
Abstract
This paper focuses on how divergent but interlinked knowledge cultures shape veterinary professionals’ practices. Embodied sensory and emotional knowing, and local and contextual knowledge, often incorporated within cultural scripts and conventions, constitute the paper's focus. Drawing upon biographic narrative interviews, we demonstrate that these different forms of knowing are enmeshed with scientific knowledge and embedded in veterinarian's interactions and work practices, influencing diagnosis, treatment and other interventions. Here, ‘knowing’ is understood as knowledge cultures that influence communication and professional practice, while transgressing boundaries between tacit and explicit, lay and scientific knowledge. We argue that these disparate yet convergent forms of knowing deepen our understanding of the multidimensionality of veterinary practice and are important for the education and training of veterinarians, their knowledge and expertise claims. We hereby expand sociological discussions of the labyrinthine character of veterinarian's knowledge, highlighting the complex, diverse ways that it intersects with science.
Introduction
Veterinary knowledge isn’t one or the other … It's science, but to do with people and working with animals, talking to the owner, finding out what s/he is about, making the diagnosis … running through options… what's best for the animal. You’re dealing with a lot of knowledge in one go (Paul, 44, small-scale mixed veterinary practice, England).
This paper is divided into five main sections and subsequent subsections. The first section grounds our research in extant literature in the sociology of knowledge and knowing, linking this to veterinary research. The second section outlines the study's methodology before discussing the principal findings, which focus on how different knowledge cultures are understood and operationalised within veterinary practice, challenging knowledge dichotomies. The fourth section discusses the intersectionality and the multidimensionality of these, with the fifth section embedding our findings within wider relevant research and then discussing their relevance for veterinary practice, education and research.
Knowledge, knowing and knowledge cultures
In recent decades, the complexity of veterinarians’ knowledge, interactions, work and communication skills has been accorded greater attention in sociology, human geography and the veterinary sciences (Donald, 2019; Everitt et al., 2013; Sanders, 2010). Research interest increased, partly due to numerous food scandals, which further underlined veterinarians’ importance in biosecurity and the surveillance and eradication of animal diseases. The growing emphasis on animals in the social sciences – the ‘animal turn’, human-animal entanglements in the Anthropocene, common worlds perspectives and multispecies justice (Tschakert, 2020), that reconceptualise human relations with ‘more than human’ others, further precipitated this research interest.
Traditionally, knowledge was often conceptualised as a predominantly dichotomous entity; tacit or explicit, scientific, or lay, although the Sociology of Scientific Knowledge (SSK) and Kuhn's The Structure of Scientific Revolutions (1970) challenged this (Knorr Cetina, 2007; Rommetveit and Wynne, 2017). Tacit knowledge is usually defined as practical, emotional, or cultural knowledge that perpetually resists verbalisation and codification, while explicit knowledge is allied with science and is therefore readily codified and accepted as independent, objective and replicable (Nonaka and Takeuchi, 1995; Seghroucheni et al., 2025). Although definitions of ‘local’ and ‘folk’ knowledge exist, they are sometimes used interchangeably with ‘lay’ knowledge, with all three being viewed as tacit, non-scientific and context dependent (Natarajan and Evrard, 2026). Tacit, lay, folk, and local knowledge therefore all describe understanding rooted in experience rather than formal codification, but they differ in scope and transmission. Tacit knowledge is deeply personal, hard to articulate, and gained through practice (Polanyi, 1966), whereas lay knowledge refers to non-expert understandings held by the general public, often shaped by everyday experience (Williams and Popay, 2006). Folk knowledge overlaps with lay knowledge but is more culturally embedded, passed through traditions, beliefs, and collective memory, while local knowledge is context-specific, tied to particular places and communities, often seen in indigenous or rural settings (Geertz, 1983). These distinctions highlight how knowledge varies in terms of articulation, transferability and cultural grounding.
Although some sociological literature illuminates intersections in knowledge types (Erden et al., 2008), these dichotomies promoted strict hierarchies: that science was strictly separate and a fundamentally more advanced knowledge than lay, tacit or folk knowledge. Scholars also further classified scientific knowledge into ‘hard’ and ‘soft’ categories (Pollock, 2009) where ‘hard’ knowledge is easily codified and falsifiable (e.g., algorithms in mathematics and physics equations), and is therefore perceived as embodying greater expertise and objectivity than so-called ‘soft science’ (e.g., social sciences). Numerous SSK studies critique ‘hard’ and ‘soft’ categorisations due to science's inability to solve or predict global ecological disasters and humanitarian crises like the Chernobyl nuclear power explosion, famines, earthquakes and COVID-19 (Zapp, 2022). Despite this, dichotomous understandings prevail but necessitate critical scrutiny when applied to veterinarians’ knowledge and the social fabric of veterinary clinics.
