
Abstract
This review examined the effectiveness of peer-mediated pivotal response treatment (PM-PRT) to increase social-communication skills for children with autism spectrum disorders (ASD). A systematic review was conducted of all published studies examining PM-PRT in school-aged children with ASD, based on an established rubric. Five PM-PRT studies utilizing single-subject research designs were reviewed, involving 29 participants (8 with ASD and 21 peer coaches). Most studies of PM-PRT observed positive outcomes. However, the existing research base did not meet criteria for classification as promising or established evidence-based practice (EBP) for improving social skill deficits in children with ASD. More research is required for PM-PRT to be considered formally as EBP. This review may be used to guide clinical decisions for school psychologists and future research. Our aim was to highlight the rationale for, and core aspects of, this intervention and discuss school-based applications.
Keywords
Introduction
The gap in availability and implementation of effective intervention models for children with autism spectrum disorders (ASD) is striking. Although school teams in Canada and elsewhere typically address the academic and behavioural needs of children with ASD, their social and communication needs often remain unmet (Dingfelder & Mandell, 2011; Parsons & Kasari, 2013). This is critical because difficulties in social communication are central in ASD (Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5; American Psychiatric Association, 2013]) and represent a major barrier for school and vocational functioning (Rao, Beidel, & Murray, 2008). Moreover, positive peer interactions and social inclusion are among parents’ most valued outcomes for their children with ASD (Bellini, Peters, Benner, & Hopf, 2007; Kretzmann, Shih, & Kasari, 2015) and are important predictors of real-world success (Happé, Booth, Charlton, & Hughes, 2006; Mesibov, Shea, & Adams, 2001).
Because children spend most of their days at school, it is crucial to identify evidence-based approaches for children with ASD that are acceptable and feasible to school stakeholders such as school psychologists and special educators. School psychologists carry large varied caseloads, and children with ASD usually require individualized programming (Corkum et al., 2014; Jordan, Hindes, & Saklofske, 2009). Peer training approaches offer a logical, face-valid, and cost-effective means of social skill development for children with ASD (Chan et al., 2009). A specific peer training approach based on pivotal response treatment (PRT; R. L. Koegel & Koegel, 2006) holds high heuristic value for implementation in the school system, owing to its emphasis on embedding learning opportunities into everyday contexts and existing routines (R. L. Koegel, Matos-Fredeen, Lang, & Koegel, 2012; Stahmer, Suhrheinrich, Reed, Schreibman, & Bolduc, 2011).
Peer-Mediated Intervention (PMI) Research for Children With ASD
PMI refers to an approach in which typically developing peers are trained to implement an intervention directed toward children with a disability (Chan et al., 2009). This contrasts with traditional intervention approaches for children with ASD in which adults (e.g., parents or clinicians) are the primary intervention agents. PMIs typically target social competence and aim to use socially adept peers as the intervention agents (Locke, Rotheram-Fuller, & Kasari, 2012).
Five previous reviews have examined the evidence base for PMI for children with ASD in general—two narrative reviews (Bass & Mulick, 2007; DiSalvo & Oswald, 2002) and three quantitative reviews using formal evaluation frameworks (Chan et al., 2009; Wang, Cui, & Parrila, 2011; Zhang & Wheeler, 2011). Overall, PMI was found to be highly effective in improving social skills of children with ASD (Cohen’s d = 1.27-2.44; Wang et al., 2011; Zhang & Wheeler, 2011). One previous book chapter examined peer-mediated (PM)-PRT studies (Ferraioli & Harris, 2011) in addition to other treatment approaches designed to increase social awareness and social skills of children with ASD, using a systematic, reliable and rigourous framework (Reichow, Volkmar, & Cicchetti, 2008). However, Ferraioli and Harris (2011) did not review several published PM-PRT studies and drew no conclusion regarding the status of PRT-based PMI as evidence-based practice (EBP). Moreover, their review lacked sufficient depth on PM-PRT to provide practical guidance for school psychologists. Such is the current focus, reflecting our position that peer-implemented PRT is an intervention approach with excellent potential for implementation in schools. PMIs have been identified as an effective inclusion strategy for children with ASD (Harrower & Dunlop, 2001). Our aim is to provide evidence to inform intervention decisions for educational teams.
