
Abstract
With the proliferation of participatory approaches to promoting youth development such as Youth-Led Participatory Action Research (YPAR), it is more important than ever that researchers and practitioners understand how to create curriculum that will authentically engage youth of color. To that end, there are important lessons public health researchers can learn from the fields of community psychology, education, and social work, among others. We explore the benefits of a youth-led research and action curriculum steeped in critical pedagogy and critical race theory focused on public health. Youth of color (N = 35) between the ages of 13 and 34 years from five U.S. cities were hired as researchers. The majority (57%) of youth were 16 or 17 years, and the gender split was female (57%) and male (43%). Key informant interviews with adults and qualitative data analysis techniques were employed to examine program products and outcomes. Materials were deductively coded for content related to critical pedagogy and race theory (e.g., empowerment, capacity building and community engagement, skill development) as well as conceptualizations of health. Findings indicate young people (a) began to think more consciously about health, what it means to be healthy, and the factors that influence health; (b) developed critical skills; and (c) described feeling empowered. When given resources and space to lead, we found youth to be insightful, resourceful, compassionate, and deeply committed to improving the lives of their peers, family members, and communities.
Keywords
Community-Based Participatory Research (CBPR) and Youth-Led Participatory Action Research (YPAR) present opportunities to engage young people of color in local decision-making (Sprague Martinez et al., 2018). Inherent in these methods is the assumption that all youth can be active agents in their own development and are capable of being important change makers in the broader community, when engaged (Lerner et al., 2005; Zimmerman et al., 2017). While creating opportunities to amplify youth voice and leadership is critical, it is equally important that participatory methods take into consideration complex systems and policies that perpetuate oppression and proliferate negative health outcomes for young people of color (Ginwright & Cammarota, 2002; Ginwright et al., 2006). Despite the extensive empirical literature showing the benefits of YPAR (Ozer, 2016; Wallerstein & Duran, 2006), little has been written about strategies for engaging youth of color in public health efforts using YPAR strategies. This article adds to the literature by (a) highlighting strategies for engaging youth of color in public health efforts using YPAR and (b) demonstrating how YPAR can add to young people’s understanding of the impact of systems of oppression on health and health-related decision-making.
Not by chance, youth of color are at heightened risk of experiencing poor health, both during early childhood and across the life span (Brown et al., 2007; Geronimus & Thompson, 2004; Jackson et al., 2010; Viner et al., 2012). Racialized policies and institutional practices (e.g., housing, schools, social welfare, and criminal justice) have historically and continue to have deleterious effects for youth of color, their families, and the broader community (Alexander, 2012; Heitzeg, 2009; Oliver & Shapiro, 2006; Shapiro, 2004). Engaging youth of color in health equity work is critical to the health of the nation, particularly given their heightened risk profile and the fact that they represent the fastest growing segment of the youth population (Colby & Ortman, 2015). Moreover, excluding their voices perpetuates a system of oppression, by failing to provide them with spaces in which they can grapple with the relationship between historical and socioeconomic conditions that affect their lives. In addition, failure to acknowledge the value of their lived experience may result in community decision-makers missing important information about the barriers and opportunities with which youth of color are presented (Sprague Martinez et al., 2018); particularly given that youth of color experience environmental conditions differently from both adults and their White peers (Sprague Martinez et al., 2017).
There is empirical evidence that, beyond individual behaviors, neighborhood context has been significantly associated with health problems, such as mortality, cardiovascular disease, depression, and cancer (Yen & Kaplan, 1999). Furthermore, findings of a systematic review of empirical research on self-reported racism and health suggest that racism is associated with ill health (Paradies, 2006). Research also suggests broader systematic social/environmental factors place individuals’ health at higher risk and limit the extent to which they can access resources for positive health promotion (Braveman et al., 2011). Given the significant research exploring health interventions enhancing access, coverage, and quality of medical health care, it is essential to promote and implement “upstream” community-driven health interventions and policies that address social determinants of health in order to reduce health disparities, particularly among disadvantaged communities (Gehlert et al., 2008; Williams et al., 2008). While health research has engaged youth of color meaningfully in identifying health threats and assets in their environments (Peréa et al., 2019; Sprague Martinez et al., 2012), there is limited research in engaging youth authentically in “upstream” approaches to health assessments, interventions, and policies. Failure to engage youth in health research that incorporates a critical historical context of the social determinants of health neglects the youth’s lived experiences and reality.
Community-driven research approaches like CBPR present an alternative research paradigm that recognizes multiple forms of creating knowledge, emphasizes relationships between academic and community partners, and leverages the strengths of community knowledge and participation (Wallerstein & Duran, 2006). Similarly, YPAR leverages the strengths of young people, engaging them in the study of social problems through critical reflection and action-driven inquiry in an effort to catalyze social change (Baum et al., 2006; Cammarota & Fine, 2010; Ozer, 2016). Both CBPR and YPAR have been shown to have positive outcomes for youth as well as the broader community, by increasing sociopolitical skill development and motivation to promote social change (Ozer & Douglas, 2013; Sussman, 2015). Although the benefit of CBPR and YPAR has been recognized across academic fields including education (Cammarota, 2014; Cammarota & Fine, 2010; Caraballo et al., 2017), public health (Sprague Martinez et al., 2017), community psychology (Chan et al., 2003), and social work (Teixeira, 2015, 2016), little is known as to the best practices for engaging youth of color in health research and action, and more specifically, which practices contribute to positive outcomes for youth of color.
Drawing on lessons learned from the first multicity youth-led health assessment implemented in the United States, this article presents a pedagogical approach and curriculum designed for implementation by adult supporters and researchers who seek to create leadership spaces in which youth can grapple with complex community health issues, and engage in research to inform action aimed at improving social factors that influence health. A brief overview of the literature on youth participation and critical pedagogy is presented. The youth engagement strategy and the process of implementing it is then discussed in depth followed by a detailed description of the youth and adult training curriculum. Research protocols developed by the young people, as well as adult perceptions of the training, are then presented and followed by a discussion of results and lessons learned associated with training implementation.
Youth-Led Participatory Research
Participation has been conceptualized in the literature as a process through which young people engage in and have influence over factors that shape their lives and the lives of others (Checkoway, 2011; Pritzker & Richards-Schuster, 2016; Teixeira, 2016). The youth participation scholarship emphasizes young people should be viewed as community assets (Checkoway et al., 2003; Finn & Checkoway, 1998). This perspective assumes that active participation of young people is important for both democracy and promoting well-being (M. Delgado, 2006). The benefits of youth engagement and participation have been well documented in the civic engagement literature. Engaging youth through service-learning and volunteerism contributes to the development of both leadership skills and civic values (Boyte, 1991; Flanagan, 2004; Morgan & Streb, 2001). Much like YPAR, these models are effective for engaging youth meaningfully by involving them in applied problem-solving while making meaningful contributions to the broader community (Andolina et al., 2003; Boyte, 2005). However, not all youth have equal access to participation, particularly low-income youth of color due to structural social, economic, and political constraints such as racism, unemployment, and violence (Ginwright & Cammarota, 2002). Thus, integrating a framework beyond service-learning that creates the space for youth to develop a critical awareness of these constraints in their lives is fundamentally important. This paper adds to literature in the area of critical service-learning, which is experiential learning steeped in social justice (Wang & Rodgers, 2006). Critical service-learning positions students as change agents, allowing them to identify inequities in the broader environment (Mitchell, 2008). We use a social justice youth-led research and action framework to provide a space in which young people of color can grapple with, study, and mitigate systems of oppression that affect their health and well-being.