These knowledge demarcations potentially devalue the complexity of veterinarian's knowledge and its application, which manifests both scientific training and complex insights learned in practice (Clarke and Knights, 2018). While vets accumulate ‘hard’ knowledge through professional training in laboratories, lecture halls and operating theatres, they gain tacit knowledge of cultural conventions, farming practices, animal diseases and client behaviours in practice (Garforth et al., 2013). Significantly, veterinarians are knowledge conduits about new treatments for pet owners, emerging technologies for improved farm productivity, and innovations in genetics and bloodlines for specialist equine breeders. They act as ‘knowledge brokers’ and intermediaries between industries (e.g., equine, bovine), government departments, their employers, abattoirs and farmers, often acting as scientific knowledge deciphers for farmers (Boden et al., 2015; Fisher, 2013). Veterinarians’ positionalities in relation to science, lay knowledge and expertise are therefore complex and multi-tentacled, pertaining to official standards for animal welfare, sound moral judgment, economic rationalism, professionalism towards human clients and accumulated experiential knowledge about animal health.
Despite recent emphases on veterinarians’ unique skill sets in the social scientific (Hamilton, 2013) and veterinary sciences literatures (Belshaw et al., 2020), communications skills in veterinary curriculums (Englar et al., 2016; Kurtz, 2006) and the complexity of veterinary consultations (Everitt et al., 2013; Klingborg and Klingborg, 2007), non-scientific knowledge cultures (e.g., tacit, lay, folk) have largely been overlooked. Furthermore, the knowledge claims of vets, including how they understand and may interpret their own knowledge as lay, tacit, folk and/or scientific, their relationships with clients and their social statuses as experts, is similarly underexplored. This paper addresses this gap, exploring four different veterinary knowledges: local, contextual, sensory, and emotional – showing that they are often combined with ‘scientific’ knowledge which frequently cannot be successfully applied in isolation, devoid of alternative knowledges.
The intersectionality and complexity of knowledge in veterinary practice
Scientific knowledge is assumed to be the prima facie knowledge vets depend on for their professional identities and claims to expertise. Still, it is how that knowledge is understood and practically applied, in combination with other knowledge forms that is investigated here. Veterinary science is factual and shares similarities with human medicine. However, the various steps, encompassed in the Calgary-Cambridge model, which are much utilised as the contextual frame par excellence for veterinary and human medical consultations (Englar et al., 2016; Radford et al., 2006), are not inherently linear as previously assumed (Kinnison et al. 2016; Russell et al., 2022). Furthermore, veterinary science is debatably more complex and multifaceted than human medicine. It involves multiple species in terms of reproduction, health, illness and euthanasia, as well as food safety and disease transmission. It incorporates many different settings - not just the laboratory, hospital and clinic, but open land spaces as in large-animal veterinary, stables in equine, zoos which house exotic species, non-land spaces, like the sea, regarding water dwelling species like fish and dolphins, aquariums, and abattoirs where animals are killed, largely for human consumption. It is also shaped in complex ways by differential cultural valuations of certain species and issues around ownership, power and money (Desmond, 2022).
In human medicine, diagnosis and treatment is largely supported by language, mutual understanding and willingness to undergo uncomfortable situations, knowing these may help diagnosis or improve outcomes. Animals cannot speak for themselves and describe their pain levels or indicate where the problem resides. They cannot pinpoint possible causes (a road traffic accident or ingesting poison), or understand that constraining or painful situations (being forcibly restrained for examination) may be necessary for diagnosis or treatment. Animals’ sensory, cognitive and physical structures and functions differ vastly from ours and each other's. Furthermore, there is limited veterinary knowledge of these for many species, and limited awareness of how animals experience pain, and how to detect this, many disguising pains for fear of becoming others’ prey (Desmond (2022, p. 8).
This complex situation is also exposed by the triadic ‘dance’ of diagnosis and communication that normatively, (excepting ownerless animals), takes place between the animal, the human owner and the veterinarian (Hobson-West and Jutel, 2020). In these situations, vets may have their expertise or knowledge contested by owners or other veterinarians. Furthermore knowledge, skills, technology and instruments often extrapolated from human to veterinary medicine may not always assume such a good fit. Desmond (2022) provides a memorable example of a small lizard that veterinary technicians exerted much effort trying to position and tape down under two large X ray machines (one designed for horses!) and unsuccessful repeated attempts by a vet to measure the heartbeat of a snake and take blood samples.
Overall, the key message emanating from this short analysis of relevant literature is that veterinary practice is a messy, uncertain, complex and contested affair, during which many types of different knowledge about diverse species, different settings, ethical conundrums, financial and ownership issues, and human behaviour, communication and emotions, as well as animal behaviour and emotional states, come into play.
