
Abstract
A new multidimensional measure of test anxiety, the Test Anxiety Measure for Adolescents (TAMA), specifically designed for U.S. adolescents in Grades 6 to 12 was developed and its psychometric properties were examined. The TAMA consists of five scales (Cognitive Interference, Physiological Hyperarousal, Social Concerns, Task Irrelevant Behavior, and Worry). The results of confirmatory factor analyses on the responses of a sample of middle and high school students to the TAMA indicated that a five-factor (target) model provided a better fit to the data than a one-factor model. Results also indicated that the TAMA scores had adequate internal consistency reliability. Evidence supporting the convergent and discriminant validity of the TAMA scores was found. Implications of the findings for school personnel who work with adolescent students are discussed.
Keywords
Students taking standardized tests and classroom examinations are a common occurrence in U.S. schools. Legislation, such as the No Child Left Behind Act of 2001, has contributed to increased testing and testing requirements in U.S. schools (Wren & Benson, 2004). For some students, feeling worried, apprehensive, and tense are common symptoms experienced when they take tests. Test anxiety is the term used to describe these different symptoms that some students experience in testing situations (Spielberger & Vagg, 1995). Research has shown that test-anxious students do not perform well on tests (Bodas & Ollendick, 2005), and they experience difficulties learning in the classroom (Sub & Prabha, 2003). Test-anxious students are reported to have poorer academic performance (Eum & Rice, 2011; Segool, Carlson, Goforth, von der Embse, & Barterian, 2013), lower self-esteem (Pekrun, 2000), and more mental health problems (King, Mietz, Tinney, & Ollendick, 1995). More recent research suggests that test-anxious students may drop out of school earlier due to their anxieties experienced in testing situations and they may be more likely to be truant from school (Wild, Hofer, & Pekrun, 2006; Yousefi, 2012). These findings suggest that test anxiety is a serious problem (Ergene, 2003), affecting more than 33% of secondary students in U.S. schools (Methia, 2004). Yet, to the author’s knowledge, no multidimensional measure of test anxiety designed specifically for middle and high school students in the United States has been developed based on theory and current research in the field to identify those adolescent students who are test anxious. The present study addresses this gap in the literature with the development of a new multidimensional measure of test anxiety, the Test Anxiety Measure for Adolescents (TAMA), for middle and high school students in Grades 6 to 12 in the United States.
Dimensionality and the Test Anxiety Construct
Earlier researchers suggested that test anxiety is a unidimensional construct (S. B. Sarason & Mandler, 1952). S. B. Sarason and Mandler (1952) stated that student test performance is based on task-directed drives and learned anxiety drives, and those students with test anxiety experience impaired test performance because of their strong anxiety drives. Their strong anxiety drives lead to task irrelevant behaviors, such as avoidant behaviors, in evaluative situations. Wren and Benson’s (2004) and Lowe, Grumbein, and Raad’s (2011) works also support a behavioral component of test anxiety; however, Wren and Benson view the behavioral component as consisting of off-task behaviors, such as distracted behaviors, and Lowe and colleagues’ work highlights both avoidant and off-task (i.e., restless, fidgety, and distracted) behaviors.
Later, Sarason and colleagues (e.g., Sarason, Davidson, Lighthall, Waite, and Ruebush) advanced the field through changes in their own thinking, as they were the first to view test anxiety as a multidimensional construct, consisting of an affective and a cognitive component (Zeidner, 1998). Shortly, thereafter, Liebert and Morris (1967) differentiated the worry and emotionality components of test anxiety. Liebert and Morris viewed the worry component as excessive concerns and worries test-anxious students have about failing in testing situations and the emotionality component, now referred to as physiological hyperarousal (see Joiner et al., 1999), as the autonomic reactions or physical symptoms test-anxious students experience in evaluative situations. Review of the test anxiety literature has shown that the worry component of test anxiety is more strongly associated with test performance than the emotionality component (Wine, 1982; Zeidner, 1998). Wine’s (1971) cognitive-attentional model states that test-anxious students divide their attention between self-relevant (i.e., self-evaluative, self-deprecatory thinking and perception of their own autonomic responses) and task-relevant variables in testing situations, whereas low test-anxious students focus their attention on the test. Test-anxious students are more self-preoccupied than low test-anxious students, and their self-preoccupied thoughts interfere with their ability to give full attention to the test, resulting in poor test performance. Research has supported a cognitive interference or cognitive obstruction component of test anxiety (Friedman & Bendas-Jacob, 1997). Friedman and Bendas-Jacob (1997) also have suggested a social derogation component in addition to a cognitive obstruction and an affective component of test anxiety. In Friedman and Bendas-Jacob paradigm, social derogation refers to the worries test-anxious students have about social belittlement by significant others after they fail a test. Theory and research have supported these five (behavioral, cognitive interference, physiological hyperarousal, social derogation, and worry) components of test anxiety. Recent research views test anxiety as a complex construct, consisting of multiple dimensions (Zeidner, 1998). The five different dimensions discussed are thought to reflect the test anxiety construct. In the present study, these five facets of test anxiety guided the item generation process in the development of the TAMA.
