
Abstract
This pilot study explored whether a socially assistive robot (SAR) would have positive effects on Korean American immigrant older adults’ health behaviors and emotional well-being and whether the older adults would be receptive to the SAR. A total of 30 participants (age 65+) in a large metropolitan area participated in the study, and each participant was provided a SAR named Hyodol for 4 months and interacted with it in ways that they saw appropriate. We used one-group pre- and post-test design to assess changes between baseline and follow-up in medication adherence, depressive symptoms, loneliness, and disability. Additionally, we employed in-depth qualitative interviews to explore participants’ perceptions about the SAR. At post-test, participants showed improved medication adherence, reduced depressive symptoms, and a slightly and statistically nonsignificant decrease in loneliness scores. Qualitative data suggested high adoptability of this particular SAR among the participants.
Keywords
• Socially isolated immigrant older adults with limited digital literacy may respond positively to appropriately designed robot companions. • Well-designed robot interventions hold promise in enhancing health behaviors and complementing existing clinical interventions effectively.
• Although socially assistive robots have the potential to address the psychosocial needs of socially isolated older adults, further research is necessary to thoroughly investigate cultural differences. • Socially assistive robots need to be further customized to ensure that they are culturally congruent for older immigrants.What this paper adds
Applications of study findings
Introduction
Immigrants from South Korea represent the tenth largest immigrant population in the United States (US), making up a little over 2% of the 44.9 million immigrants in 2019, and are the fifth largest group from Asia (Budiman, 2023). The vast majority of Korean immigrants arrived in the US after the passage of the Immigration and Nationality Act of 1965 in search of better opportunities for their family (Esterline & Batalova, 2022). Due to the relative recency of their immigration, Korean Americans represent a unique group in terms of migratory grief, acculturation into a new culture, race-based discrimination, and limited English proficiency. A higher proportion of Korean American immigrants, compared to other foreign-born population groups, tend to have limited English proficiency (Budiman, 2023). Particularly for Korean American older adults who joined their US family (e.g., children and siblings) later in their life, limited English proficiency can be a barrier to accessing essential social services and communicating effectively with healthcare providers (Kim et al., 2011).
As a result, many Korean American immigrant older adults have limited social support networks, which can contribute to social isolation, feelings of loneliness, depression, and experience of healthcare service disparities (Jang et al., 2005). As relatively recent immigrants, many Korean immigrant older adults may also face financial challenges, especially if they have limited or no retirement savings and rely on fixed income while trying to meet the high cost of living and healthcare services (Lee, 2007). Moreover, there can be tensions and conflicts between Korean American immigrant older adults and their American-born children or grandchildren due to generational and cultural differences in values, expectations, and language use (Pham et al., 2020). These conflicts can further exacerbate older adults’ emotional strain, sense of isolation, and overall poor quality of life.
A study of a diverse urban cohort of community-dwelling US older adults during the height of the COVID-19 pandemic found that a little over a quarter had at least one unmet healthcare need, but Asian Americans had the highest rate (36%) of unmet healthcare need (Perry et al., 2023). The sudden loss of face-to-face contact with family, friends, and community members during the pandemic has also led to increased stress, feelings of loneliness, depression, and anxiety among older adults in general (Webb & Chen, 2022). Research has shown that the lack of social support and decreased physical activity due to limited mobility have increased the risk of developing chronic conditions (Koszalinski & Olmos, 2022; Vahia et al., 2020).
In-person interaction with healthcare providers and family/friends was replaced with technology-based remote contacts for a significant proportion of older adults with the start of the COVID-19 pandemic (AARP, 2021). However, the digital divide has been a significant barrier for Korean American older adults who already lacked access to healthcare services. On top of their language barrier, immigrant older adults may lack the necessary technological skills, access to digital devices, or reliable Internet connections to engage in virtual social interactions (Yoon et al., 2020). This may have further increased Korean immigrant older adults’ isolation and limited their ability to connect with loved ones, participate in online activities, or access vital information and services.