PRT: A Promising PMI Approach
PRT is a naturalistic behavioural intervention in which “pivotal” areas are targeted that produce collateral changes in other aspects of children’s behaviour (R. L. Koegel & Koegel, 2006). Motivation is one such pivotal area. Interventionists use motivating items in children’s environments to provide natural language opportunities (L. K. Koegel, Koegel, Harrower, & Carter, 1999), for example, by holding up a preferred and a non-preferred toy and asking, “What do you want?” PRT also focuses on increasing children’s self-initiations and fostering self-management, and encourages responding to multiple cues (R. L. Koegel & Koegel, 2006). Teaching opportunities are embedded in the context of everyday life (often in play) to enhance generalization. PRT can be delivered by adults or peers at home, school, the clinic, or the community. For more information about PRT procedures, see R. L. Koegel and Koegel (2012).
PRT has considerable empirical support (National Autism Center [NAC], 2009; Wong et al., 2014) as an effective way to increase functional communication and associated skills for children with ASD (R. L. Koegel & Koegel, 2006; I. M. Smith, Flanagan, Garon, & Bryson, 2015; I. M. Smith et al., 2010). PRT shares the theoretical underpinnings of the broader field of applied behavioural analysis (ABA). However, PRT’s specific focus is on increasing children’s motivation for learning and communication (R. L. Koegel & Koegel, 2006). Most PRT approaches are implemented by parents (R. L. Koegel, Koegel, & McNerney, 2001; Rogers & Vismara, 2008; Suhrheinrich, 2011). In Nova Scotia, parents and clinicians implement a publicly funded intensive PRT-based intervention program for preschoolers with ASD (i.e., Nova Scotia Early Intensive Behavioural Intervention [NS EIBI]; Bryson et al., 2007). Community effectiveness data are promising, with improvements across multiple social, communicative, and cognitive domains for children with ASD (I. M. Smith et al., 2015; I. M. Smith et al., 2010), and results that are comparable with those of another preschool ASD intervention model based on the verbal behaviour approach (Stock, Mirenda, & Smith, 2013). However, even in Nova Scotia, PRT is infrequently utilized in schools, and when it is utilized, it is most often as a component of the Strategies for Teaching Based on Autism Research (STAR) approach (Arick, Loos, Falco, & Krug, 2004).
Like PMI, PRT offers a face-valid, potentially cost-effective intervention approach for children with ASD at school. Unlike discrete-trial-based ASD interventions (Eikeseth, Smith, Jahr, & Eledevik, 2002; T. Smith, 2001), PRT is designed to be conducted in the context of everyday routines and in natural environments. Several school-based studies in the United States have demonstrated initial efficacy in training teachers or school paraprofessionals such as Teaching Assistants to implement PRT (Dyer, Williams, & Luce, 1991; Robinson, 2011; A. E. Smith & Camarata, 1999). Stahmer et al. (2011) recently described class-wide application of PRT, and Renshaw and Kuriakose (2011) also provided guidelines for school psychologists to implement PRT within their practice at school. However, none of these authors mentioned PM-PRT. Given PRT’s strong evidence base and apparent good fit for school settings, surprisingly few studies have examined the effectiveness of teaching classmates of children with ASD to serve as PRT coaches (Ferraioli & Harris, 2011).
PM-PRT is also ideally suited to meeting provincially mandated inclusion policies for youth with disabilities (Timmons & Wagner, 2008). For children with ASD, evidence tells us that inclusion alone is insufficient to increase social skills (Chamberlain, Kasari, & Rotheram-Fuller, 2007; Ferraioli, & Harris, 2011; Kasari, Locke, Gulsrud, & Rotheram-Fuller, 2011). Furthermore, discrepancies often exist between provincial inclusion policies and how students with ASD are supported. PM-PRT fosters social skills in children with ASD while promoting interaction with typically developing classmates. To help school personnel bridge this gap in services, we offer this description of the specific aspects of PM-PRT that suggest its high potential for school-based services and summarize the relevant research literature.
Focus of Present Article
The purpose of this review is to evaluate systematically the effectiveness of PMI using PRT (R. L. Koegel & Koegel, 2006) for facilitating the social-communication behaviour of school-aged children with ASD. Although PMI and PRT are each separately classified as EBP (NAC, 2009; Wong et al., 2014), whether the evidence for the combined approach (i.e., PM-PRT) meets established EBP criteria is unknown. We will address this using the Reichow et al. (2008) criteria for determining EBP in ASD, based on single-subject design studies. An in-depth evaluation of PM-PRT studies is critical to summarizing and interpreting results, to external validity, and to replication and generalizability of study results (Patterson, Smith, & Mirenda, 2012). Following this analysis, we discuss implications for educational programming, practical information for school psychologists, as well as directions for researchers in educational settings (Campbell, 2013).