The benefits of engaging youth in research and action have been well documented. Research experiences provide professional development opportunities in addition to contributing to the development of civic-minded, healthy, and caring adults (M. Delgado, 2006). Ozer and Douglas (2013) found that youth who were involved in participatory research exhibited growth in sociopolitical skills, and increased motivation to participate in schools and communities. Similarly, youth research partners in a substance use prevention partnership reported learning more about the research process and the impact of substance abuse, as well as gaining leadership skills (Kulbok et al., 2015). In addition to contributing to holistic and skill development, engaging youth in research and action creates further opportunities and access for marginalized youth to be at the table through presentations to key policymakers (Kirshner et al., 2005).
Working in partnership with youth and providing them with leadership opportunities may also reduce the risk of adult-centric perspectives on youth and the broader community (Chan et al., 2003). Augsberger (2017) and colleagues found that youth participation in municipal government positively informed decision-making related to policies that affect youth (Augsberger et al., 2017). Meanwhile, during a critical service-learning intervention focused on health research and action, youth identified significant health threats related to sanitation; adults, meanwhile, were focused on the food environment, overlooking sanitation (Sprague Martinez et al., 2012). Youth, however, interpreted sanitation issues as community neglect and disinvestment (Sprague Martinez et al., 2012). It influenced how they thought about their community and themselves (Sprague Martinez et al., 2012, 2017).
Critical Pedagogy
YPAR is rooted in principles of equity and is designed to engage young people in applied inquiry and action (Ozer, 2016). A key assumption embedded within the YPAR approach is that young people are experts in their lived experiences and that the role of adults is to support them in developing a more nuanced understanding of complex social and environmental issues that affect their health and well-being. As such, YPAR draws on popular education, an approach in which individuals commit to social change by leveraging their knowledge and lived experiences, and engaging in continuous, critical reflection and action (Freire, 1970). Similarly, YPAR also draws from critical pedagogy, which is focused on learner empowerment (and broader youth empowerment). Freire (1970) pointed out the oppressive nature of the education system, which he described as Educação Bancária, a hierarchical system in which adults at the top must fill youth (empty vessels) with information. In this system, young people are not given a chance to digest the information they are gaining. They only hold it. There is no space to challenge, question, or create. Moreover, disempowered youth are discouraged from thinking critically about what they are learning in the context of their lived experience (Freire, 1970). Unlike traditional didactic educational approaches, critical pedagogy engages young people in a transformative consciousness raising process by recognizing the knowledge embedded within their personal narratives and allowing them to grapple with it. It stresses the importance of creating space for reflection, analysis, and resistance and youth are encouraged to act to ameliorate injustices (Luque et al., 2011). More recently, critical pedagogy approaches to research in education have been incorporated throughout the literature to situate youths’ lived experiences in relevant cultural and sociopolitical contexts and disrupt social inequities inside and outside of the classroom (Bellino & Adams, 2017; Chinman & Linney, 1998; Schindel Dimick, 2016).
Project Overview
In this paper, we present an illustrative description of a youth and adult YPAR training program designed to engage youth of color in health assessment and community action. We employed critical race theory (R. Delgado & Stefancic, 2017) to incorporate youths’ intersectional lived experiences, which consistently interact with racial power structures and systems of oppression. To that end, the training integrated activities in the curriculum and provided a safe environment for young people to grapple with threats to health and health-promoting assets in the context of White supremacy, an ideology embedded in U.S. culture, policies, and institutions that posits White people are supreme and thus should dominate all other races. Building on the strengths of the youth researchers and adult coordinators, the training acknowledged young people as a knowledgeable resource, valuing their perspective and lived experience. Activities were embedded in the training program with the research team’s intention to provide opportunities for the youth researchers to shape discussions based on their personal experiences and trust the process. During the trainings, youth were encouraged to think critically about what they were observing in their communities in the context of the information they were learning about health and the social determinants of health.
Getting Started
First, the adult research team identified five individual community-based organizations and local organizers across the country based on prior collaborations and project goals alignment. Initial organization interviews were conducted to learn about the programs, activities, staff, and goals of the organization and local organizers. Then, the adult research team partnered with community-based organizations and local organizers to recruit one adult staff coordinator and four to eight youth of color in each of the five U.S. cities. Youth of color in Boston, Chicago, Denver, Philadelphia, and St. Paul were engaged in a process of identifying the following: (a) health priority areas, (b) health risk and protective factors that affect young people and are embedded in the built environment which refers to person-made environments (e.g., parks, roadways, neighborhoods, and so on), and (c) strategies for closing the gap between health-promoting assets that appear to be available in communities, and youth engagement of those assets. The aim of focusing on multiple cities was to understand whether the typical highly contextualized findings of YPAR would be consistent across cities and, therefore, give greater voice to the barriers identified by young people in those cities and throughout the country. The project was implemented over a 6-month period. Figure 1 (Timeline) outlines the project life cycle from early May, when cities were being identified, through October, when sites completed the implementation phase.

Project timeline.
Local sites were responsible for having an adult coordinator and identifying 6 to 10 youth who could commit at least 20 hours per week over a 4- to 5-week period. Sites were also asked to identify one staff member who would be responsible for coordinating the youth at their site.
The training and assessment was framed as a part-time summer employment opportunity for youth interested in community health research and/or community action. Funds were allocated for sites to cover the costs associated with adult coordinator, youth researcher stipends, and travel for two youth team members and the coordinator to Washington, DC, to present their findings at a national convening of community-based practitioners.