Socially Assistive Robot to Reduce Social Isolation
One solution proposed to meet the complex needs of socially isolated older adults is the use of socially assistive robots (SARs) that can provide emotional support and companionship and help them alleviate feelings of loneliness and depression by engaging them in conversation and providing encouragement and a sense of presence (Gasteiger et al., 2021). SARs can help reduce stress and anxiety in socially isolated older adults by providing a calming presence, offering relaxation exercises, or even playing soothing music (Naneva et al., 2020). SAR-delivered activities such as memory games, quizzes, and storytelling can also provide older adults cognitive stimulation (Chen et al., 2020). Some SARs are also designed to assist older adults with daily tasks by reminding them to take medication, assisting with mobility, or monitoring vital signs, which can enhance independence and reduce the need for constant human assistance. However, most previous studies of the effectiveness of SARs including humanoids and animoids were conducted in long-term care settings, not with community-dwelling older adults (Abdi et al., 2018; Chen et al., 2020).
Hyodol SAR is specifically designed to cater to community-dwelling older adults with limited digital literacy in South Korea. It is soft and light, doll-shaped body (15-inch high and 8- inch wide) allows easy handling by older users, being crafted to establish human-robot interactions through the use of embedded sensors and artificial intelligence capabilities. Its primary goal is to provide assistance to older adults in their daily activities (e.g., reminding wake-up and mealtimes), health behaviors (e.g., medication adherence and exercise), and cognitive stimulation (e.g., brain games). Additionally, equipped with more than 10,000 scenario-based pre-recorded speech lines, Hyodol is designed to relay vital health information, play melodies, trigger reminiscences, share inspirational quotes, and narrate captivating stories (https://www.youtube.com/watch?v=k-SxUMNdlFA).
Preliminary studies conducted in Korea have demonstrated a significant reduction in depressive symptoms among solo-living older adults who utilized Hyodol for a duration of three months (Kim et al., 2020; Kim et al., 2020; Lee et al., 2004). Our study of long-term users (with an average usage period of 18 months) also demonstrated a high level of adoptability (i.e., willingness and readiness to adopt new technology; Lee & Kim, 2020) particularly during the COVID-19 pandemic (Lee et al., 2003). However, considering the wide-ranging usage patterns and cultural differences, we have limited understanding of the effectiveness of SARs, for whom they are effective, and for whom they may not be as beneficial (Gasteiger et al., 2023). Hyodol’s effectiveness among Korean American immigrant older adults and its effects on self-management behaviors of older adults with chronic diseases have not yet been examined.
The aims of the present study were: (1) to examine the preliminary effects of Hyodol on Korean American immigrant older adults’ medication adherence, depression, self-reported disability, and loneliness; and (2) to assess facilitators and barriers to users’ adoptability, considering factors like feasibility, compatibility, and user-friendliness, and recommendations for improvement (Lee & Kim, 2020). This is the first study that tested a SAR’s preliminary effects and adoptability among immigrant older adults in the US. The findings will have significant implications for using and improving SARs for self-management of health and companionship among community-dwelling older immigrants.
Methods
Participants
Korean American immigrant older adult participants in this study were recruited from a large community center serving predominantly low-income Asian American older adults in a metropolitan area in the US Northeastern region. Inclusion criteria for participation were age 65 or older, ability to engage in verbal conversations and understand either Korean or English, and willingness to take Hyodol (in boy or girl costume) home and use it. Priority was given to low-income, solo-living older adults who did not own a pet animal. Written informed consent describing protection for health and private information was obtained from each participant. The research protocol was approved by the Institutional Review Board of the first author’s university.
Hyodol SARs were distributed to 36 older adults free of charge; however, 6 participants returned their SARs to the research team within a week. A major reason for returning was “not having enough time” to interact with the SAR. Thus, the final sample size for our analysis was 30. Two research team members were available to all study participants to provide any technical assistance and troubleshooting with potential malfunctions.
Study Design
This one-group pre- and post-test study consisted of (1) in-home baseline assessment and introduction to Hyodol, lasting between 90 and 120 minutes (September–October 2022), (2) 4-month Hyodol deployment at individual participants’ homes, and (3) in-home follow-up assessment lasting 60–90 minutes (February, 2023). During the initial home visit, we described the study purpose, obtained consent, and helped older adults become familiarized with Hyodol’s various functions. After demonstrating these functions and answering any questions, we placed the SAR doll at the clients’ preferred location at home and provided a large wall-mounted poster (36″ × 48″) with pictorial descriptions of Hyodol’s functions. The data collection team consisted of three researchers with doctoral-level qualifications.