We therefore aim to broaden understandings of traditional scientific veterinary knowledge to incorporate how scientific knowledge is routinely interspersed with other knowledges. Tacit, experiential knowledge threads through these knowledge forms, thus showing interchange and confluence in scientific knowledge of vets and ‘practical consciousness’ (Giddens, 1985) learned everyday ‘on the job’. We begin with describing and giving examples of local knowledge (K1) 1 followed by contextual (K2), emotional (K3) and then sensory knowledge (K4). The section on contextual knowledge (K2) is more detailed than the others because it can often accommodate the other knowledge forms (K1, K3, K4). These knowledge forms, although distinct in some ways, are intricately connected and it is these connections that form the backbone of our analysis. Following this, we show how interconnected these subjugated knowledge forms are with scientific knowledge, thereby illuminating the intersectionality of veterinary knowledge. Furthermore, we introduce concepts of deep and shallow knowing, and spectrums of knowing, to demonstrate how in different contexts vets possess fluctuating levels of knowledge in relation to these multifaceted knowledge types.
Methodology
This paper forms part of a larger-scale qualitative study of veterinary professionals and animal owners conducted in Ireland and the UK from 2019 to 2021. All names used are pseudonyms and all data referred to is anonymised so participants cannot be identified through their roles or specific settings. We used the Biographic Narrative Interpretive Method (BNIM) (Wengraf, 2001) to trace interviewees’ emotional connections, their work practices and relations with animals since they were children. About 30 veterinarians across Ireland and the UK were interviewed and it is these interviews we cite and draw from. Guest et al. (2006) found that saturation often occurs within 12 interviews, basic themes often manifesting by six interviews, although others suggest 10–30 interviews are necessary for many qualitative studies, depending on complexity and diversity of sample (Saunders et al., 2018). At around thirty interviews, we hit data saturation where no new themes or codes emerged from the data. Information on study participants is outlined in Fig 1.
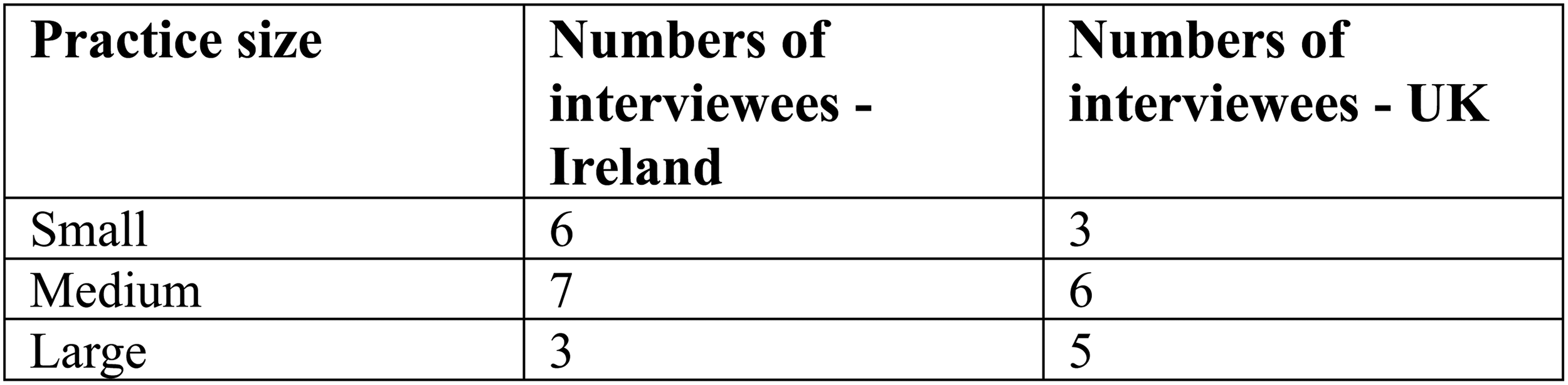
Profile of interviewees and practice size.
We subjected our data to rigorous analysis in terms of major themes relating to different knowledge cultures via Braun and Clarke's (2006) thematic analysis method. Using purposive sampling, we recruited veterinarians of different ages and genders, with varying experiences, to examine confluences and convergences in experience, knowledge and attitudes. They were working in different settings (from small-scale rural clinics, large-scale commercial clinics in urban areas, specialist equine, medium-sized rural practices through to zoos and charitable animal welfare organisations), across the UK and Ireland. Many veterinarians also had previous experience of working in different settings from the one they currently worked in, and with different groups of animals. They therefore reflected on differences in relationships and work at different stages of their careers. The analysis revealed some particularities in knowledge across different settings (e.g., rural versus urban clinics), whilst also revealing overlaps.