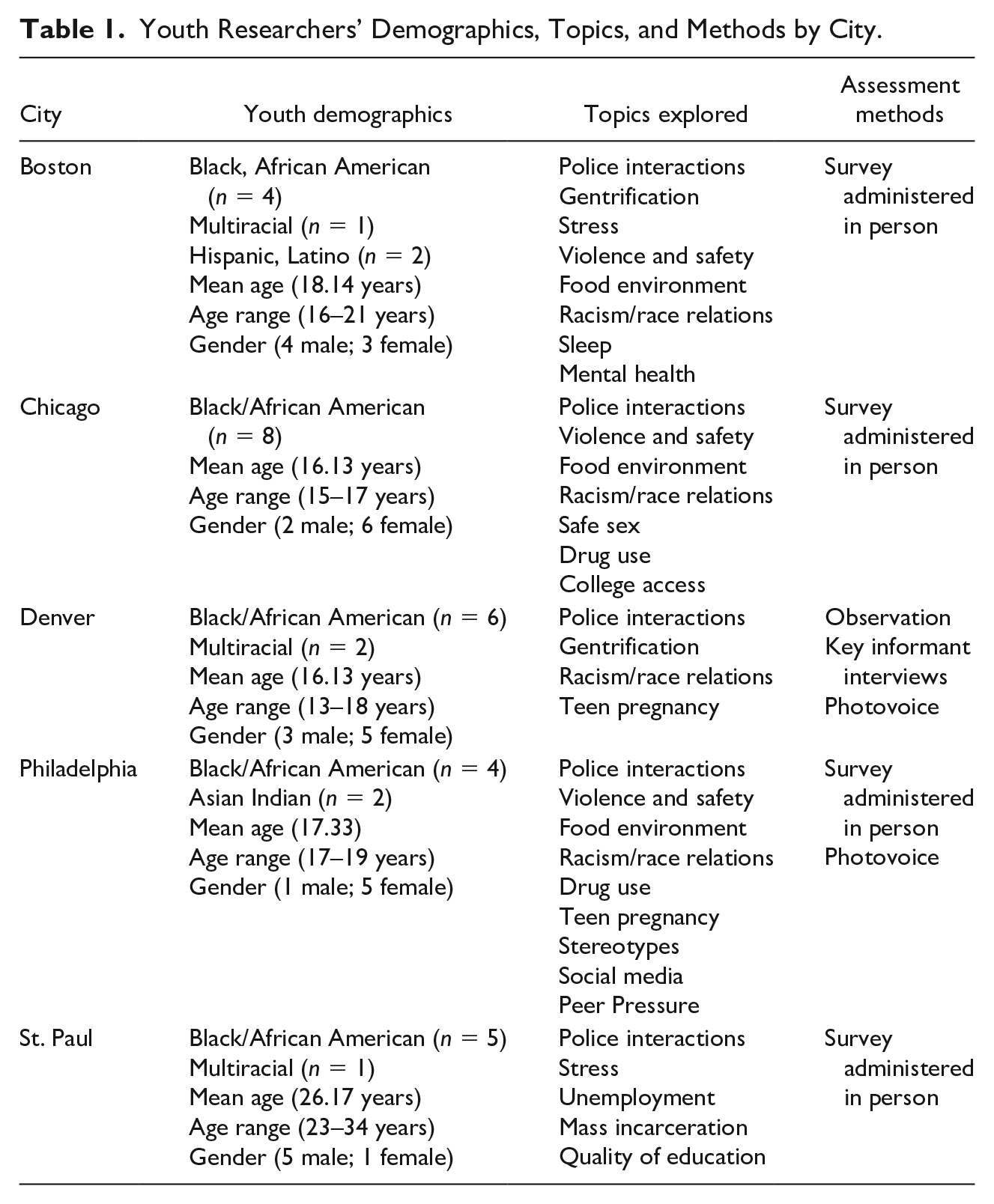
There were a total of 35 youth researchers across five project sites. Youth researchers ranged in age from 13 to 34 years (M = 18.46 years). The majority of youth researchers (57%) were 16 or 17 years of age. There was one site that worked with young men in reentry from the justice system, and youth at that site were aged 23 to 34 years. There were more female (57%) than male researchers (43%). Youth researchers identified primarily as Black or African American (74%). See Table 1 for youth researcher demographics.
Youth Researchers’ Demographics, Topics, and Methods by City.
YPAR Training
The youth research team training protocol was developed based on the Nuestro Futuro Saludable (NFS) afterschool program intervention (R24MD005095; Martinez et al., 2011; Sprague Martinez et al., 2017). The primary goals of the training were twofold: (a) to guide teams through a process of protocol development and (b) to prepare them to implement the protocols they developed. To that end, the objectives were focused on (a) group development, (b) fostering a shared understanding of health, health inequities, and the social determinants of health and inequity, (c) building a basic understanding of health assessment and data collection methods, and (d) cultivating fieldwork skills.
Roles and Responsibilities
Clear roles and responsibilities were established for both youth and adults. Youth acted primarily as lead researchers attending trainings, identifying multiple priorities of interests to examine, choosing the most appropriate research methods, collecting and analyzing qualitative and quantitative data, and also disseminating research findings. However, adult coordinators acted primarily as partners and facilitators, holding consistent meetings with the youth, coordinating logistics of meeting space and transportation for data collection, and communicating with adult research facilitators from the research team regarding any additional questions or support requested. Throughout the process of the training, adult facilitators worked to ensure that youth and adult coordinators understood and fulfilled their roles. Space was also provided for both youth and adults to process their interactions throughout the course of the training with the intention for youth participants to trust the process and to provide young people with space to lead without adult interruption.
Curricular Components
The training emphasized capacity building and empowerment and was rooted in racial justice. The curriculum began with a team-building unit had three primary threads, which focused on (a) health and health equity, (b) community systems and local assessment, and (c) changing policy rules and norms (see Figure 2). Group development was a key component of the training. Youth needed to be able to design and implement a protocol as a team. Team-building activities were used to facilitate and enhance process and phases of group development (forming, norming, storming, and performing; (Tuckman & Jensen, 1977), with the intention for the group to establish structures and a culture of leadership by which to operate. This process decreased uncertainty and facilitated relationship development and decision-making among group members.