Gender Differences
Gender differences have been examined on test anxiety measures (Harpell & Andrews, 2012; Lowe et al., 2011; Wren & Benson, 2004). Research has shown that females score consistently higher than males on test anxiety measures, and these differences have been reported in the United States and abroad (Harpell & Andrews, 2012; Hembree, 1988; Lowe et al., 2011; Putwain, 2007, 2008; Seipp & Schwarzer, 1996; Zeidner, 1998). Seipp and Schwarzer (1996) conducted a meta-analysis of more than 12 independent studies involving 14 different countries, including the United States, based on the cross-cultural adaptation of the Test Anxiety Inventory (TAI; Spielberger, 1980). The authors found that females scored higher than males on the TAI in all countries, except China and Turkey. Based on a review of the literature, it would be expected that gender differences would be found on new measures of test anxiety developed for U.S. students.
Relations With Other Variables
Spielberger (1972) made a distinction between state and trait anxiety in his state–trait model of anxiety. Spielberger viewed state anxiety as transitory in nature and a reaction to specific ego-threatening situations. In contrast, he viewed trait anxiety as a stable personality trait. Based on this state–trait distinction, Spielberger, Anton, and Bedell (1976) conceptualized test anxiety as a situation-specific form of trait anxiety. Therefore, scores of measures of test anxiety should correlate with scores of measures assessing trait anxiety.
In contrast, more recent research has found negligible relations between scores of test anxiety measures and scores of newer defensiveness or lie scales (Lowe et al., 2011; Lowe et al., 2008). Defensiveness scales assess the unwillingness of raters to admit to common imperfections (C. R. Reynolds & Richmond, 2008b). These findings are contrary to earlier research with older defensiveness or lie scales reporting a meaningful and negative relation between these two constructs (Hill & Sarason, 1966).
In the present study, a multidimensional measure of test anxiety, the TAMA, designed specifically for U.S. middle and high school students was developed and its psychometric properties were examined. To the author’s knowledge, no known multidimensional measure of test anxiety based on theory and current research has been developed specifically for middle and high school students in the United States. The factor structure, reliability, and convergent and discriminant validity of the TAMA scores were examined. Gender differences were also examined on the TAMA. The author hypothesized that (a) a five-factor model would provide a better fit to the data than a one-factor model; (b) the TAMA scores would demonstrate adequate internal consistency reliability; (c) gender differences would be found on the TAMA factors, with females scoring higher than males; (d) the TAMA (Cognitive Interference, Physiological Hyperarousal, and Worry) scores would correlate highest with the scores of another measure of test anxiety; (e) the TAMA scores would have moderate to strong correlations with the scores of a measure of trait anxiety; (f) the TAMA scores would have higher correlations with scores of similar than dissimilar dimensions on a measure of trait anxiety; and (g) the TAMA scores would have negligible correlations with the scores of a Defensiveness scale.
Method
Participants
The participants for the present study consisted of a total of 688 students, 293 (42.6%) males and 395 (57.4%) females. The students ranged in age from 11 to 19 (M = 13.38, SD = 2.05) and were in Grades 6 to 12 (M = 7.93, SD = 1.88). The racial/ethnic composition of the sample consisted of African Americans (2.8%), Asians (.4%), Hispanics (4.1%), Native Americans (3.1%), Whites (79.7%), and Others (10.0%). These students were recruited from 11 middle schools and high schools in the midwestern region of the United States.