Method
Search Procedures
Studies were identified using PsycINFO and PubMed databases using the following key words: (a) autism, autism spectrum, autistic spectrum, pervasive developmental disorder, neurodevelopmental disorder, mental retardation, and learning disorder; (b) peer mediation, peer training, peer mentoring, peer-mediated intervention, and peer support; (c) treatment, intervention, management, and peer training; (d) pivotal response treatment; and (e) children, school, and pediatric. Additional articles were sought by hand searching reference lists of all articles retrieved from the search criteria and journals of the articles selected for the present review. Publication year was not restricted; articles were included in this review if they were written in English and reported the results of any study of PM-PRT for school-aged children with ASD. Technical reports, dissertations, and unpublished documents were not included.
Inclusion and Exclusion Criteria
For inclusion in this review, each article had to describe a research study that included provision of PM-PRT with the aim of enhancing social-communication skills for at least one school-aged (4-18-year-old) child with an ASD diagnosis (i.e., autistic disorder, Asperger syndrome or pervasive developmental disorder—not otherwise specified [PDD-NOS], American Psychiatric Association, 2000; or autism or autistic spectrum disorder).
Systematic Review Framework
We evaluated the evidence for efficacy of PMI using PRT with the Evaluative Method for Determining Evidence-Based Practice in Autism (Reichow et al., 2008). Although ratings are typically used to exclude studies that lack rigour from the review process, we retained all existing studies to achieve a comprehensive examination of the extant small body of literature. A close examination of study characteristics allows us to offer suggestions for future research.
Level-of-Evidence Rating
Five primary quality indicators (participant characteristics, independent variable, dependent variable, baseline condition, and visual analysis) and six secondary indicators (inter-observer agreement, Kappa, fidelity, blind raters, generalization and/or maintenance, and social validity) were examined according to another rubric (Guidelines for the Determination of Research Report Strength) from the Reichow et al. (2008) evaluative framework. This rubric aggregates research into one of three level-of-evidence ratings (“Strong,” “Adequate,” or “Weak”).
Data Extraction and Analysis: Coding Quality Ratings
In-depth data were extracted about five variables: (a) research methods, (b) participants, (c) intervention, (d) outcome measures, and (e) success estimates. As Wang and Parrila (2008) and Reichow et al. (2008) recommended, several quality indicators were expanded from the original rating system to capture the unique qualities of PMIs (e.g., expansion of “participants” to include peer trainer characteristics, “study design” to specify types of single-subject research design, and “intervention type” to focus on specific PRT components).
Inter-Rater Reliability (IRR)
IRR was assessed on 100% of the studies, as coded by the first and third authors. IRR was calculated for the 12 quality indicators as a percentage of total initial agreements on items coded. Inter-rater agreement was good on all individual indicators (ranged from 80% to 100%), with 90% agreement across all quality indicators (Cohen, 1960).
Level of EBP
Finally, for an intervention to be classified as “evidence-based” (Buysse & Wesley, 2006), the body of single-subject research literature must have (a) a minimum of five single-subject design studies that meet minimally acceptable criteria, (b) studies conducted by at least three different researchers across three or more research sites, and (c) a total of at least 15 participants included in the five or more studies (Reichow et al., 2008). The standards to be classified as “promising EBP” consist of (a) a minimum of three single-subject studies meeting minimally acceptable criteria, (b) studies conducted by at least two different researchers across at least two different sites, and (c) a total of at least nine participants in the three or more studies (Reichow et al., 2008).
Results
The systematic literature search produced 36 citations. Three additional articles were examined for potential inclusion after hand searching reference lists of all articles retrieved from the search criteria and journals of the articles selected for the present review. After removal of duplicates and reviews, and the application of inclusion and exclusion criteria, a total of five articles were included in the present review.
Literature Synthesis
Overview
The included studies form an exhaustive list of the identified literature to date on PM-PRT for individuals with ASD of all ages. Five PM-PRT studies were identified (see Table 1). All studies were conducted in the United States.
Summary and Ratings of the Reviewed Studies.
