
Abstract
Acute care settings can expose staff to job-related stressors. Pups Assisting Wellness for Staff (P.A.W.S.) has been designed as an innovative approach to support acute care staff in the emergency department and intensive care unit. Initially, P.A.W.S. was implemented as a Comfort Dog Pilot and then expanded into a Therapy Dog Model. The Therapy Dog Model incorporated learnings from the Comfort Dog Pilot to evaluate the impact of the following: more dogs, using certified therapy dogs, and visiting at different times of the day. Results throughout the project demonstrated a positive impact on staff morale, staff stress, overall and staff satisfaction, and a strong desire for the project to continue. As a result and with a collaborative effort between a multidisciplinary team, P.A.W.S. has now been operationalized as a permanent program to support staff in acute care.
Introduction
Canine-assisted interventions have been implemented in high-stress occupational settings such as fire and police departments to support staff wellness. It has been observed that these interactions reduce staff stress levels and promote social interactions in the workplace. 1
Within the context of healthcare, another potentially high-stress occupational environment, canine-assisted interventions have had a patient focus. Canine-assisted interventions supporting patients have been successfully introduced into the Emergency Department (ED) and Intensive Care Unit (ICU) settings to reduce patient stress and support recovery. 2,3 A study of attitudes towards therapy dogs in acute care demonstrated a high percentage of both patient and staff acceptance of therapy dogs in the ED. 4 However, there are few examples of therapy dog initiatives for acute care staff.
The purpose of the Pups Assisting Wellness for Staff (P.A.W.S.) project was to evaluate the potential impacts of canine-assisted interventions on acute care staff.
This report endeavours to share the experience of implementing and evaluating canine-assisted interventions for acute care staff within an acute care setting.
Methods
The P.A.W.S. project consisted of two phases (Comfort Dog Pilot and a Therapy Dog Model) and was supported by a multidisciplinary team made up of operational leadership; the Canine Detection Unit; St. John Ambulance Therapy Dog Program; Employee Safety, Health and Wellness (ESHW); Quality and Patient Safety; physicians and clinicians from the ICU, ED, and Burns, Trauma, and High Acuity (BTHA); Volunteer Resources; and a British Columbia Patient Safety and Quality Council student intern.
Comfort Dog Pilot (August to October 2018)
In 2018, a young canine (Dr. Snuggles) was introduced to Vancouver Coastal Health’s (VCH) Canine Detection Unit, a specialized program utilizing canines to conduct Clostridium difficile screening. During the socialization phase of his training, Dr. Snuggles was introduced to the hospital setting to determine if he had an appropriate temperament for the environment. Throughout Dr. Snuggles’ training, his handlers received numerous requests for him to visit with people. As Dr. Snuggles was not a certified therapy dog, the initiative was messaged as a Comfort Dog Pilot.
Prior to the launch of the Comfort Dog Pilot, P.A.W.S. was promoted through posters and emails as an innovative pilot project to complement existing and emerging staff wellness supports. Clinician leads in each unit also conducted in-person staff polls. The poll results informed the visitation schedule and the types of visits staff were most interested in (eg, walkabouts, scheduled drop-in sessions). Staff with allergies or anxiety in the presence of canines had the opportunity to express their concerns and further inform the visitation schedule. The poll also gauged whether staff anticipated that P.A.W.S. would positively impact staff morale.
During the first month of the Comfort Dog Pilot, Dr. Snuggles visited both the ED and ICU for 1 hour twice per week, at times when the few staff members who wanted to avoid canine interactions were not present. Dr. Snuggles’ handler spent half of their visit time on a walkabout in the units and the other half of the visit occurred in a room where staff could share a quiet and private space with Dr. Snuggles. The handler promoted handwashing before and after interactions between the staff and Dr. Snuggles and utilized a tally counter to track the number of interactions. Communication materials (eg, posters, playing cards) also included messaging around the importance of hand hygiene and that Dr. Snuggles was there to support staff wellness specifically.
During the second and third months, visits remained twice a week but were reduced to 30-minute walkabouts for both the ED and ICU. Based on feedback, it was discovered that the walkabouts were preferred and that within this time frame, a point of saturation with the number of staff interactions was reached. The availability of the handler also factored into this decision.
During the first month of pilot implementation, comment cards were distributed to staff during each visit to obtain quantitative data on their overall satisfaction with the initiative and whether or not they would like the project to continue and/or expand. The cards also provided a space to share additional thoughts and feedback.
Staff experience surveys were distributed at the end of each month by the unit managers and accounted for the majority of the quantitative data obtained. The surveys used the Checkbox platform and asked staff to optionally identify their role and the specific unit they worked on. The survey inquired about whether or not they had interacted with Dr. Snuggles and, based on their response, directed them to relevant follow-up questions.
