
Abstract
We systematically reviewed studies reporting the use of the Children’s Depression Inventory-2 (CDI-2) in samples with at least 30 children and significant Hispanics enrollment (≥14.5% of the sample and at least 20 Hispanics completing the scale). We grouped studies by form (short or full-length) and language used, developmental stage, report of psychometric data (particularly for Hispanics), and other characteristics. From 252 full-texts revised, 22 met selection criteria. Six reported psychometric data for Hispanics, either for the English full-length (α = .86–.92) and short form (α = .76–.81) or for the Spanish short form (α = .69–.80). Criterion-related validity was supported via correlation/regression or comparing group means, but not using another depression self-report scale. Current knowledge on the CDI-2 psychometrics among Hispanics is mostly based on studies with the English-language version. No study has reported the psychometrics of the full-length Spanish-language CDI-2 with Hispanics.
Since 1977, the Children’s Depression Inventory (CDI) has been used to screen youth for depression and to assess the efficacy of depression treatment. A second edition of its self-report form, known as the CDI-2 SR, was published, and evidence of its psychometric properties with U.S. children was provided in a technical manual (Kovacs & Multi-Health Systems Staff, 2011). After conducting some changes in the scale, data were collected for a normative sample of 1,100 U.S. children and adolescents and a clinical sample of 319 youths, which formed a total sample of 1419 children.
The 28-item CDI-2 Total score has an alpha (α) coefficient of .91. This value was .90 for children aged 7 to 12 years and .92 for those aged 13 to 17 years. The measure has two higher order scales, named Emotional (α = .85) and Functional Problems (α = .83). The first includes the Negative Mood/Physical Symptoms (NM/PS; α = .75) and the Negative Self-Esteem (NSE; α = .77) subscales. Subscores on Ineffectiveness (INE; α = .76) and Interpersonal Problems (IP; α = .73) comprise the second scale. A 12-item short form (SF) is available (α = .82). It correlated .95 with the full-length form (Bae, 2012; Kovacs & Multi-Health Systems Staff, 2011). CDI-2 scores correlated (N = 266) with scores on the Beck Depression Inventory-Youth (.37) and the Conners Comprehensive Behavior Rating Scales-Major Depressive Episode scale (.58; Kovacs & Multi-Health Systems Staff, 2011).
Despite the normative sample for the English version of the CDI-2 aligned with the U.S. Census 2000 figures, with 14.5% of Hispanic youth (N = 160), psychometric analyses for racial or ethno-cultural groups are not available. Although White and African Americans had similar mean scores, Hispanics obtained significantly lower T-scores than Whites in the CDI-2 Total, Emotional Problems scale and NM/PS subscale (Kovacs & Multi-Health Systems Staff, 2011). Differences were significant after adjusting for age and sex, but effect sizes (partial eta squared) were very small, (.012 for the Total score). Similar differences were reported for the 12-item SF, with an effect size of .011 (Kovacs & Multi-Health Systems Staff, 2011). Yet, differences among Hispanics and Whites were not found in two studies that used the SF (Seegan, 2018) or the full-length form (Babakhanyan, 2013) with U.S. youth. In a third study, Hispanic youth were compared with a collapsed group of non-Hispanic Whites, Asian American, Native American, African American, and youth from mixed background. No difference was found in outcomes, including CDI-2 SF scores (Rogers et al., 2017). In a fourth study, being non-Caucasian was related with higher scores on the standard CDI-2 than among Caucasians (Becker et al., 2013).
Hispanics are an 18.3% (59.87 millions) of the U.S. population, being the nation’s largest ethnic/racial minority (U.S. Census Bureau, 2019a). As of July 1, 2018, about 25.2% of children 7 to 17 years in the United States were Hispanic (U.S. Census Bureau, 2019b). Among foreign-born Spanish speakers aged 5 years and over who live in the United States and speak Spanish at home, 68.2% speak English less than very well. The rate of children aged 5 to 17 years who speak Spanish at home but speak English less than very well was 19.7% (U.S. Census Bureau, 2018). Thus, knowing the state of evidence on the use and psychometrics of the Spanish CDI-2 (and not only the English version) may help to improve the quality of depression assessment not only for Spanish-speaking youth in Hispanic American countries but also for a significant amount of children in the United States.
In 2011, an official Spanish-language version of the CDI-2 was published (Kovacs & Multi-Health Systems Staff, 2011). Yet, no literature review has been conducted on studies using the CDI-2 with samples of Hispanic youth. We conducted a systematic review on studies reporting on the use of the CDI-2 full-length or SF in samples with significant enrollment of Hispanic youth and provided a qualitative synthesis of research that have reported the use of the English- or Spanish-language CDI-2 with prepubertal children or adolescents of Hispanic origin. Emphasis was given in the report of data on the psychometric properties of the scale among this population.
