
Abstract
Research on resilience in sexual minority midlife and older adults is limited. Using a multidimensional approach, this study examined trait resilience (optimism), resilience as a dynamic process (perceived control), and relational resilience (social support), analyzing their roles in physical and mental health among sexual minority adults. Analyzing data from MIDUS 2 and MIDUS Refresher, we examined a sample of 492 participants, comprising 164 sexual minority and 328 propensity-matched heterosexual individuals. Among sexual minority participants, perceived control was associated with fewer chronic conditions and optimism with lower depressed affect. Among heterosexual participants, perceived control was associated with both outcomes. Subgroup analyses found variations, particularly among lesbian and bisexual women. Resilience measures were not associated with the health outcomes for gay or bisexual men. This study highlighted the complex roles of trait resilience and dynamic resilience processes in association with health outcomes among sexual minority midlife and older adults across diverse subgroups.
• This study uncovers gender-based disparities in resilience pathways within sexual minority subgroups. • The study underscores the importance of optimism and perceived control in association with health outcomes for sexual minority midlife and older adults, providing valuable insights into their role in well-being.
• The study’s insights into distinct resilience pathways for sexual minority subgroups can inform tailored health interventions for the unique needs of these marginalized midlife and older adults. • This study underscores the need for future research with larger, more diverse samples of sexual minority midlife and older adults, comprehensive mental health measures, and refined assessments of relational resilience.What this Paper Adds
Applications of Study Findings
Introduction
The recognition of health disparities in the sexual minority community became a significant public health concern in the United States under Healthy People 2020, a comprehensive initiative to improve the nation’s well-being (US Department of Health and Human Services, 2011). This spurred substantial research efforts to uncover factors contributing to these disparities. Recent studies investigating the health of sexual minority midlife and older adults have revealed evidence of resilience in the face of challenges like discrimination and stigma, potentially influencing their well-being (Fredriksen-Goldsen et al., 2017; Nelson & Andel, 2020a, 2020b). Yet, limited research has explored resilience among sexual minority midlife and older adults, revealing a need for a deeper understanding of resilience that may identify modifiable factors to enhance sexual minority health and identify those at greater risk of negative outcomes. Current sexual minority aging research tends to problematize and pathologize older adults within this population. Shifting toward a resilience-focused approach is crucial to recognize and leverage the strengths and assets within this diverse group (Colpitts & Gahagan, 2016).
Within research on sexual minority midlife and older adults, the utilization of resilience measures is sparse. Some studies have hinted at potential resilience based on their findings but did not incorporate specific resilience measures (Fredriksen-Goldsen et al., 2017a; Nelson & Andel, 2020a, 2020b). Others used established resilience scales (King & Orel, 2012; King & Richardson, 2016), while some relied on proxy variables like psychological distress, compassion, or hardiness (Mereish & Poteat, 2015; Winiker et al., 2019). Qualitative studies identified resilience factors, including community connectedness, self-acceptance, and coping (Drabble et al., 2018; Levitt et al., 2016). Higher resilience has been linked to improved physical and mental health in sexual minority adults (Emlet et al., 2017; King & Orel, 2012; Winiker et al., 2019).
Traditionally, resilience research has tended to concentrate on one dimension of resilience at a time, overlooking the interconnectedness of these facets (de Lira & de Morais, 2018). However, resilience is inherently multidimensional, encompassing traits (Wagnild & Young, 1993), dynamic processes (Fergus & Zimmerman, 2005), and relational aspects (Bartoș & Langdridge, 2019). Embracing a multidimensional perspective enables researchers to explore the intricate interplay between these dimensions and how they collectively shape an individual’s capacity to overcome adversity and thrive. This approach offers a nuanced understanding of resilience across diverse contexts and populations, informing effective strategies and interventions for enhancing resilience (Bartoș & Langdridge, 2019; Fredriksen-Goldsen et al., 2013). Therefore, this study will adopt a multidimensional approach to examine resilience’s impact on the physical and mental health of sexual minority and heterosexual midlife and older adults.
Trait Resilience
Trait resilience, characterized as an innate personality characteristic that promotes adaptation in the face of adversity (Wagnild & Young, 1993), is explored in this study, with a specific focus on dispositional optimism as a proxy measure. Research has shown that in older sexual minority men, pessimistic future expectations were associated with loneliness (Jacobs & Kane, 2012), which is associated with adverse physical and mental health outcomes and increased mortality risk (Park et al., 2020; Rico-Uribe et al., 2018). Optimism has also been linked to resilience and positive health outcomes in the general population, including repatriated prisoners of war (Segovia et al., 2015), as well as non-smoking, healthy diet, and healthy BMI in adults with disadvantaged childhoods (Non et al., 2020).
Resilience as a Dynamic Process
Resilience as a dynamic process involves utilizing available assets to overcome adversity, such as coping mechanisms (Fergus & Zimmerman, 2005). This study employs perceived control as a proxy for resilience as a dynamic process. Perceived control represents an individual’s belief in their ability to influence situations and achieve goals, encompassing personal mastery and perceived constraints. Research in the general population has consistently linked higher perceived control to improved physical and mental health outcomes and protection against the negative effects associated with traumatic experiences such as inflammation and mortality (Elliot et al., 2017, 2018; Toyama & Fuller, 2021).