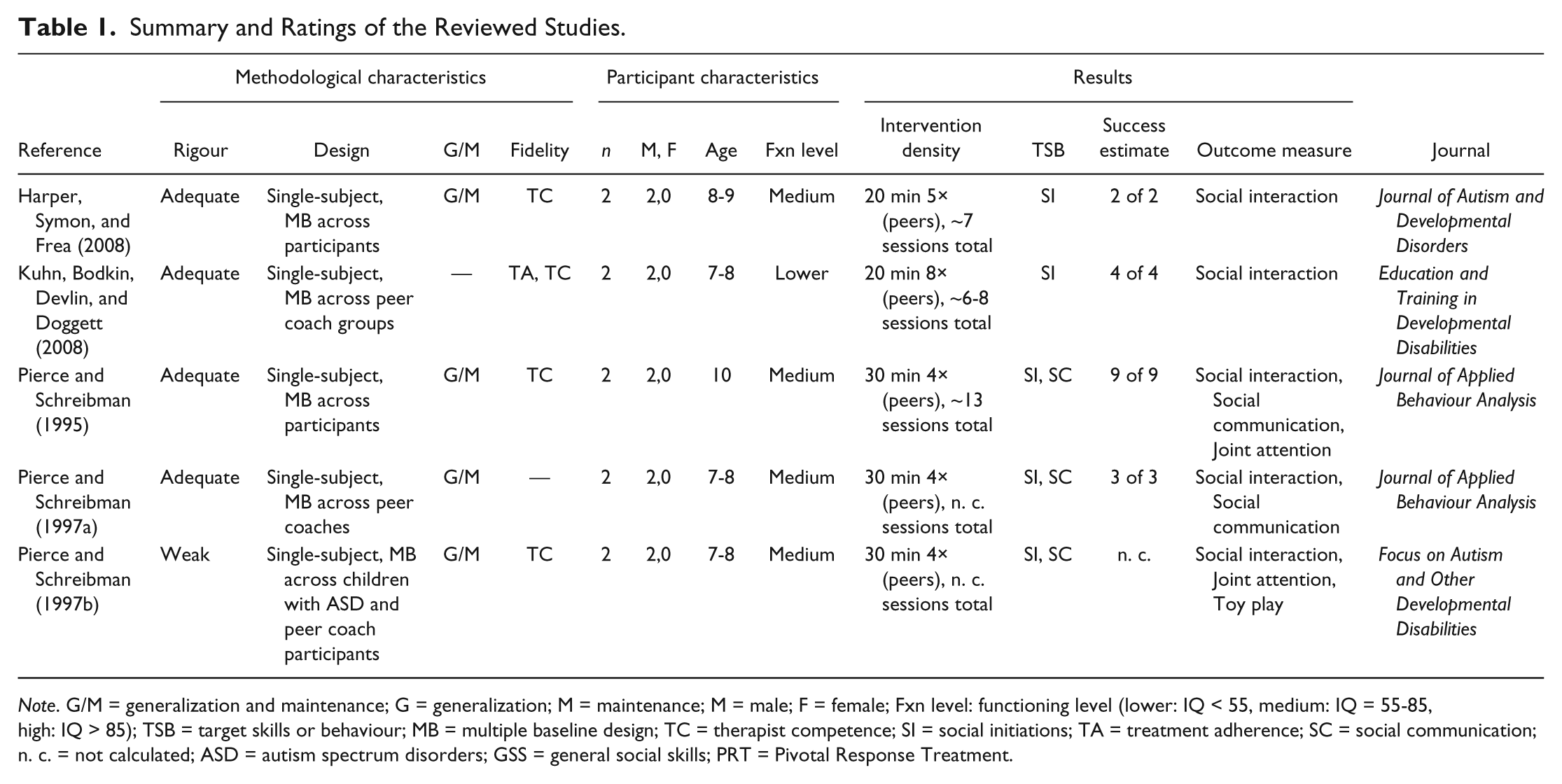
Note. G/M = generalization and maintenance; G = generalization; M = maintenance; M = male; F = female; Fxn level: functioning level (lower: IQ < 55, medium: IQ = 55-85, high: IQ > 85); TSB = target skills or behaviour; MB = multiple baseline design; TC = therapist competence; SI = social initiations; TA = treatment adherence; SC = social communication; n. c. = not calculated; ASD = autism spectrum disorders; GSS = general social skills; PRT = Pivotal Response Treatment.