Method
Eligibility Criteria and Search Strategy
Journal articles, dissertations, and other electronically available sources were part of this review. To be eligible, studies must (a) have been published between January 1, 2010, and July 31, 2019; (b) have a sample size of at least 30 youths; (c) have used the English- or Spanish-language CDI-2; and (d) have a meaningful enrollment of Hispanics (≥ 14.5% of the overall sample, and at least 20 Hispanics completing the scale). Thirty was the minimum sample size due to Nunnally’s (1978) argument against alpha estimation with sample sizes lower than the number of items in the scale. Criteria for the inclusion of Hispanics were based in the percentage of their enrollment in the CDI-2 normative sample (Kovacs & Multi-Health Systems Staff, 2011). Requiring at least 20 Hispanics completing the CDI-2 in any given sample provided certainty that studies with small samples will have a predominantly (i.e., at least two thirds if N = 30) Hispanic sample.
We identified studies using redundant search procedures, including an electronic search, followed by a hand search of the reference lists of selected articles. PsycINFO, Psychology and Behavioral Science Collection, Psychology Database, Web of Science, ScienceDirect, SpringerLink, Google Scholar, Education Source, Academic Search Ultimate, ERIC, Sociology Source Ultimate, Open Dissertations, CINAHL, Caribbean Search, Fuente Académica Plus, eBook Collection, E-Journals, and MEDLINE articles from January 2010 to July 2019 were searched. The following keywords were used in any text field: Children’s Depression Inventory-2, Children’s Depression Inventory-2nd Edition, CDI-2, CDI2, or CDI-II.
Data Analysis
After retrieving records, duplicates were eliminated. Titles, abstracts, and keywords of nonduplicate records were revised to identify articles, book chapters, manuals, dissertations, or thesis that specifically reported about the use of the CDI-2. We excluded records reporting on another scale with the same acronym or on the CDI first edition, and any other unrelated record. Once target records were identified, full texts were collected and revised to distinguish between studies using the English- or Spanish-language version vs. other versions. We also excluded records that described the English version or previous psychometric reports but did not provide results from an independent sample. Next, we examined which of the selected full texts reported on samples with sizes ≥ 30 with a meaningful inclusion of Hispanic youth (as defined earlier).
Such records were classified into those providing some reliability or validity data for the CDI-2 in the general sample, studies that did not, and those with psychometric data specific for Hispanics. We distinguished studies considering the use of the full-length vs. the SF of the scale. Third, a distinction was made among studies using the English- vs. the Spanish-language version of the measure. In addition, studies were organized considering the developmental stage of participants. For the purpose of this review, a sample was considered to be of adolescents only if most participants were aged at least 12 years but no older than 18 years. Samples in which most participants had ages 11 years or below (such as samples of students from sixth grade and under) were considered to be of prepubertal children. In the fifth place, studies were analyzed with regard of their sample size. If using the full-length form, a sample was considered small if less than 140 youths were enrolled (rate of participants per scale item is lower than 5:1). A sample size was labeled as medium if enrollment was between 140 and 279 youths (a rate of at least 5:1 but less than 10:1). Samples with 280 participants or more were considered large. If using the CDI-2 SF, sample size was labeled as follows: small (less than 100 participants), medium (from 100 to 199), and large (200 and above). Sixth, studies with a majority of Hispanic participants were identified. Seventh, we identified studies with samples comprised by youth from families of middle-low or low socioeconomic status (SES), who were living in economic hardship, or who were facing very stressful life situations. Eighth, we examined if youth from any biological sex predominated in each sample and estimated its sex ratio. Ninth, studies were grouped as peer-reviewed articles or thesis/dissertations. Last, we counted studies with samples recruited in the United States, in Hispanic American countries, or part in the United States and part in a Hispanic American country.
Results
Selection, Number, and Categories of Eligible Studies
We collected 975 records. Duplicates (419) were deleted, and a pool of 556 records was screened for eligibility. Potential useful records were reduced to 252, by eliminating studies that reported on the use of other scale or unrelated to this review. We obtained full texts for these records and excluded 230 of them, as described in the “Data Analysis” section (Figure 1).