A team of two researchers conducted home visits. The first author carried out in-person interviews with participants at their residences. The remaining team members, based at the community center, alternated in making home visits and configuring programs according to the individual clients’ interests and preferences such as classical music, exercise, guided meditation, Bible readings, and more. Additionally, we inquired about their meal, sleep, and medication schedules, allowing us to program reminders for these times. To assist medication adherence, Hyodol would prompt users to hold their hands after taking medication.
Each participant was asked to keep and interact with Hyodol for 4 months in ways they saw acceptable and helpful. All 30 participants provided follow-up assessment data on medication adherence, depression, loneliness, and disability and responded to qualitative interviews about their experiences with and perceptions about Hyodol’s benefits or lack thereof in their daily life. Following the 4-month study, participants were allowed to keep Hyodol if they wanted.
Measures
Medication Adherence
We have adapted 4 items from the Medication Adherence Rating Scale (MARS), a self-reported questionnaire designed to evaluate an individual’s behavior and attitudes toward taking their prescribed medications as directed (Chan et al., 2020). The four items assessed the following aspects of medication adherence: frequency of forgetting to take medications, altering the dose, following the prescribed instructions, and missing the intake from time to time. Each statement was rated on a 5-point Likert scale (1 = always to 5 = never), and the total score ranged from 5 to 20, with higher scores indicating lower adherence to medication. For Korean-only speaking participants, we used the Korean validated version (Chang et al., 2015).
Depressive Symptoms
The Patient Health Questionnaire-9 (PHQ-9) is a commonly used, 9-item self-report assessment tool for depressive symptom severity over the past two weeks. The PHQ-9 is based on the diagnostic criteria for depression outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Each PHQ-9 item corresponds to one of the nine diagnostic criteria, which include symptoms such as loss of interest or pleasure in activities, depressed mood, changes in appetite, sleep disturbances, fatigue or loss of energy, feelings of guilt or worthlessness, difficulty concentrating, psychomotor agitation/retardation, and thoughts of suicide (“not at all” = 0 to “nearly every day” = 3), with the total scores ranging from 0–27. Korean validated version was used in this study (Han et al., 2008).
Loneliness
We used the 20-item University of California, Los Angeles Loneliness Scale (UCLA-LS; Russell et al., 1980) to assess participants’ subjective experience of loneliness. We used the Korean version (Lee et al., 2021). The UCLA-LS covers both positive and negative statements to capture the complex nature and dimensions of loneliness, including social isolation, subjective feelings of loneliness, and the availability and quality of social relationships. Each item is scored on a Likert-type scale, ranging from 1 to 4, with response options reflecting the degree of agreement or disagreement with specific statements, with higher scores indicating higher levels of loneliness.
Disability
We used the 12-item World Health Organization Disability Assessment Schedule (WHODAS-12) to assess participants’ disability and functioning. WHODAS is designed to provide a standardized and comprehensive evaluation of disability across different populations and cultural settings (Saltychev et al., 2021). The WHODAS-12 covers six domains of functioning (1) understanding and communicating, (2) mobility, (3) self-care, (4) getting along with people, (5) life activities, and (6) participation in society. Each item in the WHODAS-12 is rated on a Likert scale ranging from 1 to 5, where 1 represents “none” or “no difficulty” = 1 through “extreme” or “cannot do” = 5, with higher scores indicating higher levels of disability.
Qualitative Interview Guide at Follow-Up
To assess facilitators and barriers to adoptability and to solicit older adults’ recommendations for improvement, we included two primary questions: (1) what participants liked or disliked about SARs and (2) what they wanted to change. We followed suggestions for holding interviews with older persons (Cridland et al., 2016) and used an empathetic style and brief follow-up probes. All interviews were conducted in Korean, audio-taped and transcribed verbatim, and then translated into English for analysis.