Participants
Two studies examined different outcome measures in the same participants (Pierce & Schreibman, 1997a, 1997b). Accounting for this overlap, five PM-PRT studies examined eight children with ASD and 21 peer coaches. Ratios of peer coaches to target children with ASD varied from 1:1 to 3:1. All studies had participants (e.g., target children with ASD and peer coaches) aged from 7 to 9 years (M = 8 years 4 months; see Table 1); no study examined PM-PRT in junior or senior high school students. The intervention was delivered by same-aged classmates in all studies. Teachers par-ticipated in one study (Pierce & Schreibman, 1995) by completing a social skills questionnaire about the children with ASD. All participants with ASD were male. Peer coaches included approximately equal numbers of males (52%) and females. No attempts to match peer dyads for gender or other features were indicated. Target children with ASD were most likely to have cognitive functioning in the moderate to borderline intellectual disability range (IQ of 55-85). Diagnoses of autism or ASD were reported for all target children; the means by which these diagnoses were made were not described. Peer coaches were reported to be typically developing in four of five studies. In the remaining study (Kuhn, Bodkin, Devlin, & Doggett, 2008), peer coaches had diagnoses of mild intellectual disability or learning disability and attended a full-time special education classroom. Peer selection method was specified in three of five studies (Harper, Symon, & Frea, 2008; Pierce & Schreibman, 1995, 1997b). In each, peer coaches were selected on the basis of teacher nomination. Teachers reportedly selected peers who were cooperative, friendly, and had good school attendance.
Method
Generalization and/or maintenance were measured in four studies (Harper et al., 2008; Pierce & Schreibman, 1995, 1997a, 1997b). Of those, generalization was measured post-intervention in one or two 10-min periods in non-training locations and/or with non-trained peers. Three studies (Pierce & Schreibman, 1995, 1997a, 1997b) measured generalization under three conditions: (a) in a non-training empty classroom, (b) with novel (non-training) toys, and (c) with non-training peers. Procedural fidelity (Billingsley, White, & Munson, 1980) was examined in one study (Kuhn et al., 2008) and analyzed using two components of treatment integrity (fidelity of treatment adherence and therapist competence; Perepletchikova & Kazdin, 2005; Reichow et al., 2008). One study (Kuhn et al., 2008) contained measures of treatment adherence and adult trainer competence. Four studies contained measures of peer coach/therapist competence (Harper et al., 2008; Kuhn et al., 2008; Pierce & Schreibman, 1995, 1997b). The nature of these measures was specified in only one study that employed a peer competence checklist (Harper et al., 2008). No study measured fidelity across experimental conditions.
All five studies met criteria for social validity according to the EBP framework definition (Reichow & Volkmar, 2010). For example, all studies displayed a minimum of four features necessary for classification as socially valid (e.g., socially important dependent variables, time- and cost-effective, independent manipulation by people who typically come into contact with the child with ASD, and natural context). However, no study examined consumer satisfaction or comparison of individuals with and without disabilities, which are other possible aspects of social validity.
Outcome measures
Increases in the frequency of social-communication behaviour of the target child with ASD were the most common targeted skills. Specifically, social initiations (e.g., beginning a conversation, approaching a peer to play without a prompt) and social responses (e.g., a verbal, gestural, or physical response to peer prompt) measured using direct behavioural observation were the most common outcome variables. These were measured reliably across all studies (IRRs = 86%-98%). Two studies (Pierce & Schreibman, 1995, 1997b) also examined post-treatment changes in collateral behaviour such as language, joint attention, and toy play. One study (Harper et al., 2008) identified individualized goals for the target children with ASD, in addition to common target behaviours measured through direct observation (initiations [i.e., any appropriate verbal or non-verbal attempt to gain a peer’s attention to initiate or engage in a play activity] and turn taking [i.e., a social exchange within a play activity]). All studies used behavioural coding schemes (video or live coding) to measure dependent variables. However, two studies (Pierce & Schreibman, 1995, 1997b) used multiple methods and/or sources of data in addition to observational measures (e.g., teacher questionnaire [Walker–McConnell Scale of Social Competence; Walker & McConnell, 1988] and 10-min pre–post language samples for target child with ASD).