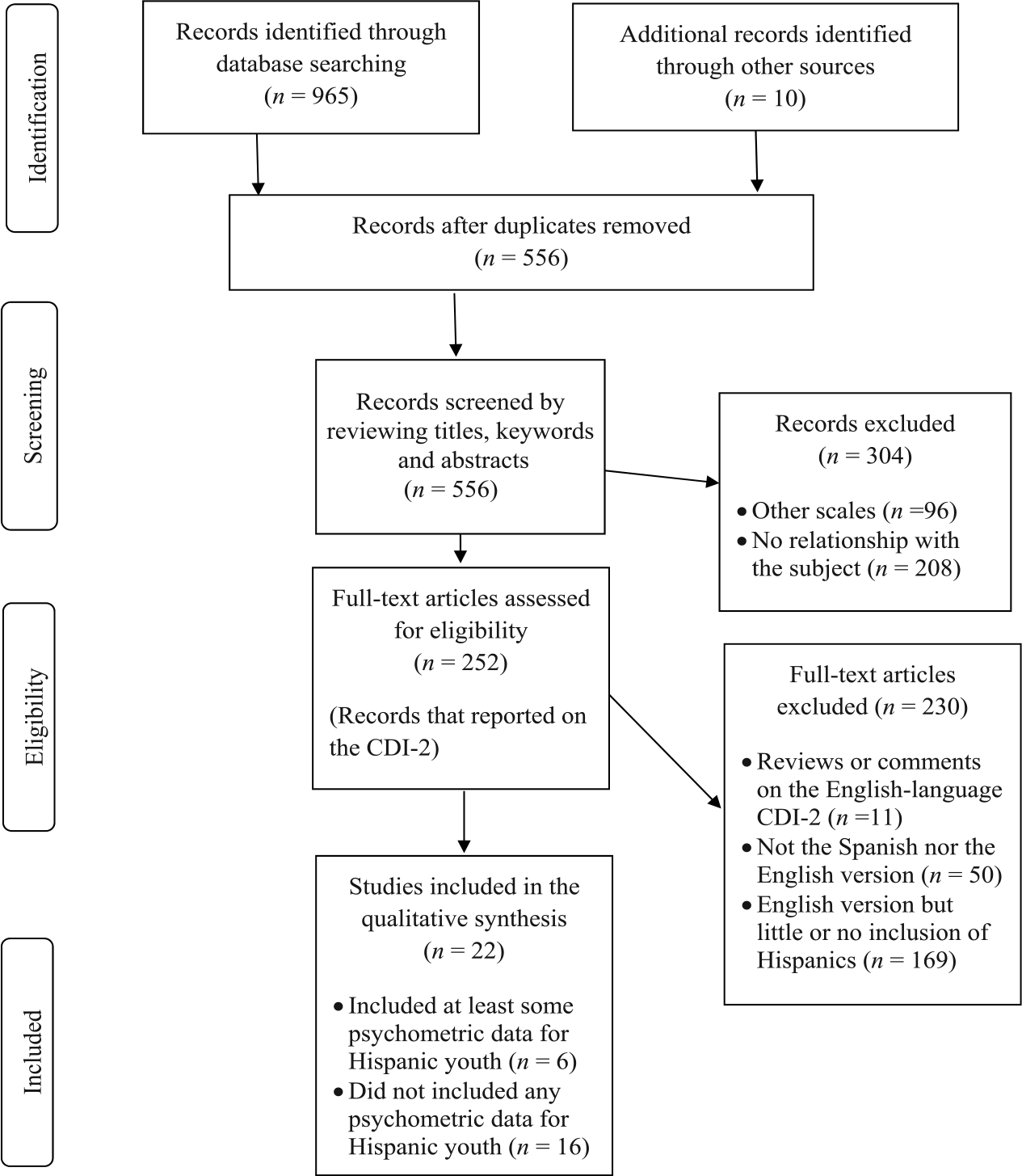
Flowchart for the systematic literature review on the use of the CDI-2 among samples with meaningful inclusion of Hispanic youth.
Table 1 includes a profile of the 22 studies that met the eligibility criteria. Six reported some psychometric data for Hispanics and 16 did not. Eleven of those 16 records (five of which did not report any psychometric data at all) described studies in which the full-length form was used. In seven of those 11 studies, the authors administered only the English version, while most participants in another study completed the Spanish version. In the remaining three, the authors did not clarify the proportion of youth who completed either version, although it was implicit that the English version predominated. In the other five studies in which the authors did not report psychometric data for Hispanics, they used the English-language SF. Among the six studies in which the authors did report some psychometric data for Hispanics, three used the full-length form (completed mostly in English) and three used the SF: one using the English-language version and two using the Spanish-language version. Psychometric data for Hispanics were reported in four peer-reviewed articles (Gulbas et al., 2016; Park et al., 2017; Suárez-López et al., 2019; Zayas et al., 2015) and two dissertations (Marchante-Hoffman, 2018; Scanlon, 2016). In these six studies, as well as in Tropez-Arceneaux et al. (2017), the sample was exclusively Hispanic.
Descriptive Profile of Eligible Studies According to 10 Categories for Classification.

Note. To increase clarity, the category about reporting of psychometric data was divided into three mutually exclusive columns. PRA = peer-reviewed article; DD = doctoral dissertation; MT = master thesis; EV = English version; SV = Spanish version; Both = English and Spanish version were available but most youth completed the English version; SF = short form; FLSR = full-length self-report form; NIC = Nicaragua; ECU = Ecuador; MX = Mexico; ALL = acute lymphoblastic leukemia patients; GEH = general economic hardship was mentioned in the sample description, although no data were provided on SES; ML/L SES = most participants were from middle-low or low socioeconomic status according to specific data provided (e.g., mean income, percent eligible for free or reduced meals at school, percent of parents with only a high school education or less, etc.); PPC = prepubertal children; ADOL = adolescents; COMB = prepubertal children and adolescents are combined in the sample; CDI-2 = Children’s Depression Inventory-2.
Over 60% of the sample recruited comprised girls, but the specific percent was not provided.