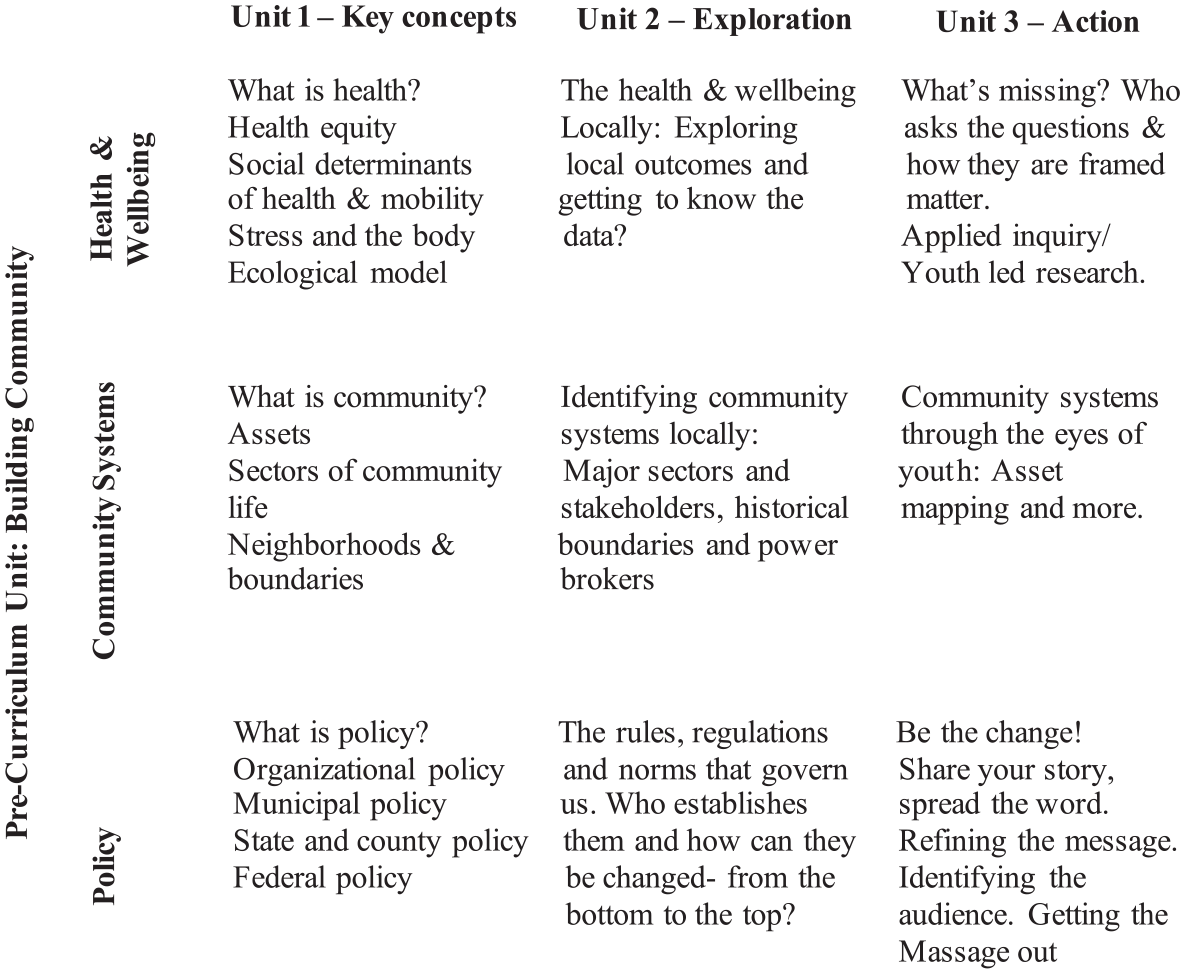
Curricular components.
The health component of the curriculum was intended to (a) provide shared understanding of health and well-being and (b) convey a multilevel framework to young people within which to conceptualize community health and well-being. In addition, the health component employed a racial equity lens for students to critically reflect on differences in health and well-being in their lives and across communities. Throughout the course of the training, young people explored health and the social determinants of health through a critical lens, examining the ways in which systems of oppression affect individual life chances and community conditions. Assessment and data collection methods were the final component of the training. This component was both theoretical and applied. In studying health, youth were introduced to the ecological model and, as such, learned about community systems and the policies that govern said systems. Through this lens, youth were able to explore health-promoting assets and the ways in which policy rules and norms have historically advantaged some communities with respect to health while systematically disadvantaging others.
A number of activities were used to communicate the training content through an empowerment approach. Interactive and hands-on activities capitalized on youth’s experiences, strengths, fostered ownership, and reinforced elements of critical pedagogy embedded within the health and assessment content and also delivered independently. Such activities included icebreakers, problem-solving, and storytelling exercises. Icebreakers were used early on during the group formation process to help team members get to know one another, whereas problem-solving exercises helped to build group norms around communication and decision-making. Recap and problem-solving exercises helped during instances of storming or group conflict, to bring the group together around common goals, as did storytelling activities. Storytelling activities also supported forming and norming processes from each group’s initial meeting. Activities employed to teach content related to health and assessment included minilectures, videos, small group and individual (written and verbal reflection) activities, and role-plays.
Training Procedures
The initial training was delivered in person at each site by a researcher–youth worker dyad over a 3- to 4-day time period. Training participants included youth as well as site adult staff coordinators. During the training, decision-making related to the focus of the assessment was led by youth, and decisions related to logistics, such as scheduling, were made collaboratively by youth and adults. Trainings began with introductions and group development activities, during which participants learned about the project background and developed group goals. For example, the Wind Blows, an interactive team-building activity, was introduced to help students get to know one another, as each youth shared their names and one characteristic that applied to themselves and others sitting in a circle. Youth got up to find other seats if the statement applied to them and youth left without a seat shared another characteristic and so forth. Adult research facilitators guided a debrief of the activity in which youth drew connections with community’s strengths and challenges when addressing health, as well as the importance of elevating youth voices through the participation of the youth-led health assessment. Group members also developed expectations during the initial introductory phase. As participants came to know one another, concepts of health and well-being were introduced. During brainstorming activities, teams reflected on the concept of health, what it means to “be healthy,” barriers to health, and the conditions that support health and well-being.
Youth then took part in a miniworkshop exploring health and the determinants of health, during which they were introduced to the ecological systems model (Bronfenbrenner, 1992; Schulz & Northridge, 2004). More specifically, youth examined their living and social environments as a multilayered ecology, with each of the layers influencing the other, and themselves influencing and being influenced by that ecology (Bronfenbrenner, 1992). Youth reflected on their own personal health and well-being and then developed ecological models outlining health risk and protective factors they experienced at the individual, peer-group, and community levels on large newsprint which was posted on the walls. As youth shared their models with the larger group, adult research facilitators recorded responses on a “team ecological model” and generated a list of health risk and protective factors, which were called “health promoting assets and threats to health.”
Participants viewed Unnatural Causes: Place Matters (Adelman, 2008), a documentary exploring the relationship between living environments and health. The documentary dissects reasons why communities in the United States look the way they do with respect to neighborhood segregation and resource deprivation. For example, the youth research teams were introduced to redlining and housing policies that created an economic detour for Black families, which continues to have implications for their health and well-being today (Adelman, 2008; Oliver & Shapiro, 2006). In small groups, youth worked to further tease out the social determinants of health for young people in their given communities. As youth research teams took turns to share factors that determined the health of youth with the larger group, adult research facilitators recorded on newsprint the list of health-promoting assets and threats to health derived from the youth brainstorm. Youth systematically revisited the list prioritizing and clarifying emergent themes. As young people explored health risk and protective factors, they were challenged to analyze the impacts of said factors varied across geographic and population-based communities.
During the training, youth also grappled with the notion of equity and explored the impact of oppression and, more specifically, racism. Teams heard the Gardener’s Tale, a short story and illustration first told by Dr. Camara Jones, a social epidemiologist (Jones, 2000). The Gardener’s Tale illustrates the levels of racism: internalized, personally mediated, and institutional. Jones (2000) presents a powerful story about how institutional racism and policies that create unequitable conditions for communities of color affect well-being and how they are reinforced by personally mediated racism and over time produce internalized racism and perpetuate components of oppressive dominant White culture.
Another activity used to help youth understand the systems of oppression was the Four I’s of Oppression. This activity involved the introduction of key concepts and role-playing. Young people were introduced to the cycle of socialization and liberation (Chmielewski et al., 2016) presenting emancipatory frameworks for youth to understand oppression, moving away from “blame,” given the lack of choice in choosing individual identities and privileges, and centering individuals instead in collective responsibility to support one another. Afterward, youth were divided into small groups to develop role-plays that illustrated ideological, institutional, interpersonal, or internalized oppression. Audience participants guessed the form of oppression. Then, that same group role-played a scene demonstrating what liberation might look like.