Intervention characteristics
All studies took place at school, usually during recess. All studies used PRT strategies and peer training procedures from a manual, Kids Helping Kids: Teaching Typical Children to Enhance the Play and Social Skills of Their Friends With Autism and Other PDDs, developed by Pierce and Schreibman (1995). Two pivotal areas/mechanisms of change were targeted: altering attention and motivation.
Peer training followed the same general procedure in all studies: (a) instruction of the peer coach in PRT techniques without the target child with ASD present, (b) strategies modeled by adult trainer, (c) role play strategies with adult, (d) role play strategies with other peer coaches, and (e) pair peer coaches with child with ASD, and adult trainer provides intermittent feedback. One study also provided training to peers about managing potential aggressive behaviour of children with ASD (Harper et al., 2008). Most studies (four of five) reported that training sessions continued until peer coaches were able to implement strategies with at least 80% mastery. See Table 2 for additional intervention details.
Summary of Intervention Characteristics.
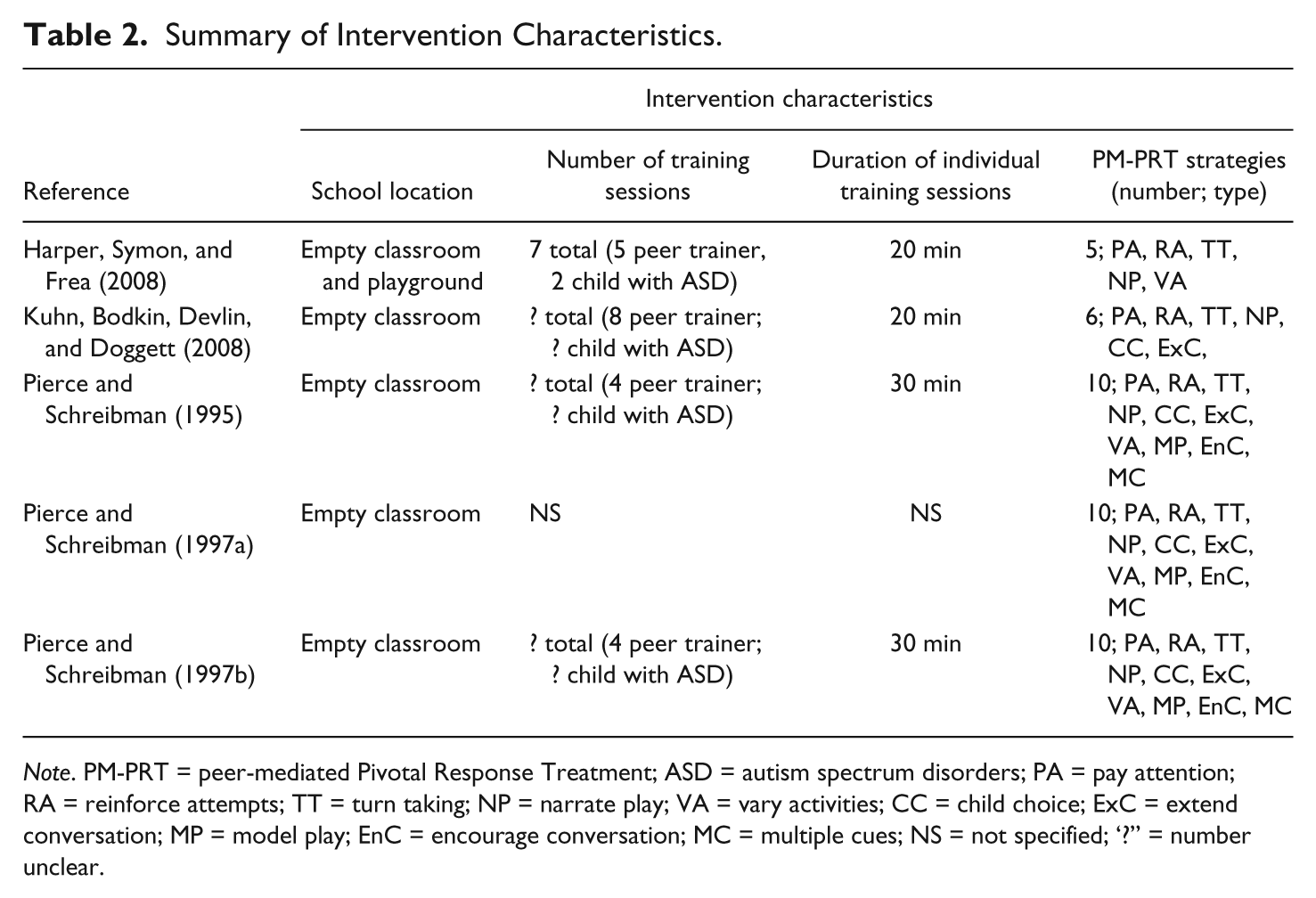
Note. PM-PRT = peer-mediated Pivotal Response Treatment; ASD = autism spectrum disorders; PA = pay attention; RA = reinforce attempts; TT = turn taking; NP = narrate play; VA = vary activities; CC = child choice; ExC = extend conversation; MP = model play; EnC = encourage conversation; MC = multiple cues; NS = not specified; ‘?” = number unclear.