Samples of prepubertal children (n = 7) or that combined them with adolescents (n = 9) were more common than those including only or mostly adolescents (n = 6). Nine of the 22 studies had medium-size samples. Among those studies, four reported on the SF and five on the standard form. Eight of the 22 studies had large samples: four used the SF, and four, the standard form. Seven of those eight studies were peer-reviewed articles. In contrast, the five studies with small-size samples reported on the use of the standard CDI-2 and enrolled more girls than boys. Three of the latter studies were exclusively with Hispanics (Gulbas et al., 2016; Tropez-Arceneaux et al., 2017; Zayas et al., 2015). Among other studies with samples in which all participants were Hispanics, two had a medium (Marchante-Hoffman, 2018; Scanlon, 2016) and two had a large sample (Park et al., 2017; Suárez-López et al., 2019). Four of the eight studies with large samples enrolled prepubertal children. Seven of the nine studies with samples combining children and adolescents had samples of at least medium size. The exceptions were studies that exclusively enrolled Hispanics. Overall, 14 studies had samples mostly comprising girls; seven had samples mostly comprising boys, and one had a sample with equal distribution by sex. The study with the largest difference in the biological sex ratio had a girls-to-boys’ ratio of 7.6:2.4 (Esposito-Smythers et al., 2019). The average ratio across studies was 5.3:4.7 in favor of girls.
Most studies (18) had samples entirely recruited in the United States. The samples from two studies were recruited in Hispanic American countries (Nicaragua or Ecuador), and the remaining two samples were recruited partially in the United States and Mexico (Gulbas et al., 2016; Zayas et al., 2015). Fourteen studies were conducted with samples mostly comprising youths living in families with middle-low/low SES or with economic hardship (9), or by youths living in extremely stressful circumstances, such as having a severe physical illness (3), being through a suicidal crisis (1), or having experienced a physical trauma (1). Seven of the eight studies with a large sample were conducted with participants who met criteria for one of these subcategories. Fourteen eligible studies were peer-reviewed articles and eight were either dissertations (6) or theses (2). Nine of the 14 studies reporting about the full-length CDI-2, and five of the eight studies that reported on the CDI-2 SF, were peer-reviewed articles. Next, we present a qualitative synthesis of the findings of studies using the SF and the full-length form.
Qualitative Synthesis of Studies Using the CDI-2 SF
In six studies, the CDI-2 SF was administered using mostly or only its English-language version (Table 2). In the only of those studies that reported data for Hispanics, 97.8% of the U.S. adolescents of Mexican origin completed the scale in English. Alpha values from .76 to .81 were found along three assessments (Park et al., 2017). Positive associations for the SF with anxiety, discrimination, and outward anger expression scores, and a negative one with anger control were observed. In Arizona, a modified 12-item English version was used with 299 sixth graders (37% Hispanic). Alpha values from .70 to .74 were reported (DeLay et al., 2017). Significant associations were found among Time 1 experiences of homophobic name-calling and Time 2 CDI-2 SF scores. In related analyses with a subsample of 280 children (44% Hispanic), a negative relation between the SF and academic engagement and a positive link with conformity to traditional masculinity were reported (Rogers et al., 2017). Glynn et al. (2019), on their behalf, found significant correlations between the English SF and measures of anxiety, childhood unpredictability, and anhedonia among 175 adolescents (30% Hispanic) from California. After assessing 1409 children aged 8 to 12 years (15% Hispanics) using the English SF in Delaware, Swift (2016) reported alphas from .81 to .82. She also found positive correlations with self-reports on bullying victimization and perpetration, with anxiety symptoms, and with teachers’ reports of youth’s depressive symptoms. Yet, in the last four studies, analyses were conducted without considering race/ethnicity. This limitation also applied to a study by Seegan (2018), who reported an alpha of .74 among 197 youth from Texas, aged 9 to 18 years (18% Hispanic), positive correlations with anxiety and peer victimization, and negative ones with hope and social support.
Studies That Reported About the Use of the Children’s Depression Inventory-2 Self-Report Short Form Among Hispanics.