Local knowing in veterinarians’ everyday lives
This type of knowledge, which we categorised as local knowing (K1) emerged strongly in datasets. It emanates mainly from deeply understanding a culture, its history, conventions, customs, people and their priorities, due to immersion in specific places and their peoples. It involves an understanding of language, how vets position and perceive animals, and their owners, an appreciation of the geography and economics of an area, as well as farming traditions and cultural conventions. This knowledge appears more relevant to veterinary practice in rural farming communities and within equine communities, rather than companion animal practices in urban areas. I’ve been around horses all my life. If you approach the horse on the wrong side, and say, “its right leg,” instead of “its off fore” or “near fore.” If you don’t use the right terminology, you’re not given a chance. Mark had the same training as I but doesn’t have the common-sense knowledge of being around horses, so clients don’t trust him… (Jan, 43, large mixed animal practice, England) You understand how things are done… The fellow who knows his own cattle and the markings, bloodlines… You understand the farmer (Tim, 56, small mixed animal practice, Ireland). After vet school I saw this farmer had holly tied in the shed's rafters. He said the spores dried up disease. The vet that I was with said ‘Leave him. He saw his own father doing it, and we need his business. Don’t challenge him.’ (Philip, aged 46, small mixed animal clinic, Ireland).
Irish vets in farming communities deployed cultural scripts around ‘the good farmer’ to strengthen farmer buy-in to treatments and animal disease prevention programmes. Meanings of ‘the good farmer’, however, vary contextually (Sutherland and Calo, 2020), from those who effectively adopt techno-scientific innovations (Leitschuh et al., 2022) to preserving traditional farming practices or mixing them with technological advancements (Enticott, 2023). However, uptake by farmers often depended on their perceived effectiveness amongst elite farmers, whose husbandry practices were well regarded locally: He wants to take the cheaper option. If I remind him that Tom down the road did things differently and Tom's animals are all shiny and healthy, he’ll take the better option (John, 53, small mixed animal practice, Ireland) They don’t want to go to the mart and have the worst looking cattle, and people looking down on them (Malcolm, 55, medium mixed animal practice, Ireland). Him and the wife sit down. They want to know who gets the best prices, whose cattle looked the best, whose sheep did the best. They want to know who to aspire to (Martin, 64, small mixed practice, Ireland). We need the business. If it means telling the young vets to sit with them for a while, I will do it (Bob, small mixed practice owner, Ireland). In the first practice many people couldn’t afford things you might suggest, so just trying your best with limits … In the second practice, clients had lots of money and were insured … The medicine they expected was different, they wanted all the investigations (Suzanne, 32, medium mixed animal practice, UK) There they were around horses and had huge knowledge. Here, the pony might be taken in once a year and taken to the show, but they are not handling the animal every day. Simple things like changing a horse's bandage they won’t know. They wouldn’t understand if I said the mare needed a wash out, so I explain what happens internally (Marie, 56, medium mixed practice, Ireland).
Contextual knowledge
This is a more amorphous knowledge type (K2) that is wider than local knowing, whilst also incorporating it. Contextual knowledge (K2) involves many facets; the veterinarian's direct employment and organisational context; national or regional policies and veterinary-specific regulatory frameworks; the expectations of specific human clients; the general behaviours and settings of their animals, as well as the norms/functioning of the community. Contextual knowledge (K2) therefore can span from knowing the human/animal clients historically and within the immediate situation, to vets’ and clients’ embeddedness in the wider community and the vet's specific position, clinic ethos and wider economic and professional associations. Even national societal norms relating to animal treatments and humans form part of contextual knowledge. In the prior examples relating to the good farmer, vets utilise knowledge of the local context and individual clients. With wider contextual knowledge, they also factor in broader economic and regulatory frameworks, their own practices and priorities, and relationalities to history and place.
The use of scripts or proverbs was evident in small animal practices, as well as farming communities, although the content was different, with these scripts becoming almost automatic and more intuitive the more experienced the vets were with both animals and the community. The knowledge imbued in these scripts, although contextual in relation to clinics, incorporated scientific, emotional, local and sensory knowledge, regulation, and technical training, thereby blurring knowledge-related boundaries.
