
Abstract
Objectives:
To evaluate the impact of the Canadian Association of Radiologists (CAR) guidelines on MRI surveillance burden for incidental pancreatic cystic lesions compared with Fukuoka guidelines.
Methods:
This retrospective single-center study included 1000 asymptomatic patients aged ≥40 years with incidental pancreatic cystic lesions identified on abdominal MRI between January 2010 and March 2025. Patients with high-risk features, cysts ≥3 cm, or a history of pancreatic cancer were excluded. Surveillance recommendations were retrospectively simulated according to CAR and Fukuoka guidelines. The primary outcome was the mean number of recommended MRI examinations over 5- and 10-year follow-up periods. Comparisons were performed using paired t-tests.
Results:
A total of 1205 consecutive patients were reviewed between January 1, 2010 and March 31, 2025. Of these, 205 patients were excluded based on study criteria, yielding a final cohort of 1000 patients for analysis. At 5 years, the mean number of recommended MRI examinations was lower under CAR guidelines compared with Fukuoka guidelines (1.45 ± 1.5 vs 3.89 ± 0.99; P < .001). At 10 years, the difference further increased (1.45 ± 1.5 vs 6.23 ± 1.64; P < .001).
Conclusion:
Application of CAR guidelines is associated with a reduction in MRI surveillance utilization over 5- and 10-year follow-up periods compared with Fukuoka guidelines. These findings have important implications in the setting of MRI resource constraints within the Canadian healthcare system.
Introduction
Pancreatic cystic lesions are increasingly encountered in clinical practice, representing a spectrum of entities ranging from benign to malignant lesions. 1 Among these, intraductal papillary mucinous neoplasms (IPMNs) are the most common incidental pancreatic cysts identified in asymptomatic individuals. IPMNs are classified as branch duct, main duct, or mixed type—with branch duct IPMNs being most prevalent and generally associated with a lower risk of malignant transformation compared with main duct lesions. 2
Surveillance is performed to monitor for malignant transformation and to account for the posited increased risk of pancreatic ductal adenocarcinoma elsewhere in the pancreas. 3 With advances in cross-sectional imaging, incidental detection of pancreatic cysts has increased substantially, resulting in a growing population undergoing long-term imaging surveillance. Magnetic resonance imaging (MRI) is the preferred modality; however, it is resource-intensive, with implications for cost, access, and system capacity.
Multiple national and international guidelines have been developed to guide surveillance strategies, with variability in recommended imaging intervals and duration of follow-up. In particular, the Fukuoka guidelines recommend prolonged or lifelong surveillance in many cases, contributing to increased healthcare utilization. 4 Emerging evidence suggests that the risk of malignant transformation in small branch duct cysts without worrisome features may be lower than previously estimated, prompting reconsideration of surveillance intensity. 5
In 2022, the Canadian Association of Radiologists (CAR) introduced updated recommendations for the management of incidental pancreatic cystic lesions, incorporating contemporary evidence and healthcare system considerations. These guidelines advocate a more conservative approach, including limited or no follow-up for very small cysts, age-based cessation of surveillance, and finite follow-up durations in low-risk patients. 6
Given the variability in surveillance strategies and the recent introduction of CAR guidelines, their impact on imaging utilization remains uncertain. This study evaluates the effect of CAR guideline implementation on the number of recommended follow-up MRI examinations compared with Fukuoka-based surveillance strategies.
Methods
Ethics Approval
This study received institutional research ethics board approval with waiver of informed consent due to its retrospective design.
Study Design and Population
This retrospective single-center study was performed at a tertiary care institution. Institutional imaging and electronic medical records were reviewed for the period from January 1, 2010, to March 31, 2025. Given the retrospective exploratory design of the study, a formal sample size calculation was not performed. A target cohort of 1000 patients was selected to provide a sufficiently large sample for comparative evaluation of surveillance recommendations between guidelines and to generate precise estimates across clinically relevant imaging subgroups. Patients undergoing abdominal MRI demonstrating a pancreatic cystic lesion were identified using keyword-based searches of radiology reports. Search results were reviewed consecutively beginning January 1, 2010, and inclusion and exclusion criteria were applied until 1000 eligible cases were identified.