Instruments
Revised Children’s Manifest Anxiety Scale-Second Edition (RCMAS-2)
The RCMAS-2 (C. R. Reynolds & Richmond, 2008a) is a 49-item self-report measure of general, manifest, or trait anxiety. The RCMAS-2 consists of a Total Anxiety scale, three anxiety (Physiological Anxiety, Social Anxiety, and Worry) subscales, and a Defensiveness scale. Students respond to the items on the RCMAS-2 using a yes/no format (C. R. Reynolds & Richmond, 2008b). Reynolds and Richmond reported test score stability coefficients of .64 to .76 over a 1-week test–retest interval for the RCMAS-2 scores. Coefficient alphas of .74 to .93 were found for the RCMAS-2 scores in the present study. Evidence supporting the construct validity of the RCMAS-2 scores has been found (C. R. Reynolds & Richmond, 2008b).
Behavior Assessment System for Children—Self-Report of Personality (BASC-2-SRP) Test Anxiety Scale
The BASC-2-SRP (C. R. Reynolds & Kamphaus, 2004b) Test Anxiety scale is a content scale consisting of seven items, which measures the physical and cognitive symptoms of test anxiety. C. R. Reynolds and Kamphaus (2004a) reported an adjusted test score stability coefficient corrected for restriction of range of .80 over a 13-to-66-day test–retest interval. A coefficient alpha of .78 was found in the present study. Evidence supporting the construct validity of the Test Anxiety scale scores has been found (C. R. Reynolds & Kamphaus, 2004a).
TAMA
The TAMA is a 44-item measure designed to assess test anxiety in middle and high school students in Grades 6 to 12. The TAMA consists of five scales. The Cognitive Interference scale (8 items) assesses the degree to which test anxiety interferes with organizing one’s thoughts, attending, concentrating, and remembering before and during an examination. The Physiological Hyperarousal scale (10 items) measures the physical symptoms associated with test anxiety. The Social Concerns scale (9 items) assesses an individual’s concerns about the perceptions of peers, parents, and teachers if one does not perform well on an examination and the Task Irrelevant Behavior scale (7 items) measures restless, fidgety, distracted, and avoidant behaviors associated with taking examinations. The Worry scale (10 items) assesses the worries one experiences before, during, and after an examination. The rater responds to the TAMA on a four-point (1 = never, 2 = sometimes, 3 = often, and 4 = almost always) Likert-type scale.
Procedures
Test development procedures