Staff were asked on approximately how many times they interacted with Dr. Snuggles and if they felt the project impacted their stress, colleagues, and overall staff morale. They were also asked about their overall satisfaction with P.A.W.S. and whether or not they would like the project to continue and/or expand. Staff were asked about potential barriers experienced while interacting with the canine, and space was provided to share additional feedback.
The P.A.W.S. pilot utilized a mixed method to capture data. Throughout the Three months of the pilot, qualitative participant observation, quotes, and field notes were obtained by the handler. Qualitative survey data and observations were analysed thematically. Quantitative survey data were analysed using basic descriptive statistics in Excel.
Therapy Dog Model (May to November 2019)
Based on the feedback received during the P.A.W.S. pilot, the team integrated the Therapy Dog Model into a Plan, Do, Study Act (PDSA) cycle with the goal of continuous improvement including more visits, using certified therapy dogs, and visiting at different times of the day. The P.A.W.S. team partnered with St. John Ambulance Therapy Dog Program and the VGH Volunteer services after Dr. Snuggles transitioned into his official role as a scent detection dog. Phase 2 of the project consisted of four external certified therapy dog teams.
Early in the planning phase, a partnership was established with VCH ESHW who co-led Phase 2 with the Quality and Safety team. There was a future vision that the P.A.W.S project would eventually be operationalized into a sustainable program under ESHW. The early partnership enhanced the knowledge translation and promoted the development of the project into an eventual program.
For 7 months, four St. John Ambulance therapy dog teams conducted 90-minute visits in the ED, ICU, and the BTHA. The BTHA was included in Phase 2 because of the unit’s proximity to the ICU. During these visits, the therapy dog team would walk down the unit hallways inviting staff to interact freely with the canine as well as any patients or families who showed interest. During each visit, the handler utilized a tally counter to track the number of interactions between the therapy dogs and staff members. Communications materials were distributed that included messaging around use of hand hygiene.
As the expanded model brought in therapy dog teams external to VCH, a curriculum was developed to mentor each therapy dog team and ensure handlers were aware of the workflow, policies, guidelines, risks, and key contacts. The goal of this mentorship was to increase the comfort level of the handlers prior to volunteering on their own.
As in the Comfort Dog Pilot, a mixed methods evaluation approach was utilized for the Therapy Dog Model. Staff satisfaction and experience with the project was primarily assessed through experience surveys. The surveys were electronically distributed twice during the therapy dog phase. One was distributed at the end of the first month (June 2019) and another at the conclusion (November 2019). LimeSurvey was utilized as the preferred platform and established a foundation for ongoing evaluation should the project transition into an operational program.
Feedback on the handlers’ satisfaction and experience was obtained through a variety of methods. A brief survey was provided to the handlers following their mentorship sessions to identify their comfortableness navigating the units and to obtain additional feedback and recommendations from them.
Qualitative participant observations were collected, recorded, and thematically analysed on an ongoing basis. Comment cards were located on the units encouraging staff to continuously provide feedback throughout phase 2. Additionally, the handlers documented their experiences on the Better Impact Volunteer Database every time they signed out of their shift. The collection of real-time data enabled the team to capture numerous stories about the interactions between the therapy dog and staff, as well as patients and families that might have otherwise been missed.
Results
Comfort Dog Pilot (August to October 2018)
A total of 1,548 interactions were facilitated over the course of 26 hours. During the 3-month pilot, a total of 22 walkabout visits in the ED and 22 walkabout visits in the ICU were conducted. On average, 28 staff members interacted with Dr. Snuggles per visit to the ED and 41 staff members interacted with Dr. Snuggles per visit to the ICU.
From both the ED and ICU staff poll results (n = 125), 49% supported having canine walkabouts, 36% preferred scheduled drop-in sessions, 14% supported canine interventions in critical incident debriefing, and 1% wanted to have a comfort dog immediately after code blues and other trauma events. Additionally, 97% of staff believed that the P.A.W.S. project could contribute positively to staff morale.
The initial electronic staff’s satisfaction and experience poll and the following monthly surveys (n = 98) both demonstrated positive staff satisfaction and experience with the pilot project. Figure 1 identifies 89% of the staff “agree” or “strongly agree” P.A.W.S. had a positive impact on staff stress. Together, ICU and ED staff reported an 85% positive impact on staff morale. The overall results indicated 93% satisfaction with the project and 96% supported its continuation.