Inclusion criteria consisted of asymptomatic patients aged ≥40 years with an incidental pancreatic cyst identified on MRI. Exclusion criteria included age <40 years, cysts with worrisome features or high-risk stigmata such as enhancing solid component or enhancing mural nodule within the cyst, main pancreatic duct dilation ≥10 mm, cyst size ≥3 cm, and prior history of pancreatic cancer (Figure 1).
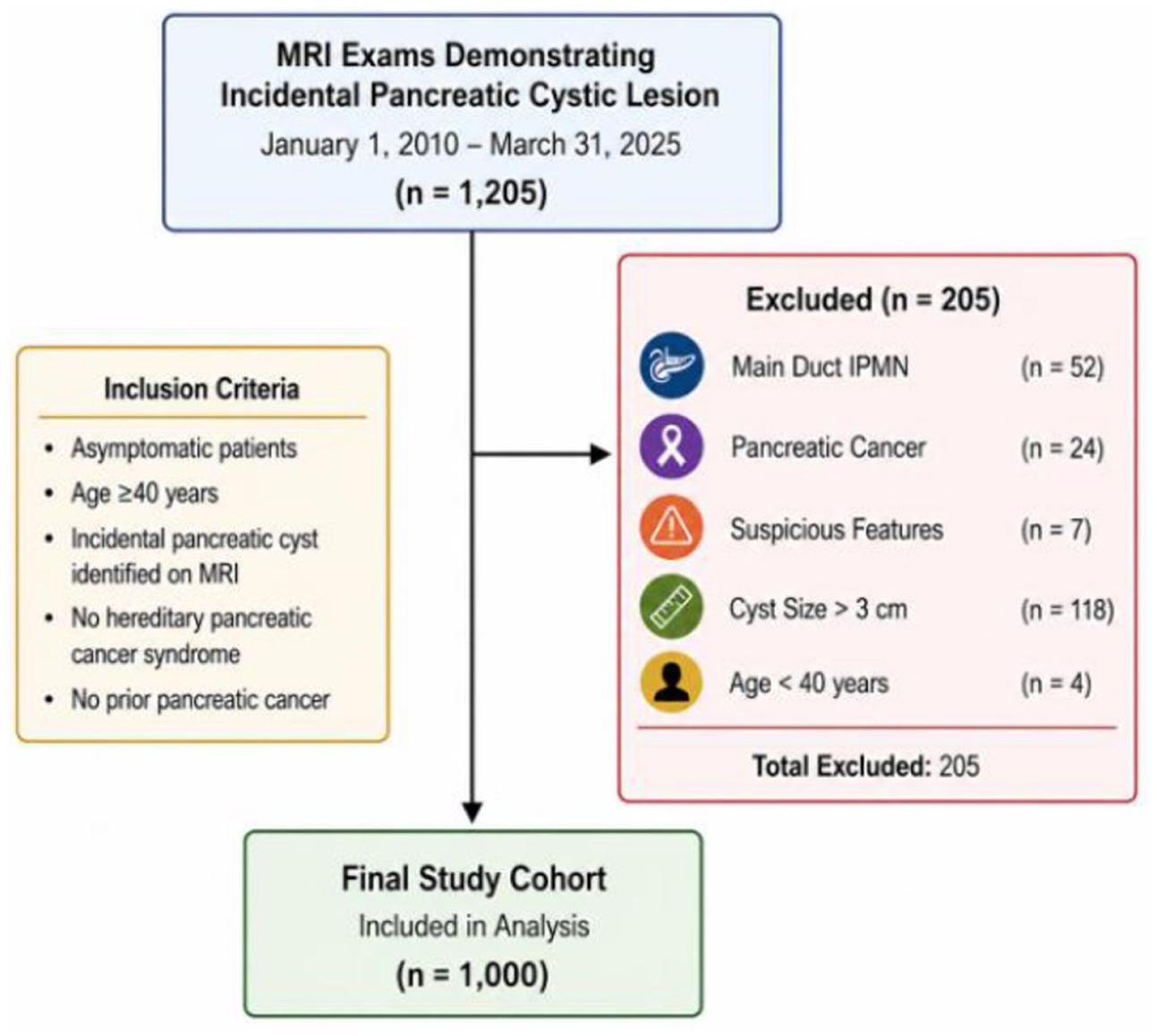
Study flow diagram. A total of 1205 MRI exams were reviewed. After application of exclusion criteria, 1000 patients were included in the final analysis.