Level of EBP
The results from the five existing studies were used to determine whether PM-PRT for school-aged children with ASD met the Reichow et al. (2008) criteria for either of the two levels of EBP: established and promising. Criteria were not met for either level (i.e., <30 points on the EBP status formula; see Reichow et al., 2008, Table 4).
Discussion
Our systematic review yielded only five studies that examined PM-PRT for school-aged children with ASD. However, the level of research rigour is commendable: Four out of five studies of PM-PRT have adequate research rigour. The most common characteristics of these four studies were (a) participants with ASD aged approximately 8 years with IQs of 55 to 85, (b) density of at least seven 20-min intervention sessions across at least 2 weeks, (c) school setting, and (d) use of Pierce and Schreibman’s (1995) manual. Owing to the small number of published studies, the intervention does not yet meet criteria for either promising or established EBP. However, given the brevity of treatment (~2 weeks) and the importance of the treatment target (social skills) for children with ASD (Bellini et al., 2007), the approach appears highly promising.
Our review of the entire body of published PM-PRT literature extends previous social skills intervention reviews (Ferraioli & Harris, 2011; Reichow & Volkmar, 2010) by analyzing the entire PM-PRT literature in depth. Our results were incongruent with those of Chan et al. (2009), who used another synthesis method. For example, we concluded that several PM-PRT studies had adequate research rigour, whereas Chan et al. (2009), using the Certainty of Evidence Framework (Millar, Light, & Schlosser, 2006), assigned “inconclusive” ratings to several of the same studies. The discrepancy arises from different operational definitions of fidelity. Discrepancies among conclusions across reviews are confusing for key stakeholders (e.g., school psychologists and other practitioners, parents, policy makers). The current review framework utilized an operational definition of fidelity congruent with ASD intervention standards (Reichow et al., 2008). Fidelity is integral to understanding the efficacy of an intervention approach and identifying essential treatment components (Wainer & Ingersoll, 2013). Future research should report additional dimensions of fidelity (e.g., individual strategy and global ratings, treatment exposure details, data throughout all experimental phases).
Limitations of Current Review Framework for Evaluating PMI
As mentioned, we expanded several coding indicators to synthesize the PMI literature. Two expanded categories are particularly relevant for summarizing the evidence base of PM-PRT:
Addition of peer coaches/peer coach selection to the “participant” category. Previous syntheses excluded consideration of peer coach participants, and focused exclusively on the characteristics of target children with ASD. This is unfortunate, because as the key intervention agents, peers are presumed to be an active treatment mechanism (Reichow & Volkmar, 2010). The omission of information about peer participants across studies and across reviews constrains our ability to draw strong conclusions about the essential characteristics of successful peer implementers (see Locke et al., 2012, for an example from an intervention other than PRT).
More detailed description of intervention characteristics. PMI reviews should characterize the number of peer training sessions, participant composition of these sessions (e.g., child with ASD, peer coach(s), adult facilitators), specific treatment model (e.g., PRT), location and class composition at school, and intervention strategies. It would also be important to understand the training and experience of adult facilitators (e.g., level of schooling, profession, training in PRT). In the present review, a detailed examination of the interventions revealed that five PRT strategies were common across studies with adequate research rigour (i.e., paying attention, reinforcing attempts, taking turns, narrating play, child choice; Pierce & Schreibman, 1995). Additional aspects to be specified include the reinforcement schedule and reinforcers, or other relevant aspects of the peer training methods (e.g., use and type of prompts, fading schedules). Detailed review of intervention characteristics is critical for revealing active treatment ingredients and for replication.