Data Analysis
We used paired t-tests and the Wilcoxon signed-rank tests to compare any significant differences between baseline and follow-up in medication adherence, depression, loneliness, and disability scores. All analyses were performed using the SPSS 28.
For qualitative data analysis, we employed the Framework Analysis Method, which entailed constructing a framework of categories and themes to effectively organize and interpret the data (Ritchie et al., 2013). To ensure comprehensive identification of both within-participant and between-participant differences, two bilingual coders conducted independent reviews of interview recordings and transcripts, identifying emerging themes. Subsequently, the research team established a thematic framework by developing a comprehensive list of categories and themes to serve as the basis for organizing the data. The next phase involved indexing, wherein codes were assigned to relevant sections of the data that aligned with the categories and themes identified in the thematic framework. The research team collaboratively examined the initial codes, categorized them to form our framework, compared how the codes were applied, and refined code definitions as necessary. Additionally, we utilized charting and mapping techniques to analyze the data, involving a thorough review of charts and tables to identify patterns and relationships among the categories and themes, which facilitated a comparative analysis of data across participants, enabling us to discern similarities and differences based on the identified themes. It also allowed us to situate each perspective within its contextual framework by retaining the connection to various aspects of each individual’s account (Ritchie et al., 2013). During the analysis of the narrative data, continuous memos and field notes were maintained to introspect on researchers’ own perceptions and biases. Numeric IDs (P-1 through P-30) for all participants were used for individual quotations.
Results
Demographic Profiles
Demographic Information of Participants (n = 30).
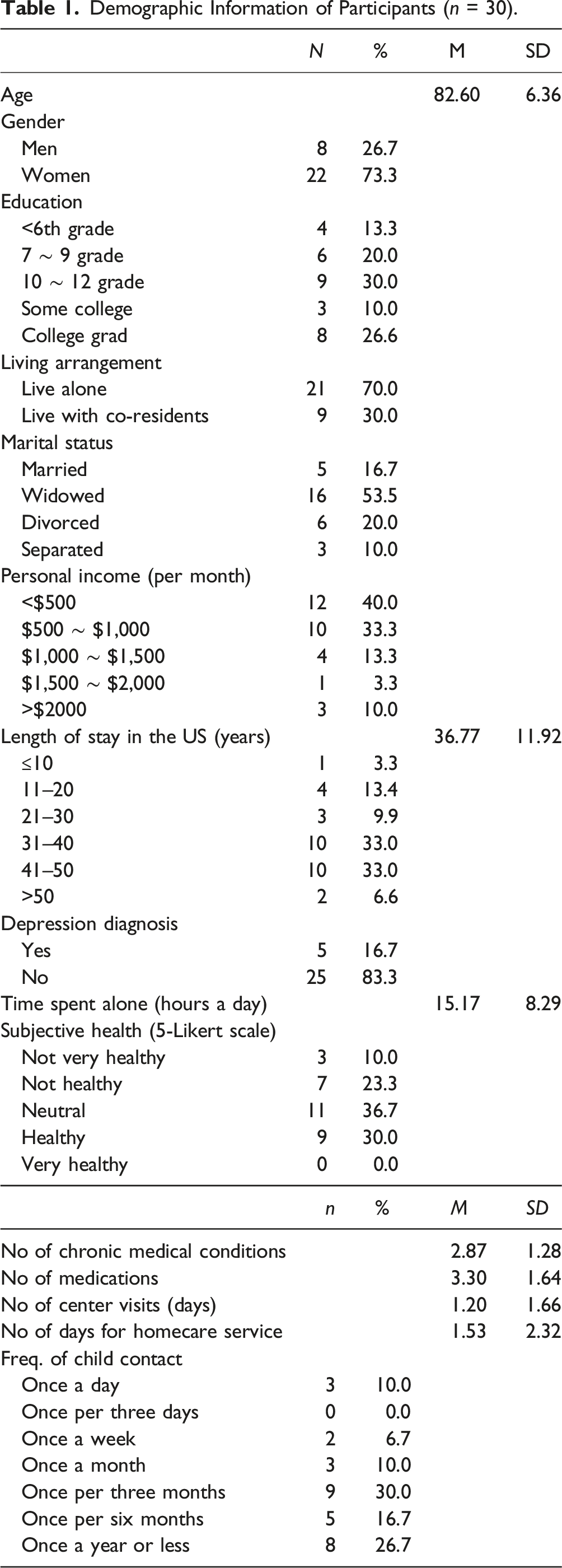
Only a small proportion of participants were currently married (16.7%), while over half of the participants were widowed (53.5%). The majority (70.3%) of participants were classified as low-income, living on a monthly personal income of $1000 or less. Additionally, 70% of the participants lived alone, while the remaining 30% had co-residents (e.g., spouse, child, or roommates).