Next, teams were asked to brainstorm the definition of community and its meaning. Then, as a group, they began to construct parameters around the meaning of community for their health assessments. At this point in the curriculum, the notion of assets was revisited and groups reflected on community assets present in the parameters of their communities. Once listed, the group assessed barriers and/or challenges associated with the health promoting community resources they identified earlier.
To further connect the content to youth’s personal narratives, adult research facilitators guided groups through a visual storytelling activity. Each youth used drawings, words, or imagery to depict major events that have affected their lives and well-being at three levels: (a) individually, (b) family, and (c) community. After youth were allocated a few minutes to reflect, write, and create a visual narrative of major events that have affected them in large flipchart paper, each youth shared their narratives with the larger group, while adult researcher facilitators recorded emergent themes. At the end of the activity, the group explored the themes reflecting on implications for health and wellness. Youth were able to identify and discuss common health-promoting factors and threats shared in the group as well as add any major health factors that were missing. This final list was posted in large newsprint paper on the wall. Through the visual storytelling activity, youth generated a list of factors that promote and threaten their health situated in their lived experiences collectively in the multiple levels of the socioecological model (i.e., micro, mezzo, macro).
Youth, again, prioritized and clarified potential areas of health assessment based on their lists of health promoting assets and threats to health. Each young person was given a set of four stickers to vote on issues. Votes were tallied and each topic was discussed. Youth were given the opportunity to bring back items without stickers that did not make the list for discussion. After items were clarified, the process was repeated and a final list was generated. Topics were listed on newsprint around the room and youth were asked to write questions and/or a hypothesis about each item.
Groups, then, participated in a minilecture on assessment and were introduced to assessment methods. Methods included the following: audits and observation, photovoice, surveys, and interviews. Youth revisited their topics and discussed methods in which they were most interested. Adult research facilitators shared examples of the data they would be able to collect dependent on the question and methods they selected. Based on the methods youth selected, the adult researcher developed sample protocols. In the case of groups that selected surveys or interviews, sample items were drawn from youth questions and themes related to prioritized items. When possible, existing survey items were identified. Protocols were presented and reviewed by youth groups who met in small teams to discuss the protocol and provided facilitators with revisions and edits. Revised protocols were developed based on the group discussions.
Groups received training in field methods, which included a discussion of human beings’ research and research ethics. Teams created role-plays and rehearsed elevator speeches explaining the goals of their assessments. In addition, teams practiced their assessment protocols. Upon culmination of the training, protocols were submitted for exempt review status to the institutional review board (IRB) of the university at which the adult researchers were affiliated. In the case of survey, observational, and interview protocols, databases were developed in Qualtrics to allow participants to upload collected data. Photovoice data were shared electronically.
Upon approval from the IRB, site coordinators worked with youth to schedule data collection and weekly team meetings. Data collection varied by site dependent on the final protocol developed. Sites held weekly meetings with youth which the adult research facilitators joined remotely and sometimes in person. During meetings, youth provided updates on their assignments. Teams also reflected on their experiences and challenges with data collection and data entry, and they also discussed solutions. Adult research facilitators and site coordinators addressed questions and concerns related to both project logistics and field experiences. Teams collected data over a 4-week period. At the end of the data collection period, adult research facilitators returned to the sites to assist with data analysis and to discuss the dissemination planning process. Teams determined their target audience, methods, and medium to communicate findings and planned for dissemination locally and nationally. Full data reports were provided to each site to facilitate local dissemination.
Evaluation Methods
We (the adult researchers) used qualitative methods to explore program benefits associated with the YPAR curriculum. The evaluation protocol was approved by the IRB of Boston University Charles River Campus. At the onset of the project as organizational partners were identified, the goal of the health research and action program, as well as the program evaluation, were reviewed with organizational staff. Baseline interviews were conducted with adult staff at all sites (n = 7) exploring the organizational mission and goals as well as efforts underway in the area of youth-led initiatives. Similarly, during initial training sessions with youth, the role of researchers, adult partners, and youth was discussed. During this process, we shared information about the program evaluation and said that we would be studying the process of implementing the training, highlighting for both youth and adult partners that choosing not to participate in the evaluation would not affect their participation in the program. As such, youth and adults were aware that we were studying their perceptions of the research and action program implementation process as well as outcomes. As part of the evaluation program, documents, including youth products and protocols, as well as facilitator debriefs were reviewed. In addition, youth completed a brief demographic survey at baseline and an online survey at the end of the program. Adult partners were interviewed at baseline. Interview and analysis procedures are described in detail.
Youth researchers (N = 35) completed a baseline questionnaire exploring their motivations for participation as well as basic demographic information. In addition, youth (n = 15) participated in an anonymous online exit survey consisting of semistructured items exploring their perceptions of the program (what they enjoyed, what they would change, and what they would tell a friend about the program). The survey also explored what they learned during the course of the program. Adult partners from each of the five community organizations and grassroots’ leaders (n = 7) participated in baseline and exit interviews before and after the completion of the program. Each interview was audio recorded with participants’ consent, and the length ranged between 30 and 60 minutes. Interview questions examined organization or grassroots leader’s key program areas and mission, catchment area, initial motivation to participate in the program, exiting youth leadership initiatives, program expectations, and potential impacts, if any, of their own as well as the youth’s participation in the program.