Limitations
The current synthesis is limited by the small number of studies and lack of independence among studies (i.e., inclusion of two studies, that is, Pierce & Schreibman, 1997a, 1997b, with the same participants). Given the paucity of studies, we considered it important to include both and to describe the research in sufficient depth to pro-vide meaningful suggestions. As the literature grows, a more conservative inclusion approach will be warranted.
Areas for Future Research
Teaching same-aged peers to implement PRT strategies to promote the social-communication skills of children with ASD is an emerging area. Although PM-PRT did not meet formal EBP criteria, one additional high-quality single-subject study that demonstrated a treatment effect for one additional child with ASD would move this intervention into the “promising” EBP category according to one evaluation framework (Reichow et al., 2008). Additional research is needed to enlarge the evidence base regarding PM-PRT, as well as to define further the parameters of its effectiveness.
All current studies of PM-PRT use a common treatment manual, that of Pierce and Schreibman (1995). However, this manual targets fewer and different pivotal areas (e.g., motivation and attention) than the manual commonly referenced for adult-facilitated PRT (which includes responsivity to multiple cues, self-management, and social initiations; R. L. Koegel & Koegel, 2006). Moreover, Pierce and Schreibman (1995) omitted several widely used PRT strategies (e.g., task variation, interspersing maintenance and acquisition tasks, rewarding attempts), presumably on the basis that these would be difficult to teach to young children. It is unclear how these changes affect the integrity of PRT as an intervention package. Additional research is needed to tease apart this issue. Another noteworthy trend is the narrow age range of existing studies examining PM-PRT. Additional research is needed both in the earliest and later school years; for instance, with an emphasis on critical transitions such as entry to school and adolescence.
PM-PRT has much to offer Canadian schools. PRT has evidence of efficacy for teaching students with ASD (Odom, Boyd, Hall, & Hume, 2010). PRT’s use of preferred activities and teaching in the context of naturally occurring routines (e.g., recess or classroom activities), along with the use of an abundant, face-valid resource (i.e., classmates) as interventionists, promotes the social development and generalization of social skills for children with ASD (R. L. Koegel, Dyer, & Bell, 1987). As PRT focuses on pivotal behaviours that produce widespread change, this intervention produces more enduring social skill gains than do some other ABA programs (Mohammadzaheri, Koegel, Rezaee, & Rafiee, 2014). Future research should focus on how to promote the uptake of this intervention approach at school (see Wood, McLeod, Klebanoff, & Brookman-Frazee, 2015, for another PMI example). School psychologists are ideally situated to foster the uptake of EBP, as well as to help teachers adapt individualized program plans to include relevant and measurable social skills goals for children with ASD (Mckenney, Dorencz, Bristol, & Hall, 2015; Renshaw & Kuriakose, 2011). Future research should also examine the effectiveness of PM-PRT as an inclusion strategy.
Conclusion
It is surprising that, 18 years after the first study of PM-PRT, evidence regarding this intervention remains limited. This is particularly striking given the recent growth in PRT research in general (e.g., Verschuur, Didden, Lang, Sigafoos, & Huskens, 2014) and the designation of PRT as an established treatment (NAC, 2009; Wong et al., 2014). A complementary body of literature on PMIs has also accumulated impressive empirical evidence of effectiveness (e.g., Reichow & Volkmar, 2010). Expanding the body of research combining these approaches (PRT and PMI) in school settings is a logical, feasible, and important next step to meet the social inclusion needs of children with ASD. As Canadian children enter school as early as 4 years in some provinces, educators need to adapt to meet the developmental needs of both typically and atypically developing children. As the gap grows between what ASD research tells us and the availability of evidence-based social skills interventions in schools (Dingfelder & Mandell, 2011; Parsons & Kasari, 2013), so too must our understanding of effective, acceptable, and feasible intervention modalities and how best to implement them.
Additional research is also needed to determine whether PM-PRT will meet the “promising” EBP category. EBP classification is increasingly important to school boards and policy makers to guide educational programming decisions (Odom, Collet-Klingenberg, Rogers, & Hatton, 2010; Reichow et al., 2008). Given the importance of social inclusion as an intervention target for children with ASD and their families (Kretzmann et al., 2015) and the considerable resources students with ASD require at school, additional research is warranted. Canadian research is also needed to address the unique benefits and challenges of implementing PM-PRT in the context of our educational systems. School psychologists are critical partners in the applied research disseminating PM-PRT at school.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Student Grant 36042 from the Organization for Autism Research.