The 2017 Fukuoka and 2022 Canadian Association of Radiologists (CAR) incidental pancreatic cyst guidelines were retrospectively applied. Surveillance schedules were operationalized as the cumulative number of MRI examinations over 5- and 10-year horizons based on published imaging intervals, assuming radiographic stability and adherence to guideline-recommended follow-up without extrapolation beyond stated recommendations.
Under the Fukuoka guidelines, cysts <1 cm underwent MRI at 6 months followed by MRI every 2 years if stable. Cysts measuring 1 to 2 cm underwent MRI every 6 months for 1 year, then annually for 2 years, with subsequent extension to every 2 years if stable. Under this operationalization, a 1.1 cm cyst corresponded to 2 MRIs in year 1, 4 by year 3, and 5 by year 5. Cysts 2 to 3 cm underwent annual MRI following an initial endoscopic ultrasound at 3 to 6 months, corresponding to 5 MRIs by year 5 and 10 MRIs by year 10.
Under the CAR guidelines, cysts <0.5 cm required no follow-up. Cysts measuring 0.6 to 2.4 cm underwent MRI surveillance according to recommended intervals; for example, a 1.1 cm cyst corresponded to MRI at 1 year followed by biennial imaging, yielding 3 MRIs by year 5. CAR-based surveillance was complete at 5 years in accordance with guideline recommendations. Cysts ≥2.5 cm were not included in the primary imaging burden comparison, as CAR guidelines recommend consideration of gastroenterology referral rather than routine radiologic surveillance for these lesions. Additionally, patients aged ≥75 years were not recommended to undergo imaging surveillance under CAR guidelines in the absence of high-risk imaging features.
Data Collection
For each patient, MRI reports were reviewed to extract demographic and imaging data, including age, sex, date of index examination, number of cystic lesions, size of the largest lesion, and recommended imaging follow-up interval.
Imaging Review
Direct image review was performed in cases where radiology reports were ambiguous or equivocal. These cases were adjudicated by a fellowship-trained abdominal radiologist to ensure accurate lesion characterization. The cases that met inclusion criteria were added for analysis.
Guideline Application and Outcomes
A total of 1000 patients were included in the final cohort. For each case, surveillance recommendations were retrospectively simulated according to both Canadian Association of Radiologists (CAR) and Fukuoka guidelines. The primary outcome was the mean number of recommended MRI examinations per patient over 5- and 10-year follow-up intervals.
Statistical Analysis
Comparisons between guideline-based surveillance strategies were performed using paired t-tests to evaluate differences in the number of recommended MRI follow-up examinations over 5- and 10-year periods. Given the large sample size, the paired t-test was considered robust to deviations from normality. All tests were two-sided, and P-values <.05 were considered statistically significant. Paired t-tests were performed using R (Version 2025.09.2+418). Statistical significance was defined as two-tailed P < .05.