Eighty items were written for the TAMA based on a review of the test anxiety literature. Items were written for the cognitive interference, physiological hyperarousal, social concerns, task irrelevant behavior, and worry dimensions of test anxiety. These dimensions are thought to reflect the test anxiety construct. Rafferty, Smith, and Ptacek’s (1997) work was also consulted in the item writing process, as these authors suggested that test anxiety may be experienced before, during, or after an examination. Once the items were developed, two measurement experts and four teachers with experience in working with students in Grades 6 to 12 reviewed the items for their readability, clarity, and congruity with the test anxiety construct. Based on their feedback, some items were rewritten and 30 items were eliminated because they were difficult to understand, redundant, or did not align well with the different dimensions purported to reflect the test anxiety construct. The final draft of the TAMA consisted of 50 items. The 50-item draft was administered to the middle and high school students in the current study. Examples of the TAMA items are presented in Table 1.
Examples of Items on Each Factor of the Test Anxiety Measure for Adolescents.
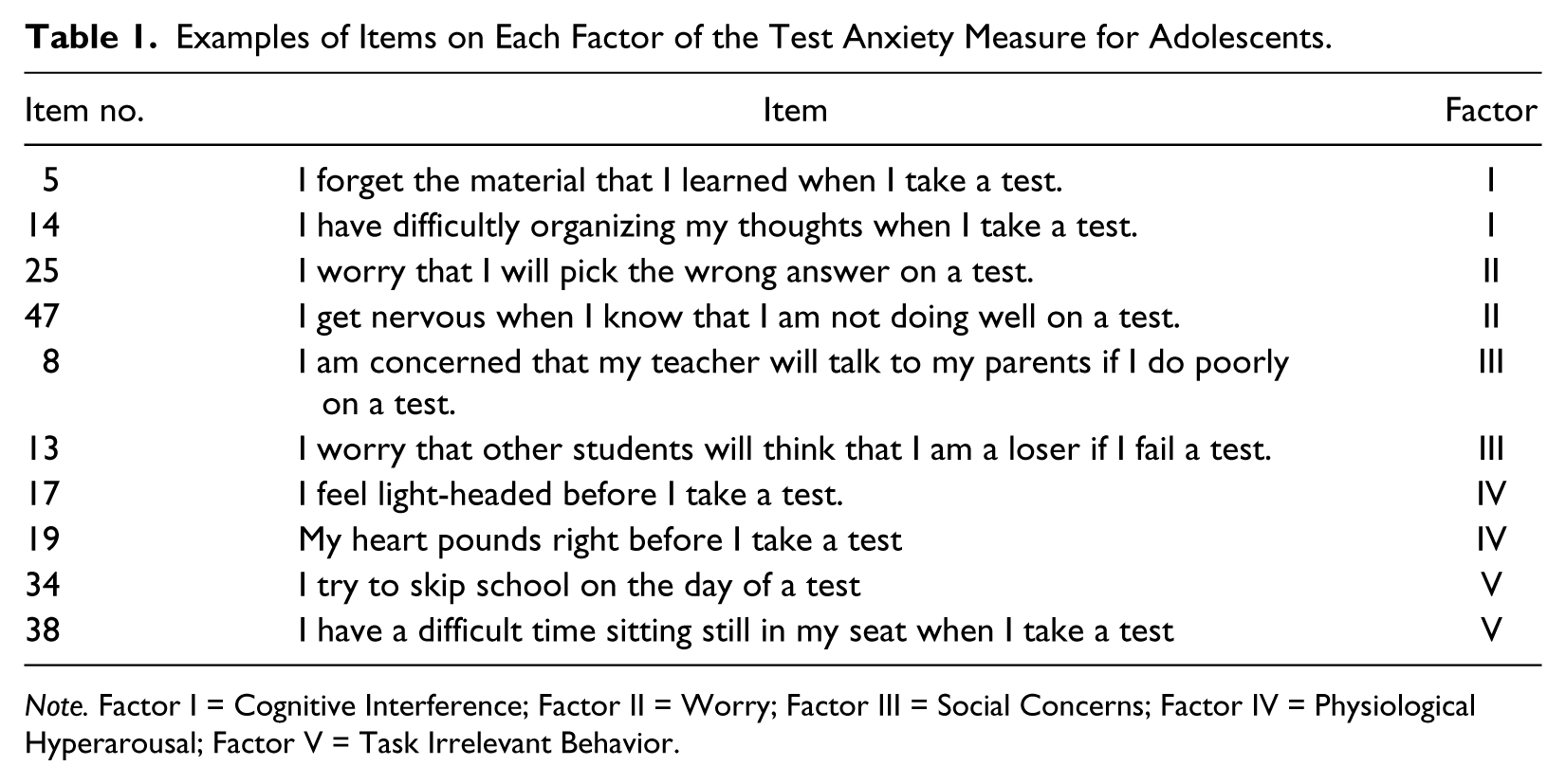
Note. Factor I = Cognitive Interference; Factor II = Worry; Factor III = Social Concerns; Factor IV = Physiological Hyperarousal; Factor V = Task Irrelevant Behavior.
Test administration procedures
Parent consent and student assent were obtained prior to the start of the study. During the study, all students were administered the 50-item draft of the TAMA, and a subsample (n = 592) was administered the 50-item draft of the TAMA, the RCMAS-2, and the BASC-2-SRP Test Anxiety scale, in large groups in their schools. For those students who completed three measures (i.e., the TAMA, the RCMAS-2, and the BASC-2-SRP Test Anxiety scale), the TAMA was administered first and the order of the other two measures was counterbalanced to prevent an order effect. Before the students began work on the measures, the test administrator requested that the students read the instructions printed on each measure.
Results
Sources of Validity
Evidence based on the internal structure
The total sample of 688 students was split in half (odd–even split) to scale and validate the measure. The first subsample (n = 344) was used to eliminate poor items on the 50-item draft of the TAMA. Criteria used to eliminate the poor items included low item-total correlations, standardized factor coefficients of less than .40 (Brown, 2006), and items with high modification index values, indicating an overlap of an item with more than one dimension (C. R. Reynolds & Kamphaus, 2004a). SPSS Version 20 (IBM, 2011) and Mplus Version 6 (Muthén & Muthén, 1998-2010) were used to perform the analyses. A total of six items were eliminated from the TAMA using these procedures; two items were eliminated because of low-item total correlations and/or standardized factor coefficients of less than .40 and four items were eliminated because the items had high modification index values, indicating that an item overlapped with more than one dimension.