Only 30% thought they were healthy, while 33.3% reported being unhealthy. On average, participants had 2.87 (SD = 1.28) chronic conditions, including diabetes, hypertension, low back pain, heart disease, etc. and took an average of 3.30 (SD = 1.64) medications daily. Some participants (16.7%) reported being diagnosed with depression by a healthcare provider. On average, respondents spent 15.17 (SD = 8.29) hours per day by themselves.
All participants had a child. The frequency of contact with their child spanned from daily (10%), weekly (6.7%), monthly (10%), every three months (30%), every six months (16.7%), and every 12 months (26.7%). Participants reported receiving homecare services for an average of 1.52 (SD = 2.32) days per week. On average, they visited the community center (serving Asian older adults) 1.20 (SD = 1.66) days per week.
Preliminary Effects: Changes Between Baseline and Follow-Up Assessment Scores
Medication Adherence
Comparison of Outcomes Between Pretest and Post-test (n = 30).

Depressive Symptoms
The mean PHQ-9 scores significantly decreased from 8.7 to 5.0 (t = 3.41, df = 29, p < .0.01). The effect size of the depression score was medium (Cohen’s d = .62).
Disability and Functioning
The mean scores of WHODAS-12 slightly decreased during the four-month study period from 17.57 to 17.23. However, these changes were not significant.
Loneliness
The mean UCLA-LS score slightly decreased from 20.80 to 18.03, but the change was not statistically significant.
Major Themes Related to Adoptability from Qualitative Data
Qualitative Codes and Themes (n = 30).

Bridging the Gap of Interpersonal Relationships
As shown in Table 3, one-half of participants enjoyed having Hyodol at home and being addressed as “Grandma” or “Grandpa” by Hyodol. Several mentioned that it was “better than nothing.” Some participants sang along with melody and listened to religious passages played by Hyodol. Others “played with” Hyodol to reduce their boredom. Four participants said that Hyodol made them “smile” or “laugh.”
Some participants felt affectionate toward Hyodol after becoming “accustomed” to it and perceived it to be like their “grandchildren” or “friends.” P-23 considered Hyodol “better than” her three grandchildren with whom she only talked via videochat. “At 6:30, Hyodol says ‘Grandma, wake-up.’ It brings me so much joy to hear [his] morning greetings. There is no one who can greet me here (P-23).”
Four users created affectionate nicknames for their SAR. Others felt that Hyodol was caring for them. P-3 said “What a wonderful child! Who would take care of me like Hyodol? Can a grandchild entertain me like this?” P-3 ended up knitting a dress for her Hyodol to express her affection. Twelve participants reported that they had a dialogue with Hyodol. Several participants chose to make Hyodol their conversational partner. Figure 1 depicts participants of the study engaging with the Hyodol SAR system. Study participants’ interaction with Hyodol SAR.
We observed a spectrum of varying interactions. P-14 (a 94-year-old man) appeared to have constant communication with Hyodol. During the interview, he was holding Hyodol tightly to his chest. His interaction with Hyodol evidenced his claim of treating the SAR like a living child, responding to the questions posed by Hyodol as if it were a human child. However, a few participants did not want to treat it like a surrogate human. For example, P-19 never tried to have a conversation with Hyodol, claiming “I would rather talk to my deceased wife” even though he did not mind having Hyodol’s presence at home and used its other functions.