Results
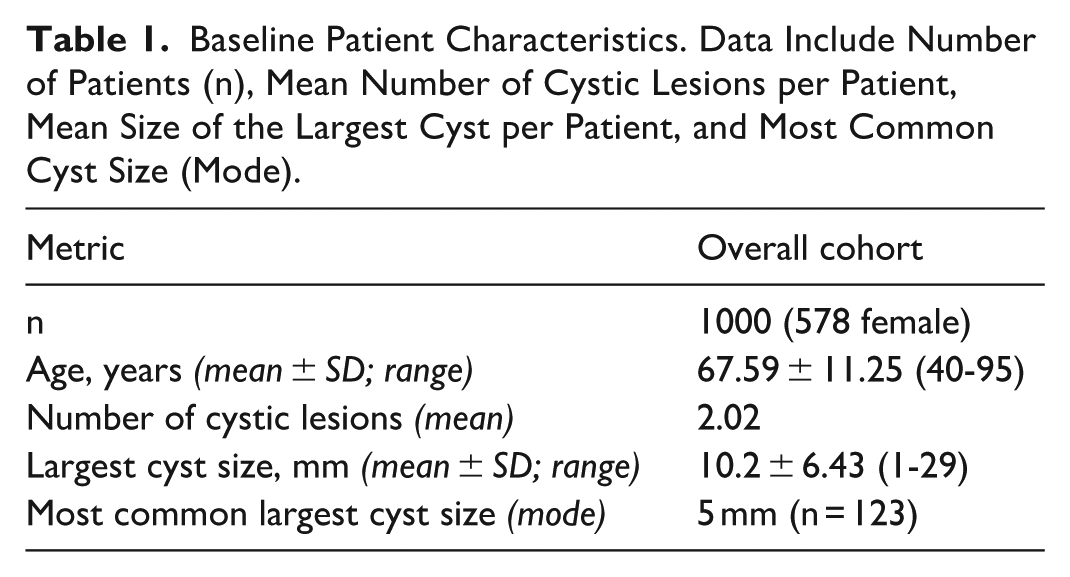
A total of 1000 patients meeting inclusion criteria were included in the analysis. Application of the 2 guideline frameworks demonstrated differences in the number of recommended follow-up MRI examinations over both 5- and 10-year surveillance intervals. Under the Canadian Association of Radiologists (CAR) guidelines, the mean number of recommended MRI examinations per patient was 1.45 at both 5 and 10 years. The constant mean under CAR guidelines reflects the finite duration of surveillance specified within these recommendations, after which no additional imaging is recommended. In contrast, the Fukuoka guidelines resulted in higher imaging utilization, with a mean of 3.89 examinations at 5 years and 6.23 examinations at 10 years (Table 1).
Baseline Patient Characteristics. Data Include Number of Patients (n), Mean Number of Cystic Lesions per Patient, Mean Size of the Largest Cyst per Patient, and Most Common Cyst Size (Mode).
At 5 years, CAR guidelines were associated with a lower number of recommended MRI examinations compared with Fukuoka guidelines (mean difference, 2.44 examinations per patient; 95% CI: 2.34-2.54; P < .001).
At 10 years, the difference between guidelines increased (mean difference, 4.79 examinations per patient; 95% CI: 4.66-4.92; P < .001), corresponding to higher cumulative imaging utilization under the Fukuoka framework (6.23 vs 1.45 examinations).
A substantial proportion of patients in the cohort (n = 288) had pancreatic cystic lesions measuring ≤5 mm, representing the subgroup in which the greatest divergence between guideline recommendations was observed. In addition, 257 patients were aged ≥75 years, also contributing to differences between the Fukuoka and CAR guidelines. Of these, 75 patients were both ≥75 years old and had cysts ≤5 mm.
Discussion
In this retrospective study, we evaluated the impact of applying CAR guidelines compared with Fukuoka guidelines on MRI surveillance burden for incidental pancreatic cystic lesions. Our findings demonstrate a substantial reduction in the number of recommended follow-up MRI examinations when CAR guidelines are applied, with statistically significant differences observed at both 5- and 10-year intervals. Notably, the magnitude of this reduction increases over time, with a mean difference of 2.44 examinations per patient at 5 years and 4.79 examinations per patient at 10 years. These results highlight the potential for meaningful decreases in imaging utilization associated with adoption of CAR recommendations.
A substantial proportion of patients (n = 288) had cysts ≤5 mm, a subgroup driving much of this divergence, as these lesions continue to undergo surveillance under Fukuoka but not CAR in the absence of worrisome features. Similarly, patients aged ≥75 years (n = 257) would not undergo routine surveillance under CAR, further contributing to reduced imaging. Differences in downstream management, including the lower EUS referral threshold under Fukuoka (≥2.0 cm vs ≥2.5 cm under CAR), may also influence overall utilization but were not fully captured in this analysis.