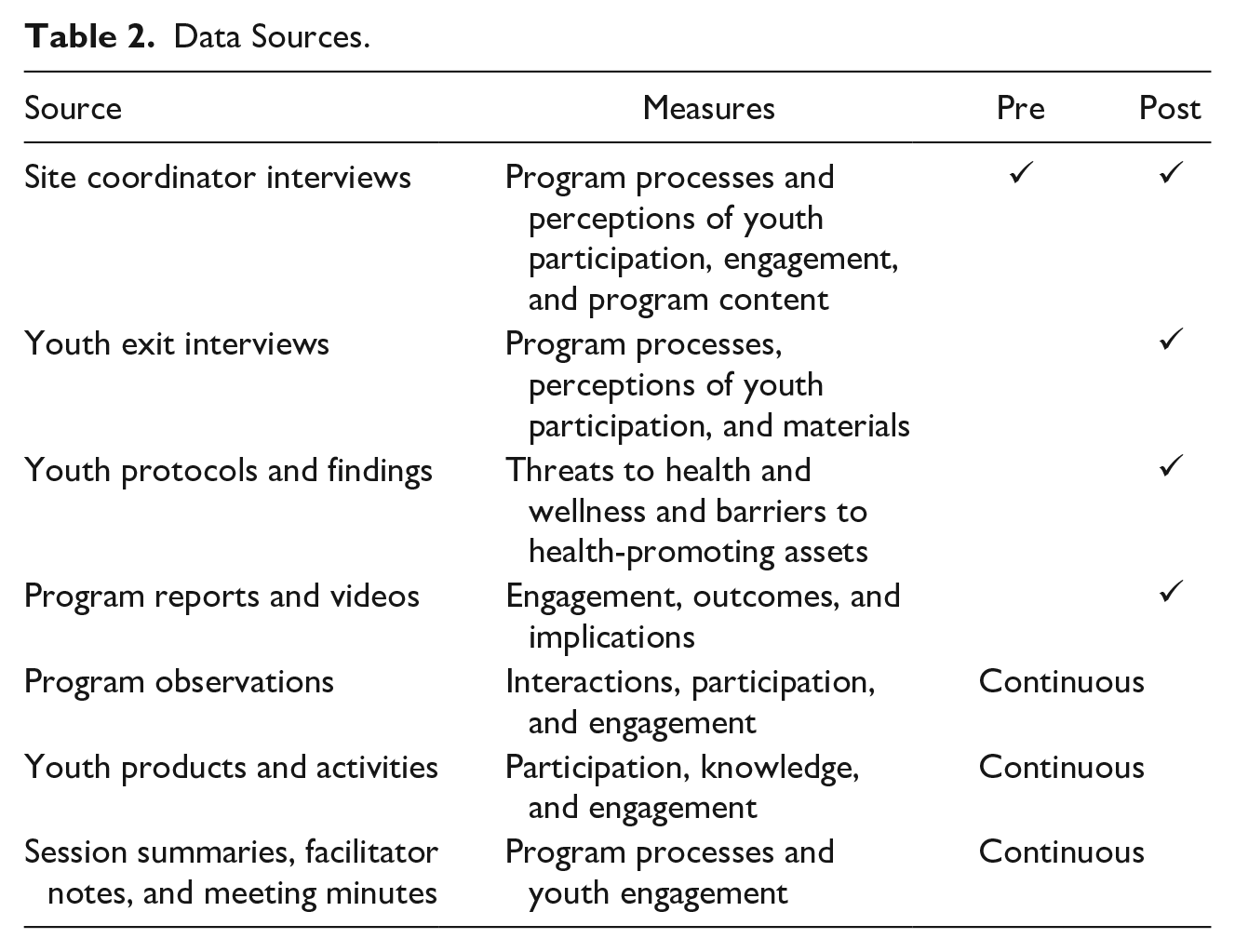
Audio recordings were transcribed by members of the research team. The investigators also took field notes and conducted observations throughout program activities. Direct content analysis (Hsieh & Shannon, 2005) was used to examine interview transcripts as well as program materials such as meeting summaries and notes, facilitator notes, youth research protocols, and youth participant reflections. The adult investigators deductively coded materials as well as key informant interview transcripts for the existence of themes related to key terms drawn from major theoretical frameworks informing the research in the context of health development: critical pedagogy and race theory (e.g., empowerment, capacity building and community engagement, skill development). Investigators identified and categorized themes that emerged. Then, the investigators met several times to clarify any questions and reach agreement on coding discrepancies. After data collection and analysis was completed, the team selected a final set of illustrative quotes relevant to adult staff’s perceptions of benefits of the program. Table 2 provides a summary of data sources used to inform our exploration of the benefits of the curriculum.
Data Sources.
Results
As was anticipated, three primary themes emerged as the result of this work. First, young people began to think differently about health, what it means to be healthy, and the factors that influence health. Second, both young people and adults reported gaining important career readiness skills and research-related knowledge. Third, the acquisition of skills for some contributed to feelings of empowerment.
Rethinking Health
At the onset of the training, when we asked young people about health, they talked about health behaviors such as “healthy eating” and getting exercise. Over the course of the training, however, their conceptualization of health shifted as they began to think critically about health ecologically and the relationship between health and social conditions. One youth researcher from Philadelphia stated the following: Before I joined this project I just thought wellness was about being in shape and eating right. I never thought about how all of these outside contributors had anything to do with wellness. But now my definition of wellness has changed because I realize that it’s way more than that. I feel as though everything that happens around us makes us a product of our environment. (Youth researcher, Philadelphia)
After participating in the program, youth conceptualized barriers to health in the context of broader social determinants of health as opposed to focusing on individual-level factors. This shift is also reflected in the research protocols developed by the young people. Teams across the five cities identified interactions with the police (relationships between police and young people) as a risk factor for health. These themes are very different from the individual-level (behavioral) health risk factors identified by youth at the onset of the training.
Youth protocols demonstrated a critical understanding of the complex interactions between individuals and their environments and the ways in which systems of oppression influence both their environments and interactions. Figure 3 presents the barriers to health and well-being identified and investigated by youth across the five sites. Health conditions identified by teams included stress, mental health, personal safety, sexual health, and substance use. At the peer groups and family, or network level, important factors influencing health and well-being included personal safety, peer pressure, social media, drug use by family members, stereotypes, and racism. At the neighborhood and broader community level, factors influencing health and well-being included violence, police relations, mass incarceration, gentrification, inadequate education and transportation, unemployment, unhealthy food environments, and inadequate access to transportation. Youth also discussed postincarceration policies, such as loss of voting rights, and restrictions on access to housing, employment, and higher education as detrimental to health and well-being.

Barriers to health and well-being.
After the training, youth from each of the five sites talked about the importance of learning about “our history.” All youth across the five sites, with the exception of youth in St. Paul, shared not knowing about redlining and the ways in which policies after World War II contributed to present-day conditions. They described not having the language or the historical context to make sense of their experiences in the community, which can lead them to internalize what they are experiencing or to boil it down to individual processes as opposed to linking it to broader societal structures. Relevant historical and structural key understandings also provided opportunities for youth to further examine their individual and racial identities in their neighborhoods. Once they had a historical understanding of social problems and community context, it was easier for them to critically reflect on their lived experiences and the lived experiences of families, friends, and communities.