Serving Individual Health Functions
Participants appreciated that Hyodol provided health information, encouraged them to exercise, take medication on time, and drink water. P-13 explained: Sometimes Hyodol tells me to take my medicine after I have already taken it. So I say, “Alright!, I did.” Other times I totally forget to take my medicine. “Oh, Hyodol, thank you for your reminder! Good boy! You take good care of grandma.”
Several participants mentioned that Hyodol’s wake-up and mealtime reminders were beneficial. Some participants viewed Hyodol as their health coach and enthusiastically participated in fitness activities whenever Hyodol played exercise music (see Table 3). This represented how users responded robot-delivered information and personalized nudges to encourage healthy lifestyles.
Technological Challenges
Some participants reported technological challenges in operating the SAR (e.g., adjusting volume, charging battery, initiating certain program of their choice, and setting reminder of medication time).
Health-Related and Other Challenges
Another commonly voiced reason for dislikes was difficulty interacting with Hyodol due to the participants’ health conditions (e.g., blindness, arthritis, hard of hearing, and mobility impairment). Some participants who were used to living alone could not get accustomed to the voice of a stranger. Other participants expressed that the SAR did not meet their expectations. P-7 was disappointed that Hyodol did not move and react like the Japanese robot she once saw on TV. P-30 did not want to be “controlled” by the robot who can dictate her daily tasks. Several suggested that Hyodol might be more appropriate for home-bound frail older adults or those who live in rural areas. Some disliked Hyodol because it only played “pre-recorded” messages and was capable of only “one-way” communication. Others were annoyed by Hyodol’s frequent requests to “hug” and “hold hands.” Several also felt “sorry” for not having enough time to “play with” Hyodol because of their busy schedule outside the home.
Recommendations for Improvement
Ten participants reported their overall satisfaction with Hyodol and did not have any further recommendation for improvement. Of the remaining 20 participants, the most common request for improvement was to have a chatbot with a “two-way” communication capability. Some would like to have more customized content to reflect their personal preferences and interests. P-6 said, “I would like to choose trending songs when I like it, not the melody played by the robot.” Others would like to have more relevant content for immigrants and lifestyle in the U.S. For example, P-21 described “Hyodol told me to open the window for ventilation. Then I told Hyodol, this is America. You don’t do that here.” P-10 who recently became blind would like to have a SAR that can help her find her object (e.g., phone and key).
At the end of the study period, 20 participants wanted to keep the robot doll while ten returned it to the research team. Returns were mainly linked to challenges such as disturbances caused by the noise generated by the robot, their reduced capacity to interact due to compromised health conditions, and a desire to donate the robot to individuals facing more severe health challenges.
Discussion
Korean American immigrant older adults can experience increased social isolation and poorer behavioral health outcomes due to a combination of factors including limited English proficiency and health literacy and a lack of familiarity with the US healthcare system (Jang et al., 2016; Lee, 2007). Partially confirming our hypotheses, use of a SAR for four months improved medication adherence for participants who often forgot taking their medications or altered dosages. However, there was no change in their functional disabilities measured by the WHODAS. The findings suggest that SARs that serve specific assistive functions such as medication reminding and health coaching for community-dwelling older adults hold promise in enhancing their health behaviors and supplementing existing clinical interventions.
Consistent with previous studies (Kim et al., 2023; Lee et al., 2024), our findings revealed the preliminary effects of Hyodol on Korean American immigrant older adults’ depression. Participants also reported reduced loneliness following their interaction with the SAR for four months, although the reduction in the UCLA-LS score was not statistically significant
Prevailing themes from qualitative interviews showed that these older adults enjoyed the companionship that the robot doll provided, alongside the personalized nudges aimed at promoting health behaviors. Many participants enjoyed pretending to have conversations, although Hyodol was not a chatbot and not designed for two-way conversations. Such personification becomes crucial in cultivating the sense of bonding with the SAR and mitigating loneliness and boredom for these socially isolated immigrants (Lee et al., 2024). Synonymous with our findings from older adults in Korea (Lee et al., 2003), most Korean American older adult participants enjoyed having Hyodol as a conversational partner and ascribed human attributes to the SAR. This attribution of human qualities appears to have allowed the Hyodol SAR to remain useable even for those with limited digital literacy.