Confirmatory factor analyses were then performed on the 44-item TAMA using the responses of the second subsample (n = 344). Mplus Version 6 was used to perform the analyses. A five-factor (target) model, consisting of 8 Cognitive Interference items, 10 Physiological Hyperarousal items, 9 Social Concerns items, 7 Task Irrelevant Behavior items, and 10 Worry items, was compared with a one-factor model. Model parameters were estimated using robust weighted least squares (WLSMV) due to multivariate non-normality and univariate non-normality (skewness = −.32 to 3.34 and kurtosis = −1.41 to 12.29) of the data and the categorical nature of the response options of the measure (see Flora & Curran, 2004; Wirth & Edwards, 2007). Fit indices (χ2, Comparative Fit Index [CFI], Tucker–Lewis Index [TLI], and root mean square error of approximation [RMSEA]) were computed to evaluate the overall fit of the models. Hu and Bentler’s (1999) guidelines (CFI and TLI values close to .95 and an RMSEA value less than .06) and a nonsignificant WLSMV χ2 value were used to indicate a good model fit.
Fit indices for the one- and five-factor models are presented in Table 2. Examination of the fit indices indicated that the majority of the fit indices for the five-factor model provided a good model fit to the data, whereas the fit indices for the one-factor model provided a poor model fit to the data. The standardized factor coefficients for the superior five-factor model are shown in Table 3. Standardized factor coefficients between the factors ranged from .53 to .85 and factor correlations ranged from .49 to .73 (see Table 3). The high correlation (r = .73) between the TAMA Physiological Hyperarousal and Worry scores is comparable in magnitude to the correlation reported between the Emotionality and Worry scores in other studies with other test anxiety measures (Everson, Millsap, & Rodriguez, 1991; Hembree, 1988), and the high correlation (r = .73) reported between the TAMA Cognitive Interference and Worry scores in the present study is not surprising as these scores both measure cognitive aspects of test anxiety.
Fit Indices From the Confirmatory Factor Analyses of the Test Anxiety Measure for Adolescent (TAMA) Scores (N = 344).
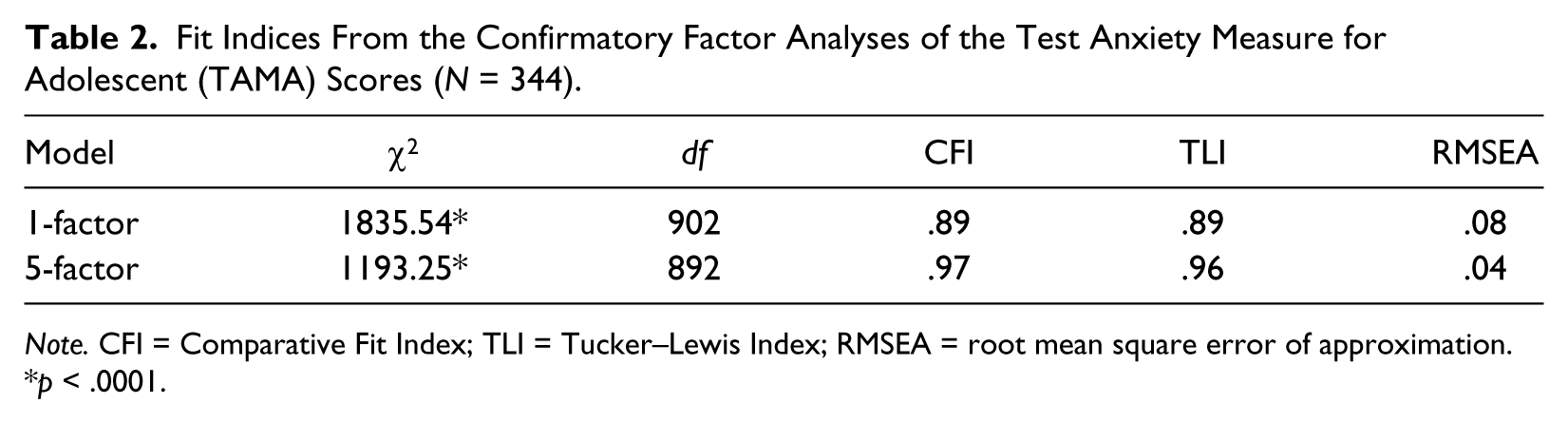
Note. CFI = Comparative Fit Index; TLI = Tucker–Lewis Index; RMSEA = root mean square error of approximation.
p < .0001.
Standardized Factor Coefficients and Factor Correlations for the Five-Factor Model for the Test Anxiety Measure for Adolescents (TAMA) Scores (n = 344).