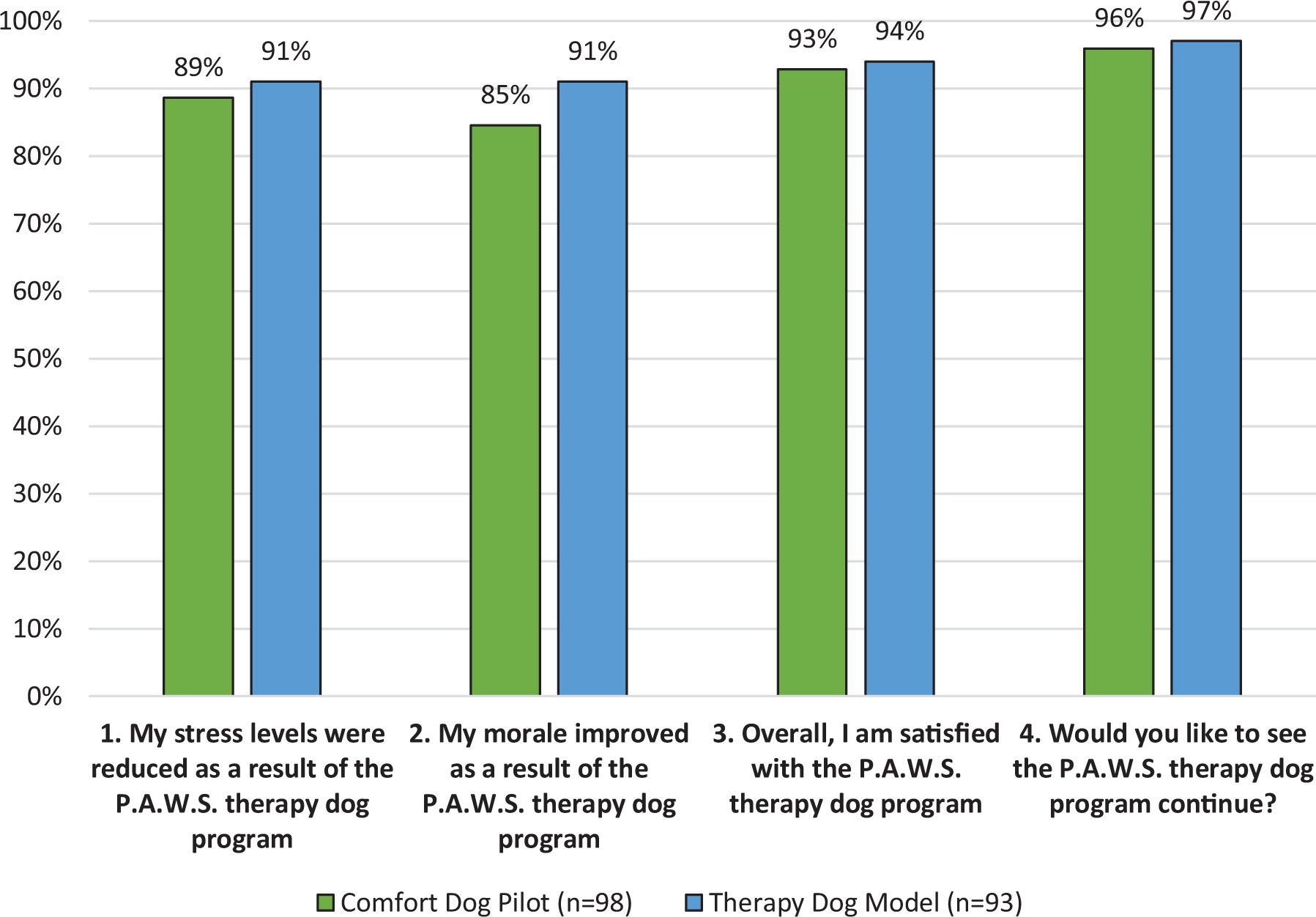
Summary of Pups Assisting Wellness for Staff (P.A.W.S.) final results: comparison of the comfort dog pilot and therapy dog model results.
Several staff members requested expanding P.A.W.S. to include more visits, using certified therapy dogs, and visiting at different times of the day. This feedback was utilized to inform the planning of the second PDSA cycle with the intent of better meeting the diverse needs of the staff.
Therapy Dog Model (May to November 2019)
A total of 5,354 interactions were facilitated over the course of 107 volunteer hours. During the 9 months, a total of 70 walkabout visits in the ED, ICU, and BTHA were conducted. On average, 77 interactions per visit were recorded between staff members and the therapy dogs.
Results from the two staff experience surveys (n = 93) demonstrated positive staff satisfaction and positive staff experience with the therapy dog model phase. Figure 1 demonstrates 91% of the staff “agree” or “strongly agree” the program appears to be inversely related to stress. Survey results indicated 91% of ED and ICU staff saw an increase of morale, with an overall 94% satisfaction rate of the program and 97% supporting its continuation.
Handler survey feedback (n = 5) indicated 100% of handler participants found the mentorship sessions beneficial, with one recommending more time was needed to become acquainted with key contacts.
Qualitative feedback from the Better Impact Volunteer Database demonstrated consistently positive interactions with staff, and several reports indicated that the canine visits occurred when staff expressed they really needed the visit. The handlers further reported that the therapy dogs often provided much needed comfort to patients and their visiting family members as well. More information relating to the qualitative themes will be discussed in the Results summary section.
