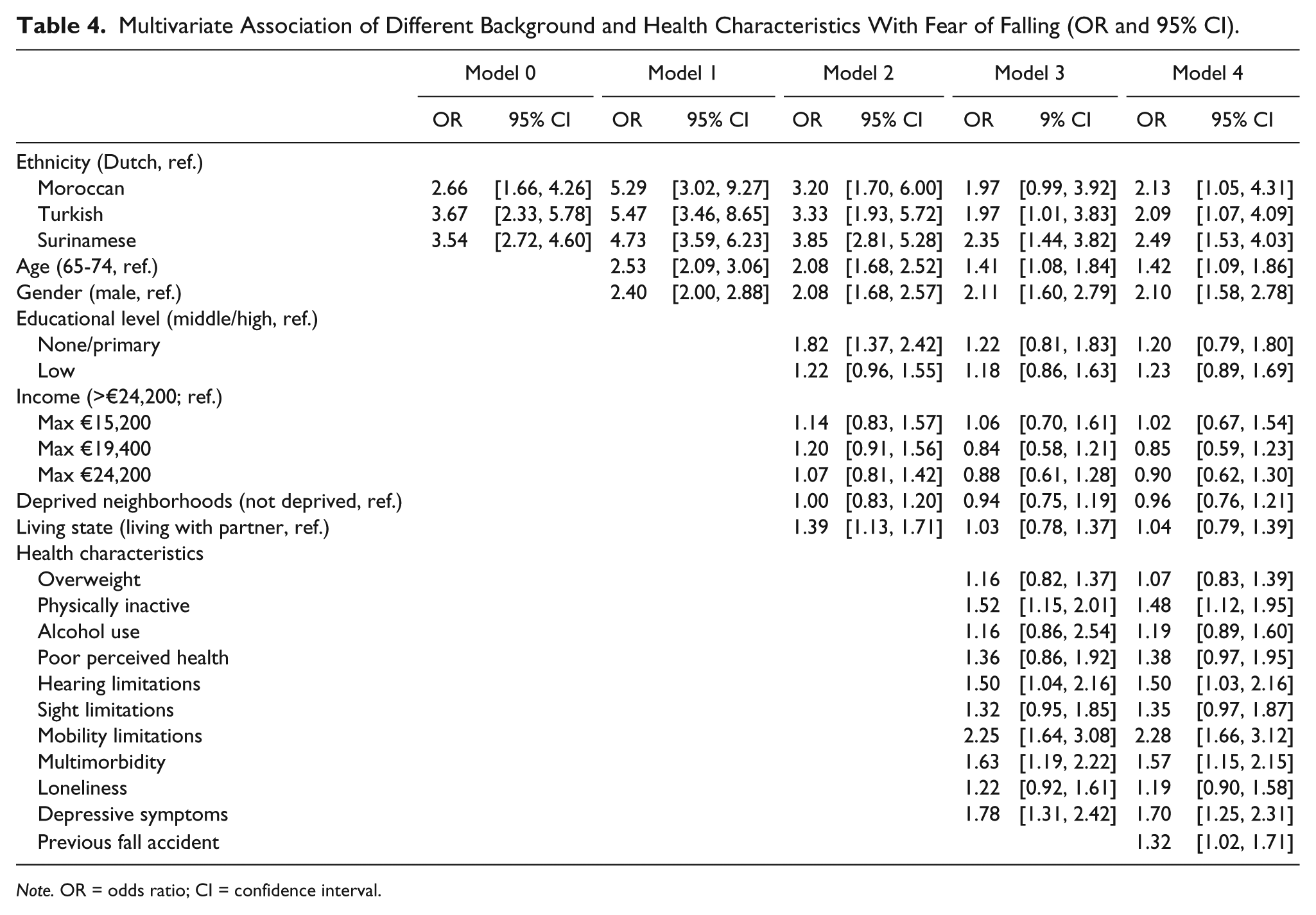
Note. OR = odds ratio; CI = confidence interval.