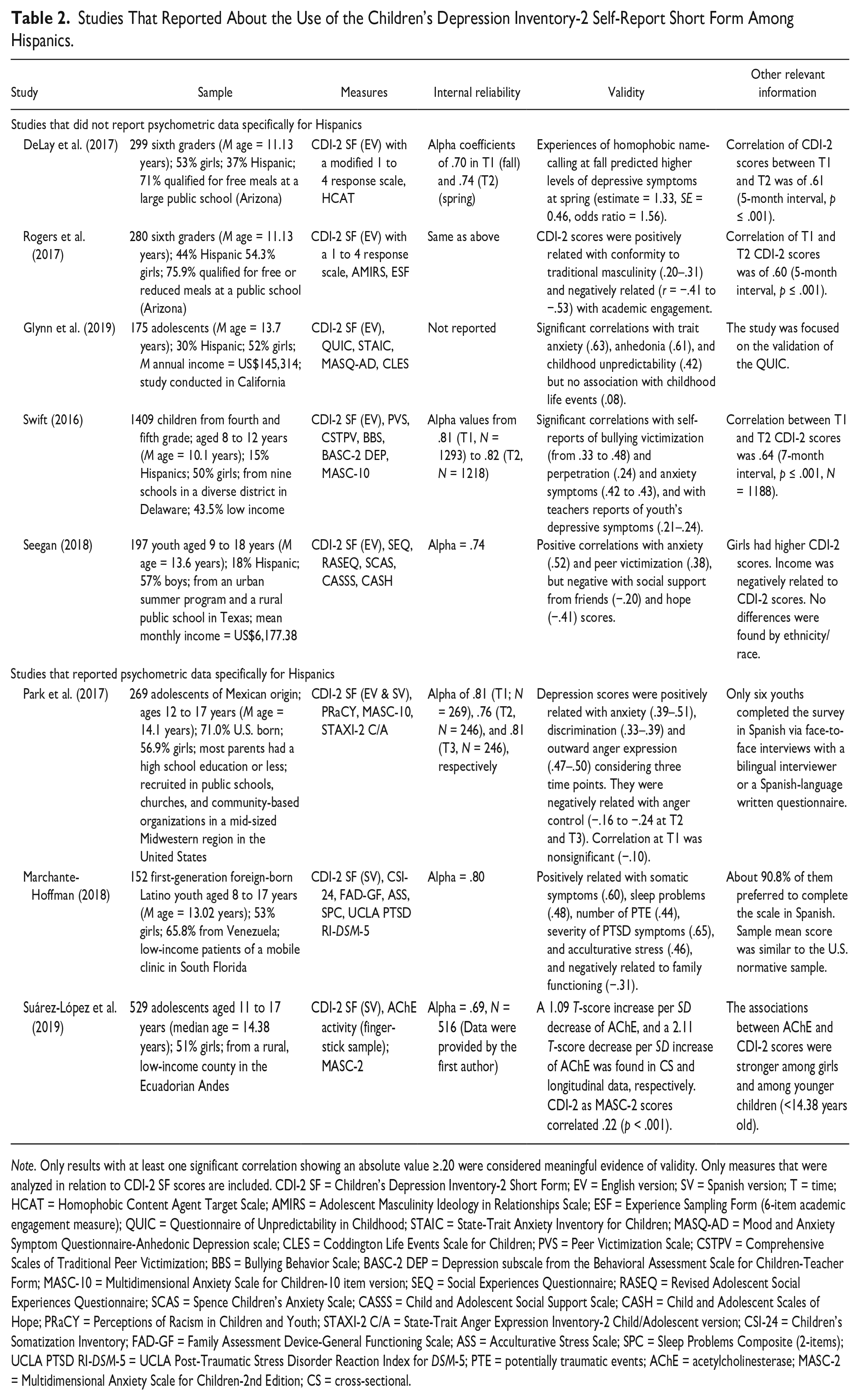
Note. Only results with at least one significant correlation showing an absolute value ≥.20 were considered meaningful evidence of validity. Only measures that were analyzed in relation to CDI-2 SF scores are included. CDI-2 SF = Children’s Depression Inventory-2 Short Form; EV = English version; SV = Spanish version; T = time; HCAT = Homophobic Content Agent Target Scale; AMIRS = Adolescent Masculinity Ideology in Relationships Scale; ESF = Experience Sampling Form (6-item academic engagement measure); QUIC = Questionnaire of Unpredictability in Childhood; STAIC = State-Trait Anxiety Inventory for Children; MASQ-AD = Mood and Anxiety Symptom Questionnaire-Anhedonic Depression scale; CLES = Coddington Life Events Scale for Children; PVS = Peer Victimization Scale; CSTPV = Comprehensive Scales of Traditional Peer Victimization; BBS = Bullying Behavior Scale; BASC-2 DEP = Depression subscale from the Behavioral Assessment Scale for Children-Teacher Form; MASC-10 = Multidimensional Anxiety Scale for Children-10 item version; SEQ = Social Experiences Questionnaire; RASEQ = Revised Adolescent Social Experiences Questionnaire; SCAS = Spence Children’s Anxiety Scale; CASSS = Child and Adolescent Social Support Scale; CASH = Child and Adolescent Scales of Hope; PRaCY = Perceptions of Racism in Children and Youth; STAXI-2 C/A = State-Trait Anger Expression Inventory-2 Child/Adolescent version; CSI-24 = Children’s Somatization Inventory; FAD-GF = Family Assessment Device-General Functioning Scale; ASS = Acculturative Stress Scale; SPC = Sleep Problems Composite (2-items); UCLA PTSD RI-DSM-5 = UCLA Post-Traumatic Stress Disorder Reaction Index for DSM-5; PTE = potentially traumatic events; AChE = acetylcholinesterase; MASC-2 = Multidimensional Anxiety Scale for Children-2nd Edition; CS = cross-sectional.
In a couple of studies, youth completed the CDI-2 SF using mostly or only its Spanish version. In one of those, the authors reported an alpha value of .80 among 152 first-generation foreign-born Latino youth aged 8 to 17 years (Marchante-Hoffman, 2018). About 90.8% of them preferred to complete the scale in Spanish. CDI-2 SF scores were positively related with somatic symptoms, sleep problems, number of potentially traumatic events, severity of post-traumatic symptoms, and acculturative stress, and negatively related to family functioning. In a recent publication, Suárez-López et al. (2019) used the Spanish-language SF with over 500 adolescents from the Ecuadorian Andes. In cross-sectional analysis, greater exposure to cholinesterase inhibitors (lower acetylcholinesterase activity) was associated to higher T-scores in depressive but not in anxiety symptoms. In longitudinal analysis (n = 223), reductions in T-scores on the SF were related to increases in acetylcholinesterase activity from 2008 to 2016. Although these data were not included in the published report, the alpha coefficient obtained within the sample was .69 and the CDI-2 SF showed a significant positive correlation (.22) with self-reports of anxiety symptoms (Suárez-López, personal communication, July 2, 2019).