Results summary
A comparison of key staff experience indicators demonstrated a consistent positive experience between the comfort dog pilot and therapy dog model, with a trend towards improved experience by all indicators, as shown above in Figure 1.
Throughout the project phases, the qualitative data obtained confirmed and further supported the quantitative results. Open-ended questions in polls, comments cards, surveys, and field observations revealed positive staff experiences and satisfaction. Key themes that emerged from the thematic analysis included:
A. Feelings of being cared for by the organization
Thank you for caring for us. (ICU, Therapy Dog Model)
One of the best things the hospital has done for us!” (ED, Therapy Dog Model)
B. Improved unit environment
The therapy dogs brighten up everyone’s day. They make me smile and laugh, even if it is only for a brief moment in my day. Thank you so much!” (ICU, Therapy Dog Model)
Not only did the therapy dogs help decrease staff stress levels but also aided with visiting family members. This program has made a positive impact on our unit and I hope to see it continue in the future. (ED, Therapy Dog Model)
C. Increased staff wellness
The best part of my day—I really needed this. (ED, Comfort Dog Pilot)
The program is fantastic. As a concrete action aimed at improving staff wellness, it is a visible example of the organization’s commitment to its employees. I think it is a natural extension of the value of holism that we professionally embrace. Personally, it brings me great joy to see my colleagues light up when they interact with the dogs. (ICU, Therapy Dog Model)
Opportunities for future implementation were identified: continuing to support having more therapy dogs, increasing the number and duration of the visits, including therapy dogs in debriefs, and implementing P.A.W.S in other care settings across VCH.
One unexpected outcome of the project was how staff would frequently engage in conversations with each other while interacting with the therapy dog, and it appeared the dog helped them discover positive commonalities with each other.
Discussion
A dedicated multidisciplinary team invested approximately 2 years into the planning, implementing, and evaluation of the P.A.W.S project. It was demonstrated throughout this initiative that canine-assisted interventions had positive impacts on acute care staff.
The P.A.W.S. has been recognized by the organization’s Senior Leadership Team (SLT) as well as the ESHW Department as an innovative initiative for supporting staff wellness. In particular, it was brought forward by SLT that P.A.W.S. was aligned to the organization’s core value of “caring for everyone.”
There are limitations to this study. One limitation is that staff who disagreed with the project may be underrepresented in the data. Limited negative feedback was obtained; yet, a few staff members documented on the open-ended feedback section of the surveys that they felt the project did not address the foundations of staff stress. Additionally, assessing the impact of the project on staff wellness is limited taking into consideration that wellness is a complex and multidimensional concept to measure. The indicators of staff satisfaction and staff experience may or may not be necessarily correlated with staff wellness. Furthermore, it is possible that the hazards of canine interactions, which may include allergies, zoonotic infections, and animal bites, 5,6 were not captured by the data. However, these hazards were minimized by ensuring each dog was clean, up to date on vaccinations, and was always in the presence and partnership of the handler. 7
This study describes a positive impact of the P.A.W.S. program on acute care staff and highlights an opportunity to build and sustain the program under the Employee Wellness portfolio. The program will continue to be evaluated for improvement and expansion. This additional information will explore the potential of extending the program’s services beyond the acute care setting. In sharing the experience and preliminary findings from a canine-assisted intervention for acute care staff, the P.A.W.S. team hopes to demonstrate a need for further, more rigorous research in this area and inspire others to implement similar interventions.
Footnotes
Authors’ note
Caton is a student at University of British Columbia, Vancouver, British Columbia, Canada. Brumwell is a Clinical Coordinator of Indigenous Mental Wellness & Substance Use, Aboriginal Health Services, Vancouver Coastal Health (VCH), Vancouver, British Columbia, Canada.
Acknowledgments
The authors would also like to acknowledge the St. John Ambulance Therapy Dog Program Coordinators and Volunteers, Vancouver General Hospital Volunteer Resources Team, and the Vancouver General Hospital Leadership Team for their support on this staff wellness initiative. The authors would also like to acknowledge the contributions of Critical Care Managers Jackson Lam, Lori Korchinksi, Suzie Logie Allen, and Lori Quinn; Epidemiologist Elisa Lloyd Smith; and Executive Sponsors and Senior Leadership representatives Michelle de Moor, Allison Muniak, and Dr. Stacy Sprague. It is through their leadership and commitment to care for everyone that the P.A.W.S. program was able to achieve the impact it did at Vancouver General Hospital.
Funding
The work was supported by existing Vancouver Coastal Health human resources and the therapy dog handlers volunteered their time. The student supporting the comfort dog pilot was initially by the British Columbia Patient Safety and Quality Council as part of their summer internship program.