These scripts emanated from university, regulations, client management, and how to perform critical tasks including euthanasia. Comparable to Benner's (2004) ‘novice to expert’ theory, veterinarian's learning progressed through distinct stages: novice, advanced beginner, competent, proficient and expert. The latter status of ‘expert’ was attained not at graduation but often, later in one's career, when vets were recognised by clients and peers alike as having high-level technical knowledge and personal knowledge of how to deal effectively with clients, manage their practices, and negotiate different social situations. While vets commented they initially rote learnt the steps for different procedures, like euthanasia, they later adapted the script in a way that worked for them, their situations and specific veterinary practices, applying their own contextual knowledge. When I call owners, I write down the main points. I follow a script in consulting, that I’ve adapted myself and we’re advised that you follow the same routine with consultations so that you don’t forget anything (Katya, 26, small-animal practice, Wales). In Uni we were taught a general consult … with closed and open-ended questions … If the cat is going to be put to sleep, I ask what happened … if they want the cat put down today and be present. Then I ask if they have been with a pet that's been put to sleep before. Then I explain what will happen …that it's one injection, the cat won’t feel pain just woozy …Their eyes won’t close, they might lose bladder control… (Sarah, 43, small-animal practice, England). It's a case of saying, ‘I’ve seen this before and this happened’. Sometimes they don’t want to change but the animal would do better if they did. A story of someone changing and the animal is in better form doesn’t insult them (Fergus, 50, small-animal practice, Ireland) A zoo animal, treatment must fit in with the animal's nature, and it may go back to its natural environment and breed. You don’t approach a giraffe because it will kill you. You observe and listen to what the ranger is telling you, and then anything invasive is done remotely via anaesthesia, sedation and darting guns … (Kevin, 40, Zoo Vet, Ireland).
Profit-making and contextual knowledge
With farming, animals were economic commodities and were generally not kept longer than their financial viability. While vets were generally empathetic towards animals, some sympathised with farmers’ economic situations, even where they had an affinity with a certain animal. One cow liked human company. She would follow you everywhere, licking you. I went back one year and when I asked where she was, the farmer said she hadn’t calved that year, so he’d sent her for slaughter (Keith, 55, large-scale mixed practice, UK). We can do X, Y or Z but farmers will always want to know the cost because that animal is only worth that amount (Simone, 30, medium-sized, mixed practice, Ireland). Elderly clients have traditional cattle breeds. They won’t be called 7174. They’ll say, ‘Snowy, the shorthorn’. They’ll talk to them like cats and dogs (Mike, 55, small-scale rural practice, Ireland). We were pushed to sell flea treatment to owners who had indoor pets. Someone could possibly come into their house with another pet who had fleas, or bring something in on their shoes or clothes, but it was a fine line as to whether they needed that product (George, 35, large-scale, small animal practice, Ireland). The owner made us treat every animal that came in, even when that animal would have been better referred on to specialist facilities. Moneymaking was not why I became a vet (Laura, 34, charitable organisation, UK). That older farmer had a problem with scour, and I told him to vaccinate the cows that hadn’t calved yet to protect the young ones …. It improved a lot. This younger farmer, he's dismissive because I’m a girl … I told him to vaccinate his cows, and he was like ‘you’re going to say that to sell vaccines’ (Grace, 26, medium-sized mixed animal practice, Ireland).
Emotional knowing
Emotional knowing (K3) involves self-knowledge of the veterinarians’ own emotions, and their knowledge of and responses to human clients’ emotions, which profoundly influences veterinary practice. Emotions are created and expressed within social contexts, framed by wider understandings about what emotions are acceptable and accepted in relation to different human–animal relationships. Given that most interviewees revealed an affinity for animals and a commitment to their welfare since childhood, we expected them to express distress when euthanising animals, or encountering their ill treatment or neglect, and to understand human clients’ distress when cherished companion animals were euthanised. There were, however, differential responses to how they dealt with this according to the context, experience and individual personalities. The first quote interestingly also exemplifies the interaction and enmeshment of medical scientific knowledge (euthanasia) with technical knowledge (constructing a casket) and emotional understanding and empathy (emotional knowledge). She came to us to have her old dog euthanised and just out of the blue asked me if I could make a casket. I’m an amateur carpenter and good at orthopaedics, which is mainly screws and stuff, so I knocked one up. It made me think though, this is a retired nun and only has one brother in the whole world, no family- this dog means an enormous amount to her [and] maybe I’m not paying enough attention to this stuff (Fergus, 60, small-animal practice, Ireland). This dog had been his daughter's who was killed in an accident so putting that dog down was devastating (Asha, 43, small animal practice, England). I didn’t need to tell him the result, my face said it all. We went to the shed in silence, and the animals went in the lorry in silence. The bank were on top of him and at the market there was silence (Martin, 64, small mixed practice, Ireland). I put this cow down, around twenty years old and it was like a dog to her. She could have got a few bobs at the factory, but she wouldn’t. She said, ‘she's been here this long, she's not going anywhere’ (Tim, 56, small mixed animal practice, Ireland).