Studies exploring perceived control in sexual minority samples are relatively scarce. For instance, personal mastery and resilience independently contribute to psychological well-being in HIV-positive gay and bisexual men (Emlet et al., 2017). Higher personal mastery is associated with lower rates of depression and higher quality of life in sexual minority older adults (Fredriksen-Goldsen et al., 2019). Additionally, locus of control moderates the impact of workplace-based prejudice on psychological distress in sexual minority individuals (Carter et al., 2014).
Relational Resilience
The third dimension of resilience under examination is relational resilience, characterized by deriving strength from family, friends, communities, and social resources, including political movements (Bartoș & Langdridge, 2019). Emerging evidence suggests that relational resilience plays a vital role in the well-being of sexual minority adults. Qualitative studies reveal that narratives of resilience in sexual minorities often revolve around social support and resources (Bartoș & Langdridge, 2019). Moreover, social support and community connectedness have been identified as resilience factors in both qualitative and quantitative studies (Drabble et al., 2018; Emlet et al., 2017; King & Richardson, 2016; Mereish & Poteat, 2015). Lower social support is associated with reduced resilience in sexual minority adults, excluding lesbians (Krueger & Upchurch, 2022).
Research Aims and Hypotheses
This study aimed to (1) examine how three dimensions of resilience—trait resilience (specifically, dispositional optimism), resilience as a dynamic process (measured through perceived control), and relational resilience (specifically, social support)—influence the physical and mental health outcomes, focusing on the number of chronic conditions and depressed affect, of sexual minority individuals in midlife and older age, (2) explore potential disparities in the results between sexual minority and heterosexual groups, aiming to discern whether any dimension of resilience holds greater significance for one group compared to the other, and (3) explore variations in the impact of the three resilience dimensions on health outcomes among different sexual minority subgroups, including gay men, lesbians, bisexual men, and bisexual women. For the first aim, it was hypothesized that all three dimensions of resilience would be significantly associated with the number of chronic conditions and depressed affect for both sexual minority and heterosexual groups. For the second aim, we expected a stronger association between relational resilience and the number of chronic conditions and depressed affect for sexual minority individuals, consistent with prior findings highlighting the protective role of social support in this population. For the third aim, no hypotheses were made given the scarcity of prior research on variations in resilience factors among different sexual minority subgroups.
Methods
Data and Sample
This study merges data from the nationally representative Midlife in the United States (MIDUS) study, which surveys midlife and older adults using random telephone digit dialing. Participants provided verbal consent and completed a 45-min telephone interview along with two self-administered questionnaires. MIDUS 2, conducted from 2004 to 2006, included 4963 of the original 7108 participants. The MIDUS Refresher, conducted from 2011 to 2014, added 3577 adults aged 25 to 74. Combining participants from both MIDUS 2 and the MIDUS Refresher yielded a total of 8540 participants.
For the current study, the sample was restricted to participants aged 40 and older, and exclusions were applied for missing data on study variables. Among the 5171 remaining participants, 96 identified as homosexual (gay/lesbian), 68 as bisexual, and 5007 as heterosexual. Combining homosexual and bisexual participants formed the sexual minority group (n = 164). Before propensity score matching, notable differences existed between sexual minority and heterosexual groups in certain demographic variables. To address this, a 1:2 propensity-matched heterosexual group was created through propensity score matching (Parsons, 2004), as outlined in the analysis section. This process balanced covariates such as age, sex, education, race, and employment status, resulting in a final analytical sample of 492 participants, with 164 from the sexual minority group and 328 from the heterosexual group. Propensity score matching aimed to minimize potential biases and enhance the comparability of the two groups for more robust analyses.
Measures
Sexual Orientation
Participants were asked whether they would describe their sexual orientation as “heterosexual (sexually attracted to only one sex), homosexual (sexually attracted only to your own sex), or bisexual (sexually attracted to both men and women).” For this study, homosexual (i.e., lesbian and gay) and bisexual participants were combined into the sexual minority group. Propensity score matching was conducted to create a propensity-matched heterosexual group.
Dimensions of Resilience
Three dimensions of resilience were assessed in this study using proxy measures: trait resilience, resilience as a dynamic process, and relational resilience. Trait resilience was assessed using a measure of optimism. Optimism and pessimism were assessed using the Life Orientation Test-Revised (LOT-R; Scheier et al., 1994). The 6-item scale assesses the tendency to expect positive outcomes (3 items for pessimism and 3 items for optimism). The items were assessed on a scale of 1 (agree a lot) to 5 (disagree a lot). The optimism items were reverse coded so higher scores represent higher optimism. Scores ranged from 6 to 30 (Cronbach’s α = 0.82).
Resilience as a dynamic process was assessed by a composite measure of personal mastery and constraints, or perceived control (Lachman & Weaver, 1998). Perceived control was assessed by combining a 4-item personal mastery scale and an 8-item perceived constraints scale. Responses for the items ranged from 1 (strongly agree) to 7 (strongly disagree). The items from personal mastery were reverse coded so higher scores would indicate higher perceived control (Cronbach’s α = 0.88).
Relational resilience was assessed using two measures of social support: support from friends and support from family, each with four items. Participants were asked about how much their friends and family understand the way they feel, really care about them, whether they can rely on them for help with problems, and whether they feel they can open up to them about their worries. Responses for each item ranged from 1 (not at all) to 4 (a lot). The items for both family and friend social support were summed and averaged to create the relational resilience variable (Cronbach’s α = 0.86).