Note. Factor I = Cognitive Interference; Factor II = Worry; Factor III = Social Concerns; Factor IV = Physiological Hyperarousal; Factor V = Task Irrelevant Behavior; Factor correlations are in parentheses.
p < .01.
Internal consistency reliability estimates and the 95% confidence interval (CI) around each reliability estimate were computed for the TAMA scores for the second subsample (see Table 4). Coefficients alphas ranged from .78 to .93 for the TAMA scores. Nunnally and Bernstein (1994) suggest a criterion of .70 as an acceptable level for a coefficient alpha. Therefore based on this criterion, the reliability estimates for the TAMA scores in the present study are considered acceptable for research purposes. In addition, the 95% CIs are also considered acceptable for research purposes, given the current data set. However, coefficient alpha is a biased estimate of reliability, but the degree of bias tends to be more substantial with fewer items on a scale (Green & Yang, 2009); this was not the case in the present study, as the TAMA scales are not short based on the number of items on each scale.
Coefficient Alphas (α) and the 95% Confidence Intervals (CI) for the Test Anxiety Measure for Adolescents (TAMA) Scores for the Second Subsample (n = 344).

Evidence based on group differences
Tests of measurement invariance are important to perform to be able to use the same test score interpretation across groups of interest (M. R. Reynolds & Keith, 2013). Lowe, Goldenberg, and Wheeler (2014) conducted tests of measurement invariance across gender on the TAMA and found support for partial measurement invariance. Therefore, means and standard deviations for the TAMA scores for the total sample, and male and female subsamples were computed (see Table 5), and independent t-tests were performed with gender (male, female) serving as the independent variable and the TAMA scores serving as the dependent variables in separate analyses in the present study. All t-tests performed were statistically significant for the TAMA Cognitive Interference, Physiological Hyperarousal, Social Concerns, Task Irrelevant Behavior, and Worry variables, with females scoring higher than males, with small to moderate effect sizes (see Table 5).
Means (M) and Standard Deviations (SD) for the Test Anxiety Measure for Adolescents (TAMA) Scores for the Total Sample (N = 688) and Male (n = 293) and Female (n = 395) Subsamples and Effect Sizes (d).

p < .001.
Correlation Coefficients Between the Test Anxiety Measure for Adolescents (TAMA) Scores and the Behavior Assessment System for Children, Second Edition—Self-Report of Personality (BASC-2-SRP) Test Anxiety Scores and the Revised Children’s Manifest Anxiety Scale (RCMAS-2) Scores for Middle and High School Students (n = 592).
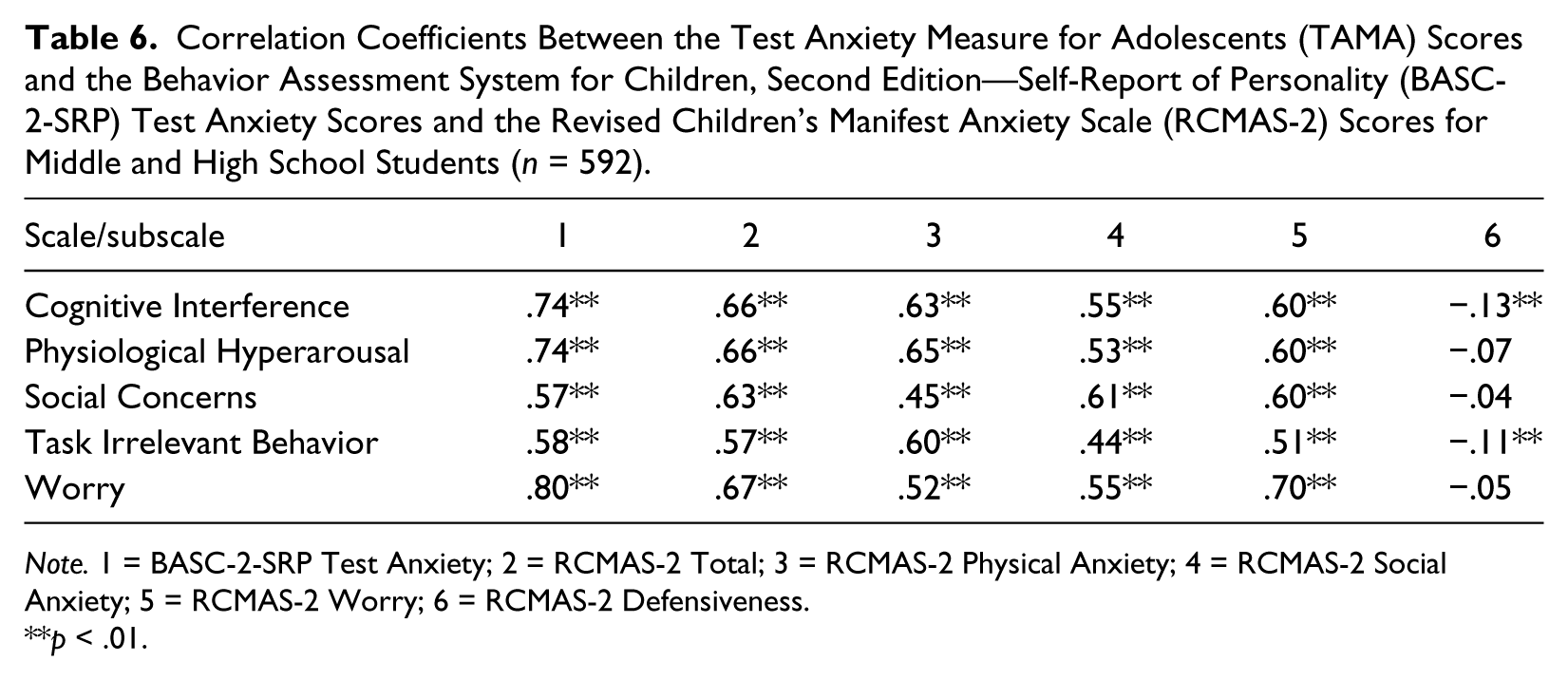