How different vets respond to this knowledge about human clients’ emotions was, however, entwined with both the context and the vet's own personality and how s/he had (successfully) dealt with emotionally charged situations in the past. This involved both respectful silence and/or witnessing and affirming the clients’ (conflicting) feelings, including guilt, grief, loss and anger when euthanasia was necessary. There's no need to say anything after euthanasia. They’ve made their minds up and need to grieve (Martin, 64, small mixed practice, Ireland). If we know them, we say ‘go home and pay later’. With other people, we say it would be less stressful to pay first, and they can go out the back door rather than through the waiting room (Jan, 43, large mixed animal practice, England). He was a brilliant surgeon, but insensitive. People would come to euthanise their dogs, and he was like ‘what's wrong with you’?’ We lost clients (Martin, 64, small mixed practice, Ireland).
Emotions and uncertainty
Some newly trained vets discussed their own distress during early experiences of euthanasia, trying different treatments (unsuccessfully) and feeling mistrusted by clients due to their perceived inexperience. Many reported going home upset, some even suffering from insomnia, because they were unsure whether they had done the right thing. I drove home crying because I didn’t know if I’d done enough with a cat, and I was worrying about whether I should have tried something else (Katie, 26, small animal clinic, England). If it's a young healthy animal such as a working dog that hasn’t worked out as such, for a farmer, I try and get them to sign over the dog to me, and I try and find a home for it. Most do, because they don’t have pay a fee for putting it down (Mark, 50, medium mixed practice, Ireland) There are worse things than putting an animal down. Most of the shelters are full of unwanted animals and if that animal gets passed from pillar to post and then dies or gets put down, it's kinder to do it then and there (Susan, 43, small mixed practice, England) I had an idea of what being a vet was but …it's a business. When you bring your dog to the vet, it's like eating in a restaurant …. It's mental out back but you’re getting a smiley face and calm (Grace, 26, medium-sized mixed animal practice, Ireland). It used to be if there was a complaint, you’d not see it as serious, but if the client threatens to complain to the RCVS, that creates huge stress and takes up so much time. The minute someone comes into the consulting room I’m sizing them up if they are likely to be aggressive or make a complaint (Sarah, 43, small animal practice, UK)
Sensory knowing
This is a form of sensorium knowledge (Hockey and Allen-Collinson, 2009) which involves deploying one's senses to understand, diagnose, treat or respond to non-human clients (K4). While veterinary ethnography on diagnosis and euthanasia is expanding (Morris, 2012) sparse sociological and ethnographic research exists on how non-humans including farm, companion and zoo animals affect veterinary communications through sighing, vocalisation, eye contact and bodily movements (Llewellyn et al., 2022). However, as shown here, animals’ appearance, noises, smells, feel and movements are significant for sensory diagnosis, handling and treatment.
In our findings, sensory knowledge (K4) was embodied, channelled through the senses, and in the scenario below is seen as more valuable knowledge than scientific test results. Although the vet does not elaborate, suggesting tacit knowledge is at play, he makes professional knowledge claims based on visual observation [and possibly other sensory examinations]. He therefore accords scientific results less priority than sensory knowledge in the context of an ailing elderly animal. You look at a geriatric animal, you know he's not going to survive long and there's no point overmedicating because there's side effects … and no point doing things that last a few days (Patrick, 63, medium-sized mixed practice, Ireland). The blood tests showed the horse had mild liver issues. The owner phoned me at 10pm that night to say they couldn’t get it out of its stable and that it was profoundly distressed. When I turned up the horse was neurological and in mental retardation. It wasn’t thinking. It had gone from mild to severe in a few hours – the only option was to put the horse to sleep (Jan 28, equine practice, England). A lot of what we do is, knowing what something looks like. The contours of the skin, the feel, hard to describe. Then there are the conditions the animal is in, what it feels like, the smells, comes with experience (Patrick, 63, medium-sized mixed practice, Ireland).
The intersectional and Spectrum character of veterinarian's knowledge
The preceding sections presented different veterinary knowledge forms as separate from each other and from scientific knowledge, for ease of comprehensibility and clear delineation. However, almost every quote deployed to illustrate one form of knowledge could be used to demonstrate another form, and different knowledges are often drawn on simultaneously. Veterinarians’ knowledge cultures are therefore at once scientific, deploying knowledge of multiple species in relation to animal health and disease transmission, whilst involving tacit knowledge in local contexts. Veterinarians routinely manage uncertain and incomplete knowledge in relation to different species, the animals’ inabilities to articulate and the local and geographical contexts they encounter. Except with ownerless or wild animals, there is always a tripartite connection between the veterinarian, the human owner and animal. A wavering balance therefore exists between ethics, knowledge and responsibility, incorporating ‘some degree of incomprehensibility between human and non-human animals, all anchored within a particular historical moment and within specific human communities’ (Desmond (2022, p. 3). In this section we therefore demonstrate both the intersectionality and spectrum nature of veterinary knowledge.