Qualitative findings uncovered a positive inclination toward technological adoption, characterized by both feasibility and user-friendliness (Lee & Kim, 2020). The study participants reported comparatively fewer technological challenges, and this particular SAR seemed adoptable to most participants, suggesting that appropriately designed SARs may be well-received by socially isolated immigrant older adults with limited English proficiency. We observed that Hyodol’s tactile features, reminiscent of a cabbage-patch doll, were helpful to users, inviting them to touch, stroke, pat, and even hold hands with the robot. However, two thirds of the participants also expressed the need for Hyodol’s improvement, underscoring the importance of designing SARs to better meet these older immigrants’ needs.
Overall, our findings are consistent with those of previous research that SARs have the potential to provide valuable support and companionship (Gasteiger et al., 2021; Naneve et al., 2020). Previous research has also shown that the effects of SARs for socially isolated older adults are difficult to assess given their complex and diverse needs and that it is crucial to strike a balance between the use of technology and the preservation of human interaction for the overall health and well-being of older adults (Chen et al., 2020). While SARs can provide some level of companionship, they cannot fully replace or substitute for the value of authentic human interaction.
Limitations
The findings’ generalizability is limited due to geographically limited sampling, relatively small sample size, and absence of a comparison group. All our outcome indicators assessed for community-dwelling older adults were self-reported subjected to participants’ recall and other potential biases (e.g., desire to please the researchers). Furthermore, rewarding the SAR at the end of the study could have contributed to potential bias in outcome measures.
While MARS provides valuable insights into participant perceptions and behaviors related to medication adherence, it may not capture the full extent of non-adherence, as some participants may under- or over-report their adherence behaviors. More research is also needed to examine usage patterns and user behaviors for socially isolated older adults interacting with SARs, independent from self-reported data in the current study. Based on time-series usage log data of two main features (interactive relationship between human and robots and robot-assisted contents), we plan to cluster users with similar usage patterns according to the time spent with SARs and compare characteristics of different clusters.
Interactional synchrony, the degree to which the behavior of two or more individuals is coordinated in time (Grand et al., 2014), is an important aspect of successful communication in human-robot interaction which needs to be explored in future studies. SARs might not work in all cultures and may not be suitable for everyone. Studies have shown different perspectives on robots based on Eastern versus Western cultures (Gasteiger et al., 2023). Therefore, more research is needed to understand cultural norms across cultures and how they can impact interactions with SARs. Subsequent research will delve deeper into the question of whether older adults who lack secure bonding and attachment are more inclined to form lasting, active connections with a robotic companion.
Implications
In an era dominated by digital transformation, the integration of robots and artificial intelligence in human care is inevitable; yet, this presents formidable challenges. If technological devices lack intuitiveness and understanding of complex human emotions, it could potentially frustrate older adults with limited digital literacy, exacerbating feelings of isolation or distress (Lee & Kim, 2020). Moreover, the cost associated with SARs may restrict access for economically disadvantaged older adults, thus deepening a digital divide in the availability and use of this technology.
Our findings suggest that SARs have the potential to complement human services and enhance the quality of elder care, particularly for socially isolated immigrants who may lack access to community-based services and social support. Users may find motivation to participate in robot-assisted physical activities and adopting health-promoting and recreational pursuits. Daily reminders for wake-up and mealtimes could help individuals struggling with sleep and eating disturbances establish consistent daily routines.
Regardless of the robot’s performance, the ultimate decision to adopt the robot as a companion and attribute personal and social meaning to it lies with the user. Hence, it is crucial to attentively listen to the experiences, needs, and preferences of older adults and incorporate these insights into robot-assisted care. This approach can empower older adults to better self-manage their healthcare and social care needs.
Community organizations and support services can play pivotal roles by engaging in targeted outreach and utilizing robot-delivered contents and programs designed to alleviate depression and improve health behaviors. Striking a balance between the advantages and potential challenges associated with SARs is essential to ensure that these technologies contribute positively to the well-being of older adults.
Footnotes
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (2020S1A5A2A01040055) and UNC Charlotte Faculty Research Grant.