Health Outcomes
The health outcomes for this study include depressed affect and number of chronic conditions. To assess depressed affect, a composite measure was derived from seven “yes” or “no” items. These items asked about experiences during two weeks in the past year when participants felt sad, blue, or depressed, such as losing interest in most things, appetite changes, concentration difficulties, sleep problems, thoughts about death, increased fatigue, and negative self-perception. The composite score, ranging from 0 to 7, reflected the sum of “yes” responses, with higher scores indicating more significant depression levels.
The number of chronic conditions was assessed by summing the number of reported conditions participants experienced or received treatment for in the past year. Participants were asked about 30 chronic conditions, including stroke, diabetes, hay fever, and incontinence, resulting in a range from 0 to 30. To focus solely on physical health, two mental health-related conditions, namely, “anxiety, depression, or some other emotional disorder” and “alcohol or drug problems,” were excluded. Consequently, the total chronic conditions sum ranged from zero to 28.
Covariates
The covariates for this study included age (in years), sex (male or female), education (highest achieved), marital status (married, separated/divorced, widowed, and never married), employment status (employed, retired, and other), and race (White or non-White).
Statistical Analyses
Missing data were addressed through casewise exclusion (Kang, 2013). As missing data comprised less than 5% of the dataset and appeared to occur at random, it was deemed not to pose a significant threat to data integrity (Bennett, 2001). Survey weighting was not utilized in the analyses. Propensity score matching (Parsons, 2004) was employed using SAS, version 9.4 (SAS Institute, Cary, NC), pairing two heterosexual participants with each sexual minority participant. Propensity scores were calculated through logistic regression, adjusting for age, sex, education, race, and employment status. A SAS add-on macro for greedy propensity matching was then applied. In this approach, matching began by considering the first eight digits of the propensity score, followed by seven digits, and so forth, until each sexual minority participant had two matched heterosexual counterparts. All sexual minority participants successfully matched with two heterosexuals. Matching success was confirmed through chi-square and t-tests.
Subsequently, linear regression analyses were performed to investigate the associations between the resilience measures and two health outcomes (i.e., the number of chronic conditions and depressed affect). In the first step, covariates were introduced into the model, and in the second step, optimism, perceived control, and social support were added simultaneously to assess their combined associations with health outcomes. These regression analyses were conducted separately for sexual minority and heterosexual adults.
Additionally, exploratory analyses were carried out to compare sexual minority subgroups. Chi-square and ANOVA analyses were employed to identify demographic differences among subgroups (gay, lesbian, bisexual men, and bisexual women), and regression analyses were conducted for each subgroup using the same methodology as described above.
Results
Sample Characteristics
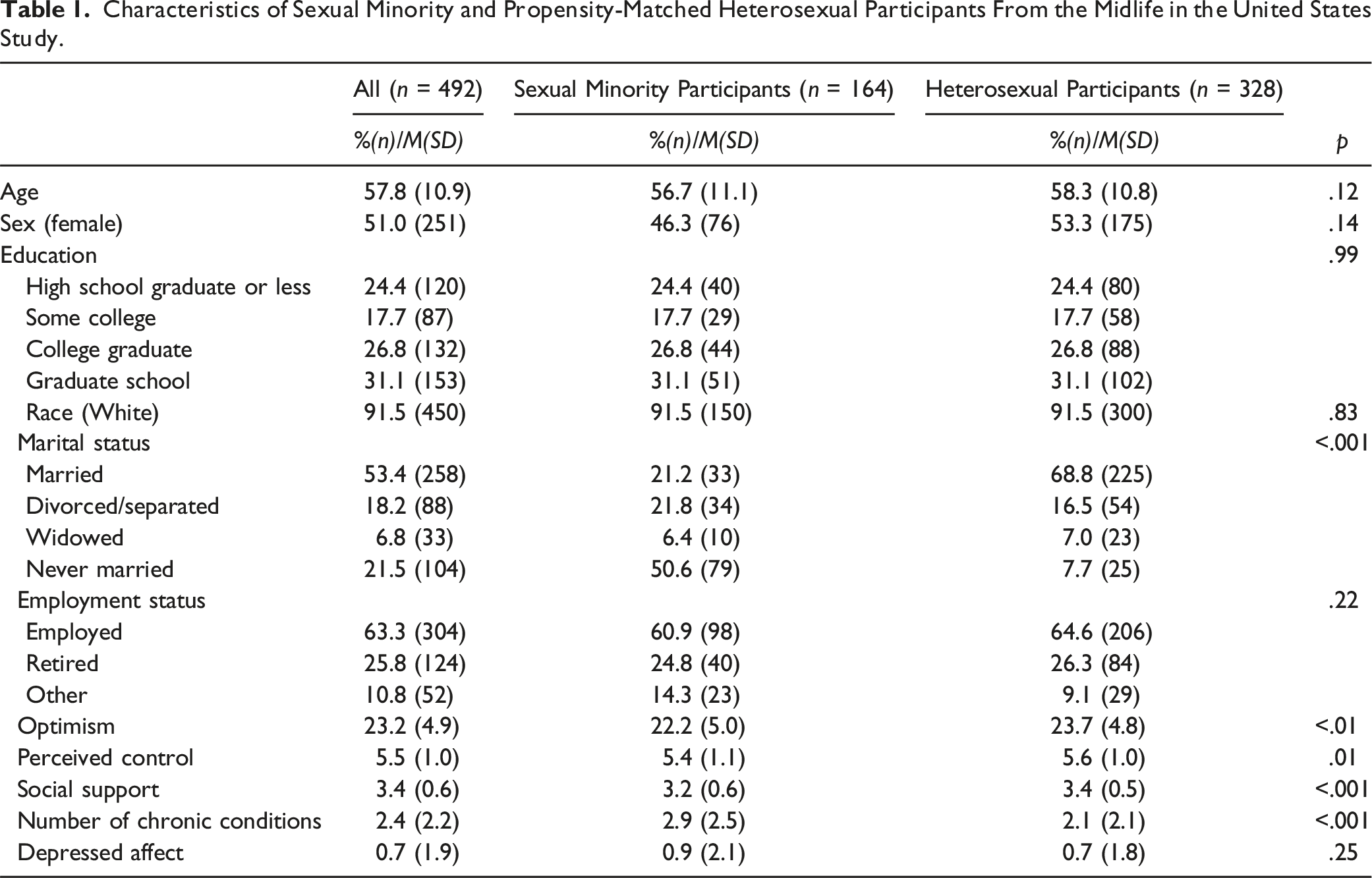
Characteristics of Sexual Minority and Propensity-Matched Heterosexual Participants From the Midlife in the United States Study.