In terms of intersectionality, the quote below demonstrates that a compromise must be reached between best scientific practice and what is realistic, drawing on scientific, emotional, contextual and sensory knowledge.: If money wasn’t an issue, and it was possible to put ten different eye drops into the dog's eye every day. Can the owner do that emotionally, pragmatically and financially? Is it possible to do that without being bitten? There are a lot of things to know at the same time (Martin, 64, small mixed practice, Ireland). I enjoy seeing an animal as a puppy and through its life and knowing its owners. I enjoy the diagnostic challenge; it's detective work, solving complex cases (Sarah, 43, small animal practice, UK)
Discussion and conclusions
We have demonstrated that knowledge forms other than explicit and scientific, such as tacit and implicit knowledge, are vital to successful veterinary practice, in diagnosis, treatments, animal welfare, and repeat business. For ease of comprehensibility, we subdivided these non-scientific knowledge forms into local (K1), contextual (K2), emotional (K3) and sensory (K4), but then showed how they intermesh in labyrinthine ways with scientific knowing. Scientific knowledge is always situated within and moderated by constantly changing micro and macro contexts (Bonnaud and Fortané, 2021; Hobson-West and Jutel, 2020). These include the specific human and animal clients interacting with the vet, the animal's environment, community norms and customs, differential cultural and financial valuations of companion vs commodity animals, the positionality and power of the veterinarian, financial constraints, and the availability of diagnosis and treatment technologies, alongside professional and legal codes of practice and policies.
Both contextual and local knowing involve awareness of communicative conventions and community norms, with contextual knowing extending to wider societal norms and legislation. Sensory and emotional knowing are important for vets (see Desmond, 2022), although both involve tacit, often embodied knowledge which may be seen as inferior because of their associations with illogicality and the problems with semiotically describing them. Knowing can also be conceptualised along a spectrum between deep and shallow, so although the knowledge forms we delineated are often combined, in one scenario, one vet might have deep knowledge in relation to one knowledge form and lesser knowledge about another (author's own, 2011). The earlier example of the vet whose business partner had the same veterinary training as her but little knowledge of how to talk about horses and handle them, which made equine clients wary of his expertise, is one example. The melanges of knowledge in veterinary practice are far too complex to be divisible into science versus local or other knowledge cultures; they are instead messy, interlaced, and intermingled (see also Hobson-West and Jutel, 2020; Scholz and Trede, 2023). Good veterinary practice is about communicating and relating well with clients, accurate diagnoses, administering effective treatments, operationalising professional standards, and caring for animals (Clarke and Knights, 2018; Pun, 2020) as well as showing care for their human owners. It is also about demonstrating deep knowledge of the local context including communicative conventions and stories of the community, or showing emotions like compassion and empathy, as well as manifesting scientific expertise. Our research illustrates the power of these conventions and forms of knowing that traverse scientific and tacit knowledge, whilst engendering deeply contextual and emotional elements.
Regarding local and contextual knowledge, research in farming communities shows that cultural scripts defined as a ‘story or common line of argument or an expected unfolding of event … expected in a particular socially defined context’ (Flachs, 2019, p. 256), are significant to veterinary-client interactions. Vanclay and Enticott (2011) discern four script types shaping farmer-vet interactions: catchphrases, allegories, metaphors and common arguments or behaviour in different situations. In Enticott's (2011) study, farm families also took tea with vets before TB testing began, legitimising farmers’ peer status and facilitating relationship-building. There is no research on knowledge and scripts in small animal practices, other than our research. However, in their study of small animal clinics in Canada, MacMartin et al. (2014) illustrate that the phrase ‘I know’ has several functions, including showing empathy with companion animals’ suffering to owners and the term functioning as a linguistic tool to offset emotional distress of pet owners, including anger and fear. Other research shows that during euthanasia, companion animal owners want vets to validate their complex emotions including guilt, obligation and pain and end the animals suffering, alongside recall of happy memories (Fisher, 2013; Morris, 2012). Our research showed this but located these emotions as part of contextual and emotional veterinary knowledge.
In relation to emotional knowing (K3), this coincided with vets learning to control their own emotions of sadness, anger or self-blame regarding euthanasia, ill treatment or uncertainty about their own scientific knowledge. This included how to apply treatments with due cognisance to the emotions of both individuals and communities and how to respond appropriately to both satisfy clients and ensure repeat business. To understand this behaviour, we draw on emotional knowing (K3) to describe how emotion can be seen, rather than as anti-knowledge because of its assumed links with unreason, but as a source of knowledge where not only people possess emotions, but various places, spaces and landscapes may resonate emotionally too (Bondi, 2009). Hochschild's (2012 [1983]) concept of emotional labour involves the performance of certain emotions, as part of the expected job role, that may or may not be subjectively felt. In veterinary practice, this may involve minimising or suppressing rage and anger when an animal is ill-treated or when convenience euthanasia is requested or expressing unfelt feelings of concern and empathy to an unfamiliar client. Alternatively, if vets feel very emotional during euthanasia, perhaps because they knew the pet and owner well, or they are newly qualified, they might suppress those emotions to demonstrate calm and deal with the human client's distress.