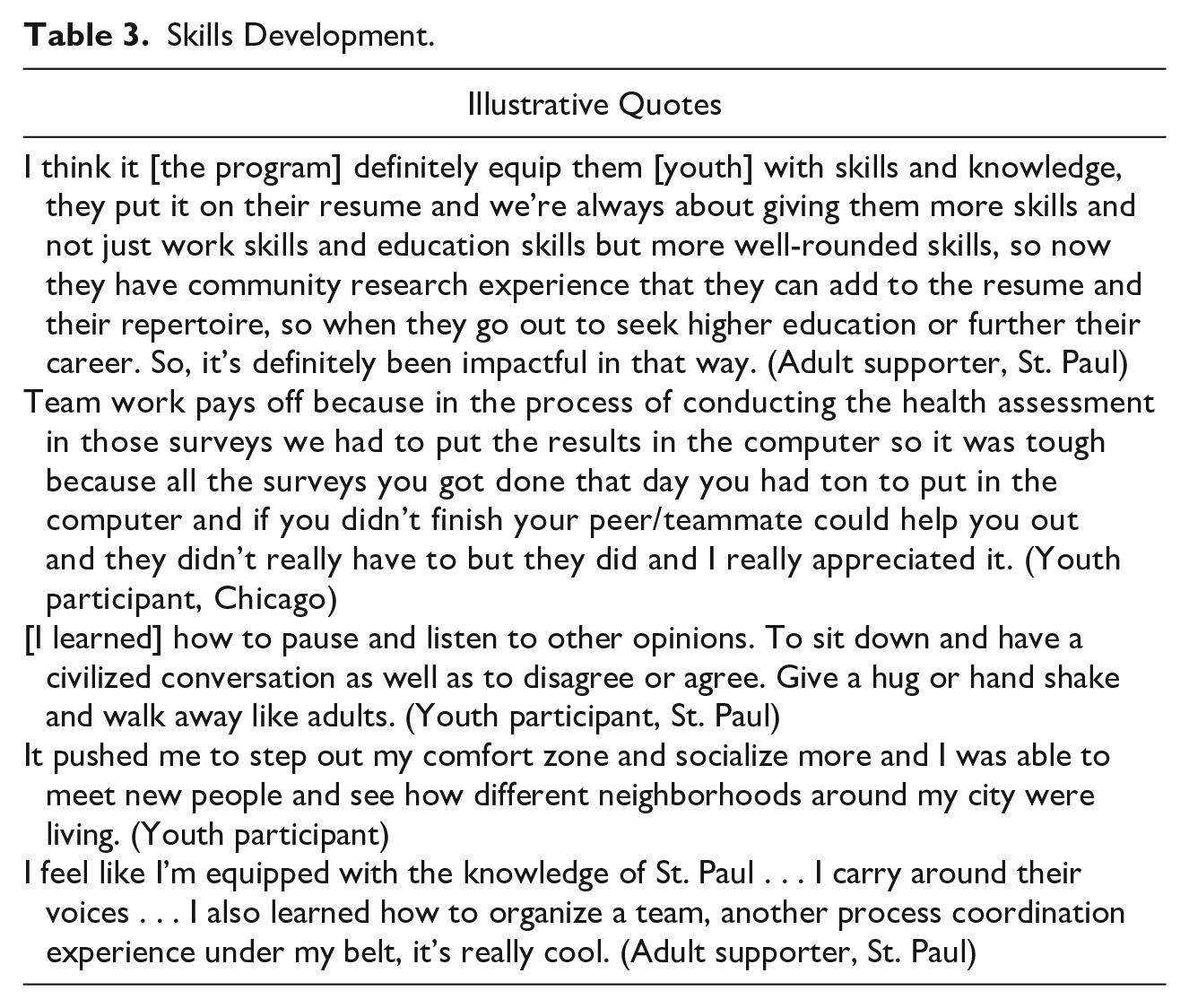
Skills Development and Knowledge
Across all sites, youth and adults described developing new skills, which increased their competence and influenced their personal, professional, and organizational growth. Skills illustrated in Table 3 included research skills, public speaking, and teamwork. In alignment with scholarly literature, this list includes social-emotional learning, (cognitive creativity, critical thinking, and problem-solving), interpersonal (communication, teamwork, leadership), and intrapersonal (persistence, self-efficacy and time management) skills relevant to academic success and the transition of youth into adulthood in the new social and economic contexts of the 21st century (Kay & Greenhill, 2011; Taylor & Kilgus, 2014; Trilling & Fadel, 2010). Meanwhile, youth gained health-related knowledge and a greater understanding of their communities. Youth also reported building meaningful relationships, in addition to learning to collaborate and communicate effectively.
Skills Development.
Empowerment
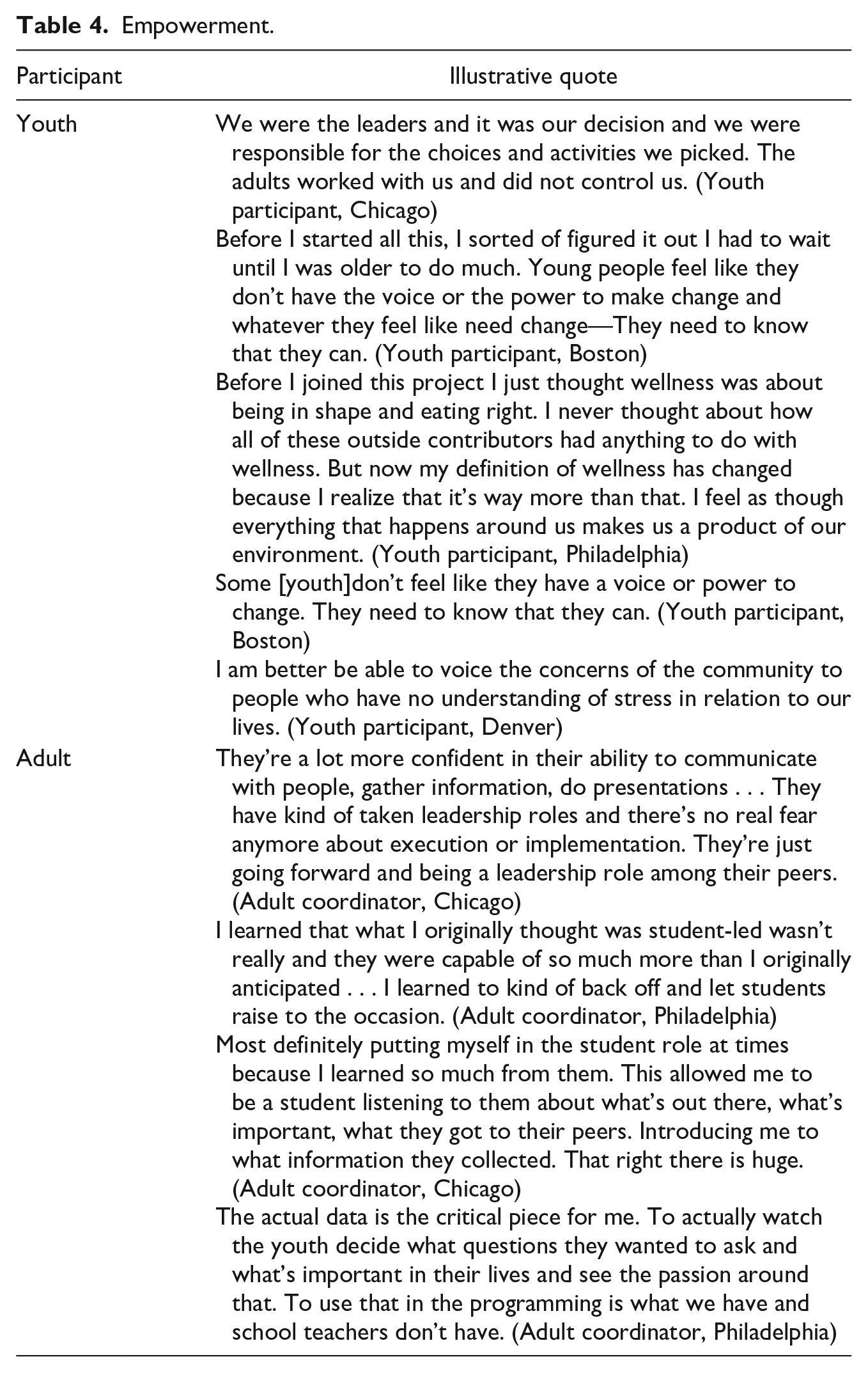
Youth felt an increased sense of agency and ownership over the project, while adults learned to act as allies for the youth by sharing power and promoting youth-led initiatives throughout the research. Youth spoke about the freedom of choice, agency, and responsibility contributing to their feelings of ownership, empowerment, and confidence. Adults, meanwhile, reported feeling more confident in youth and their ability to lead. Teaching and learning became bidirectional where adult educators were also students learning from the youth. These themes are illustrated in Table 4.