Note. 1 = BASC-2-SRP Test Anxiety; 2 = RCMAS-2 Total; 3 = RCMAS-2 Physical Anxiety; 4 = RCMAS-2 Social Anxiety; 5 = RCMAS-2 Worry; 6 = RCMAS-2 Defensiveness.
p < .01.
Evidence based on external relations
Correlation coefficients were computed between the TAMA scores and the scores of the BASC-2-SRP Test Anxiety and RCMAS-2 (see Table 6). Validity coefficients between the TAMA scores and the BASC-2-SRP Test Anxiety scores ranged from .57 to .80, accounting for 32.49% to 64.00% of the variance in the TAMA scores. For the TAMA Cognitive Interference, Physiological Hyperarousal, and Worry scores, they had their highest correlations with the BASC-2-SRP Test Anxiety scores. These findings were expected as the BASC-2-SRP Test Anxiety scale scores assess cognitive and physical symptoms associated with test anxiety (C. R. Reynolds & Kamphaus, 2004a). Correlations between the TAMA scores and the RCMAS-2 anxiety scores ranged from .44 to .70. These findings were also expected as test anxiety, as measured by the TAMA scores, is viewed as a form of trait anxiety (Zeidner, 1998) and manifest anxiety, as measured by the RCMAS-2 anxiety scores, was derived from a trait theory of general anxiety (C. R. Reynolds, 1985). It is interesting to note that the TAMA Physiological Hyperarousal, Social Concerns, and Worry scores had one of their highest correlations with the scores of a similar dimension on the RCMAS-2. Overall, these findings provide support for the convergent validity of the TAMA scores.
In contrast, correlations of −.13 to −.04 were found between the TAMA scores and the RCMAS-2 Defensiveness scores. These findings were expected as test anxiety and defensiveness are theoretically distinct constructs. Overall, these findings provide support for the discriminant validity of the TAMA scores.
Discussion
In the present study, a new multidimensional measure of test anxiety, the TAMA, designed specifically for middle and high school students in Grades 6 to 12 in the United States was developed and its psychometric properties were assessed. The TAMA is based on the most recent conceptualizations of the test anxiety construct and consists of five scales. The results of confirmatory factor analyses revealed that overall a five-factor model provided a good model fit to the data. These findings are in agreement with recent researchers’ view of the test anxiety construct as a complex construct, consisting of multiple dimensions (Lowe et al., 2011; Stöber & Pekrun, 2004; Zeidner, 1998). The results also revealed that the TAMA scores had adequate internal consistency reliability. In addition, evidence supported the convergent and discriminant validity of the TAMA scores. Furthermore, gender differences were found on all five scales of the TAMA, with females scoring higher than males. These findings are in agreement with the gender differences reported in the test anxiety literature (Harpell & Andrews, 2012; Lowe et al., 2011).