Qualitative Synthesis of Studies Using the CDI-2 Full-Length Self-Report Form
In the first 11 studies on Table 3, the English or the Spanish full-length CDI-2 was used, but psychometric data were not reported or not analyzed separately for Hispanics. For example, Hockenberry et al. (2017) administered the CDI-2 to 236 children with acute lymphoblastic leukemia (ALL; 45.8% Hispanic). Only those aged ≥ 7 years filled the self-report form. Even though English- and Spanish-speaking children participated, the authors did not report how many youths completed either version. Two related reports (Hooke et al., 2018; Rodgers et al., 2019) were based on children with ALL who completed the standard CDI-2 but using a larger sample (N = 327; 47.4% Hispanic). Esposito-Smythers et al. (2019) used the English full-length form during the assessments of a Randomized Control Trial (RCT) for youth (N = 147; 16.55% Hispanic) who had experienced a suicidal crisis. In a study with 33 Hispanics in Nicaragua (aged 12–25 years) who have suffered burns, Tropez-Arceneaux et al. (2017) administered the Spanish version to those aged younger than 18 years (n = 20). However, none of these five studies reported any data on reliability or validity.
Studies That Reported About the Use of the Children’s Depression Inventory-2 Full-Length Self-Report Form Among Hispanics.

Note. Only results with at least one significant correlation showing an absolute value ≥.20 were considered meaningful evidence of validity. Only measures that were analyzed in relation to CDI-2 SR scores are included. NDR = no data reported; ALL = acute lymphoblastic leukemia; CDI-2 SR = Children’s Depression Inventory-2 Full-Length Self-Report Form; EV = English version; SV = Spanish version; T = time; BDI = Beck Depression Inventory; DPS-C = Depression Process Scale-Children; SES = socioeconomic status; BAI-Y = Beck Anxiety Inventory for Youth; BAI = Beck Anxiety Inventory; SASC-R = Social Anxiety Scale for Children-Revised; PARQ/Control = Parental Acceptance and Rejection/Control Questionnaire; PCS-YSR = Psychological Control Scale-Youth Self Report; PCDS = Psychological Control-Disrespect Scale; PCM = Psychological Control Measure (Parental report); Hx = history; MASC-2 = Multidimensional Anxiety Scale for Children (Child and Parent versions); MGI = Maladaptive Guilt-Induction Measure; EC = executive control; RCMAS = Revised Children’s Manifest Anxiety Scale; RCMAS-2 = Revised Child Manifest Anxiety Scale, second edition; BASC = Behavior Assessment System for Children; ADHD-I = attention-deficit hyperactivity disorder-predominantly inattentive type; NM/PS = CDI-2 Negative Mood/Physical Symptoms subscale; NSE = CDI-2 Negative Self-Esteem subscale; SCS = Self-Construal Scale.
On the other hand, Babakhanyan (2013) studied 168 youth aged 7 to 17 years (22.6% Hispanic) from Los Angeles and found CDI-2 scores to be significant predictors of depression diagnoses and to correlate with scores in the Depression Process Scale (DPS). Gelley (2014) used the full-length English version with 233 youth (27.04% Hispanic) in Grades 7 to 8, reporting an alpha of .82. Similarly, Morton (2018) reported an internal consistency of .89 among 133 youth aged 8 to 12 years (27.8% Hispanic), as well as positive correlations with measures of anxiety and maternal psychological and behavioral control, but a negative association with maternal warmth. Inter-rater agreement between youth and maternal ratings on the CDI-2 was .50. Within the same sample, Mathai (2018) reported correlations for the CDI-2 with scores of parental and youth anxiety, and mother’s maladaptive guilt-induction on children. Children with history of nonpharmacological mental health treatment showed higher CDI-2 scores. Nelson et al. (2018) reported an alpha of .80 among 280 youth aged 8 to 10 years (14.64% Hispanic). CDI-2 scores and anxiety symptoms correlated. Moreover, among 188 attention-deficit hyperactivity disorder (ADHD) children aged 7 to 11 years (15.43% Hispanic), Becker et al. (2013) found correlations with self-reported anxiety, ratings of youth symptoms in the Parent version of the CDI-2, and teachers’ ratings of child’s externalizing problems. However, in these latter six studies, no separate analysis for Hispanics was reported.