Empowerment.
Discussion
As a result of engaging youth in health research and action through a curriculum steeped in racial equity and critical pedagogy, young people began to think about health much more structurally beyond individual dimensions. Youth conceptualized health initially from the perspective of individual preventive habits such as “exercising more, drinking less . . .” and later evolved to a more complex and nuanced perspective integrating a structural and systemic approach when thinking about what factors determine the health of their communities. Furthermore, youth felt empowered to take initiative and generate social change beyond the research program. This finding is consistent with the social justice service-learning literature that highlights how a critical approach to engaging urban youth of color increases their awareness of broader structure issues, provides space for healing, and sparks community action.
This finding is of particular importance in the area of health, where education models are often focused on individual behavior. We found that working in the context of youth’s lived experience to introduce concepts related to health and health equity, as well as explicitly naming racism (structural, interpersonal, and internalized), provided a space for them to think differently about health, what it means to be “healthy,” and health advantages afforded to some based on race. Initially, youth thought major constraints to health and well-being consisted solely of individual behaviors, while neglecting broader external ecological factors. Exposing youth to the social ecological framework and the impact of White supremacy producing inequitable outcomes facilitated the conditions for youth to reflect on the living environment and individual health behavior and gain a deeper understanding of their own lived experiences at the intersection of racial identities, social location, and counter-narratives. Moreover, youth appreciated learning about the historical context contributing to present-day neighborhood conditions and characteristics. It is easy for young people, and adults alike, to internalize oppression if they are unaware of the ways in which racialized oppressive social policies established and continue to sustain racial inequity.
By grappling with individual and structural health priorities in relation to personal lived experiences, youth engaged in developing a critical dimension of consciousness that positioned them as agents of change. Freire’s (1970) critical consciousness or conscientization conceives individuals not just merely existing in the world objectively, but rather existing with the world with others with the capacity to transform the world’s reality in relation to their lived experiences. Throughout the training curriculum and research processes, youths’ personal lived experiences were considered key domains of knowledge in relation to the health threats identified individually and structurally. Youth not only understood their lived experiences in the context of health individually and structurally but also felt deeply motivated to generate change in the community. While previous youth development models have not explored thoroughly critical forces that affect the lives of urban youth (Ginwright & Cammarota, 2002), social justice youth development models are expanding youth critical consciousness through pedagogy and education (Cammarota, 2011). This YPAR youth and adult training model presents an alternative strategy to engage youth as key leaders and change agents in public health efforts, while recognizing their unique value and experiences.
Both youth and adults described the need for more spaces for young people to participate in meaningful ways in the community. Beyond competency building and skill development, youth and adult participants expressed interest in having increased spaces to be involved in both critical reflection and decision-making processes that affect their lives, their loved ones, and their communities. From prioritizing items that threaten young people’s health in their communities to choosing their methods and dissemination strategies, young people developed ownership by participating in meaningful ways throughout the youth-led health assessment. Instead of being perceived as passive recipients of services, youth and adult participants demonstrated the value and the positive impact of working with youth when they are seen as a resource. Adults chose to trust young people and cocreate environments that engage, support, and empower young people to reach their potential.
Although the benefits of models that engage youth using critical pedagogy, building on the assets and capabilities they bring, have been well documented, they are only recently gaining momentum in public health research. YPAR has led to this increased momentum but has not consistently demonstrated a focus engaging youth in a process of examining the racial hierarchy and/or creating space for young people to grapple with and heal from the deleterious impacts of White supremacy culture. Sprague Martinez et al. (2017) found that engaging young people in an afterschool research and action service-learning program focusing on health equity and the social determinants of health increased youth perceptions of their ability to make change in the community and also increased their understanding of an interest in local health initiatives. This work further contributes by providing a successful strategy for engaging youth of color in health research and action.
Of note, this work is not without limitations. The program was advertised as a work opportunity for youth interested in health research. This poses selection bias, which is enhanced, given there is no baseline youth data exploring motivations for program participation. It may be that youth in the program were already highly interested in health. In addition, we did not collect baseline data related to youth attitudes or conceptualizations of health or measures of empowerment. In this respect, significant bias is introduced in the fact that we draw heavily on facilitator and adult supporter observations. Moreover, it is likely that participant who enjoyed the program were more likely to complete the exit interview and to report positive skills and empowerment gains, regardless of their actual improvements. It will be important for future studies to explore more explicitly the extent to which the program is seen a beneficial for a wider range of youth. In addition, all teams received the same curriculum, and future studies might also explore the benefits of this curriculum compared with other models of engaging youth in the area of health. Moreover, we explore the benefits of the curriculum relying on data collected during and immediately following its implementation. It is also unclear if the benefits described will have long-terms effects. Furthermore, a larger representative sample of youth participants and cities could be incorporated in future research. Despite the limitations described, this article provides an illustrative example of the development of a YPAR training curriculum steeped in critical youth empowerment and critical race theory designed to engage youth in community health research.
Conclusion
With the proliferation of YPAR and CPAR approaches to development, it is more important than ever that researchers and practitioners understand how to create curriculum that will authentically engage and benefit youth of color. Consistent with previous studies, we found that involving youth in relevant decision-making processes generates positive outcomes. By incorporating the diverse experiences of youth of color through a critical youth empowerment and critical race theory, youth were empowered to not only identify health threats that are relevant to their lives but also to examine the relationship of these with their own experiences in order to enact change. When given an opportunity, appropriate resources, and space to lead, we found youth to be insightful, resourceful, compassionate, and deeply committed to improving the lives of their peers, family members, and communities. This work highlights an approach to engaging youth of color in youth-led health assessments through a critical youth empowerment framework steeped in critical race theory.
Footnotes
Acknowledgements
This research was conducted for America’s Promise Alliance and sponsored by Target. The content is solely the responsibility of the authors and does not necessarily represent the official views of Target and/or America’s Promise Alliance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.S.M., PhD, is a research consultant for America’s Promise Alliance (APA) and CCI Health and Wellness. For APA, she provides technical assistance for the Healthy Schools Initiative, and for CCI, she is an evaluator for a pediatric obesity intervention.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.