Regression Analyses for Sexual Minority Group
Association Between Resilience Variables and Health Outcomes in Sexual Minority Participants (n = 164).
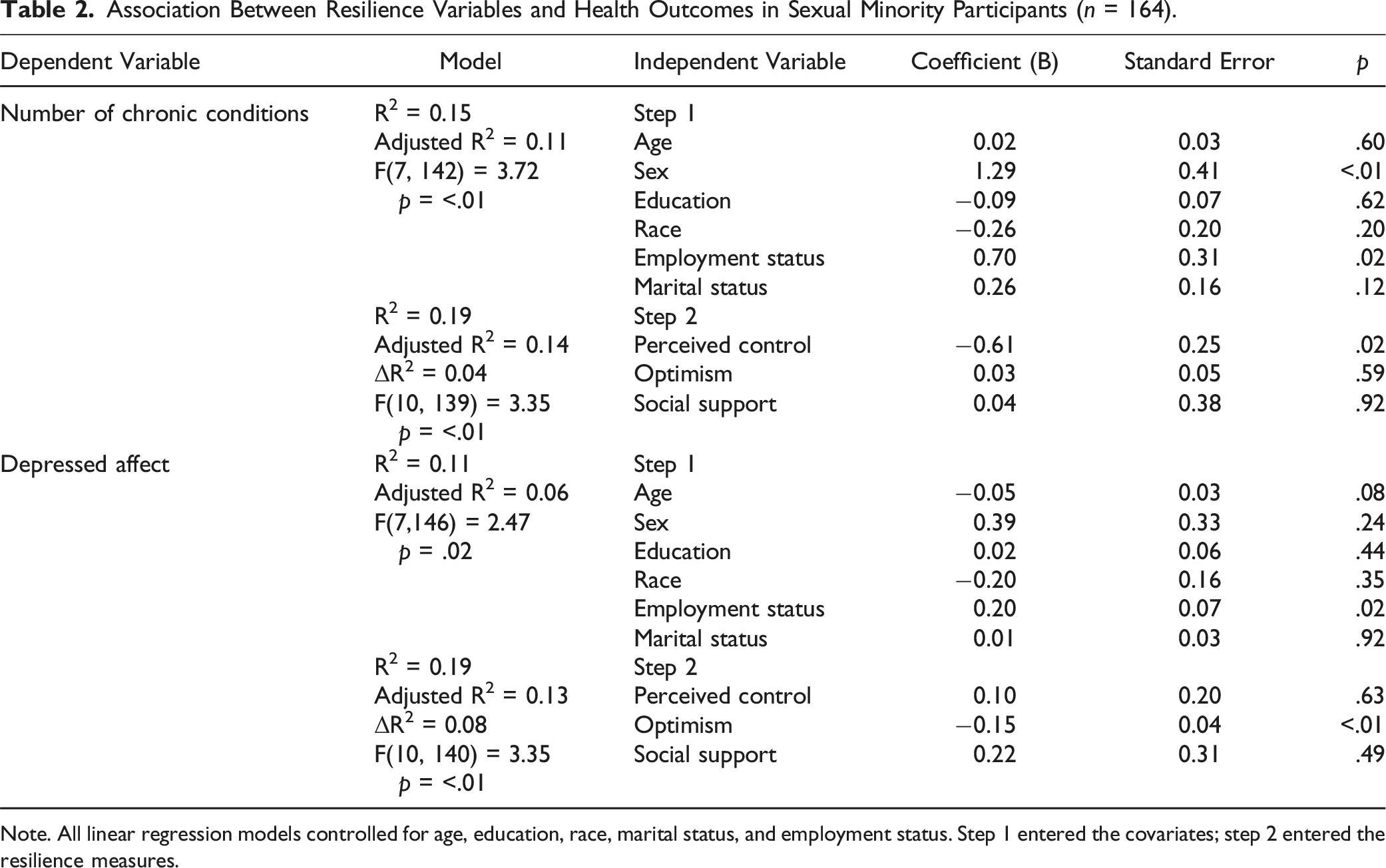
Note. All linear regression models controlled for age, education, race, marital status, and employment status. Step 1 entered the covariates; step 2 entered the resilience measures.