Knowledge and understanding of human clients’ feelings is therefore important, as well as how vets react to this in response. Empathic responses not only validate the human client's emotions but encourage repeat business. Showing empathy towards clients was especially important in small and medium-sized clinics that specialised in companion animals and in mixed practices that dealt with pets and farm animals. It was less significant in larger and corporate-run clinics than small/medium ones, mainly due to prioritising KPIs and intense workloads. Although dealing with client emotions can be an occupational stressor associated with suicide and burnout in vets (Andela, 2020, 2021), in one study of 107 Italian veterinarians, empathy for human clients increased rather than decreased with experience and was not linked with burnout or compassion fatigue (Costello et al., 2019). In veterinary literature there is much reference to the psychological concept of ‘emotional intelligence’ (EI) (Shilcock, 2014) - one's percipient ability to identify, make sense of and moderate/control one's own and others’ emotions (Zeidner et al., 2009). EI used occupationally in a manipulative fashion, however, can elevate stress levels (Davis and Nichols, 2016). This could occur within corporate veterinary contexts and the time [deficit] culture, where taking time and/or failing to sell certain treatments minimised profit margins, mediated against vets engaging deeply with clients. EI also focuses on the individual rather than addressing structural issues. Consequently, workers may be monitored and ‘appropriate’ emotional expression enforced. Stress or inequality may also be reframed as a lack of EI which can shift blame onto workers instead of organisations or cultures. This manipulation can overlap with Hochschild's idea of emotional labour as a form of employer control over feelings, although the two concepts emanate from different disciplines (sociology and psychology).
In relation to sensory embodied knowledge (K4), this was an important part of veterinary practice. In human medicine there is a crisis around the legitimacy of clinical judgement focused on the senses (Maslen, 2016), for example, being able to feel and identify where a tumour is or hear and diagnose an issue from someone's breathing or heartbeats via a stethoscope. Such sensory diagnosis is seen as less accurate than test results, although Maslen and Harris (2021) offer multiple examples of how human medics use their senses in diagnosis, often tacitly and un/subconsciously, for example, orthopaedic surgeons being aware of sound pitch changes the closer they get to the edge of the bones. Sensory knowledge (K4), except for vision, is not only marginalised within human medicine and arguably veterinary medicine too, but has also received minimal attention in SSK and social science more generally, with certain senses such as touch and smell being highly complex but less researched and more debased than vision and hearing (Green, 2017, 2021; Green et al., 2021). Minimal research deals with the multisensory nature and integration of experience and knowledge, as most research just concentrates on one sense although ‘sensory experiences are produced, enacted and perceived in combination with each other, intertwined with emotion, meaning and memory (Hsu, 2008, p. 440). In Jakubowska's (2019) sociological analysis of sensory knowledge he shows how sensory knowledge becomes internalised as particular skills or techniques, learned through observation, imitation, experience and practice. These enable ‘experts’ to make sense of scans, smells, touch, sounds and sights a layperson would not understand. Experience also enables more subtle differences in sensory perception to be noticed and made sense of. Such embodied skills are difficult to transmit purely via words and diagrams, particularly with more debased senses like touch and smell, which have minimal vocabularies. Polanyi's assertions that tacit knowledge is untellable have been contested by claims it can be expressed verbally but only in a particular context or to a particular audience (Thornton, 2013). However, this counter claim would appear difficult to substantiate in veterinary practice regarding sensory knowledge, where animals cannot articulate their issues and a limited vocabulary for the senses exists. Even when blood tests or X-rays are conducted, a physical examination involving all the senses is necessary to give some indication of what the problem is and its potential severity.
Although the complexity of veterinarians’ work is beginning to be acknowledged, and communication skills, ethics and public health now form part of the veterinary curriculum in universities in the UK and Ireland, the emphasis is still on the ‘hard’ sciences like anatomy, physiology, chemistry, parasitology, microbiology and pharmacology. Our research on the intersectionality, spectrum nature and indivisibility of different knowledge forms, illuminating their hybridity and cultural importance, therefore has important consequences for the education and training of veterinarians and future research into how different forms of knowledge are transmitted, acquired and applied in different veterinary settings.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Investment Fund, Edge Hill University (grant number MORAN17).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.