Only three studies have reported psychometric data for the full-length CDI-2 among Hispanics. Scanlon (2016) used the standard form with 141 Hispanic children aged 9 to 13 years. Internal consistency was .87. Symptoms were higher for children with a history of psychological treatment. CDI-2 scores were negatively related with reports of independent and interdependent self-construal, and maternal acceptance, and positively related to self-reports of manifest and social anxiety and maternal hostility/rejection/neglect, and with mothers’ reports of their child depressive (r = .40) and anxiety symptoms. Although available in English and Spanish, only one child completed the Spanish version. Zayas et al. (2015) used the full-length form with 83 US-born citizen-children of Mexican origin, aged 8 to 15 years. Some lived in Mexico with deported parents. Some lived in the United States but had at least a parent affected by detention or deportation (D/D), and others lived in the United States with undocumented parents not affected by D/D. Youth affected by a parent’s D/D reported higher scores than others in Total and Emotional Problems scores, and in the NM/PS and NSE subscales. An alpha of .86 was found. Although data were collected in either Spanish or English, separated psychometric data for each version were absent and no information was given on how many youths completed the scale in Spanish (Zayas et al., 2015). This suggests that most children completed the English version. Further analyses with a subsample of 48 youth (α = .92) showed that 50% of those (n = 16) with probable depression (independently of their parents’ D/D status) cited the stressed relation with parents as a factor that was salient to their experience of suffering, compared with only 9% of those (n = 32) without depressive symptoms (Gulbas et al., 2016).
Discussion
Some important points emerged from our review. Although 17 studies reported some psychometric data, only six included psychometric data for Hispanics. Four reported about either the short (Park et al., 2017) or full-length (Gulbas et al., 2016; Scanlon, 2016; Zayas et al., 2015) English version and two reported about the 12-item Spanish version (Marchante-Hoffman, 2018; Suárez-López et al., 2019). These six studies included data about internal consistency (α) and criterion-related validity. Four of them documented validity using correlations (Marchante-Hoffman, 2018; Park et al., 2017; Scanlon, 2016; Suárez-López et al., 2019) or a linear regression (Suárez-López et al., 2019) and three used analyses to compare group means (Gulbas et al., 2016; Scanlon, 2016; Zayas et al., 2015). Studies documenting validity with correlations or regression used both some criteria expected to be negatively related and criteria expected to be positively related to CDI-2 scores. No study that provided validity data on the CDI-2 when used among Hispanics included another depression self-report scale as criterion. The only study that reported a correlation with another depression scale (not just with another form of the same measure) only enrolled 22.6% of Hispanics, did not report separate analyses for this group, and was aimed to support the validity of another scale (Depression Process Scale-Children [DPS-C]) not the CDI-2 (Babakhanyan, 2013).
Among studies that included evidence on the validity of the CDI-2 SR among Hispanics, one provided inter-rater correlations (IRCs) with mother’s ratings on the parent-rated English version (Scanlon, 2016). Other two studies reported IRCs using these two forms of the English-language CDI-2, in a range from .25 (Becker et al., 2013) to .50 (Morton, 2018), but these studies only enrolled from 15.43% to 27.8% of Hispanics. By contrast, the IRC of .40 reported by Scanlon (2016) was obtained in a 100% Hispanic sample. This IRC value compares favorably with coefficients (.34–.36) reported in the CDI-2 manual (Kovacs & Multi-Health Systems Staff, 2011).
Many eligible studies (11) reported psychometric properties that were not specific to Hispanics. That was the case for five studies that reported on the use of the English-language CDI-2 SF, finding alpha coefficients from .70 to .82 and a wide range of convergent and divergent associations with validity criteria. Similarly, six studies reported on the use of the English full-length form without considering ethnicity/race, finding alpha values from .80 to .89 and a variety of correlations with validity criteria. In samples of the aforementioned studies that focused on the SF, inclusion of Hispanics ranged from 15% (Swift, 2016) to 44% (Rogers et al., 2017), while such inclusion ranged from 14.6% (Nelson et al., 2018) to 27.8% (Morton, 2018) in studies focused on the full-length form. Thus, in those 11 studies, the minority of children were Hispanics, and their inclusion was considerably lower in studies that used the full-length form.
Although it is uncertain to what extent psychometric findings of those 11 studies apply to Hispanics in their samples, there are similarities between their results and those from samples in which all participants were Hispanics. For example, in studies using the CDI-2 SF with Hispanic youth (either in English or Spanish), alpha values ranged from .69 to .81 (Marchante-Hoffman, 2018; Park et al., 2017; Suárez-López et al., 2019). Meanwhile, in studies that reported on the full-length form, reliability coefficients were from .86 to .92 (Gulbas et al., 2016; Scanlon, 2016; Zayas et al., 2015). In both cases, the range of reliability indexes was similar to the one reported within samples for which separate psychometric data for Hispanic were unavailable. Although patterns of correlations supported the validity of both CDI-2 forms in samples for which separate data for Hispanic were unavailable and in those comprising only Hispanics, correlational evidence of validity for Hispanics was more frequent for the SF than for the full-length form.