Similarly, for depressed affect, the regression analyses indicated that the three resilience variables jointly explained 8% of the total variance after accounting for the covariates for sexual minority participants (R2 = 0.19, ΔR2 = 0.08, F(10,140) = 3.35, p < .01). Optimism was significantly associated with depressed affect in the sexual minority group (B = −0.15, SE = 0.04, p < .01). Thus, a one-unit increase in optimism was associated with a 0.15 unit decrease in depressed affect. However, social support and perceived control showed no significant associations with depressed affect in this group.
Regression Analyses for Heterosexual Group
Association Between Resilience Variables and Health Outcomes in Heterosexual Participants (n = 328).
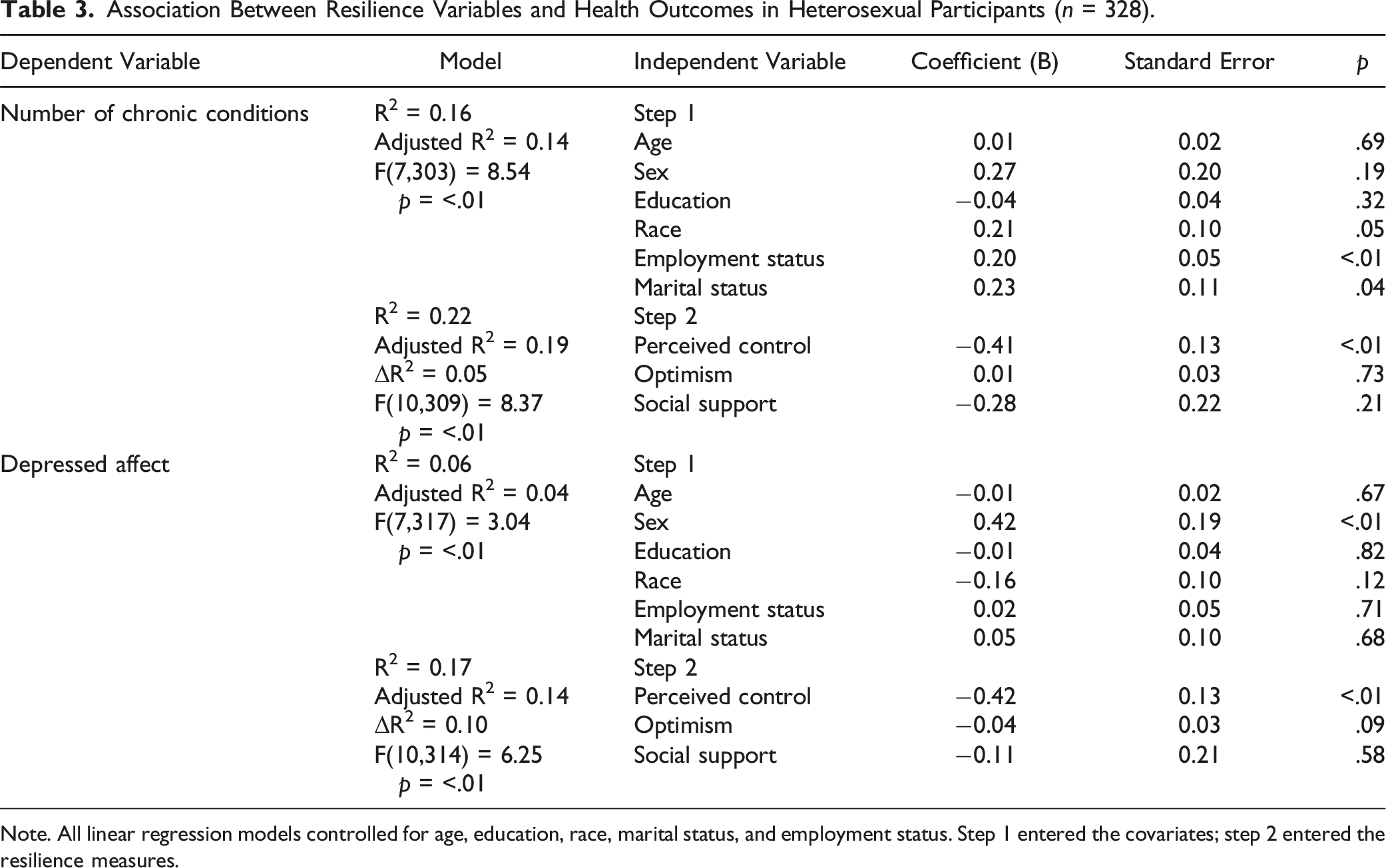
Note. All linear regression models controlled for age, education, race, marital status, and employment status. Step 1 entered the covariates; step 2 entered the resilience measures.
For depressed affect, the three resilience variables explained 10% of the variance after controlling for covariates (R2 = 0.17, ΔR2 = 0.10, F(10,314) = 6.25, p < .01). Only perceived control was significantly associated with depressed affect for the heterosexual group (B = −0.42, SE = 0.13 p < .01). Social support and optimism were not significantly associated with depressed affect.