Researchers have reported developmental differences in the test anxiety construct (Lowe et al., 2011; Wren & Benson, 2004). Both Lowe and colleagues (2011) and Wren and Benson (2004) developed test anxiety measures for younger children, and these researchers found younger children responded to the items that assess cognitive interference and worry similarly. In both studies, Lowe and colleagues (2011) and Wren and Benson (2004) reported that the cognitive interference and worry dimensions of test anxiety did not separate from each other when the authors performed confirmatory factor analyses. This is in contrast to the finding reported in the present study, as adolescents, like adults (I. G. Sarason, 1984), responded to the items that assess cognitive interference and worry differently on the TAMA. The relevance of this finding is that the test anxiety construct may vary somewhat with age, and there may be a strong need to develop measures of test anxiety, such as the TAMA, for specific age groups. Additional research is needed to explore this issue.
The TAMA appears to be a promising new multidimensional measure of test anxiety designed specifically for adolescents in Grades 6 to 12 in the United States. Although additional research is needed, the TAMA may be helpful to school personnel in identifying adolescents who are test anxious and assisting those adolescents in reducing their test anxiety and improving their academic performance, as research has found there is a stronger negative association between anxiety and academic performance in adolescents than children (Hill & Wigfield, 1984). High scores on the different dimensions of the TAMA may guide school personnel’s intervention efforts to reduce test anxiety and its negative effects among test-anxious adolescents. For example, school personnel may find differential reinforcement, modeling, or possibly relaxation training effective in reducing avoidant, fidgety, distracted, and restless behaviors some students experience when they take examinations. To reduce intense physiological reactions, test-anxious students may benefit from behavioral strategies, such as relaxation and biofeedback training (Huberty & Dick, 2006). Cognitive-attentional training programs may assist test-anxious adolescents to attend to task-relevant stimuli, such as reading and thinking about items on a test, and to inhibit self-relevant thinking (Zeidner, 1998). Furthermore, positive self-statements and reattribution of faulty beliefs may assist test-anxious students who worry excessively when they take tests. These cognitive-behavioral strategies may help test-anxious students who worry excessively about tests to recognize and dispute their irrational thoughts and help them alter their negative attributions (Huberty & Dick, 2006).
Several limitations are associated with the present study. First, the sample used in the current study was a sample of convenience. A sample of convenience may limit the generalizability of the study. Therefore, replication of the present study yielding similar results would lend support to the findings reported in the current study. Second, the current study had fewer male adolescents and ethnic minorities, with the exception of Native Americans, in the sample based on current U.S. Census data (U.S. Census Bureau, 2011; U.S. Census Bureau, Population Division, 2012). In addition, only students from the Midwestern region of the country were represented in the study. Therefore, replication of the current study with a more diverse sample of U.S. adolescents from different geographic regions of the country and ethnic backgrounds and the inclusion of more males are needed to determine whether similar results would be found to those reported in the present study. More representative studies are needed in the future to help establish interpretative guidelines for the TAMA, so the TAMA can be used by practitioners who work with adolescents who may experience test anxiety. Third, the author analyzed the scores of self-reports in the present study to examine the convergent and discriminant validity of the TAMA scores. The use of self-report only may introduce method bias. Future studies with the TAMA should include a multi-trait multi-method analysis to examine the convergent and discriminant validity of the TAMA scores. Other directions for future research include studies that assess the test score stability of the TAMA scores and measurement invariance studies across ethnicities and adolescents with and without special needs to determine whether the same test score interpretation on the TAMA may be applied to these different groups. Lowe (2014) did conduct tests of measurement invariance across middle and high school students on the TAMA and found support for partial measurement invariance. Grade-level differences were also examined, and high school students scored higher than middle school students on the TAMA Cognitive Interference, Task Irrelevant Behavior, and Worry scales. Little research on grade-level trends on the different dimensions of test anxiety measures has been reported.
Although additional research is needed, the TAMA appears to be a promising new multidimensional measure to assess test anxiety among U.S. adolescents in Grades 6 to 12. Test anxiety is reported to be associated with poor academic performance (Eum & Rice, 2011; Segool et al., 2013), low self-esteem (Pekrun, 2000), anxiety and depression (King et al., 1995), grade retention (Beidel & Turner, 1988), and possibly truancy and early school dropout (Wild et al., 2006; Yousefi, 2012). Therefore, a measure, such as the TAMA, may prove invaluable to school mental health professionals in identifying those adolescents who are test-anxious, so intervention efforts can be directed to reduce their test anxiety and the additional problems that often accompany test anxiety among middle and high school students in U.S. schools.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.