Three of the eight studies that used the 12-item SF had a sample comprised exclusively by adolescents: two with the English (Glynn et al., 2019; Park et al., 2017) and one with the Spanish version (Suárez-López et al., 2019). The other studies had either samples comprising prepubertal children (DeLay et al., 2017; Rogers et al., 2017; Swift, 2016) or a combination of prepubertal children and adolescents (Marchante-Hoffman, 2018; Seegan, 2018). Alpha values from .69 to .81 were observed in adolescent samples, with two of the three studies being conducted in Hispanic samples. Alpha coefficients showed magnitudes from .70 to .82 in studies with prepubertal children, although none of these published separate analysis for Hispanics. Alpha values from .74 to .80 have been found in studies combining youths from both developmental stages, with the higher coefficient belonging to the one conducted only with Hispanics. This suggest that, based on available studies, the internal consistency of the SF of the CDI-2 may be similar for children and for adolescents of Hispanic origin, at least to the extent that results from studies conducted exclusively with prepubertal children apply to Hispanic children. However, it is noteworthy that, as far as studies combining prepubertal children with adolescents did not publish separate analysis for either developmental group, no study has published psychometric data on the 12-item CDI-2 exclusively derived from prepubertal children of Hispanic origin.
Four of the 14 studies that reported on the use of the full-length form enrolled only prepubertal children, with alpha values from .80 to .89. Two studies included only adolescents, and one had a sample comprising mostly (61%) adolescents, but only Gelley (2014) reported an internal consistency value (.82) estimated exclusively for adolescents. No study has published psychometric data on the full-length CDI-2 (in either English or Spanish) exclusively derived from prepubertal children or from adolescents of Hispanic origin. Among the seven studies that reported on the full-length form in samples that combined children and adolescents, alpha values varied from .86 to .92, and those reporting reliability data were all conducted among Hispanics. Yet, none of those studies reported the psychometrics of the full-length Spanish CDI-2 among Spanish-speaking youth of any age group. In fact, our current knowledge on the psychometrics of the full-length form among Hispanics is based on three studies that used only or mostly the English version within samples that combined youth from different developmental stages.
We identified additional limitations in the current state of literature on the use of the CDI-2 with Hispanic youth. For example, none of the studies that included psychometric data for Hispanics reported results from a formal test–retest reliability study. The three studies (conducted on two samples) that estimated a correlation coefficient between CDI-2 scores obtained at two different assessment points reported coefficients in a range from .60 to .64 (DeLay et al., 2017; Rogers et al., 2017; Swift, 2016), but the interval between the two assessments (from 5 to 7 months) was too long. All three studies were conducted with the CDI-2 SF and the authors did not report separate analyses for Hispanics. Among eligible studies, a factorial or structural validity analysis was also lacking. In addition, only one eligible study provided any evidence of the sensitivity to change of the measure when used to assess treatment gains (Esposito-Smythers et al., 2019), but separate analyses by race/ethnicity were not considered. Although in other two studies do the authors mentioned that CDI-2 full-length form scores decreased over time (Hooke et al., 2018; Rodgers et al., 2019), such reduction did not support the sensitivity to change of the full-length scale as no treatment for depression was provided. On the other hand, only one study was conducted in a clinical sample of depressed youth (Esposito-Smythers et al., 2019) and none compared a clinical sample with a nonclinical one. Finally, as mentioned, no study reported the psychometric properties for the full-length CDI-2 using only (or mostly) the Spanish version.
In summary, what we currently know about the psychometrics of CDI-2 scores among Hispanic youth is based mostly on the use of the SF (in Spanish or English), or in the use of the English full-length form in studies that combined prepubertal children with adolescents, but did not provide separate psychometric analysis for either age group. Further studies should explore the psychometric properties of the CDI-2 in samples comprising only Hispanic prepubertal children, using exclusively either the Spanish- or the English-language version. The need for such studies applies for both the full-length and the SF of the scale. In addition, research on the Spanish-language version of the full-length CDI-2 using samples comprising exclusively Hispanic adolescents is needed. Either within samples of Hispanic prepubertal children or adolescents, future research should also examine the concurrent validity of the short and full-length forms of the English- and Spanish-language CDI-2 using another depressive symptoms self-report scale as validity criterion, not just the parent or teacher version of the CDI-2. Finally, researchers should conduct test–retest reliability studies of the CDI-2 (particularly for the Spanish version) among Hispanic youth, as these are currently inexistent. The same is true for studies on its factor structure among Hispanic youths, and for examinations of its sensitivity to change.
The current systematic review may encourage the conduction of additional empirical studies and systematic reviews regarding the use and the psychometrics of the CDI-2 not only among Hispanics but also among other ethno-cultural groups in the United States and in other countries. Findings from this study suggest the need for researchers to include psychometric data about the CDI-2 in their publications, even if their main purpose is not psychometric in nature. If conducting state-of-the-art research and clinical assessments grounded on best practices and research evidence when using the CDI-2 is a desired goal, evidence of its validity and reliability with specific groups must be provided. As far as we know, this is the first systematic review on the use and psychometric properties of the CDI-2 with a particular ethno-cultural group. More research is needed to increase the cumulative of evidence on its validity, reliability, and applicability across different ethno-cultural groups.
Footnotes
Author’s Note
The content is solely the responsibility of the author and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was possible thanks to funds granted by the President of the University of Puerto Rico to the Institute for Psychological Research, and to funds granted to the author by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health, under award number R03DK092547.