Exploratory Analyses by Sexual Minority Subgroup
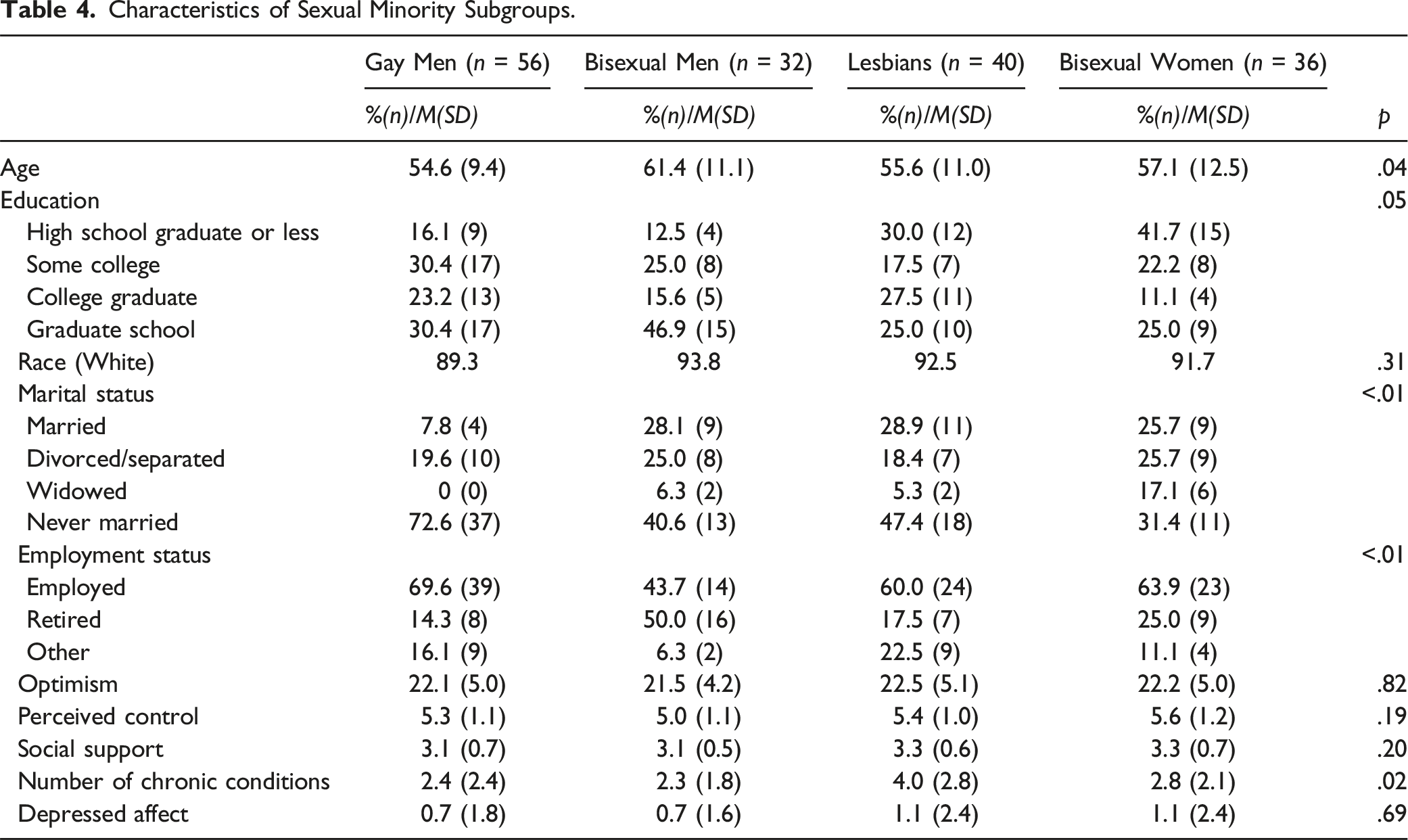
Characteristics of Sexual Minority Subgroups.
Association Between Resilience Variables and Health Outcomes for Each Sexual Minority Subgroup.