After including age and gender in the analysis (Model 1), belonging to an ethnic minority remained significantly associated with a higher OR of fear of falling: The ORs were 5.29 (95% CI = [3.02, 9.27]) for the Moroccan, 5.47 (95% CI = [3.46, 8.65]) for the Turkish, and 4.73 (95% CI = 3.59, 6.23) for the Surinamese older adults. Including the other demographic factors and determinants concerning lifestyle, physical, and psychological health reduced the ORs for ethnicity (Model 3). Compared with the Dutch older adults, being from a Turkish and Surinamese ethnic group was significantly associated with a high OR for experiencing fear of falling. After adding the variable “having a previous fall” to the multivariate analysis (Model 4), the results of the association between ethnicity and fear of falling persisted. A Moroccan, Turkish, or Surinamese ethnicity was significantly associated with higher ORs of fear of falling. Differences in fear of falling between the Dutch and other older adults from ethnic minorities were partly explained by age, gender, physical inactivity, multimorbidity, mobility and hearing limitations, depressive symptoms, and previous fall accidents.
Discussion
This study examines whether ethnicity is associated with the prevalence of falls and fear of falling among older adults aged 65 years and above in the Netherlands. The present study is, to our knowledge, the first study to analyze falling and fear of falling among different ethnic groups of older adults in the Netherlands. In addition, the study sample includes a sufficient number of ethnic minority individuals living in the Netherlands, which strengthens the ability to generalize the findings regarding the ethnic differences. This study also examined whether ethnic differences could be explained by a wide range of different modifiable and non-modifiable determinants of falls and fear of falling.
Our findings indicate that ethnicity is associated with fear of falling. Ethnic minority older people, especially those of Surinamese background, had higher OR of experiencing fear of falling than their Dutch counterparts. We also find a relationship between ethnicity and recurrent falls as Turkish and Surinamese ethnic backgrounds were associated with a higher OR compared with Dutch ones. Being of a Moroccan background was not significantly associated with a higher OR for recurrent falls. However, this association between ethnicity and falls did not persist after correcting for other determinants and risk factors of falling reported in this study.
The findings of previous studies examining ethnic differences in fall rates are inconsistent. In the studies by Faulkner et al. (2005), J. T. Hanlon et al. (2002), and Landy et al. (2011), higher risks of fall accidents were reported in Whites or Caucasian older people compared with African Americans and other ethnic groups such as Italians. However, Stanaway et al. (2011) demonstrated a lower rate of falls among Whites or Caucasian older people, and Landy et al. (2012) showed no ethnic differences at all, with regard to falls. The study of Karlsson et al. (2014) compares the fall rates of men in three different countries: the United States, Sweden, and Hong Kong. The proportion of fallers was highest in the United States, intermediate in Sweden, and lowest in Hong Kong. Although our study demonstrated differences in fall rates between the Turkish, Surinamese, and Dutch ethnic groups, the association between ethnicity and falls did not persist after controlling for relevant determinants of falling that were reported in previous studies. This study differs from previous studies as it comprised other ethnic minority groups. Furthermore, the present study included additional information on different physical, psychological, and lifestyle-related variables, which could explain the ethnic differences. Such information, however, was lacking in some previous studies. Another explanation is that because our study included relatively few ethnic minority older people, it lacks sufficient power to detect significant differences between the ethnic minority groups and the Dutch majority population. This is particularly the case with the Moroccan ethnic group.
With regard to fear of falling, the limited number of similar studies involving ethnic groups living in the same country makes comparison difficult. The average proportion of older people who experienced fear of falling in our study (21%) was found to be lower than in other studies, but higher among ethnic minority groups compared with their Dutch counterparts. In addition, the association in this study between ethnicity and fear of falling persisted, even after controlling for other correlates of fear of falling that were reported in other studies. The finding that some ethnic minority groups experience a higher fear of falling is consistent with the studies of Chang et al. (2010), Kim and So (2013), and Kumar et al. (2014). In addition, most risk factors identified in previous studies, including socio-demographic and economic characteristics and health-related indicators, were controlled for potential confounding of the relationship between falls/fear of falling and ethnicity. Furthermore, similar to previous research, this study showed that fear of falling was more likely in females, the oldest age group (75+), subjects with depression and loneliness, physically inactive individuals, older adults with mobility limitations, and multimorbidity.
Environmental factors such as traffic, lighting, and public transportation could contribute to different fear of falling profiles (Balfour & Kaplan, 2002; Chippendale & Boltz, 2015; Yoo, Kim, Yim, & Jeon, 2015). The same can be applied for the home environment which may be different in the various ethnic groups due probably to cultural differences in home decorating. Whether these factors could further explain the association between ethnicity and fear of falling could not be determined in this study. The information provided by this study concerning the neighborhoods deprivation may be too general (deprived or not deprived) to differentiate between the groups. Further research is required on this aspect.