The increasing detection of incidental pancreatic cystic lesions is a well-recognized consequence of the widespread use of high-resolution cross-sectional imaging. Among these lesions, branch duct IPMNs are particularly common and are generally associated with a relatively low risk of malignant transformation, especially in the absence of worrisome imaging features. 5 Despite this, traditional surveillance strategies—most notably those based on the Fukuoka consensus guidelines—have advocated for prolonged, and in many cases lifelong, imaging follow-up. While such approaches prioritize sensitivity for early malignancy detection, they also contribute to escalating healthcare utilization, increased costs, and growing demand on imaging resources.
Our findings align with emerging evidence suggesting that the malignant potential of small, simple branch duct IPMNs may be lower than historically estimated. 5 This evolving understanding has prompted reconsideration of surveillance intensity and duration, particularly in patient populations without high-risk features. The CAR guidelines reflect this paradigm shift by incorporating risk stratification, age-based recommendations, and finite surveillance intervals. Specifically, the CAR approach limits follow-up in very small cysts (≤5 mm), introduces upper age thresholds for surveillance cessation, and defines maximum follow-up durations in low-risk patients. These modifications are intended to balance patient safety with pragmatic considerations related to healthcare resource allocation.
From a health system perspective, reduced MRI utilization may have implications for resource allocation; however, cost estimates should be interpreted cautiously given the absence of a formal economic evaluation. A 2023 study reported that at 10-year follow-up, the CAR guidelines were associated with an expense reduction of $1 392 242 compared with the American Gastroenterological Association guidelines and $1 408 424 compared with the American College of Radiology guidelines. 7 These costs reflected MRI utilization, gastroenterology consultation, and surgical consultation. Further research is needed to evaluate the comparative cost implications of the CAR and Fukuoka guidelines. Reduced surveillance imaging may also help alleviate imaging demand and improve access for higher-acuity indications. Furthermore, limiting follow-up in older patients or in those unlikely to benefit from surgical intervention aligns with broader principles of patient-centered care and may help avoid unnecessary medicalization.
These findings should be interpreted in a clinical context. Although reduced surveillance intensity improves resource utilization, it raises concern for delayed detection of malignant transformation. The risk of malignancy in small, asymptomatic branch-duct IPMNs without worrisome features is low but not zero, making safety dependent on appropriate patient selection and adherence to guidelines. This study was not designed to assess outcomes such as malignancy or survival, so oncologic safety cannot be inferred. A 2023 study of CAR implementation reported that 5 of 419 patients in whom surveillance was discontinued subsequently developed pancreatic malignancy. 7 Additionally, there is limited evidence that more intensive surveillance improves clinically meaningful outcomes even when malignancy is detected.
Our study has several limitations. First, as a retrospective analysis, it is subject to inherent biases, including reliance on the accuracy and completeness of radiology reports and clinical documentation. Although imaging review was performed in cases of ambiguity, most data was derived from report-based extraction, which may introduce variability. Second, the application of guideline recommendations was performed retrospectively and assumes strict adherence to each guideline, which may not reflect real-world clinical practice where individualized decision-making often occurs. A 2023 study evaluating adherence to the CAR recommendations demonstrated that 45.7% of patients received follow-up recommendations outside of the proposed guidance. 7 Third, this study was conducted at a single tertiary care center, which may limit generalizability to other practice settings with different patient populations, referral patterns, or resource availability.
Despite these limitations, our study provides practical and clinically relevant data that may inform decision-making at both institutional and policy levels. The findings support the notion that guideline selection has a significant impact on imaging utilization, and that adoption of CAR recommendations could lead to reductions in MRI demand. Given the increasing prevalence of incidental pancreatic cysts and the ongoing pressures on healthcare systems, such data are timely and relevant.
Future directions include multicenter studies to validate these findings across diverse practice environments, further economic analysis, as well as integration of risk prediction models that incorporate imaging, clinical, and potentially molecular biomarkers to further refine surveillance strategies and research on impact on patient important outcomes.
In conclusion, this study demonstrates that application of CAR guidelines for incidental pancreatic cystic lesions is associated with a significant reduction in recommended MRI surveillance compared with Fukuoka guidelines, particularly over longer follow-up periods. These findings highlight the potential for improved resource utilization and reduced healthcare burden with adoption of a more pragmatic, risk-based surveillance strategy. Ongoing evaluation of clinical outcomes will be essential to ensure that these benefits are achieved without compromising patient safety.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.