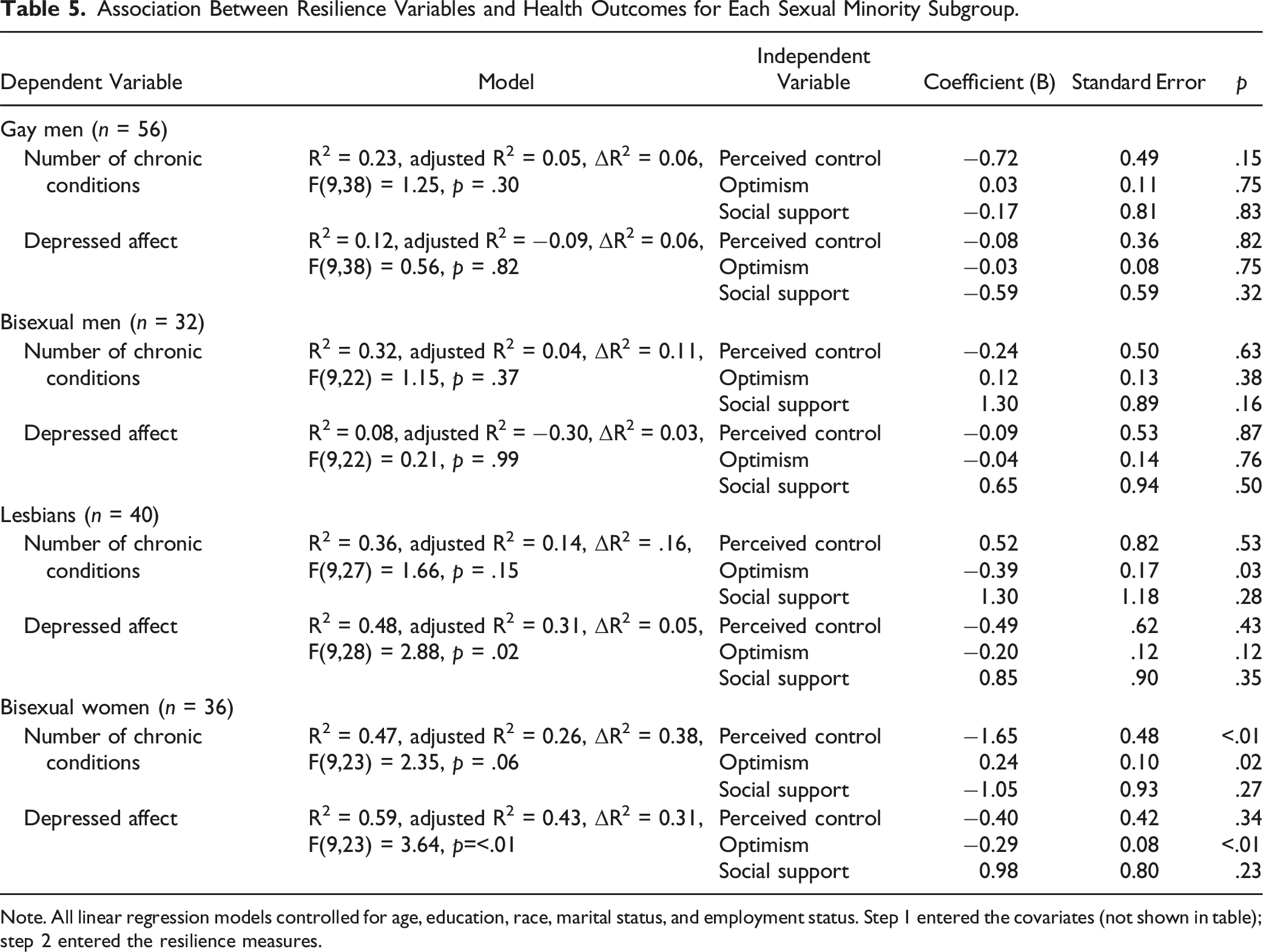
Note. All linear regression models controlled for age, education, race, marital status, and employment status. Step 1 entered the covariates (not shown in table); step 2 entered the resilience measures.
Regarding depressed affect, the three resilience measures explained 31% of the variance for bisexual women (R2 = 0.59, ΔR2 = 0.31, F(9,23) = 3.64, p < .01), but only 5% for lesbians (R2 = 0.48, ΔR2 = 0.05, F(9,28) = 2.88, p = .02). For lesbians, none of the resilience measures were significantly associated with depressed affect. However, for bisexual women, optimism exhibited significance after controlling for covariates (B = −0.29, SE = 0.08, p < .01), indicating that a one-unit increase in optimism corresponded to a decrease of 0.29 units in depressed affect. No resilience measures were associated with the outcomes for gay or bisexual men.
Discussion
This study represents a pioneering effort to examine the impact of three distinct resilience dimensions on the physical and mental well-being of both sexual minority and heterosexual midlife and older adults. Despite the hypotheses not finding support in the results, as not all resilience measures demonstrated significant associations with health outcomes in both sexual minority and heterosexual participants, intriguing patterns emerged. Perceived control exhibited significant links to the number of chronic conditions and depressed affect in heterosexual adults but displayed variability across health outcomes for sexual minority participants. Additionally, optimism was significantly associated with depressed affect exclusively in the sexual minority group. Surprisingly, social support was not significantly associated with health outcomes in the sexual minority group, contrasting with the expectations. The findings also highlighted variations within sexual minority subgroups, emphasizing the need for further research to explore the nuanced differences in resilience factors based on sexual orientation.
Resilience Disparities Between Sexual Minority and Heterosexual Adults
Perceived control was significantly associated only with the physical health outcome for sexual minority participants, while not manifesting the same association with the mental health outcome. This suggests a nuanced perception among older sexual minority individuals, shaped by their unique historical experiences, wherein they might feel more control over their physical well-being than their mental well-being. These individuals grew up during a time when homosexual conduct was not only illegal but also pathologized as a severe mental disorder (Foglia & Fredriksen-Goldsen, 2014; Fredriksen-Goldsen, 2016). Furthermore, sexual minority individuals may perceive having less control over external stressors like discrimination and victimization, which have been consistently linked to negative mental health outcomes (Feinstein et al., 2012; Lee et al., 2016). In contrast, among the heterosexual group, perceived control was significantly associated with both physical and mental health. Given that perceived control comprises elements of mastery and constraints, these findings may suggest that sexual minority individuals face additional constraints, such as discrimination and victimization, impacting their perception of control over their mental health.