This study has some limitations. First, because of its cross-sectional design, the study cannot determine possible cause–effect relationships. However, this study’s findings point into the same direction as previous longitudinal follow-up studies (Andresen et al., 2006; Mackenzie, Byles, & D’Este, 2009). Second, as this study is restricted to the three ethnic minority groups living in the Netherlands, the findings cannot be generalized to other ethnic (minority) groups. Nevertheless, these three ethnic minorities form the largest ethnic minority groups in the Netherlands. Third, our study did not include a definition for what is meant by a fall, nor did it distinguish between home hazards and hazards outside the home. Although we recognize the necessity of providing respondents with an appropriate definition because of the possible different interpretations between older adults, researchers, and health professionals (Zecevic, Salmoni, Speechley, & Vandervoort, 2006), we have no evidence that older adults from ethnic minorities interpreted the questions very differently than their Dutch counterparts. Fourth, self-reporting of falls and fear of falling are other limitations, as these measures may be affected by social desirability or recall bias, and could possibly have led to an underestimation of falls or fear of falling. According to King and Bruner (2000), socially desirable responding is more likely to occur in socially sensitive questions (which is not the case in falls) and is more likely to be mitigated in older subject groups. With regard to recall bias, some studies indicate that retrospective self-reporting of falls is likely to be less accurate than, for example, a calendar method, predominantly due to under-reporting (Mackenzie, Byles, & D’Este, 2006). As our findings are only based on self-reported measures, we acknowledge that we cannot oversee the consequences of this limitation on the study findings. Nevertheless, we believe that, if any underestimation occurred, this is unlikely to have differed between the various ethnic groups. Future prospective studies examining potential ethnic differences in falls and fear of falling using different data collection methods and cross-culturally validated instruments are warranted.
Finally, reporting of falls or fear of falling in non-Western immigrant older adults may be affected by differences in culturally based interpretations of (fear of) falling or subtle language differences, especially because we provided no supplemental information with regard to what is meant by “a fall.” According to Zecevic et al. (2006), older adults will likely interpret the word fall in many different ways, if not provided with an appropriate definition. We acknowledge that we cannot oversee the consequences of the absence of an appropriate definition for the term falls. Nevertheless, we assume that older adults, regardless of their ethnic backgrounds probably interpreted the questions in a more or less similar way. The possibility of over-reporting of (fear of) falling among ethnic minority older people is limited, as the findings of this study are supported by and in line with national data indicating worse health outcomes in immigrant populations in general, and also national data of hospitalizations for fall-related injuries. Furthermore, data collection procedures were tailored to these ethnic minority groups, including translation of the questionnaires into the Turkish language for the Turkish people, and, at least in two of the three locations, conducting the interviews in the first language of respondents, limiting differences in interpretations of the questions.
Conclusions and Implications
Older ethnic minorities living in the Netherlands, especially the Surinamese, are more likely to experience fear of falling than the indigenous Dutch population. We found no evidence for ethnic differences in the prevalence of (recurrent) falls between older ethnic minority adults and their Dutch counterparts. Additional research including larger numbers of ethnic minority groups is needed to better examine potential differences in falls and fear of falling or to establish these relationships in older people from different minority groups.
Nevertheless, we recommend that, in addition to focusing on modifiable risk factors for (fear of) falling, ethnicity of the older population should also be taken into account when targeting intervention programs. This is particularly the case in Turkish and Moroccan older people, who make a large share of the ethnic minority older adults in the Netherlands. These groups are still considered as “hard to reach,” because of their limited proficiency in the Dutch language, low SES, and limited health literacy.
To be successful, it is essential that such interventions focus on increasing physical activity; reducing functional limitations, for example, improving vision and hearing; and decreasing depressive symptoms and feelings of loneliness. Early interventions are important as immigrants at a younger age have to deal with health problems and functional limitations and become less physically active and more socially isolated than their Dutch counterparts. Moreover, such interventions should take into account the specific characteristics and strategies to reach older people at a high risk in general and older immigrants in particular, and have the potential to be attractive to the older people.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.