The study found a negative association between optimism and depressed affect in sexual minority adults, consistent with previous research (Morrison, 2012), but this pattern was not observed among heterosexual adults. Findings from Gonzalez et al. (2021) and Nelson (2023) offer valuable context to this association between sexual minority midlife and older adults, contrasting with their heterosexual counterparts. Optimism expressed by sexual minority individuals, fostered by their resilience developed through past adversities (Gonzalez et al., 2021; Nelson, 2023), suggests a complex interplay between optimism, resilience, and the impact of discrimination. It implies that the protective effects of optimism against depressed affect may be nuanced and influenced by the unique challenges faced by sexual minority individuals.
Contrary to expectations, social support showed no significant association with physical or mental health in sexual minority midlife and older adults. The decision to combine social support from family and friends may explain the lack of significant findings between social support and health outcomes. Previous research has found significant differences in the composition of social support networks between sexual minority and heterosexual individuals, with sexual minority individuals typically having fewer family members but more friends in their networks (Hawthorne et al., 2020). In the absence of robust family support, sexual minority adults often rely on their “chosen family” or friends who provide the emotional support that biological family might not (Dewaele et al., 2011). However, a study found that only support from biological family was associated with lower depression (Milton & Knutson, 2023). Therefore, combining support from family and support from friends may have obscured any significant associations between social support and the health outcomes.
Exploring Sexual Minority Subgroup Differences
We explored resilience variations among different subgroups of sexual minority adults, revealing significant differences in the regression results. Notably, for gay and bisexual men, none of the three resilience measures were significantly associated with the health outcomes. Gender-based differences in resilience have been supported by prior research. A meta-analysis demonstrated that gender moderates the association between trait resilience and mental health, indicating a weaker effect for male participants as the male sample size increased (Hu et al., 2015). These gender disparities in resilience may stem from distinct socialization experiences. For example, Fredriksen-Goldsen and colleagues (2012) found that gay and bisexual men had smaller social networks and less social support compared to lesbian and bisexual women, suggesting differences in available resilience resources among various gender groups within the sexual minority community.
Lesbian and bisexual women also showed an interesting contrast. Optimism was significantly associated with the number of chronic conditions for these subgroups, with a potential dichotomy in its impact. While optimism appeared beneficial for the physical health of lesbians, it may have potentially detrimental effects on the health of bisexual women. The contrasting impact of optimism on the number of chronic conditions among lesbian and bisexual women may be influenced by the intersectionality of sexual orientation and gender identity. The unique health disparities and stressors faced by bisexual women, distinct from those experienced by lesbians (Fredriksen-Goldsen, 2016; Fredriksen-Goldsen et al., 2017), could contribute to the divergent effects of optimism. Factors such as biphobia, discrimination, and the invisibility of bisexuality within both heterosexual and LGBTQ+ communities (Dodge et al., 2016; Hayfield et al., 2014) may shape the relationship between optimism and health outcomes differently for bisexual women compared to lesbians.
Implications
This study significantly advances our understanding of resilience in sexual minority midlife and older adults by exploring the combined impact of various resilience dimensions within this demographic. It highlights nuanced psychological pathways that differentiate between sexual minority and heterosexual older adults, impacting their physical and mental well-being. The study suggests distinct resilience factors among sexual minority subgroups, with potential variations by gender.
While certain results remain inconclusive, the study strongly advocates for a resilience-focused paradigm in gerontological research, particularly regarding sexual minority older adults. Departing from deficit-based approaches, the findings underscore the importance of adopting a resilience-centered lens for understanding the unique challenges and strengths within this aging population. Recognizing and exploring the heterogeneity within sexual minority individuals and older adults becomes crucial, countering the tendency to homogenize these diverse groups. Although the study may not directly inform interventions, it lays the groundwork for future research endeavors characterized by larger and more diverse samples. These endeavors promise to uncover nuanced distinctions in strengths across diverse social identities, specifically relating to sexual orientation and age. This paradigm shift toward resilience and nuanced recognition of diversity holds substantial potential for enriching gerontological research, providing a more comprehensive understanding of the experiences and needs of sexual minority older adults, and guiding tailored interventions in subsequent studies.
Limitations
This study has several limitations to consider. The predominantly white and well-educated sample may limit generalizability, and participants’ older age (born between 1935 and 1964) cautions against extending findings to younger generations. The sample size, especially within the sexual minority group, may underpower certain analyses, warranting future research with larger, more diverse samples. Additionally, focusing on depressed affect as the mental health measure provides a limited view of overall mental well-being in older adults. Comprehensive mental health measures, such as the Geriatric Depression Scale (Brink et al., 1982), and improved measures of relational resilience are recommended for future research. Given the inconclusive results of this study, further investigations are needed to refine our understanding of resilience dimensions and their impact on health outcomes in sexual minority midlife and older adults.
Conclusion
This study sheds light on the complex relationship between resilience and health outcomes among sexual minority midlife and older adults. Optimism and perceived control were significantly associated with the health outcomes, albeit with varying impacts across subgroups. This study emphasizes the importance of ongoing research to deepen our understanding of resilience dimensions and their influence on health outcomes in this population, providing valuable insights for future interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.